
Abstract
Background
Minimal information exists regarding the sub-supraspinatus recess superior to the labrum and inferior to the supraspinatus. Furthermore, movement of the superior labrum during glenohumeral range of motion has not previously been defined. The objectives of this arthroscopic study were to describe the (i) sub-supraspinatus recess dimensions and (ii) superior labral motion.
Methods
Forty-four patients were enrolled and underwent standardized arthroscopic assessment. Analysis consisted of static measurement of the sub-supraspinatus recess depth, as well as the amount of labral motion during passive shoulder motion. Labral movement was categorized relative to the glenoid rim (lateral to the rim, to the rim, or medial to the rim).
Results
All patients had a well-defined sub-supraspinatus recess varying from a depth of 0 mm to 5 mm (n = 10; 22.7%), 5 mm to 10 mm (n = 23; 52.3%) or >10 mm (n = 11; 25%). External rotation in abduction demonstrated the greatest labral movement (p < 0.001) with 28 (80%) shoulders moving medial to the rim.
Conclusions
The sub-supraspinatus recess is consistently present with an average depth of 5 mm to 10 mm. Superior labral motion is present in most patients and is most pronounced in external rotation in abduction. This finding likely has clinical implications for superior labral repair surgery, especially for overhead athletes and laborers who require external rotation in an abducted position for a successful outcome.
Keywords
Introduction
Superior labral anatomy has been well described, with the attachment of the superior labrum to the glenoid being highly variable.1–3 Pathology of the superior labrum has also been well characterized with ten different types of SLAP (Superior Labrum Anterior and Posterior) lesions being identified.4,5 The entity of ‘peel back’ of the superior labrum has been suggested as a pathological motion that predisposes to a SLAP tear. This is particularly pertinent in throwing athletes who frequently enter the arm position associated with peel back – abduction and external rotation. However, we hypothesize that the superior labrum is normally a very mobile structure leading to some nonpathological ‘roll back’.
Shoulder stiffness after superior labral repair is common.6–9 This may occur as a result of tethering the superior labrum, inhibiting the normal roll back of the superior labrum and, in essence, restricting the normal excursion of the supraspinatus tendon, which lies directly above the repair. Boileau et al. 6 noted severe scarring after SLAP repair and has recommended biceps tenodesis rather than SLAP repair in all patients including overhead athletes.
Superior to the posterosuperior labrum is a synovial recess, which is adjacent to the undersurface of the rotator cuff. Unlike the glenoid attachment of the superior labrum, this area has been poorly characterized. Alterations in the anatomy of this region following superior labral repair may contribute to postoperative stiffness. Currently, a sub-labral foramen less than 5 mm is considered normal with any larger foramen being considered pathological. These two recesses together may provide the necessary tissue capacity for normal excursion of the supraspinatus muscle. Reducing the size of either of these recesses (i.e. as may occur with a SLAP repair) may act as a tether on supraspinatus muscle excursion, thereby limiting shoulder range of motion. To date, there has been no formal description of the sub-supraspinatus recess to our knowledge.
The purpose of the present study was to (i) describe the depth of the sub-supraspinatus recess (i.e. the area between the superior labrum and the undersurface of the rotator cuff) and (ii) assess the superior labral motion during different patterns of shoulder motion. We hypothesized that there would be variability in the sub-supraspinatus recess depth and also that superior labral motion would occur during normal glenohumeral motion.
Materials and Methods
Subjects
Patients aged under 65 years who were undergoing shoulder arthroscopy, with a normal superior labrum (no tear present), and no full-thickness or high-grade partial thickness rotator cuff tear evident, were recruited for the present study by four fellowship trained shoulder surgeons. Patients were included if they provided their written informed consent for a video to be made of their superior labral anatomy and to allow access to their operative report. Patients with significant long head of the biceps tendon pathology, as well as extensive synovitis within the shoulder joint that could obscure the view of the superior labrum and sub-supraspinatus recess, were excluded.
Procedures
A standardized arthroscopic technique with patients positioned in the beach chair position was used for all subjects. The surgical limb did not have any constricting bandages placed above the elbow to prevent tethering or restriction of the biceps. The arm was positioned in 30° of flexion, 30° of abduction and neutral rotation using an articulated pneumatic arm holder. In-line traction was minimized to recreate a resting position of the shoulder. Pump pressure was held at 30 mmHg for all assessments. Diagnostic arthroscopy was performed to document intra-articular pathology and a subjective assessment of the labral attachment was made. The measuring instrument was used to determine the depths (in mm) of the sub-labral foramen and sub-supraspinatus recess at three separate locations starting superior at the biceps and moving posterior at the 12, 11 and 10 o’clock positions.
