
Abstract
Introduction
Itoi et al. introduced the concept of bracing in abduction and external rotation to treat traumatic anterior shoulder dislocations. However, controversy remains as studies have reported variable results. Our study investigates whether there is a difference in outcomes between treatment with a conventional sling or external rotation brace.
Methods
A prospective, multi-centre randomised control trial was conducted between 2006 and 2010. The study was discontinued early with 72 (36 cases in each group) first-time anterior shoulder dislocations recruited.
Results
The re-dislocation rate over 24 months was comparable 30% (95% CI: 17–47) sling vs. 24% (95% CI: 13–41) external rotation bracing. Sixteen percent (95% CI: 7–32) of sling patients and 12% (95% CI: 5–27) of external rotation-bracing patients had shoulder stabilisation surgery within 24 months of the initial dislocation (p > 0.05). There was no difference in OSI scores at 24 months between the two treatment groups and intolerability of the external rotation brace was high.
Conclusion
Recruitment to this study was difficult, and lost-to-follow-up rates were high leading to early discontinuation of the study. The results suggest that ER bracing is unlikely to provide clinical benefit in traumatic first-time anterior shoulder dislocation.
Keywords
Introduction
The glenohumeral joint has a large range of motion due to a relative lack of bony restraint. 1 As a result, it is the most commonly dislocated major joint in the body. 2 The majority of dislocations are anterior 3 and result in disruption of the anterior labrum and capsuloligamentous attachment (Bankart lesion 4 ) with a corresponding Hill Sachs lesion. 5
The aim of treatment is to prevent further dislocation. The established treatment for first-time traumatic anterior glenohumeral joint dislocation, following initial assessment and reduction, is immobilisation in a sling with the arm held in adduction and internal rotation. However, this method has high recurrence rates ranging from 40 to 92%,3,6 and some surgeons prefer early surgical stabilisation in certain circumstances. Studies comparing immobilisation versus no period of immobilisation have shown no difference in recurrence rates for further dislocation. 7
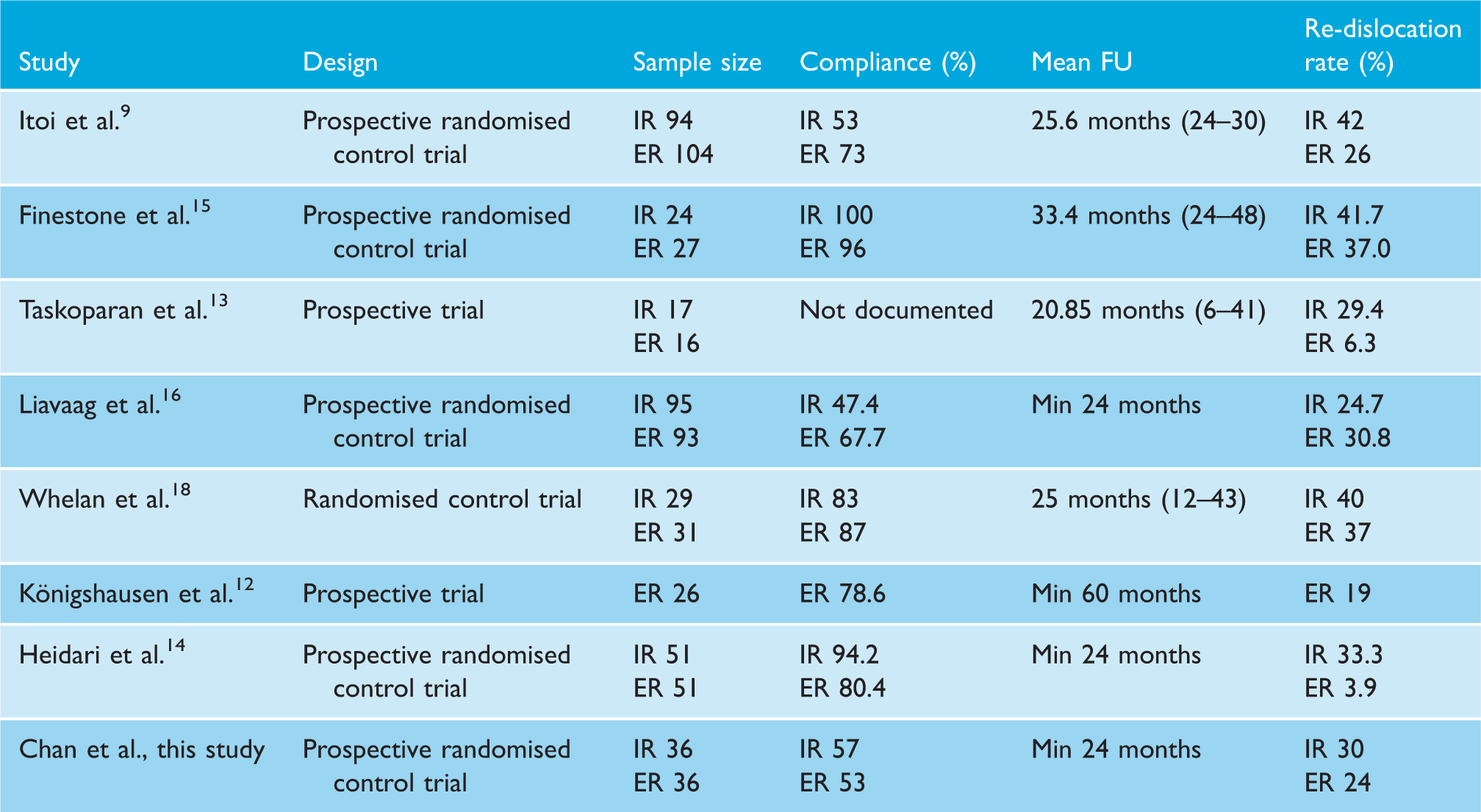
Studies to date assessing clinical outcomes on ER bracing.
Materials and methods
