
Abstract
The elbow is the second most commonly dislocated major joint in adults. Good long-term outcomes have been reported after non-operative management; however, a small proportion (<10%) of patients have a poor outcome and some do require surgical intervention. A review of the anatomy, pathoanatomy, management and outcomes of simple elbow dislocations is presented. Emphasis is placed on emerging concepts regarding the soft tissue injury, the stabilising structures that are injured, the sequence and mechanism of injury and the relationship to elbow stability. The benefits of nonsurgical and surgical management are discussed and a treatment algorithm based on the pathoanatomy is proposed.
Introduction
The elbow is the second most commonly dislocated major joint in adults. 1 Josefsson et al. 2 described simple dislocations as those where there had been no concomitant fracture apart from small periarticular avulsions 1 mm or 2 mm in diameter. Good long-term outcomes have been reported after nonoperative management; however, a small proportion (2%) of patients do require surgical intervention 3 and approximately 8% of patients with simple elbow dislocations will go on to have symptoms of persistent instability if treated nonoperatively. 4
Epidemiology
Anakwe et al. 4 reported an incidence of 2.9 per 100 000 population per year in those over 16 years of age. Men were more likely to sustain a dislocation after assault or sports, whereas women were likely to suffer dislocations in a fall from standing height.
Josefsson and Nilsson 5 reported an incidence of 6.05 simple elbow dislocations per 100 000 individuals during their lifetime.
The largest epidemiological study was conducted by Stoneback et al., 6 who used a multicentre database in the USA to estimate an incidence of 5.21 simple elbow dislocations per 100 000 person-years. There was a statistically significant male predominance (53% men). The greatest difference in incidence was found in the 10-year to 19-year-old age group, with males having almost twice the incidence (8.91 per 100 000 person-years). 6 Other studies show a similar epidemiology, with dislocations occurring most commonly in those under 30 years of age.5,7–9
Falls were the most common mechanism of injury (56.5%) and most dislocations occurred at home (51.5%). Forty-four percent of dislocations occurred as a result of sporting activities, 6
Normal anatomy
Bony anatomy
The elbow joint is a highly congruent articulation that confers substantial bony stability. 10 The coronoid process enhances stability particularly in flexion and the contact area of the radio-capitellar joint increases with flexion. 11 The rotary engagement of the olecranon has a stabilising role in extension.
Capsuloligamentous anatomy
The medial collateral ligament (MCL) complex consists of three parts. The anterior bundle originates from the antero-inferior surface of the medial epicondyle of the humerus and inserts onto the sublime tubercle. 12 The posterior and transverse bundles are often less discrete structures. 12
The lateral collateral ligament (LCL) has four components: the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), the accessory collateral ligament and the annular ligament. The annular ligament attaches to the anterior and posterior margins of the lesser sigmoid notch. The remaining three components take origin from inferior surface of the lateral epicondyle. The LUCL inserts on the crista supinatoris, the RCL inserts onto the annular ligament and the accessory collateral ligament attaches to both. 10 The medial and lateral ligament complexes contain mechanoreceptors including Golgi organs, Ruffini terminals, Pacinian corpuscles and free nerve endings.
Muscles
Four main groups of muscles cross the elbow joint providing dynamic stability via joint compression. 10 The biceps and triceps are considered to play an important role in proprioception.
Stabilising structures
Stability of the elbow is derived from both static constraints and dynamic forces. The static constraints are commonly divided into primary and secondary based on their contributions to joint stability and the dynamic stabilisers consist of all muscles that cross the elbow joint. Primary constraints are the ulnohumeral articulation, the LCL and the anterior MCL. 13 Secondary constraints are the radio-humeral articulation, common extensor group, brachioradialis and the common flexor-pronator group. In the uninjured elbow, the greatest laxity is found with the forearm in neutral rotation. 14
Primary stabilisers
It has been postulated that the ulnohumeral articulation contributes up to 50% of the stability of the elbow.13,15–19 By definition, the osseous stability is not compromised in simple dislocations.