An intra-operative video was recorded prior to any shoulder repair using a standardized approach and patient positioning. Video 1 documented static measurement of the depth of the sub-supraspinatus recess with a graduated probe. Videos 2 to 5 were dynamic assessments of superior labral motion during four shoulder movements: (i) external rotation in an adducted position; (ii) scaption with the elbow bent ninety degrees; (iii) scaption with the elbow fully extended; and (iv) 90° external rotation in an abducted position. For dynamic assessments, the arm was removed from the pneumatic holder and taken through each range of motion without traction.
Analysis of these data was performed at a later date by two blinded observers (two fellowship trained shoulder surgeons) who were unaware of the arm position. Consensus was achieved by the observers for the measurements. Sub-supraspinatus recess depth was categorized as being 0 mm to 5 mm, 5 mm to 10 mm or 10 mm to 15 mm in depth. Motion of the superior labrum was quantified using a four-point grading system determining maximum displacement and position reached by the labrum relative to the superior glenoid rim. The four points of maximum displacement were: 0, no movement of the labrum; 1, the labrum moving medially from its starting point but remaining lateral to the superior glenoid rim; 2, the labrum moving medially from its starting point to the level of the superior glenoid rim or 3, the labrum rolling medial to the superior glenoid rim.
Statistical analysis
Descriptive statistics (mean, SD, frequency, proportion) were calculated for all variables. In addition, analysis of variance was used to compare the degree of labral movement among the four shoulder movements. Statistical analysis was performed with PASW, version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics.
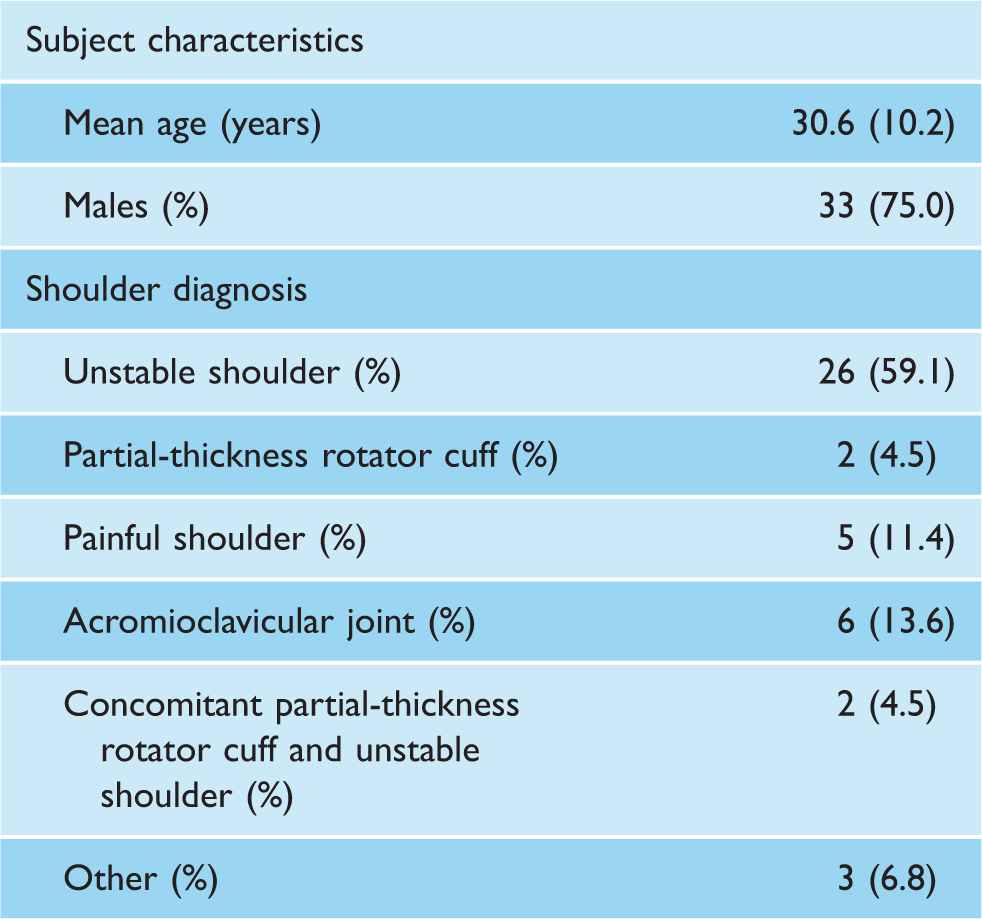
Data are the mean (SD).
