
Abstract
Background
Cerclage wire is the current standard for circumferential bone fixation. Advances in technology have improved modern sutures, allowing for expanded utility and broader application. The present study compared the strength and durability of cerclage fixation between modern suture materials and monofilament wire.
Methods
The Surgeon’s Knot, the Nice Knot and the Modified Nice Knot, were each tied using three separate suture materials: no. 2 FiberWire (Arthrex, Naples, FL, USA), no. 2 Ultrabraid (Smith & Nephew, Andover, MA, USA) and no. 5 Ethibond (Johnson & Johnson, Somerville, NJ, USA). These sutures were compared with monofilament wire. Sutures were secured around a fixed diameter using three additional half hitches, whereas a 1.2-mm (18 gauge) stainless steel monofilament wire was used for comparison. One fellow and one orthopaedic surgery resident each tied five trials with every knot/material combination. Samples were subjected to cyclic loading and quasi-static load testing. Respectively, cyclic displacement over time and load to failure were analyzed. Clinical failure (3 mm of cyclic displacement) and absolute failure (opening of the knot or material failure) were the outcomes of interest.
Results
During cyclic loading, Ethibond displaced significantly less over time compared to monofilament wire (p < 0.003), whereas FiberWire showed no significant difference. Ultrabraid also behaved similar to wire, except displacing significantly more than wire only with the Surgeon’s Knot (p = 0.02). During load to failure, Ethibond and FiberWire failed at significantly greater loads than monofilament wire (p < 0.001), whereas Ultrabraid performed similar to wire. Knot types did not appear to impact the results.
Conclusions
High-performance sutures achieve superior results in biomechanical testing under cyclic and quasi-static load compared to monofilament wire, suggesting that they provide an alternative to wire for cerclage fixation with select clinical application. Biomechanical security of suture cerclage is dependent on suture material, although it is not altered significantly by choice of knot. An ex-vivo study with clinical application would further reinforce whether suture cerclage offers a valid alternative to wire cerclage.
Introduction
Cerclage fixation, an orthopaedic technique for circumferential bone fixation, is beneficial when used independently or for augmentation when screw fixation cannot be used, or is undesirable. Monofilament wire has been widely used for cerclage fixation and is still standard practice. Stainless steel wire is typically preferred for its strength, affordability and the fact that it is readily available. 1 Cerclage fixation is commonly employed when repairing sub-trochanteric fractures, 2 or for management of peri-prosthetic fractures during total hip or shoulder arthroplasty. 3
However, wire cerclage causes radiographic interference, 4 and can fracture due to low cyclic fatigue. Wire fracture causes metallosis, and patient outcomes can be negatively affected if fragments migrate or a non-union occurs. At larger gauges, wire is stiffer and more difficult to use. 1 Wire also poses a risk to the operative team because sharply cut ends may perforate surgical gloves and cause puncture wounds.
Modern suture materials have become more refined and robust4,5 with increased tensile strength. Sutures are widely available, cost effective and easy to use. Furthermore, they pose no risk of metallosis and create no radiographic interference; therefore, sutures are now being used for cerclage fixation when a wire may have been previously chosen. Multiple studies have examined the best knot types and tying techniques. The Nice Knot is a double stranded knot that outperformed other commonly used knots (e.g. Surgeon’s Knot) demonstrating adequate biomechanical characteristics for clinical use. 6 A recent modification to the Nice Knot has been proposed, altering the locking tie in attempt to make the Nice Knot even more secure. This Modified Nice Knot has never been tested under standard experimental conditions.
The primary purpose of the present study was to compare the biomechanical properties of modern suture materials as a potential alternative to monofilament wire with regard to cerclage fixation. Secondarily, we compared the security of the Modified Nice Knot with two previously proven surgical knots: The Nice Knot and the Surgeon’s Knot.
Materials and methods
The biomechanical properties of three suture materials, tied using three varying surgical knots, were tested against those of monofilament wire. Suture materials and knots for the study were selected based on availability and common use. The suture materials consisted of no. 5 Ethibond (Johnson & Johnson, Somerville, NJ, USA), no. 2 FiberWire (Arthrex, Naples, FL, USA) and no. 2 Ultrabraid (Smith & Nephew, Andover, MA, USA). Ethibond is comprised of a braided high molecular weight polyester fibre with plastic polymer coating. FiberWire is composed of an ultra high molecular weight polyethylene (UHMWPE) central core with a braided polyester coat. Ultrabraid is made with braided UHMWPE fibres but without a central core. All suture materials were non-absorbable. Each suture material was tied using a standard Surgeon’s Knot, as well as the Nice Knot and a Modified Nice Knot (Fig. 1).