This study was a prospective, pragmatic, multi-centre randomised control trial with approval from the Research Ethics Committee in May 2006 (Ref: 06/Q2604/34). It included six centres across England (Basildon University Hospital, Basildon and Thurrock University Hospitals NHS Foundation Trust; Northumbria Healthcare NHS Foundation Trust; Queen Elizabeth Hospital, Queen Elizabeth Hospital King’s Lynn NHS Foundation Trust; Royal Oldham Hospital, Pennine Acute Hospitals NHS Foundation Trust; Royal Shrewsbury Hospital and Princess Royal Hospital, Telford, The Shrewsbury and Telford Hospitals NHS Trust; The Ipswich Hospital NHS Trust). All trial participants received standard manipulation under local or general anaesthetic to reduce the dislocation in the acute setting and were referred to an orthopaedic clinic. Confirmation of the diagnosis with standard radiographic images was performed. Prospective patients received a patient information leaflet (online Appendix 1), were allowed time to ask questions and written consent obtained before enrolment. Due to the nature of the intervention, blinding of the patient or index surgeon was not possible.
From September 2006, eligible patients aged between 16 and 45 presenting with a first-time traumatic anterior shoulder dislocation were enrolled. Exclusion criteria included an associated fracture, an indication for surgery (as determined by the recruiting surgeon), inability to provide informed consent, learning difficulties, mental illness, dementia, significant co-morbidities or if the patient was unwilling to participate.
Randomisation was carried out independently by the York Trials Unit by telephone, with participants assigned to receive a conventional sling (Polysling, Mölnlycke Health Care, Gothenburg, Sweden) immobilising the arm in internal rotation or an ER brace (Smartsling, Ossur, Reykjavik, Iceland) which held the arm at 30° of external rotation and 30° of abduction (Figure 1). Participants in both groups were instructed to keep the arm in the sling or brace for four weeks (day and night) except when showering or bathing. Participants were also instructed by a physiotherapist to follow a course of specific shoulder exercises and received written instructions for completing the exercises at home (online Appendix 2). Compliance with the exercise regime was reinforced by a telephone call to participants by the trial coordinator a few days after the sling/brace was fitted. All participants received an appointment to return to clinic at four weeks to be reviewed by the clinician and have the sling/brace removed.
External rotation brace, Smartsling, Ossur, Reykjavik, Iceland.
Outcome measures
Clinical and functional evaluations took place at 3, 12 and 24 months after dislocation and were conducted by site co-ordinators. If patients failed to attend follow-up appointments, data were collected by telephone interview. All outcomes were analysed on an intention to treat basis and were collected by a research co-ordinator.