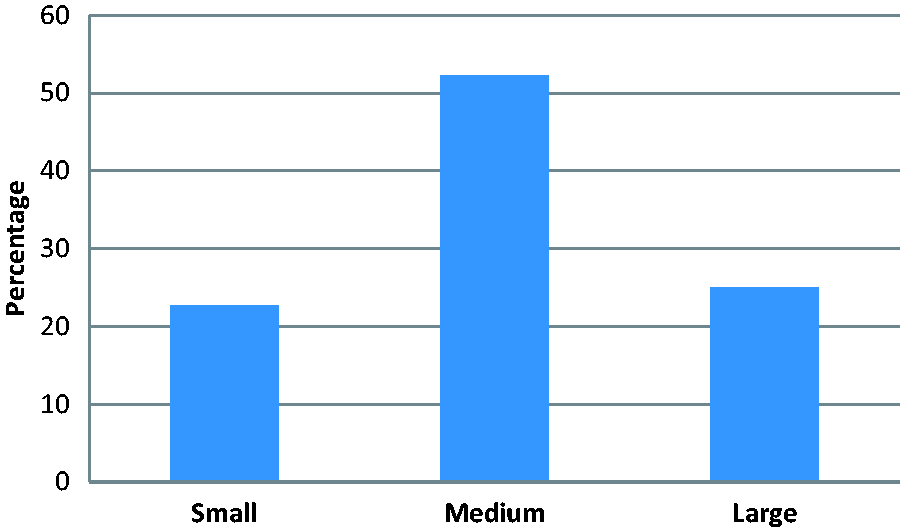
Sub-supraspinatus recess (small: <5 mm, medium: 5 mm to 10 mm and large: >10 mm).
Labral motion was seen in 42 (95.5%) subjects in external rotation, 43 (97.7%) subjects in scaption with the elbow bent and 42 (95.5%) subjects in scaption with the elbow straight (Fig. 2). The distribution of labral motion was similar in these groups, with most of the motion being lateral to or to the level of the superior glenoid rim. External rotation in abduction had the most labral motion of all four movements (p < 0.001); All subjects demonstrated labral motion and 35 (79.5%) subjects exhibited roll back of the superior labrum medial to the glenoid rim (Fig. 2). There was no relationship between the size of the sub-supraspinatus recess and the amount of labral motion in any plane.
Movement position versus movement pattern cross-tabulation.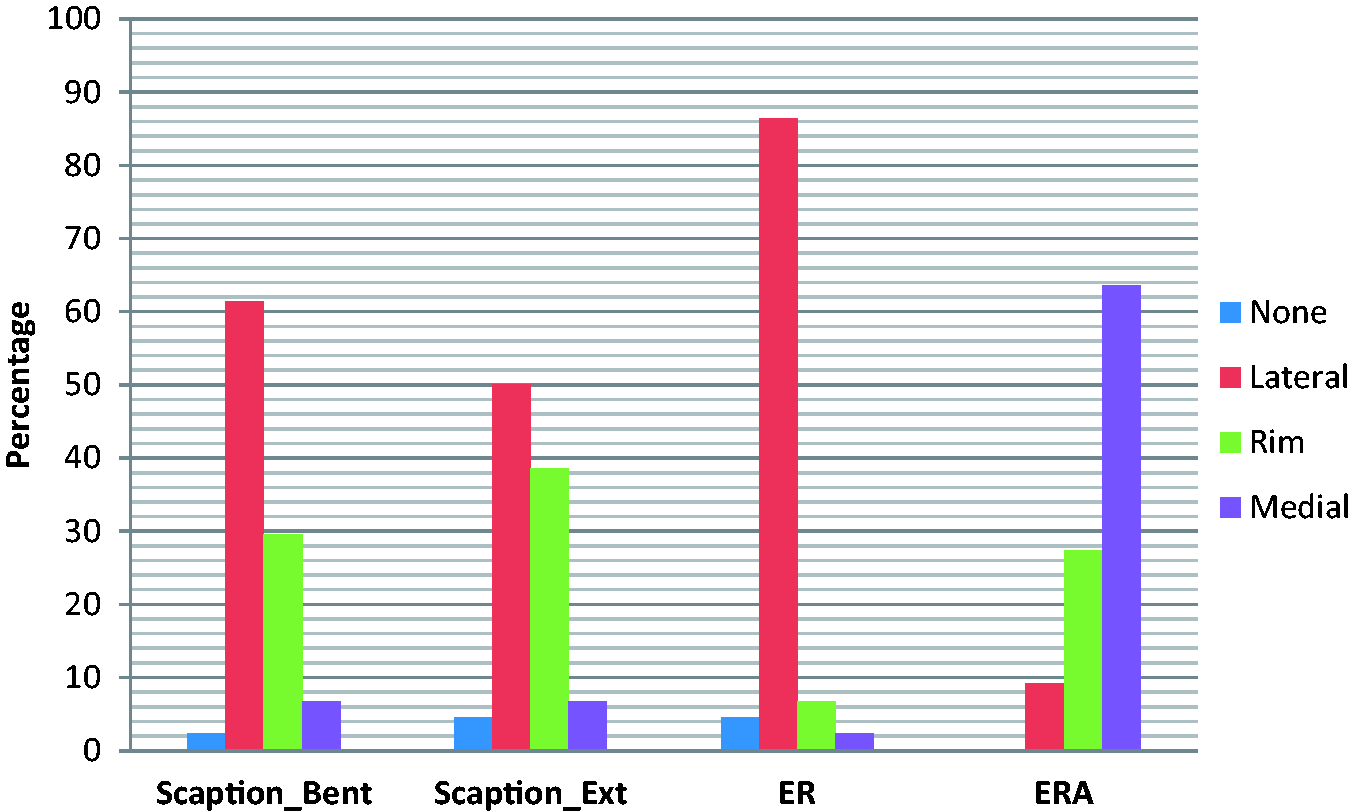
Discussion
The present study determined that the sub-supraspinatus recess is a variable, yet definable, anatomic entity of approximately 5 mm to 10 mm in depth. Our findings support previous studies suggesting that motion of the posterosuperior labrum, which we have termed ‘roll back’, is a normal, physiological phenomenon, particularly in external rotation in the abducted position.6,10
Thus, in addition to the effect of the biceps, posterosuperior labral roll back may also be a result, in part, of the medial movement of the rotator cuff and its capsular connection to the posterosuperior labrum. Posterosuperior roll back is present to some degree in most subjects and is most pronounced in the position of abduction and external rotation, or the late cocked phase of throwing. Burkhart et al.11–13 described a ‘peel-back’ lesion as a pathological condition. We suggest that peel back occurs as a pathological condition only when the labrum is torn and can sublux or migrate further medially than otherwise would normally occur.
The clinical implication of this finding may be significant as the treatment of SLAP tears is a subject of considerable debate. Several studies indicate less than favourable outcomes when these lesions are treated with standard labral repair techniques.6–9,14,15 Ongoing pain, stiffness and a failure to return to sport have been attributed to repairing superior labral lesions.6,16 Older age and overhead athletes, specifically pitchers, are those particularly at risk.6–8 In a systematic review, Sayde et al. 17 found that, although most patients undergoing SLAP repair did well, overhead athletes faired poorer. In a prospective evaluation of 179 surgically treated type II surgically treated superior labral repairs, Provencher et al. 9 found a limited return to full activity, with a 37% failure rate and a 28% revision rate. Similarly, Kim et al. 15 found that only 22% of patients could return to the same level of activity after SLAP repair. Thus, some studies have recommended tenodesis of the long head of the biceps over labral repair to avoid these complications.6,18,19