Surgical knots: (a) Surgeon’s Knot; (b) Nice Knot; and (c) Modified Nice Knot.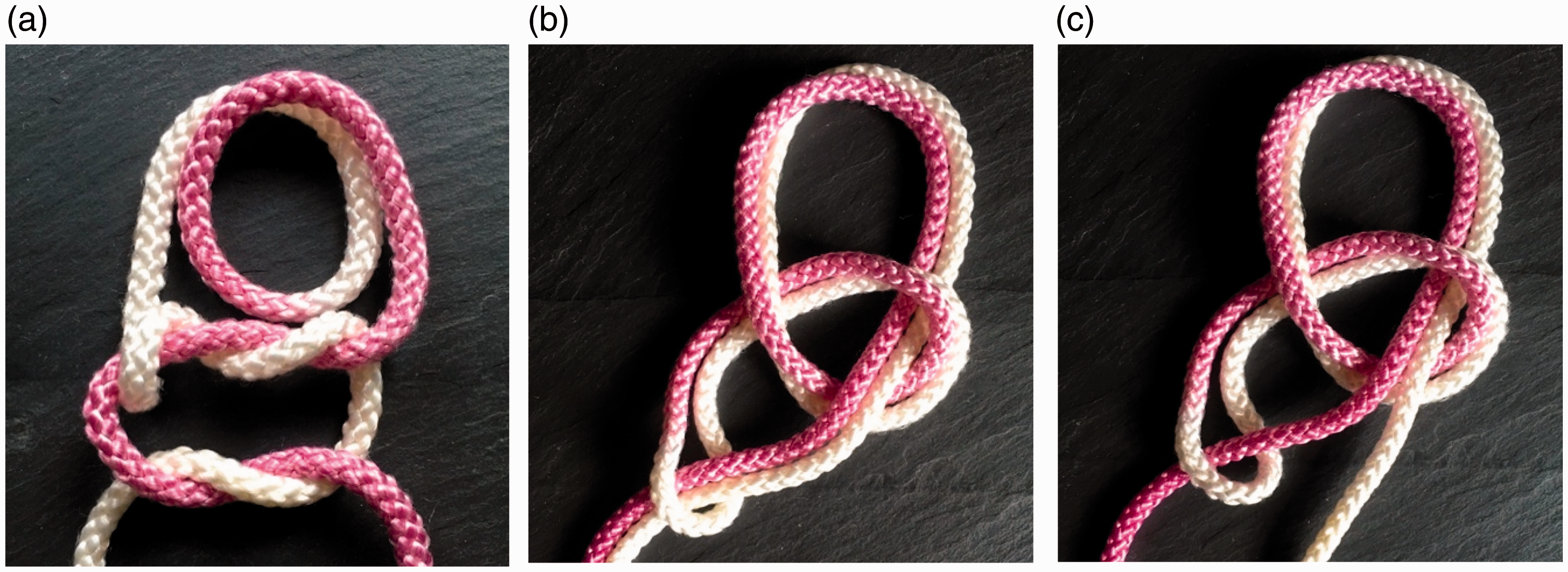
The Modified Nice Knot differs from the Nice Knot in its locking throw. To secure all knots, three additional half hitches (Fig. 2) tied on alternating posts were chosen because knot security plateaus with greater than three half hitches.6,7 Because the Nice Knots are double stranded, the Surgeon’s Knots were double thrown to ensure equal load distribution. A standard 1.2-mm (18 gauge) stainless steel monofilament wire (Fig. 3) was used for comparison.
Suture cerclage loops complete with three additional half hitch throws: (a) Ultrabraid; (b) Ethibond; and (c) FiberWire. Monofilament stainless steel wire cerclage.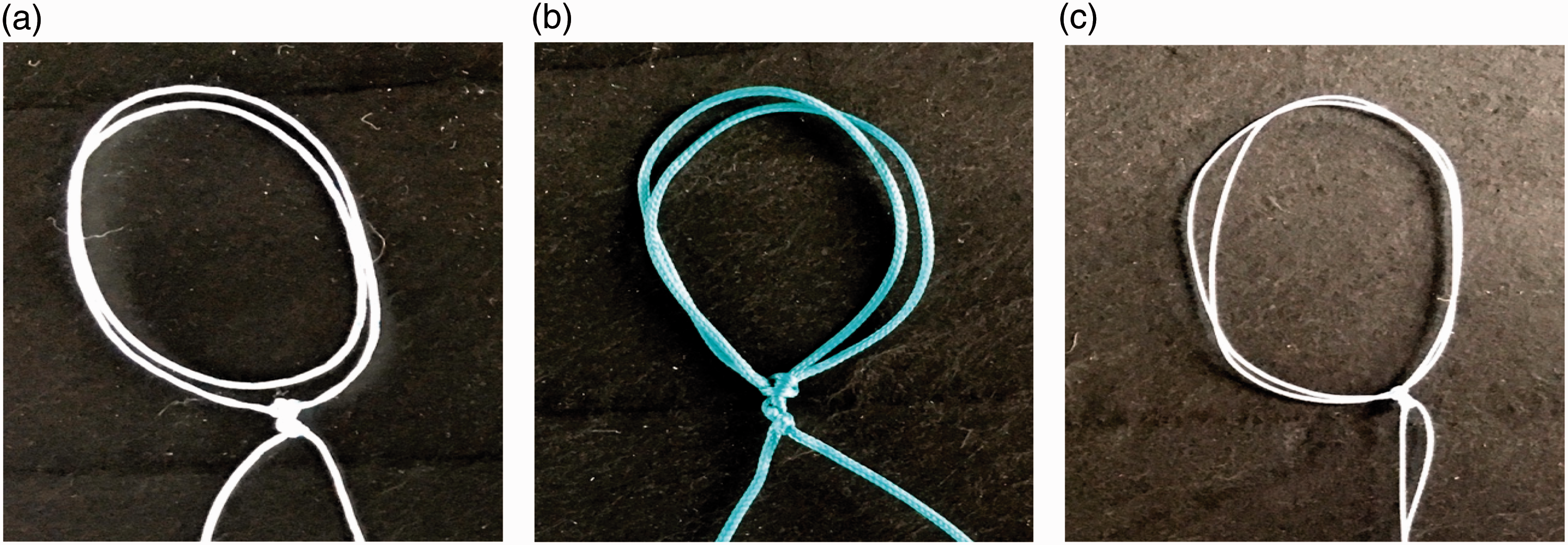

The wire and all sutures were fastened around a solid, cylindrical piece of finished wood with a fixed 90-mm circumference to establish consistency in cerclage loop size. The cerclage wires were twisted until taut, applying in-line tension to obtain equal involvement of both ends, which is typical of the technique used in the operating theatre. An orthopaedic fellow and a second year orthopaedic resident each fastened five suture cerclages with every variation of knot and suture material, as well as five wire cerclages. Completed samples were removed from the cylinder to be loaded for testing.