The MCL complex plays a vital role in primary stability of the elbow in valgus and posteromedial directions. The insertion of the MCL is slightly posterior to the medial epicondyle (and the centre of rotation) and hence the components of the MCL have variable tension during flexion and extension. The anterior part of the anterior bundle is the most important contributor to valgus stability through almost the entire range of flexion; the posterior part contributes equally at 120° of flexion. 20 Division of the anterior bundle alone is sufficient to destabilise the elbow to varus–valgus load independent of forearm position. 21 The posterior bundle plays a role in posteromedial instability, demonstrated by the resultant instability following its isolated transection. 22 The transverse bundle of MCL does not contribute significantly to stability. 23
The LCL is the primary constraint to external rotation and varus stress. Complete sectioning of the LCL causes not only varus and posterolateral instability, but also subluxation of the radial head posteriorly. 24 The origin covers the flexion axis and therefore it remains isometric throughout the range of flexion extension. 23 This may help explain the fact that the LCL complex acts as a single functional unit, with section of any one of the three structures having only minimal impact on elbow stability.24,25 It requires injury or sectioning of at least two to significantly impact on stability. The LUCL provides varus and posterolateral stability. 26
Secondary stabilisers
The radial head is an important secondary stabiliser that in combination with the coronoid provides posterolateral stability after reduction of a simple dislocation. The anterior capsule stabilises in extension 16 and plays an important role in resisting valgus stress. 13
The muscles that traverse the elbow are important secondary stabilisers and have both passive and active stabilising effects. The degree of contribution from each muscle depends on the degree of flexion 27 but the forearm rotation does not affect the stabilising effect of biceps, brachailis or triceps. 21 This dynamic stabilising effect must not be overlooked. The varus force generated during throwing has been extensively investigated and the maximal torque generated is higher than the load to failure of the MCL. 28 Thus, the secondary stabilisers must play a vital role, and simulation of the contraction of FCU and FDS restores stability in a MCL deficient cadaveric model. 29
Passive tension within muscles also provides a stabilising effect. The unloading of biceps, triceps and brachialis causes an increase in varus–valgus laxity in all positions of flexion. 21 The flexor–pronator mass on the medial side is an important secondary stabiliser to valgus force. The combined tendon provides a stabilising force that is maximal when the forearm is supinated. 21 It may be that FCU is best positioned to provide medial support to the elbow as it lies directly over the anterior bundle of the MCL. This stabilising effect is more pronounced at 120° of flexion. 30 The muscles from the common extensor origin have maximal tension in full pronation and it is in this position that they function most effectively as a varus stabiliser. 21 Anconeus is assumed to act as a dynamic constraint to varus and posterolateral instability.31–33
Forearm rotation may play a role in stabilising the elbow joint especially in the presence of injury. Supination stabilises the MCL deficient elbow 34 and those in which there is a large coronoid fracture, 15 whereas pronation stabilises the LCL deficient elbow. 25 It is likely that this is explained by increasing tension and contribution from the secondary stabilisers.
This is relevant because work by Joseffson et al.35,36 identified disruption of the tendinous secondary stabilisers, particularly the long wrist flexors and extensor origins, as an important determinant of acute instability after simple elbow dislocation.
Mechanism
The most common direction of elbow dislocation is posterior or posterolateral;5, 8 however, the exact mechanism has been the subject of debate.
Valgus external rotation theory
Osborne and Cotterill 37 stated that dislocation was the result of a fall on a partially extended elbow. The lateral sloping medial surface of the trochlea, by a cam action, converting the force transmitted via the forearm into a combination of lateral rotation and valgus strain. The greatest movement is on the outer side of the joint where the lateral ligament is stripped superiorly and the posterolateral capsule torn, allowing the radial head to rotate backwards from the capitellar surface. It was postulated that the medial ligament was stripped from bone but remains in continuity with the periosteum, therefore appearing intact upon stressing after reduction.
This theory was further developed by O’Driscoll et al.,26,38,39 who proposed that dislocation occurred by falling onto the outstretched hand with the elbow extended. Immediately upon hand impact with the ground, the elbow begins to flex and the triceps is eccentrically loaded (principally the medial head), producing an external rotation moment at the ulnohumeral joint. Contraction of the adductors and internal rotators of the abducted shoulder internally rotate the humerus against the forearm and hand, which are stabilised by the ground. Further internal rotation torque develops as the body rotates internally with respect to the hand (forearm rotates externally on the humerus). A valgus moment results because the mechanical axis is medial to the elbow. Posterolateral rotatory subluxation results from a combination of supination (or external rotation) with valgus and axial compression during flexion.26,38,39
Valgus hyperextension theory
Linscheid and Wheeler contended that dislocation of the elbow results from a fall with the elbow in hyperextension. 40 More recently Schwab et al. 41 stated that ‘the initial step in elbow dislocation is hyperextension of the joint, which either ruptures or avulses the medial collateral ligament, or fractures the medial epicondyle with the medial collateral ligament attached. Disengagement of the coronoid process from the laterally sloping surface of the trochlea then initiates the posterolaterally directed dislocation of the olecranon–coronoid complex, with the radial head frequently following. The dislocation cannot proceed medially because of the bony block afforded by the trochlea’.