The primary outcome measure was re-dislocation of the shoulder within 24 months from baseline or recurrent instability, as captured by the self-reported Oxford Shoulder Instability Questionnaire. Any shoulder stabilisation surgery during the study period was noted.
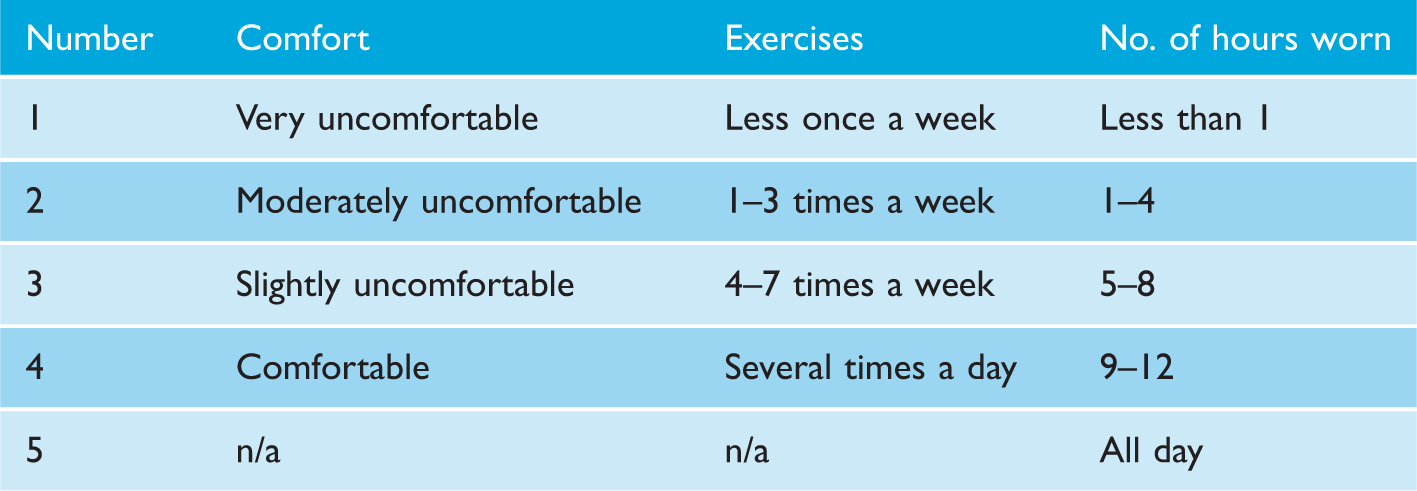
Assigned values for patient responses with regard to tolerability of sling/brace.
Statistical methods
The sample size was calculated on a statistical superiority basis taking into account that 30% of patients with acute anterior dislocation will have a subsequent dislocation of the same shoulder within two years. A sample size of 69 patients per group was calculated to enable detection of a reduction from 30 to 10% (a standardised effect size of 0.26) using a two-tailed Fisher’s exact test at p = 0.05 and with 80% power, allowing for a 15% lost-to-follow-up rate. The trial aimed to recruit 80 patients per group (160 in total).
After one year, a blinded interim analysis was to be undertaken to adjust the sample size if required and to confirm whether recruitment should continue.
The primary endpoint of further dislocation within the pre-specified timeframe of two years was analysed using a Chi-squared test or Fisher’s exact test if an expected cell frequency was below 5. The same analysis was also used for all other count data, such as the compliance rates. Because interval data were non-normally distributed, all ordinal and interval data were analysed using a non-parametric test (Mann–Whitney U test). A p value of 0.05 or less was considered to denote statistical significance. All statistical analyses were performed using R version 2.8.1 (R Foundation for Statistical Computing).
Results
Patient demographics
By February 2011, a total of 72 cases of shoulder dislocation in 71 patients had entered the trial, with 36 cases allocated to each treatment group. At that point, recruitment had become very slow, and it was decided to do a blinded sample size recalculation using the method proposed by Wüst and Kieser. 21 This analysis suggested that the overall re-dislocation rate in the trial would be 29%. Using this number, and assuming the trial should still be powered to find a 20% difference in dislocation rates between the two groups, the sample size should be increased to 95 per group (assuming a Chi-squared test, p = 0.05, 80% power, 15% lost to follow-up). Against the background of slow recruitment and the finding that the overall dislocation rate in the trial was similar to that assumed for the control group, it was decided to stop recruitment into the trial at that point but complete the remaining outcomes collection.