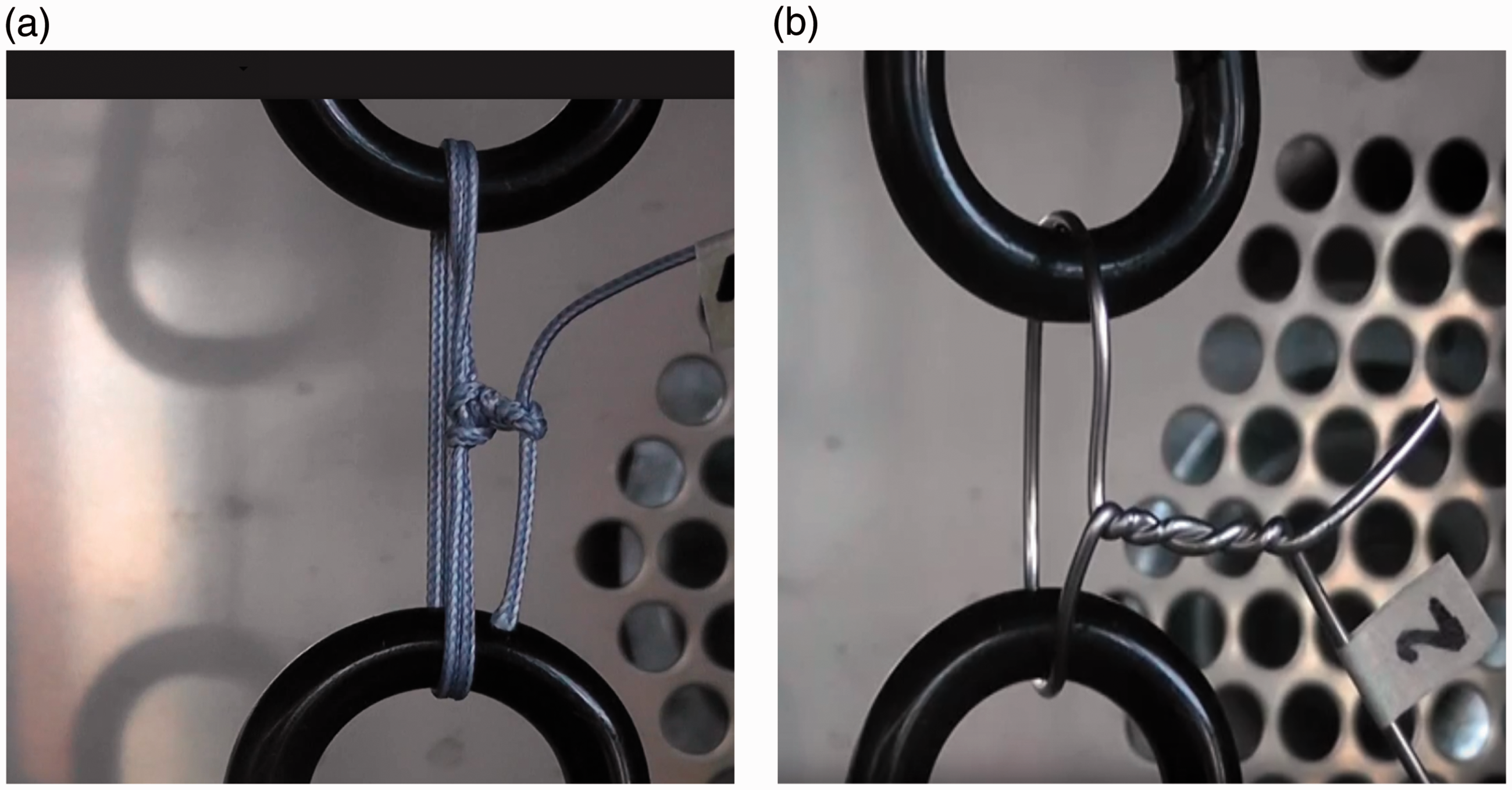
Two phases of testing were conducted using an ElectroForce 3200 test instrument, manufactured by Bose Corp. (Framingham, MA, USA) (Fig. 4). This machine is equipped with a 450-N load cell, a motor capable of applying dynamic tension and compression with frequencies that can reach 100 Hz, and a displacement transducer capable of 0.03 mm (or 0.5%) calibrated accuracy within its 6.5-mm measurement range. Two high strength carabiners were secured to the instrument’s tension grips and each sample was then hooked around the carabiners (Fig. 5) such that the tensile load would act to circumferentially expand the specimen. During Phase One, we subjected samples to cyclic load, to test displacement over time. Similar to previous study techniques, samples were pre-tensioned to 10 N and cycled between 10 N and 45 N, at a frequency of 1.8 Hz.5,8,9–11 Cyclic displacement over time was measured using the displacement transducer as samples were subjected to 1000 cycles. This number was chosen to represent the average number of cycles a repair may experience in the first 6 weeks of postoperative healing time.