Evidence supporting this theory has been published more recently by Schreiber et al. 42 In their analysis of YouTube (www.youtube.com) video footage of 62 elbow dislocations, they reported that most elbow dislocations are the result of a hyperphysiologic valgus moment in an extended elbow. This mechanism would require an initial disruption of the anterior portion of the anterior band of the MCL. In their model, the soft tissue disruption progresses from the medial to the lateral side of the elbow. The most common arm position at the time of dislocation was forearm pronation, shoulder abduction and forward flexion, with the elbow at near or full extension. The typical deforming forces experienced were a valgus moment with an axial load and progressive supination.
Pathoanatomy
O’Driscoll et al.38,39 described sequential soft tissue disruption from lateral to medial, termed the ‘Horii circle’. The soft tissue injury was said to occur in stages, with stage 1 beginning on the lateral side of the elbow with partial or complete disruption of the LUCL, resulting in posterolateral rotatory subluxation of the elbow. In stage 2, further disruption both anteriorly and posteriorly leads to incomplete posterolateral dislocation. In stage 3A, all the soft tissues are disrupted around to and including the posterior band of the MCL. This leads to posterior dislocation of the elbow. In stage 3B, the entire medial ligament complex is disrupted. In stage 3C, the entire distal humerus is stripped of soft tissues; the flexor–pronator origin is disrupted. This mechanism was supported by video analysis of a college wrestler sustaining an elbow dislocation. The evidence presented for the validity of the Horii circle included a cadaver study in which 12 of 13 elbows could be dislocated posteriorly with the anterior band of the MCL intact. 38 Schwab et al. 41 found, however, that it was not possible to experimentally cause posterior or posterolateral elbow dislocation with a functionally intact MCL.
The ‘Horii circle’ describes an injury originating on the lateral side, although other studies have proposed that the soft tissue injury sustained during elbow dislocation begins on the medial side. Evidence supporting this has been published recently by Schreiber et al. 43 who reviewed magnetic resonance imaging (MRI) scans (performed within 8 weeks of injury) of the elbows of 16 patients after a simple elbow dislocation. All scans showed either high-grade partial tears or complete disruption of the anterior or posterior parts of the anterior bundle of the MCL; 69% of patients had a complete disruption of the anterior part of the anterior bundle of the MCL and 81% complete disruption of the posterior part. On the lateral side of the elbow, the LUCL was uninjured or only had a partial tear in 37% of cases. Although 63% had complete LUCL disruption, this was significantly fewer than those with medial-sided injuries. All of the scans showed increased fluid signal in the common flexor origin and the flexor–pronator origin. However, the study is prone to exclusion bias as a result of the small proportion of simple dislocations that underwent MRI examination (16/107).
Rhyou et al.
44
examined elbow MRI scans in fifteen patients who had sustained simple elbow dislocation and nineteen with pure ligament injuries but without dislocation. In posterolateral dislocations, there was always more severe soft tissue injury on the medial side of the elbow compared to the lateral side (Fig. 1). This was described as greater displacement and signal changes of the torn MCL and overlying muscles. In the much rarer posteromedial dislocations, the soft tissue injury was more severe on the lateral side of the elbow (Fig. 2). In the posterolateral dislocations, an MRI appearance consistent with a distractive mechanism of soft tissue injury was seen on the medial side of the elbow. The associated appearances on the lateral side of the elbow were consistent with a soft tissue stripping mechanism. Associated bone contusion was seen in the radial head and capitellum. It was concluded that the injury begins medially with most of the energy disrupting of the medial soft tissues (MCL and flexor–pronator mass) in a distractive type mechanism. The coronoid becomes disengaged and the radiocapitellar joint dislocates with a pathological forearm external rotation, causing radiocapitellar bone contusion and stripping of the lateral soft tissues from the humerus, ending in posterolateral dislocation.