Patient characteristics for the two treatment groups.
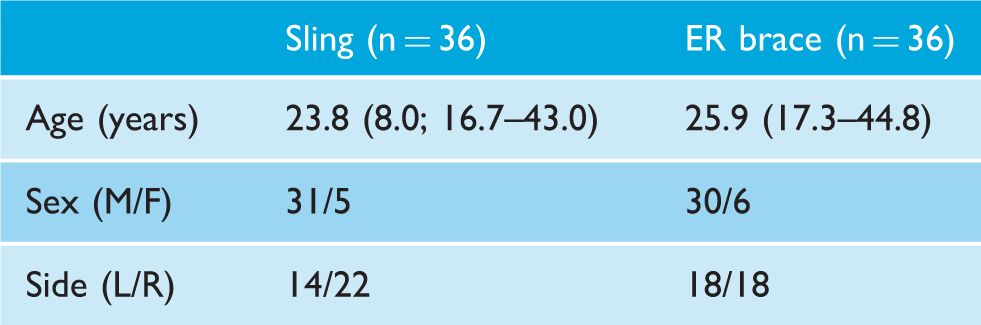
Age is given as median (IQR; range). p Values for differences between the two groups were calculated using the Mann–Whitney U test for the age, a Chi-squared for sex and side.
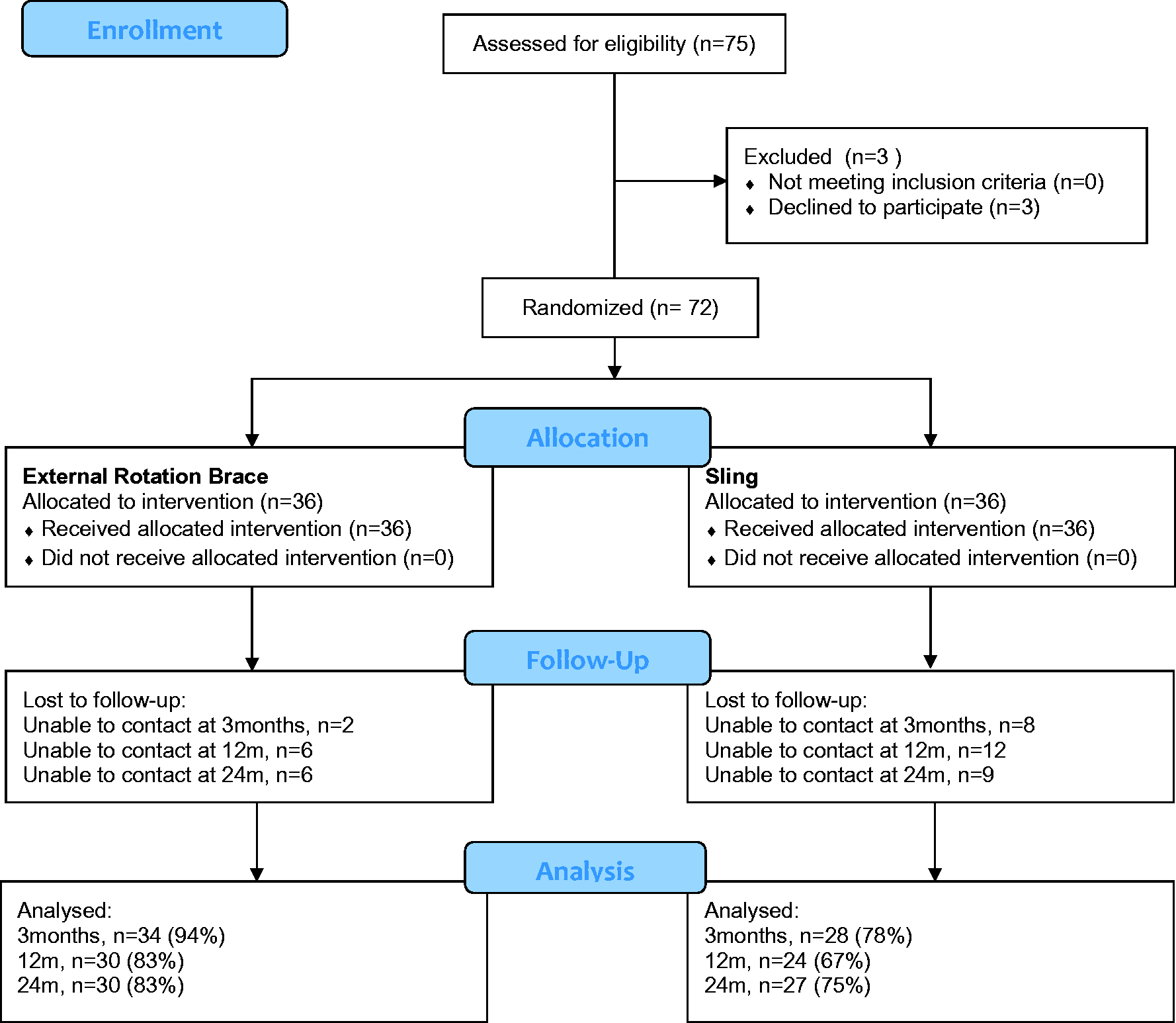
Consort diagram for patient enrolment and follow-up.