10
Phase Two testing assessed load to failure through quasi-static tensile loading at a rate of 1 mm/s to a maximum load of 320 N. Failure was defined as either clinical or absolute failure. Clinical failure, marked by ≥ 3 mm of cyclic displacement (after pre-tensioning) and absolute failure, via opening of a cerclage or material failure, were used as determinants. Previous studies6–8 selected 3 mm of displacement to represent clinical failure, although the clinical relevance of this measurement is unverified.
Bose ElectroForce 3200 Test Instrument. Cerclage samples mounted to carabiners for testing: (a) FiberWire Nice Knot and (b) Monofilament stainless steel wire.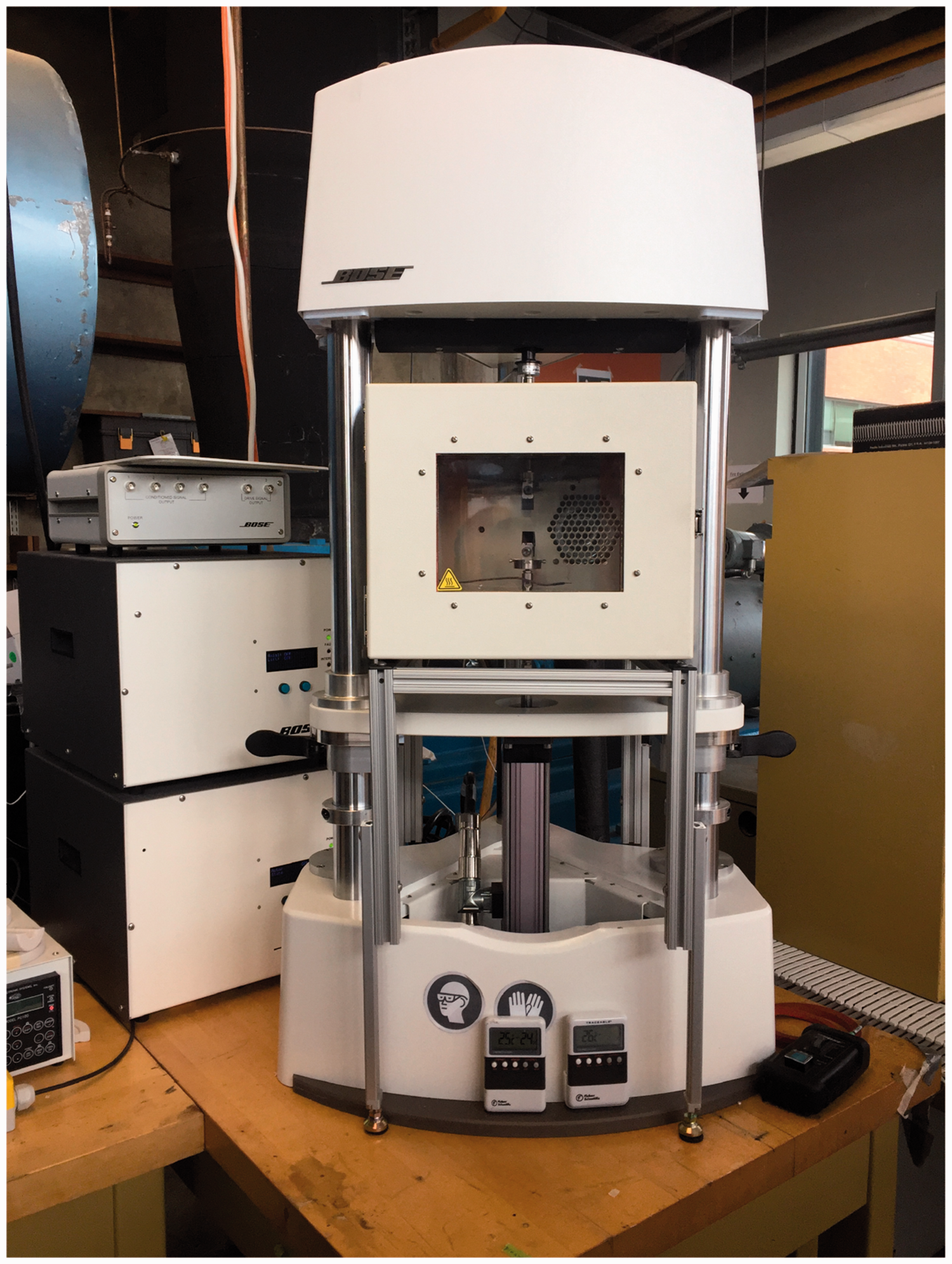
In Phase One, displacement was measured as the slope of cyclic displacement over time, with an inverse relationship regarding stability: a smaller slope (less displacement with time), indicating greater stability. Load to failure during Phase Two was determined as the force (N) at which materials experienced failure. The most durable samples were able to resist greater forces, thus experiencing failure at higher loads. With the instrument tension grips and carabiners both orders of magnitude stiffer than the knots, the displacement transducer was used to measure each sample’s opening displacement. A video showing one of the samples being tested can be found on YouTube (https://youtu.be/spVQvaEG87k). WinTest software (TA Instruments, New Castle, DE, USA) was used to program the machine for both phases of testing and to extract the applied forces and resulting displacements. Frequencies (mean and standard