Perched elbow dislocation. (a) Plain lateral radiograph of perched dislocation of the elbow. (b) Magnetic resonance imaging of the same elbow after reduction demonstrating isolated medial ligament avulsion (arrow) with intact lateral structures. A rare posteromedial dislocation. (a) Plain radiograph. (b) Magnetic resonance imaging demonstrating intact medial structures (white arrows common flexor origin and medial collateral ligament) and complete avulsion of all soft tissue structures from lateral epicondyle (large black arrow common extensor origin and small black arrow lateral ligament complex).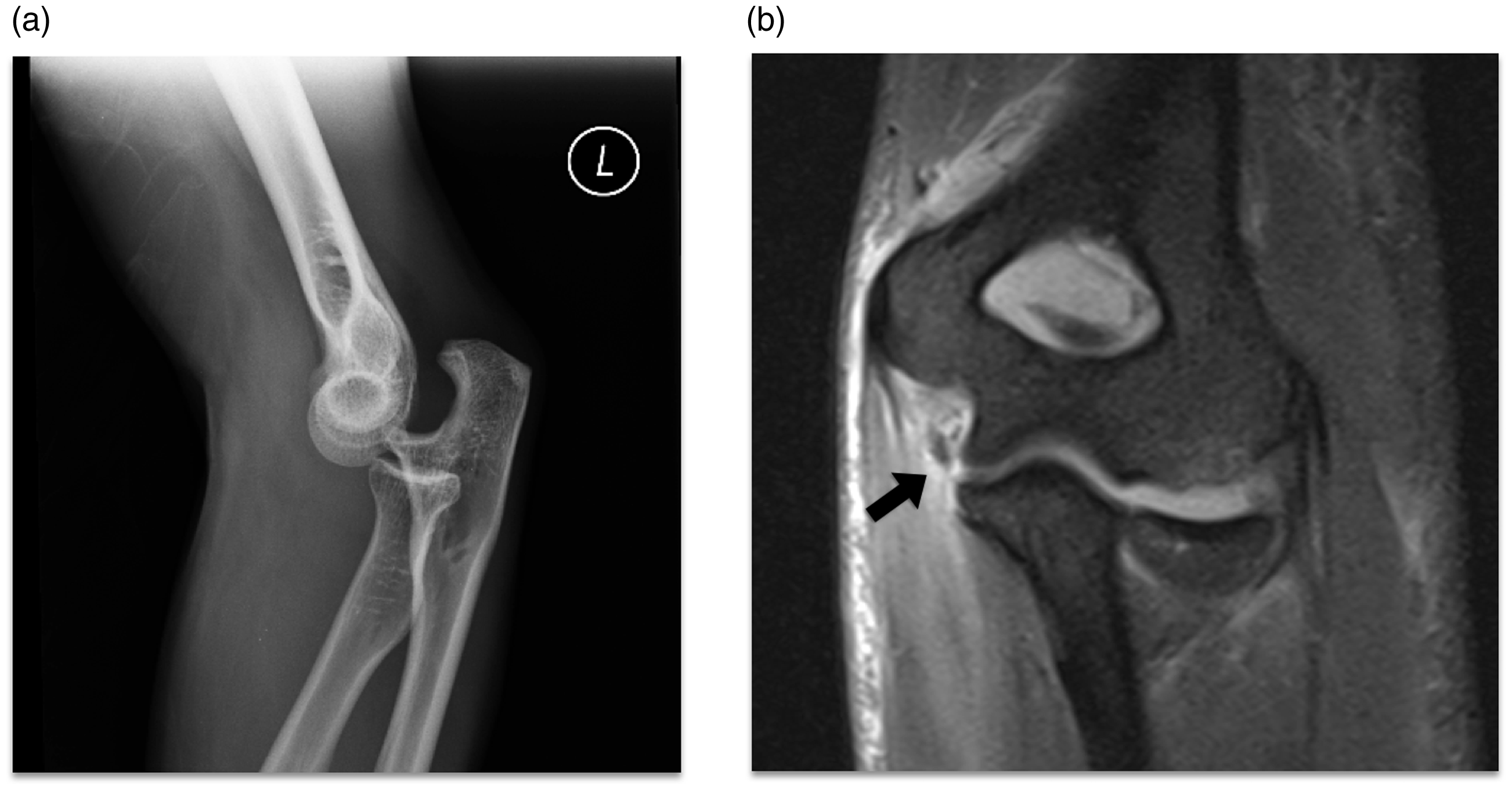

Other evidence comes from cadaveric studies where posterior elbow dislocation was simulated by applying valgus and external rotation forces to elbows in 30° of flexion. 45 Out of ten elbows tested, eight sustained an injury to the anterior bundle of the MCL and five to the posterior bundle of the MCL. Only two specimens sustained injuries to the LCL; these were avulsions from the humerus.
In a randomised trial comparing surgical and nonsurgical treatment of ligament injuries after simple elbow dislocation in 30 patients, Josefsson et al. 35 reported their intra-operative findings from the 15 surgically treated elbows. The muscles originating from the epicondyles were found to be either completely or partially avulsed; medially in 12 patients and laterally in six patients. Both the medial and lateral collateral ligaments were found to be completely ruptured, although only eight elbows exhibited lateral instability. Prior to randomisation, all patients underwent examination under anaesthesia (EUA). All elbows showed medial ligamentous instability in full unforced extension. Sixteen elbows also had lateral ligamentous instability; this was generally less severe than the medial instability.