Primary outcome
The overall re-dislocation rate during the 24 months follow-up period was 10/33 (30%; 95% CI: 17–47) in patients with a sling and 8/33 (24%; 95% CI: 13–41) in patients with an ER brace (Table 2). In all, 5/32 (16%; 95% CI: 7–32) of patients with a sling and 4/33 (12%; 95% CI: 5–27) of patients with an ER brace had further surgery within two years of the initial dislocation. There was no significant difference in the dislocation rate (p = 0.58) or the surgery rate (p = 0.68) between the two groups.
Secondary outcomes
At three months, 62 patients (34 in the ER brace group and 28 in the conventional sling group) returned the questionnaire. Both devices were worn for a median period of four weeks, mostly all day, with no significant difference between the two groups (Table 3). Over three-quarter of the patients (47/62) wore the devices at least sometimes at night, with no significant difference between the two groups. There was no significant difference in compliance rates between the two groups. However, almost twice as many patients wearing the ER brace reported difficulties compared to those wearing a conventional sling, a significant difference (79% vs. 46%; p = 0.007).
In the ER-bracing group, 62% (21/34) of patients complained of difficulty wearing the brace at night. Reasons for this included pain, difficulty sleeping and the straps coming loose overnight. Other complaints include feeling that the brace did not support the arm (21%), functionally awkward in the daytime (18%), difficulty in application of the sling (15%) and pain when in external rotation (12%).
In the conventional sling group, difficulties described include night symptoms (25%), difficulty in application/loosening of the straps (14%), feeling hot/itchy (11%) and pain around the neck strap (7%). Although patients wearing a sling reported a statistically significant higher level of comfort (3.5 vs. 3.0) and exercise frequency (4.0 vs. 3.5), this relates to a level of comfort between slightly uncomfortable and comfortable and an exercise level between four and seven times per week and several times per day (Table 2) and appears to be of limited clinical significance.
At 12 months, 55 patients (31 in the brace group and 24 in the sling group) returned the Oxford Shoulder Instability Score (OSIS) questionnaire. Patients who had worn the ER brace reported slightly higher median scores than those who had worn the sling (43 vs. 42.5, Table 2) but this difference was not significant (p = 0.35). Based on specific questions in the OSI questionnaire, no significant difference was found in pain or re-dislocation rates between the two groups (p = 0.32 or more).
Outcomes at 3, 12 and 24 months for the two treatment groups.