deviation) were recorded and displayed graphically for all data points. These results were then exported into Excel (Microsoft Corp., Redmond, WA, USA) for processing. One-way analysis of variance (ANOVA) was performed to compare suture material and knot type using SPSS, version 22.0 (IBM Corp., Armonk, NY, USA) with Bonferroni post-hoc testing. Because there is no ‘knot type’ for wire cerclage, we created a composite variable of knot type and material and compared 11 groups of 10 subjects using one-way ANOVA. p ≤ 0.05 was considered statistically significant.
Results
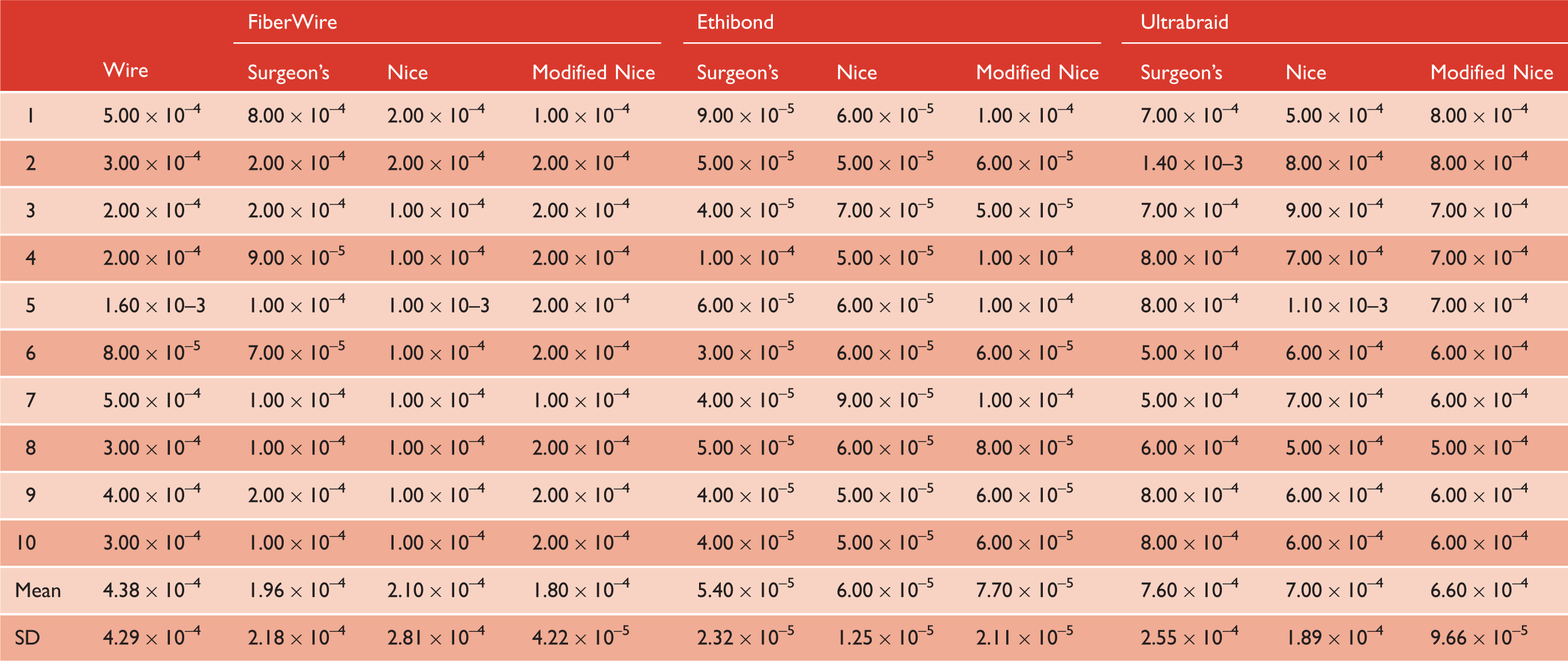
During Phase One cyclic loading (Fig. 6), no. 5 Ethibond was the most durable, with significantly less cyclic displacement over time when compared to monofilament wire (p < 0.01). The results were not significant for no. 2 FiberWire when compared to cerclage wire with regard to cyclic displacement (p > 0.23). No. 2 Ultrabraid had the weakest performance under cyclic load. Although it was not significantly worse than wire with the Modified Nice Knot (p = 0.74) or the Nice Knot (p = 0.20), it demonstrated significantly more displacement than cerclage wire for the Surgeon’s Knot (p = 0.02). No significant differences were seen with knot type when using Ethibond or Fiberwire (p = 1.00). The pattern of results was similar between the fellow and the resident during cyclic loading (p = 0.72). Although only one cerclage wire experienced clinical failure during cyclic loading (Table 1), no materials experienced absolute failure; thus, all were subsequently exposed to Phase Two load to failure testing.