In a further series of 31 simple elbow dislocations, all underwent EUA an average of 2 days (0 days to 5 days) after injury. 36 All had valgus instability and eight had varus instability. All 31 had surgical exploration of the medial side of the elbow. Nineteen of the 31 had partial or complete rupture either from the medial epicondyle or a tear in the ‘tendinomuscular’ substance. Eighteen elbows were explored on the lateral side either as a result of varus instability (eight elbows) or lateral haematoma (ten elbows). All were found to be completely ruptured or avulsed from the epicondyle. Fourteen of the 18 elbows had varying degrees of lateral tendon ruptures or avulsions from the epicondyle. All elbows in the study had extensive damage to the anterior capsule and the brachialis muscle. Of the nine elbows that were easily dislocated under anaesthesia, eight were explored both medially and laterally, and these all had injuries to the muscles originating from the epicondyles. The study raises some interesting points. First, there is always some instability present upon EUA after acute elbow dislocation; second, considerable medial elbow instability in the extended position is common, whereas lateral instability is not; and, third, dislocation was always associated with complete rupture of the MCL. Of the elbows that were easy to dislocate at EUA, musculotendinous injury was more commonly seen.
Eygendaal et al. 46 analysed outcomes after simple posterolateral elbow dislocation in relation to medial collateral ligament function. Patients were treated in a cast for three weeks after dislocation. Medial instability on standardised stress radiographs (>3 mm opening compared with uninjured elbow) was correlated with persistent pain and a worse Hospital for Special Surgery score. Medial instability was also correlated with arthrosis. Six of the eleven patients with a normal MRI appearance of the MCL had instability on stress radiographs. All elbows with an MRI diagnosed MCL rupture or avulsion were unstable on stress radiographs.
Taken together, the literature indicates that most injury patterns fall into two groups: posterolateral and posterior dislocation in which the soft tissue disruption initiates and is more severe on the medial side of the elbow, as well as posteromedial dislocation (rare) in which the injury initiates and is more severe on the lateral side of the elbow. Common to all studies is the finding that elbow dislocations have a spectrum of soft tissue injury. For most simple elbow dislocations, the injury ladder starts with a medial ligament avulsion and ascends to complete avulsion of the common extensor origin (Fig. 3).
Injury ladder for the more common posterolateral simple elbow dislocations. The injury starts medially. The aim of surgery is to reduce the risk of chronic instability by downgrading the injury: ‘bringing the patient down the ladder’.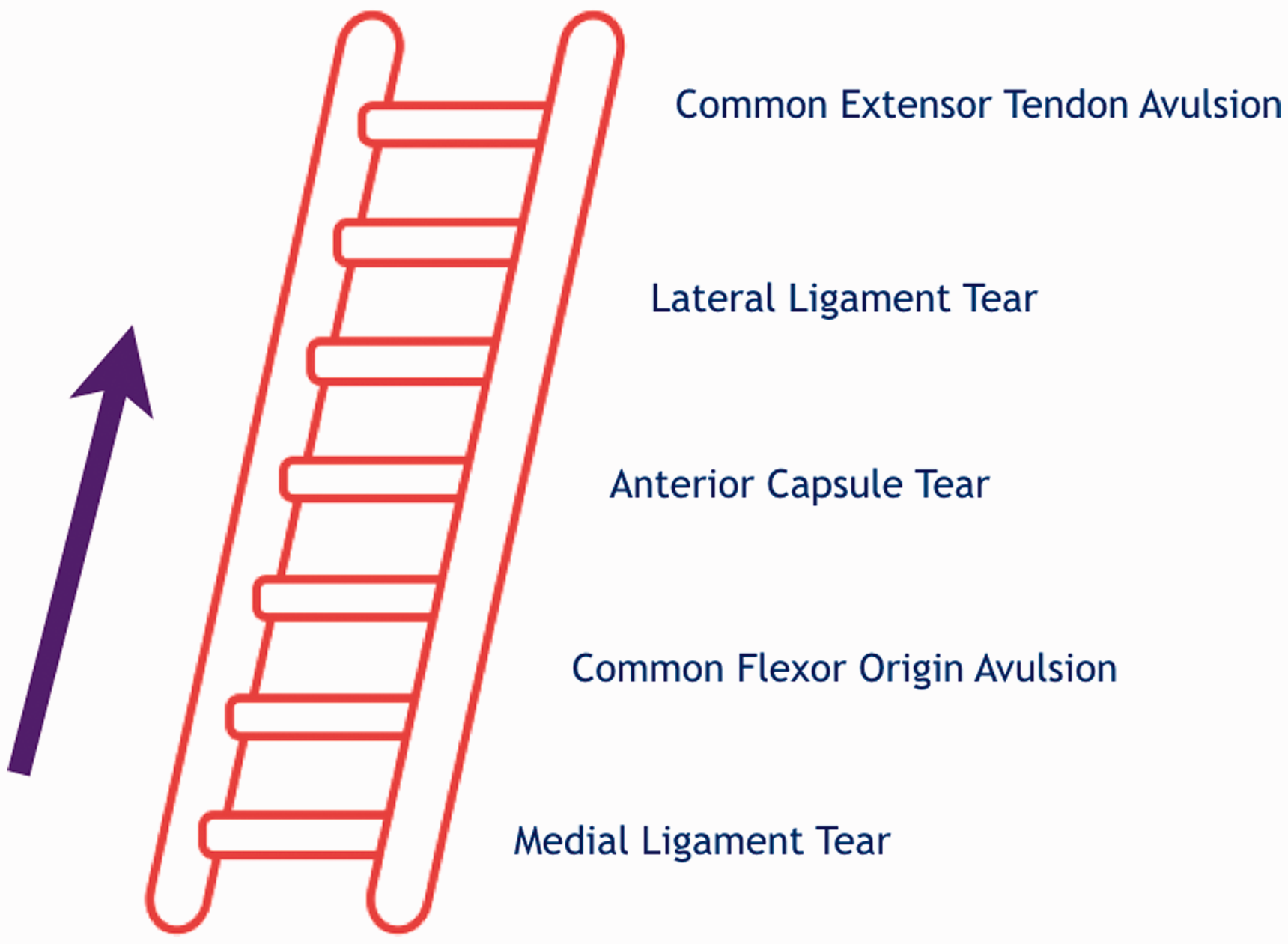
Divergent dislocations, where the radius dislocates laterally and ulna medially, are very rare and are usually paediatric injuries. 47 Anterior dislocations of the elbow without fractures are extremely uncommon. 48
Diagnosis