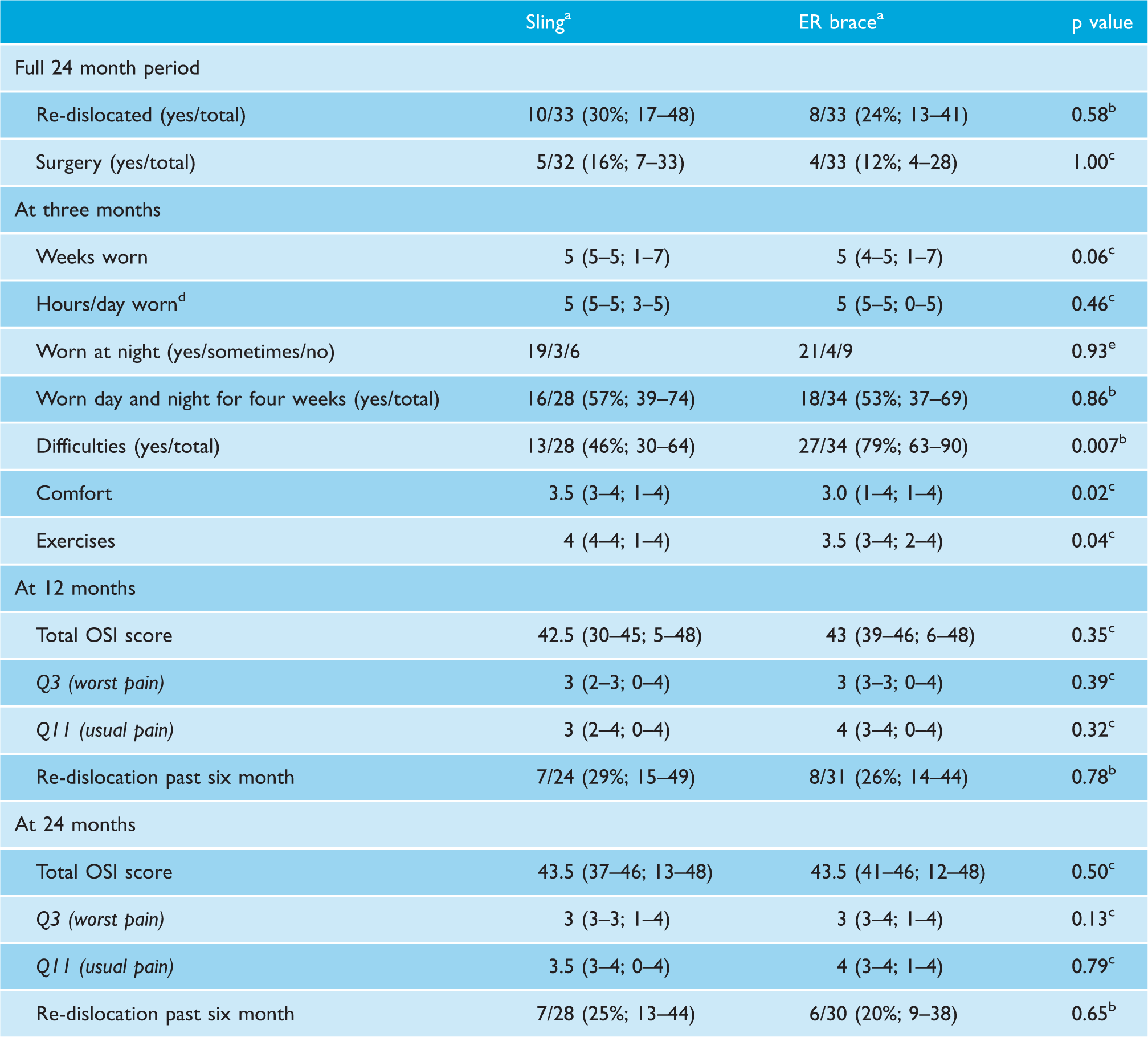
aCounts given as numbers/totals (%; 95% CI); Ordinal and interval values given as median (95% CI; range).
bp Value calculated using a chi-squared test.
cp Value calculated using a Mann–Whitney U test.
dResponses: 1 = less than 1 h, 2 = 1–4 h, 3 = 5–8 h, 4 = 9–12 h, 5 = all day.
ep Value calculated using Fisher’s exact test.
Discussion
Immobilisation in internal rotation has been a long established treatment for anterior glenohumeral dislocation. Studies have shown that 52–80% of patients stabilise and do not lead to further dislocations with conservative management. 7 The duration of sling immobilisation has been studied and we now know that the duration of bracing is not critical to the outcome in first-time dislocators.7,22 The authors believe that a period of relative immobilisation in a conventional sling for two to three weeks is reasonable for patient comfort only.