Cyclic loading. Phase One: cyclic displacement over time (mm/s).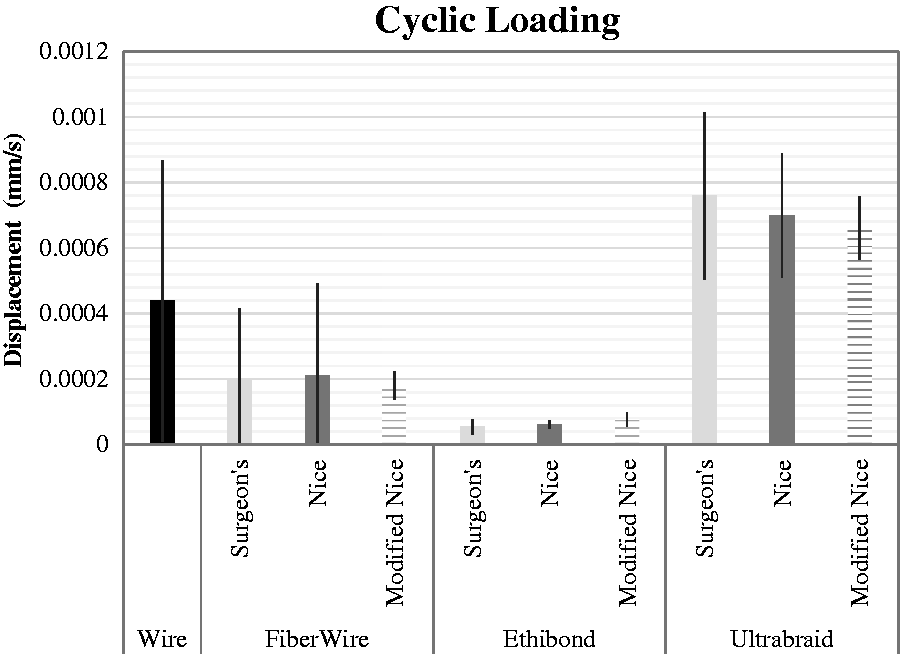
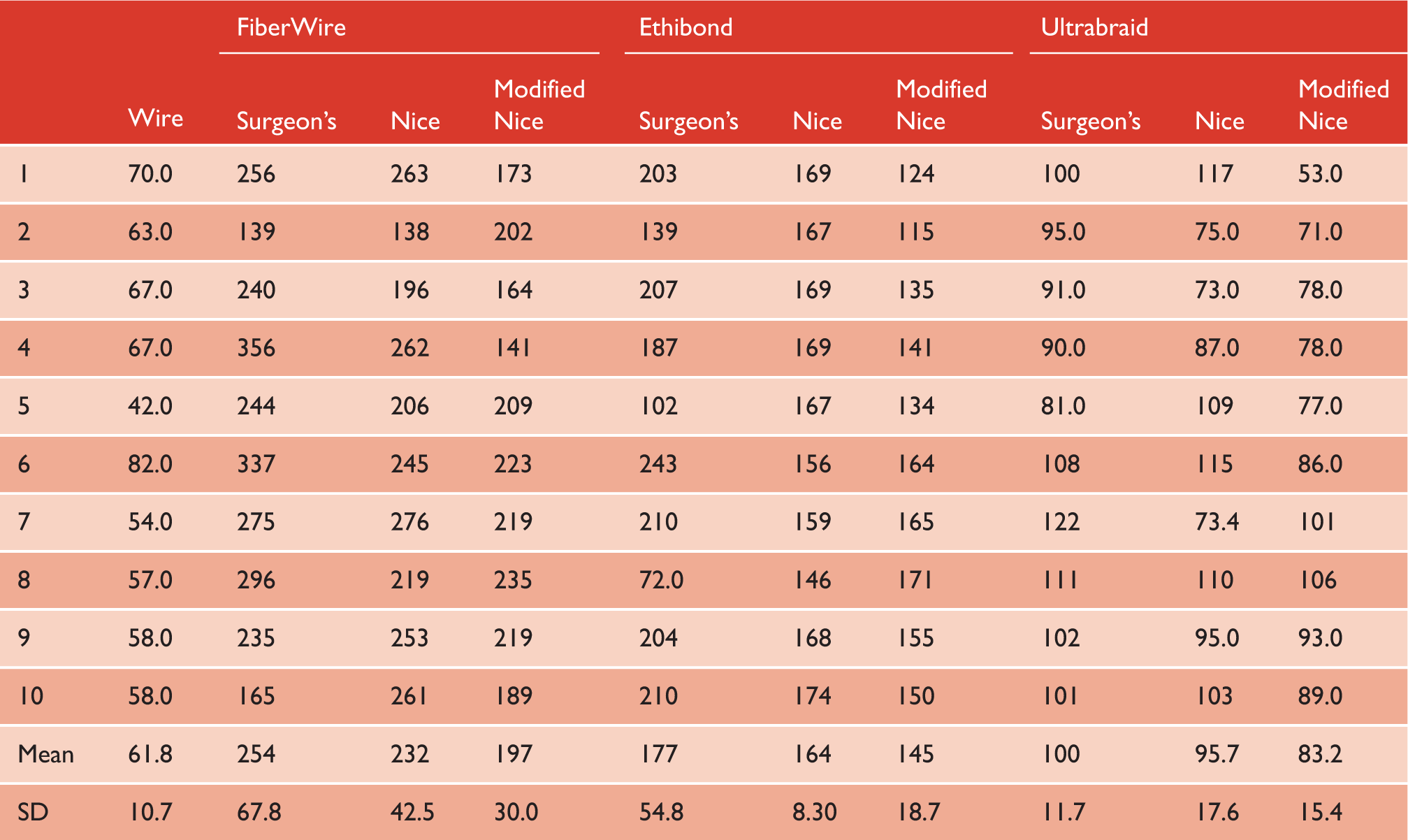
For load to failure (Fig. 7), both the no. 2 FiberWire and the no. 5 Ethibond withstood significantly higher tensile loads than monofilament wire (p < 0.01). No. 2 Ultrabraid did not fail at greater loads than cerclage wire with any statistical significance (p > 0.95). Again, no significant differences were seen in the pattern of results between the fellow and the resident during load to failure testing (p = 0.86).