In most cases, the orthopaedic surgeon will encounter the patient for the first time in the fracture clinic with the elbow having been reduced in the emergency department. In our experience, it is rare that an assessment of stability was performed at the time of reduction. This may differ between units and communication with the emergency department regarding this is encouraged. Examination of elbow stability at the time of reduction gives important information to guide management. This depends greatly on who reduces the elbow and where this is performed.
History
The history and initial examination will usually provide the diagnosis but the exact mechanism of the dislocation (limb position upon impact) and the direction of fall should be determined as accurately as possible. If the patient presents without a dislocated elbow but with a history of apparent dislocation, inquiries should be made about a history of a clunk or click, deformity at the time of injury and a subjective feeling of elbow instability. The patient should be asked about any neurological symptoms.
Examination
Any cast or dressing should be removed. The elbow should be examined for medial bruising. Lateral bruising suggests high-grade injury as a result of disruption of the tough lateral fascia. Tenderness should be sought over the medial and lateral structures. Testing for ligament integrity in clinic in the acute injury is unlikely to be fruitful as a result of pain inhibition. The patient should be asked to try to actively move the elbow, and reluctance to do so may be a sign of more significant soft tissue injury. A thorough neurovascular assessment of the distal extremity should be undertaken and documented. The elbow can usually be placed into a sling at this point.
Imaging
Anteroposterior and lateral plain X-rays are essential in elbow injuries. These should be examined for fractures and joint congruency. Radiographs should be repeated at 1 week after reduction or stabilisation to ensure the reduction has been maintained. Computed tomography scanning is useful if there is suspicion of a significant fracture that is not defined satisfactorily by radiographs, or to better delineate associated fractures. However, it is the preference of the senior author (ACW) to use MRI scanning after simple elbow dislocation (obtained within 1 week of the consultation). MRI will demonstrate the pathoanatomy of the soft tissue injury (Figs 1b, 2b and 4). The integrity of the stabilising ligaments and tendons can be determined and therefore the stage and severity of the injury can be clarified. Attention should be paid to the integrity of the anterior and posterior bundles of the MCL, flexor–pronator origin, lateral ligament complex and common extensor origin. The role of MRI is controversial and the results should be taken in the context of the whole clinical picture. There is a risk of over-treating patients if MRI is relied upon too heavily.
Ultrasound scanning may provide a valuable adjunct to the clinical examination. The collateral ligaments and the common flexor and extensors can also be viewed in the dynamic situation, although examination may be limited by soft tissue swelling and patient comfort.