Itoi postulated that these patients had an unreduced Bankart lesion which could result in potential instability. 9 Itoi originally introduced the concept of external bracing to ‘coapt' and reduce the capsuloligamentous complex in anterior shoulder dislocations in the 1990s. 10 This concept evolved from cadaveric studies to magnetic resonance imaging studies and culminated in a randomised control trial showing rates of dislocation reducing from 42 to 26%.8–10 Itoi’s bracing was customised to the patient (Alcare, Tokyo, Japan), whereas recent papers, including this study, have used commercial off the shelf braces that could be easily removed by the patient. Previous studies have included the following braces – Ultrasling ER, Donjoy, Vista, California, USA12,16,18 and an ER brace produced by Uriel, Nesher, Israel. 15 However, it has remained uncommon orthopaedic practice for the management of anterior shoulder dislocations.
This RCT was hampered by poor recruitment, poor compliance and difficulties in outcome follow-up. This may be to do with the nature of the population who are generally young, mobile and working people. In the light of the smaller sample size, it may not be surprising that the study found no evidence for a difference in re-dislocation rates at two years between patients wearing a sling and those wearing an ER brace (30% vs. 24%, p = 0.58). The secondary outcomes measured also show that there was no significant difference between the two groups – the proportion of patients requiring surgical stabilisation due to recurrent symptoms (16 vs. 12% respectively), the OSI scores at two years (43.5 vs. 43.5). These results are in concordance with similar and more recent studies performed by Finestone et al. 15 and Liavaag et al. 16
The main reasons for discontinuing the trial were difficulties in recruitment, combined with a larger than anticipated overall dislocation rate. The trial was commenced in 2006 and had recruited 72 patients over a four-year period, far less than anticipated. The difficult recruitment may be related to the population group, predominantly young males not enthused by research and trials. Some patients who might have been eligible for inclusion refused to participate in the trial when shown the ER brace. In addition to the poor recruitment, a blinded interim sample size recalculation showed that the overall re-dislocation rate (29%) was higher than the 20% anticipated when designing the trial, which would mean that more patients had to be recruited than originally planned to maintain sufficient power. It was therefore decided to halt recruitment but continue the follow-up of all trial patients as planned.
Obviously, the early discontinuation of the trial reduced the power of the trial. The final analysis found no statistical evidence of a difference between the two groups, but this could be related to a lack of power. The trial was originally powered to detect a standardised effect size (ES) of 0.26. However, the reduced sample size of 31 per group reduced the sensitivity of the trial (the smallest detectable ES) to 0.42 if we assume that the dislocation in the control group would be 30% or 0.39 if we assume an overall dislocation rate of 29%. These ESs are between a small (ES = 0.25) and medium (ES = 0.5) effect size. Therefore, we feel confident that our trial demonstrates that external bracing will at best have a medium effect on dislocation. Moreover, the lower 95% confidence limit of the actual re-dislocation rate in patients wearing the ER brace (13%) was clearly above the anticipated re-dislocation rate of 10% when designing the trial. Our results therefore also show that wearing the external rotation device in this trial is highly unlikely to achieve this anticipated rate, and we feel justified in halting recruitment early.
Compliance with the outlined treatment might be a factor affecting the overall results. Itoi defined compliance as continuous wear over 20 h a day for three weeks and achieved a compliance rate of 72%. 9 Finestone et al. achieved a 100% compliance rate in a largely military population of continuous wear for four weeks, 15 whilst Liavaag defined compliance as immobilisation of more than 16 h per day for 20 consecutive days and achieved a rate of 67.7% in the ER-bracing group. 16 Compliance rates in both groups of our study were lower than these three studies. However, the results from two of the three suggest that higher compliance rates still do not ensure lower dislocation rates in ER braces.15,16 Moreover, the re-dislocation rates in our study are not higher than in those two studies, suggesting that our poorer compliance may not have affected the outcome.
There are further limitations to this study. In our study group, the patients’ age range was 16–44 years. In the current literature, it is generally accepted that patients who are younger at their first dislocation will face a higher the rate of recurrence and symptoms of instability. Patients under 30 have a rate of over 50%, whilst those over 30 decrease to 16–28%.9,23 It is accepted that in our cohort, due to the age range included, there may be an inherent variation in risk of re-dislocation rates within this group. However, the two groups were balanced in terms of demographics, and therefore, this factor is unlikely to bias the results.