Load to failure.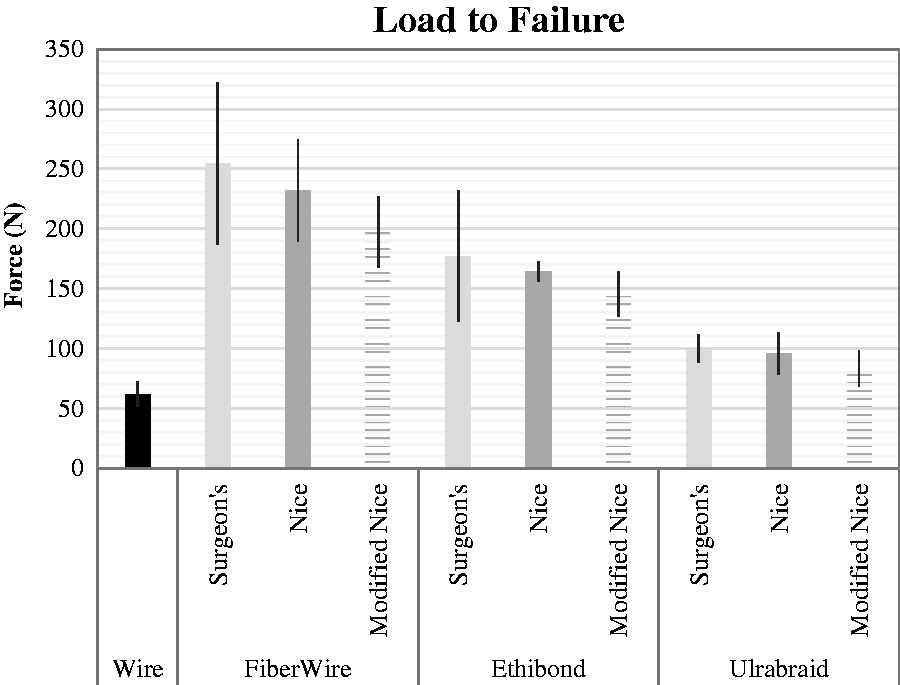
Phase Two: load to failure (N).
Discussion
Substituting suture for monofilament wire is a relatively newer concept, bolstered by the clinical successes of UHMWPE suture materials. We found that certain suture materials were superior to monofilament wire for cerclage fixation with regard to cyclic displacement over time and load to failure under cyclic and quasi-static loading, respectively. Additionally, the choice of surgical knot had no significant impact on the strength of our cerclage constructs.