Examination under anaesthesia
It is the practice of senior author (ACW) to undertake EUA if the MRI scan shows that the soft tissue injury extends to the lateral structures, or if there is a clinical suspicion of a high-grade soft tissue injury. This is usually performed in the first 1 week to 2 weeks after the injury. Under fluoroscopy, the elbow is assessed in full extension and 30° flexion, in full pronation and supination, and under varus and valgus stress. During maximal varus and valgus stress, the angle is measured between the distal humeral joint line and the proximal ulnoradial joint line on the anteroposterior image. Gross instability is defined as an elbow that re-dislocates under examination. Mild and moderate instability are determined by angular displacement of 10° or less (mild) or more than 10° (moderate) on stress testing. 49 Schnetzke et al. 49 used this protocol to determine whether initial joint stability affected the outcome after simple elbow dislocation. 49 Those with moderate instability had a worse Mayo elbow performance score, elbow extension was significantly worse, and there was an eight-fold higher odds ratio for secondary surgery. A retrospective study has indicated that those with more than mild instability are best managed with early surgical stabilisation. 50
It is acknowledged that use of MRI is not current practice in most units. Instead, treatment decisions are made at the time of elbow reduction and immediate EUA. This area requires further research.
Treatment
Nonsurgical management
Nonsurgical treatment typically involves immobilisation in an above-elbow plaster. There is good evidence that immobilisation for longer than 2 weeks to 3 weeks leads to poorer outcomes with respect to elbow range of movement.9,51–53
Recently, the results of the FuncSiE (functional treatment versus plaster for simple elbow dislocations) trial were reported. 54 This was a multicentre randomised trial of 100 patients that compared 3 weeks of plaster immobilisation with early mobilisation after simple elbow dislocation. The primary outcome measure was the Quick-Disabilities of the Arm, Shoulder and Hand (QDASH) score at 1 year. In the early mobilisation group, the arm was put in a bandage for up to 7 days. Patients could use a sling to relieve pain during the first few days. Early active movements within the limits of pain were started after 2 days, according to a predefined protocol. In the plaster group, the elbow was immobilised for 3 weeks in full above elbow cast. After removal of the plaster, physical therapy was initiated according to a standardised protocol. The QDASH was significantly better in the early mobilisation group at 6 weeks, although there was no significant difference at other time points. Patients reported significantly more pain at 1 week in the early mobilisation group, although analgesic use was the same. The flexion–extension arc was significantly better in the early mobilisation group at 6 weeks only. There was no significant difference in the radiographic presence of heterotopic ossification, although there were only three grade 3 ossifications and these all occurred in the plaster immobilisation group. Complications and secondary interventions were similar in both treatment groups. No residual instability, subluxation or secondary dislocations were found. The early mobilisation group also returned to work sooner (median 10 days versus 18 days).
Rafai et al. 55 reported on 50 patients randomised to early mobilisation or plaster immobilisation for three weeks. In the early mobilisation group, functional therapy was begun on day 3. At the 12-month follow-up, there was an extension deficit in 4% of the early mobilisation patients versus 19% in the immobilisation group.
Surgical management
The role of surgical management of acute elbow dislocations is controversial. Based on the literature presented, surgery is required in less than 10% of individuals, who will otherwise go on to develop chronic instability.3,4 Modi et al.
3
reported that 2.3% of patients went on to require stabilisation surgery (most within the first year after injury). The degree of instability is dependent on the extent of the soft tissue injury, particularly the loss of secondary dynamic stabilisers. Therefore, in the practice of the senior author (ACW), the decision to perform an acute repair is based on MRI and/or fluoroscopic stress examination (EUA) of the elbow. Surgery is indicated if there is significant lateral joint line gapping or disruption of the common extensor origin (Fig. 4) or if EUA reveals moderate or gross instability.
49
The aim of surgery is to downgrade the level of injury (to bring the patient down the injury ladder) (Fig. 3). Acute repair can be performed open or arthroscopically with a suture anchor to secure the lateral ligament and common extensor origin. Open medial stabilisation is only undertaken if instability persists after the lateral structures have been addressed.
Magnetic resonance imaging of a posterolateral dislocation after reduction showing a high-grade injury with disruption of all medial (large black arrow common flexor origin and small black arrow medial collateral ligament) and lateral (white arrow) structures. Note the soft tissue injury is more extensive on the medial side of the elbow.
Josefsson et al. carried out two studies; a retrospective cohort study 56 and a randomised trial comparing surgical and nonsurgical treatment of ligamentous injuries after simple elbow dislocation. 35 At more than 12-months follow-up, there was no statistically significant difference between the two groups in terms of elbow range of movement in either study. Both groups had extension deficits, with almost full flexion, full supination and pronation. There was no subjective instability or re-dislocation. These studies aimed to address an important question, although no stratification of the severity of the soft tissue injury was performed. The value of early surgery for those with high-grade injuries may be diluted by the larger number of lower grade lesions in which surgical stabilisation is not required.