Boileau et al. 6 suggested that pain and stiffness after SLAP repair results because the repair tethers the superior labrum and prevents its normal physiological roll back. We suggest that stiffness following SLAP repair may also occur as a result of scarring of the superior labrum to the undersurface of the rotator cuff which obliterates the sub-supraspinatus recess (as described in the present study). This may inhibit full rotator cuff excursion, in turn blocking glenohumeral motion, which results in clinically apparent stiffness and/or pain. McCormick et al. 19 have confirmed this mechanism in a review of 42 failed SLAP repairs undergoing re-operation. They identified scarring between the superior labrum and undersurface of the rotator cuff in 33 of 42 (79%) of cases. 18 Because maximal physiological posterosuperior motion, or roll back, is seen in external rotation in abduction, this potential negative consequence of SLAP repair will be most noticed by those who predominantly require their arm in an abducted and externally rotated (late cocked) position.
The strengths of the present study are that it was prospective and followed a standardized procedure for measuring both recess depth and labral movement using a trained assessor independent of the surgical procedure. However, this was a descriptive study only and further work is required to determine whether our hypotheses are correct. In addition, our selection criteria were chosen to minimize focal pathology of the superior labrum and sub-supraspinatus recess. However, patients enrolled in the present study were predominantly male (75%) with a diagnosis of instability (65%). The effect of sex is uncertain, although we would not anticipate significant variations in a female cohort. Patients with instability may, in theory, demonstrate increased motion given underlying laxity. A group of asymptomatic control subjects would be the gold standard but, given the surgical intervention, would not be appropriate. In the future, inclusion of patients with a broader range of diagnoses may determine the impact of variations in anatomy and motion.
The present study identified a definable sub-supraspinatus recess cephalad to the posterosuperior labrum and caudal to the rotator cuff that typically measured 5 mm to 10 mm in depth. We further identified that the posterosuperior labrum has physiological motion, or roll back, with glenohumeral motion in the majority of subjects and is most pronounced with the arm in a position of external rotation in abduction. This finding may have clinical implications for the overhead athlete undergoing SLAP repair because post-surgical alterations of the normal physiological motion of the superior labrum and sub-supraspinatus recess may result in a limitation of their sports performance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Review and Patient Consent
The regional Health Ethics Research Board approved this study (Pro00018860); all subjects signed informed consent.