
Abstract
Surgical exposure for total elbow replacement should provide complete visualization of the joint surfaces. The soft tissue reconstruction following replacement often requires protection and can lead to complications such as triceps tendon rupture. We describe a modification of the posterior approach to the elbow that provides optimal exposure and allows early mobilization.
Introduction
Total elbow replacement is a surgical procedure that aims to restore pain-free, functional range of movement in patients with arthritic elbows or complex elbow fractures. Various surgical approaches have been described for performing this procedure and the optimal approach should allow access to the entire articular surface without causing subsequent morbidity. Access for elbow replacement is commonly gained posteriorly, using surgical approaches that either disrupt the continuity of the extensor mechanism or maintain the continuity. Campbell described a posterior triceps splitting approach to gain access to the joint. 1 The tendinous portion may be turned as an inverted U-shaped flap to aid repair later. Bryan and Morrey published their extended posterior approach in 1982, where the extensor mechanism is reflected radially by releasing the triceps tendon, forearm fascia and the periosteum as one unit from medial to lateral off the olecranon. 2 Lifting the triceps insertion with an olecranon osteotomy offers the best exposure to the joint, although its use for total elbow arthroplasty is limited by the need to repair the osteotomy with the prosthesis in place. 3 There have been other variations of these approaches, such as Ranawat's modification of the extensor sliding approach, 4 a paratricipital approach, a medial epicondyle osteotomy approach 5 and a radial approach. 6 Complications such as weakness of triceps or avulsion of triceps have been reported with these approaches. 7 We describe an approach that is a modification of the Bryan–Morrey approach and aims to minimize this risk by allowing better repair of the mechanism, thereby promoting better healing and early mobilization.
Surgical technique
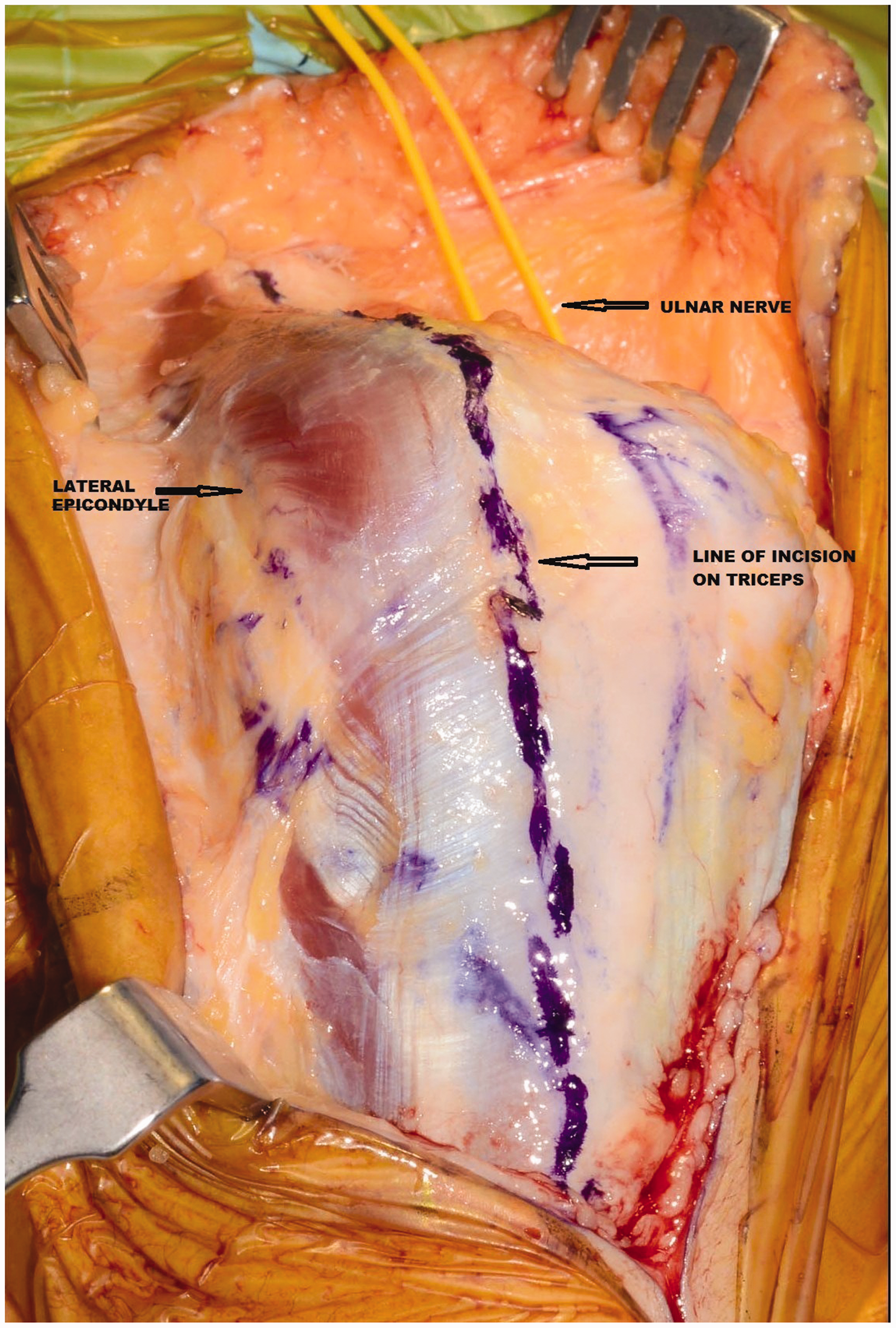
The procedure is carried out with the patient in a lateral decubitus position with the elbow flexed over an arm support. A posterior midline incision is made starting 8 cm proximal to and ending 8 cm distal to the tip of the olecranon curving laterally around it in the middle. The incision is deepened to the muscular plane and fasciocutaneous flaps are raised on either side to the epicondyles. On the medial side, the ulnar nerve is identified, decompressed superficially within the cubital tunnel, and protected. Transposition of the nerve is not routinely performed and is reserved for cases with bony deformity or in revision surgery. A longitudinal incision is made on the exposed triceps tendon, on the radial side of the midline, avoiding the tip of the olecranon. The incision is carried distally to expose the radial head and the radial head is excised proximal to the annular ligament. A 5-cm sliver of olecranon is elevated using a sharp osteotome from lateral to medial direction and the incision is carried medially at the distal end with subperiosteal elevation of flexor carpi ulnaris (FCU). This allows the whole flap of the triceps insertion along with the sliver of olecranon and FCU be reflected medially, exposing the dorsal capsule of the joint and the fat pad. The dorsal capsule and tip of olecranon process are excised to help instrument access to the proximal ulna. Release of the posterior parts of the medial and lateral collateral ligaments allows the elbow to be dislocated. The extent of release of these ligaments is decided based on the type of prosthesis that is used, with more liberal release for linked prostheses to enable accurate alignment of the components. The implants are inserted in accordance with the manufacturer’s instructions after appropriate preparation of the joint surfaces. Once the prosthesis are inserted, the extensor mechanism is repaired, starting with transosseous sutures to secure the elevated sliver of olecranon down to its bed. The repair is completed with side-to-side sutures for the triceps tendon and distal soft tissues. The wound is routinely closed after inserting drains and a compression bandage is applied to prevent haematoma formation and subsequent infection. The drains are removed after 24 hours to 48 hours, leaving an adhesive dressing to cover the wound. All patients undergo a streamlined physiotherapy regime starting with gentle active and passive mobilization limited to 90° for 6 weeks, followed by resisted flexion and extension exercises until triceps function is fully restored.
Patient in lateral decubitus position with elbow flexed over arm support. Posterior midline incision marked, curved radially around the tip of olecranonLegend. Fasciocutaneous flaps raised on both sides, Ulnar nerve identified and protected. Line of incision along lateral border of triceps tendon and extended distally along lateral border of ulna.
Discussion
A few surgical approaches have been described to perform elbow replacement surgery and complication rates can be as high as 43% with 2% to 5% complications related to the triceps. The crucial and difficult step in Morrey’s approach is to elevate the triceps insertion off the olecranon at the same time as maintaining distal continuity through a thin layer of periosteum and the anconeus. Our modification of the approach makes this process easier by elevating the sliver of olecranon which gives a more substantial thickness to the reflected extensor mechanism compared to the thin layer of periosteum over the olecranon, which can tear easily, causing a break in the extensor mechanism. Furthermore, our medial based flap allows more direct access to the proximal radius and ulna as opposed to the Morrey's approach where a radial based flap is raised. We have used this approach for more than 100 elbow arthroplasties in the last 4 years with no reported triceps ruptures. This modified approach offers excellent exposure of the elbow joint, allows a solid repair of the triceps mechanism, and enables early mobilization after total elbow arthroplasty.
Extensor mechanism of the elbow repaired securely after insertion the elbow prosthesis.
Footnotes
Acknowledgements
We would like to acknowledge the help of the Medical Illustrations Department at Wrightington Wigan and Leigh NHS trust for providing the photography for the illustrations.