Rehabilitation
Overhead rehabilitation protocols for the elbow have been described in recent years. Schreiber et al. 57 reported the results of one such protocol, beginning within 1 week of simple elbow dislocation. The decision for nonsurgical management was based on imaging, injury pattern and stability. Range of motion exercises were performed in a safe overhead position that maintains stability at the same time as allowing motion. Exercises were performed in a supine position with the shoulder flexed to 90°, adducted and in neutral rotation. This position minimises the effect of gravity, decreases posteriorly directed forces and allows the triceps to function as an elbow stabiliser. 58 By avoiding abduction and internal rotation, the gravitational varus and extension-distraction force is eliminated, thereby allowing the lateral collateral ligament to heal in an isometric position. Two exercises were performed: active-assisted forearm pronation and supination and active and active assisted elbow flexion without limits and elbow extension tailored to the instability of the injury. The limits of motion were determined by patient tolerance.
Commencement of motion in an upright position depended on joint congruency seen on the lateral extension radiograph. There were no recurrent dislocations or clinical instability.
Ross et al. 59 also described a successful immediate motion protocol after simple elbow dislocation, without the use of slings or splints. The protocol was more complex than that described by Schreiber et al. 57 involving the use of underwater electrical stimulation, cryotherapy and compression wrapping of the arm. It is not clear whether overhead rehabilitation was used. There are no randomised trials that demonstrate a superior outcome using overhead rehabilitation protocols.
Long-term outcomes of nonsurgical treatment
The long-term functional outcomes of conservatively treated simple elbow dislocations are generally reported as being favourable. In their retrospective long-term outcome study, Josefsson et al. 2 followed up patients at an average of 24 years (range 15 years to 38 years) after simple elbow dislocation. There was no recurrent dislocation and no instability, despite eight elbows demonstrating valgus instability upon testing. One patient is described who had gross valgus instability with a 30° flexion contracture who was forced to change occupation because of the elbow. Only two had pain at rest and three had pain at work. By far the most common finding was a decrease in the range of movement. Similarly, Borris et al. 60 reported on the long-term outcomes of 35 conservatively treated simple elbow dislocations in adults at a median of 8 years (range 2 years to 19 years). 60 All were treated with closed reduction and immobilisation in an above elbow splint for a median of 22 days (range 10 days to 42 days). There were no re-dislocations. Fifteen patients complained of pain in the elbow.
Anakwe et al. 4 reported a less favourable outcome of simple elbow dislocations in 110 patients at a mean follow-up of 88 months. Eighty-five percent of the cohort was immobilised for between 1 week and 3 weeks. The mean DASH was 6.7 and the mean Oxford Elbow Score was 90.3. Eight percent had objective elbow instability and 8% reported subjective instability. Fifty-six percent reported stiffness and 62% reported pain. Of 54 who participated in sports, 19% had either given up or had to modify their technique because of their elbow. Reduced elbow flexion independently predicted a poor DASH and Oxford Elbow Score. There were no recurrent dislocations, although two patients required ligament reconstruction for instability. These findings are supported by Mehlhoff et al., 9 who reported that 60% of 52 simple elbow dislocations complained of symptoms from the elbow at an average follow-up of 34 months (range 12 months to 84 months). 9
Eygendaal et al. 46 evaluated 41 patients at a mean of 9 years. 46 Twenty-four had evidence of medial instability on stress radiographs and this correlated with a worse HSS score, degeneration and persistent pain.
Conclusions
Simple elbow dislocations occur most commonly in males in their second decade. In most cases, hyperextension and valgus forces cause a posterolateral dislocation with a spectrum of soft tissue injury to medial-sided structures in all cases and lateral stabilisers in some. Injury to the musculotendinous secondary stabilisers determines whether a simple dislocation is stable or not after reduction and therefore it is the opinion of the senior author (ACW) that MRI can identify those that may require surgical intervention. It is also the practice of the the senior author (ACW) to screen under anaesthesia all elbows that have injury extending to the lateral structures and to acutely repair those with gross or moderate instability (>10° angulation on stress testing) to permit early mobilisation in the supine position in an attempt to avoid long-term instability or stiffness. It is acknowledged that this is not the practice of most elbow specialists and this represents a new way of thinking about these injuries. Prospective studies are required to investigate whether there is a role for early surgery in a minority of simple elbow dislocations with high-grade soft tissue injuries to prevent recurrent instability or stiffness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The paper has not been presented at any society or meeting.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical review and patient consent
Ethical review was not required. Patient consent was not required.