In 2008, Kuruvalli et al. 12 produced unions in all of 20 extensile trochanteric osteotomy cases fixed using woven suture, trialing this technique aiming to avoid vascular interruption (theoretically caused by wire or cable cerclage), to decrease risk associated with passing wire (sciatic nerve injury and fragment migration following fixation failure), to decrease cost and to improve ease of application. In a 2011 study, Flanigan et al. 13 examined the biomechanical properties of FiberWire compared to monofilament wire as augments in bovine patellar tendon repair and found the two equivalent in maintenance of reduction of the repairs. In 2002, Rothaug et al. 1 compared tensile strength, fatigue strength and maintenance of reduction between polyethylene sutures and stainless-steel wire for in-vitro fixation of equine sesamoids (analogous to the human patella) and found sutures to be superior in all categories. In 2014, Renner et al. 4 tested no. 5 FiberWire suture cerclage alongside 1.25-mm stainless steel cerclage for resisting subsidence of shoulder arthroplasty stems in cadaveric humeri. The cerclage wire had greater tightening force for reducing a fracture gap, whereas there was no difference in the stabilization of a nondisplaced periprosthetic fracture. Renner et al. 4 did not test for cyclic displacement over time by subjecting their cerclage samples to cyclic loading. The present study found that certain suture materials were displaced less and failed at greater loads than cerclage wire, when subjected to cyclic loading and load to failure testing, respectively.
With continual advancement in synthetic suture constructs, clinical researchers have directed much effort to comparing the performance of various suture materials. In 2006, Mahar et al. 5 compared the performance of Ethibond to Force Fiber (similar to FiberWire) under cyclic load, using several different knot types. Force Fiber sustained greater failure loads, regardless of knot type. 5 In 2007, Mahar et al. 11 consistently found FiberWire to be significantly stronger than Ethibond, again concluding that knot type had negligible impact on results. A large biomechanical study from 2008 compared several knots and suture materials for displacement and load to failure. FiberWire and other UHMWPE sutures sustained significantly higher loads at failure than braided polyester sutures, such as Ethibond, among others, including Ultrabraid. 8 FiberWire has repeatedly sustained greater failure loads compared with other suture materials, which was also reflected in our results. The strength of this suture material is likely attributed to the core structure designed with large numbers of filaments that help decrease the variation in force required to induce failure. 14 It is noted that UHMWPE sutures are more likely to displace than braided polyester sutures, emphasizing the need for locking throws and highlighting the fact that material should be chosen carefully for its clinical requirement.
The idea that suture materials have more significant impact for overall strength than choice of knot was further enforced in 2013 by Baums et al. 10 when they compared several open versus arthroscopic tying techniques using various materials, concluding that no specific knot type significantly outperformed another under cyclic load. However, a 2016 study reported that the Nice Knot was significantly superior to the Surgeon’s Knot with respect to both load to failure and resisting displacement. 6 One possible reason for the opposing observation in the present study is that our Surgeon’s Knot was doubled up. Therefore, the knot was tied using only two strands instead of four, as with the Nice and Modified Nice knots. Although not improving upon the Nice Knot, the present study identified the Modified Nice Knot as comparable to both the Nice Knot and the Surgeon’s Knot. Each surgical knot exhibits different characteristics, with surgeon-specific selection routinely based on comfort and required utility, rather than clinical performance.15,16 Emphasis must be continually directed toward diligent testing of knot properties and their role in postoperative healing. 10
The design of the present study closely resembles those of previous biomechanical knot analyses; however, there are some limitations. Although we tested variable knot types and suture materials, we only tested one wire size and the use of a staircase loading protocol was not implemented. Furthermore, although we replicated an intra-operative technique, we did not standardize the number of twists for each wire cerclage. We did not perform in-vivo clinical comparison of wire or suture application, nor did we simulate ex-vivo conditions with cadaveric bone. Neither body temperature, nor aqueous environment were used to reproduce the in-vivo conditions to which these materials would be exposed. The impact of these limitations on our study parameters is unknown. We also did not assess cerclage materials for wear resistance. This may be of no consequence for intra-operative fissure type fractures in primary arthroplasty, although sharp bone fragments in some fracture patterns could affect suture cerclage. Finally, the present study did not account for cabling, another modern cerclage technique worth evaluating alongside wire and suture cerclage.
Future studies comparing biomechanical properties between cable, monofilament stainless steel wire and UHMWPE sutures under ex-vivo conditions closely simulating clinical parameters may yield valuable data regarding the clinical application of these various cerclage materials. With new materials being produced faster than the evidence to support them, testing these materials with our knots and tying techniques remains essential.
Conclusions
High-performance suture materials common to current clinical practice experienced less displacement with time and failed at greater loads when compared to monofilament wire in biomechanical tests of cyclic load and quasi-static load to failure. These results suggest that some suture materials may provide a superior alternative to wire for cerclage fixation techniques with select clinical application. Determining which surgical knot to use is less critical than the selection of a suture material when considering the integrity of cerclage fixation. As new surgical techniques and materials become available, it is pertinent that comparative testing be performed to provide evidence-based best practice guidelines.
Footnotes
Acknowledgements
Dr Lauren Beaupre (Division of Orthopaedic Surgery) for help with statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical review and patient consent
Not required for this article.