Poor compliance with the treatment protocol was a major drawback of the study. However, the design of the study included patient information given at the outset and telephone conversations were made after two to three days to reinforce the treatment protocol. It was felt that all practicable efforts were made to reinforce the importance of correct wearing of the braces. Therefore, the results are interpreted on an intention to treat basis, despite the variation in compliance levels between the two groups. In each case, the patients were recruited after closed reduction and a plain X-ray showing the absence of obvious fracture or major bony Bankart lesions. This was the current clinical practice at the time. The exact pathological anatomy such as displaced Bankart lesions, major Hill Sachs humeral head lesions, loose bodies and tendon injury could only evaluated by routine bone and soft tissue scanning and possible diagnostic arthroscopy. Future studies may be more valuable with this information available at randomisation. Also, in further research, it would be worth clarifying whether patients who fully comply with 30° ER bracing show any significant decrease in symptoms of instability and recurrence rates. In addition, we are not aware of any studies comparing different types of ‘off the shelf’ ER braces.
Surgery for first-time dislocators may be considered depending on age, pathological lesion, physical demand and patient choice. Due to the pragmatic nature of the study, patients were excluded from this study if the surgeon felt that a particular patient merited operative stabilisation. The authors acknowledge that there is an increasing move towards early assessment of the pathological anatomy with a view to surgery especially in the developed countries. However, the vast majority of traumatic dislocators globally are managed conservatively on their first dislocation. We believe the pursuit of excellence in conservative management is a valid philosophy in this condition.
Conclusions
We conclude that our study illustrated the difficulties in completing a large scale study of this type. Recruitment, compliance and outcome follow-up proved challenging and compromised the scientific value of this study. We found no evidence that ER bracing decreases re-dislocation rates or surgery rates or improves shoulder function compared to standard sling immobilisation. There is no significant difference in compliance rates between the two groups although levels of reported tolerance were significantly worse in the ER-bracing group. This study has shown lower levels of compliance for ER bracing and sling immobilisation than has been previously reported in the literature, which may relate to variable factors in the populations studied. The authors recommend a further more extensive RCT study taking into account the difficulties encountered in our study. However, the decline in the use of ER bracing in recent years makes it unlikely that such a study would be supported or resourced appropriately.
Supplemental Material
Appendix 1 -Supplemental material for External rotation bracing for first-time anterior dislocation of the shoulder: A discontinued randomised controlled trial comparing external rotation bracing with conventional sling
Supplemental material, Appendix 1 for External rotation bracing for first-time anterior dislocation of the shoulder: A discontinued randomised controlled trial comparing external rotation bracing with conventional sling by Samuel KL Chan, Kieran R Bentick, Jan H Kuiper and Cormac P Kelly in Shoulder & Elbow
Supplemental Material
Appendix 2 -Supplemental material for External rotation bracing for first-time anterior dislocation of the shoulder: A discontinued randomised controlled trial comparing external rotation bracing with conventional sling
Supplemental material, Appendix 2 for External rotation bracing for first-time anterior dislocation of the shoulder: A discontinued randomised controlled trial comparing external rotation bracing with conventional sling by Samuel KL Chan, Kieran R Bentick, Jan H Kuiper and Cormac P Kelly in Shoulder & Elbow
Footnotes
Acknowledgements
We thank the following surgeons, who submitted cases for this trial: Tim Peckham, Usha Mathias – Basildon University Hospital, Basildon and Thurrock University Hospitals NHS Foundation Trust Jaime Candal-Couto – Northumbria Healthcare NHS Foundation Trust (Wansbeck General) Anil Chakrabarti – Queen Elizabeth Hospital, Queen Elizabeth Hospital King’s Lynn NHS Foundation Trust Leo Jacobs R.I.P. – Royal Oldham Hospital, Pennine Acute Hospitals NHS Foundation Trust Ron Dodenhoff, Stuart Hay, Cormac Kelly – Royal Shrewsbury Hospital and Princess Royal Hospital, Telford, The Shrewsbury and Telford Hospitals NHS Trust Chris Roberts, Mark Bowditch, Patricia Hanna – The Ipswich Hospital NHS Trust Research Department, The Robert Jones and Agnes Hunt Orthopaedic Hospital NHSFT, with special thanks to Samantha Griffith Norris
Declaration of Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by: The British Elbow and Shoulder Society; Institute of Orthopaedics, Robert Jones and Agnes Hunt Hospital, Oswestry Shropshire; Ossur UK provided the ER braces and were not involved in the design, data analysis or preparation of this paper.
Ethical Review and Patient Consent
This study was approved by the Research Ethics Committee (REC number: 06/Q2604/34).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.