
Abstract
Objective
To compare tenotomy versus tenodesis for the treatment of long head of the biceps tendon pathologies. The primary outcome was the shoulder functional outcome. The secondary outcomes consisted of postoperative pain, elbow flexion and forearm supination strengths and postoperative complications.
Methods
PubMed, MEDLINE, Google Scholar and Web of Science were searched until April 2020. Included studies were randomized controlled trials with a minimum 12 months’ follow-up.
Results
Both treatments had similar improvement on the Constant–Murley score at 6 months and 12 months. However, tenotomy had a significantly lower Constant–Murley score at two years with a mean difference of −1.13 (95% confidence interval −1.9, −0.35). Furthermore, tenotomy had a risk ratio of 2.46 (95% confidence interval 1.66, 3.64) for developing Popeye’s deformity. No significant difference was detected in other functional outcomes, pain, or elbow flexion and forearm strength indices.
Discussion
Tenodesis and tenotomy are both well-established techniques that similarly yield satisfactory outcomes. Despite that tenodesis had a statistically significant better Constant–Murley score at two years, this was clinically irrelevant. With the current evidence, we recommend either technique for the management of the long head of the biceps tendon pathologies.
Level of evidence
Therapeutic, Level II
Introduction
Although the role of the long head of the biceps tendon (LHBT) is debated, any pathology that affects the LHBT can lead to anterior shoulder pain. 1 Several proposed mechanisms are implicated in the development of LHBT pathologies. 2 Degenerative changes due to the aging process are often associated with rotator cuff tears, which lead to LHBT tendinitis, partial and full thickness tears, and instability. Whereas, LHBT injuries in the younger population are associated with acute traumatic tears of the subscapularis tendon. Repetitive overhead activities, as in throwing athletes, lead to labral pathologies involving the LHBT anchor such as the superior labrum anterior-to-posterior (SLAP) lesions.
The management of isolated LHBT pathology is usually non-operative, with surgical treatment reserved for recalcitrant cases after the non-operative treatment. However, the surgical treatment for LHBT lesions is often carried out in the same setting of rotator cuff repairs, as 48–52% of cases with rotator cuff tears are associated with LHB tendinitis and subluxation/dislocation, respectively. 3
The two main surgical options are tenotomy and tenodesis. Tenotomy consists of releasing the LHBT tendon, whereas soft tissue tenodesis involves releasing and reattaching the tendon on the humerus. Tenotomy is a relatively safe, simple and quick procedure with shorter rehabilitation demands. On the other hand, tenodesis is less associated with cramping and cosmetic deformity despite being a more demanding procedure, higher rate of surgical complications and more rigorous postoperative rehabilitation protocols. 4 Latest meta-analyses on mixed randomized and non-randomized studies reported that tenodesis had superior functional outcomes with lower complications.5,6 However, since then several randomized trials were published on this topic that contradicted the findings of the aforementioned meta-analyses. Therefore, the aim of this study was to provide updated evidence consisting of randomized controlled trials (RCTs) comparing LHBT tenotomy versus tenodesis.
Materials and methods
This systematic review and meta-analysis was conducted with adherence to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 7 The primary aim of this study was comparing the shoulder function between LHBT tenotomy and tenodesis. The secondary outcomes consisted of postoperative range of motion, strength, pain and complications.
Eligibility criteria
Studies comparing LHBT tenotomy versus tenodesis were sought. Included studies had to be RCTs (Level 1 and 2 studies) reporting functional outcome measures and having a minimum follow-up of 12 months. Non-randomized studies, abstracts and articles not published in English were excluded.
Information sources and search strategy
PubMed, MEDLINE, Google Scholar and Web of Science were searched until April 2020. The search strategy involved the use of the following keywords: ‘Biceps’ AND ‘Tenotomy’ AND ‘Tenodesis’. Studies were screened by titles and abstracts. A full-text review was performed if a study matched the eligibility criteria. Furthermore, the references of each eligible article were manually sought to ensure no eligible studies were missed. The search strategy was performed by two authors independently.
Data collection process and data items
Data collection forms were used independently by two authors. The data items that were collected included: the first authors’ surnames, study year and location, age, sex, number of patients, the treatments performed, follow-up time points, the Constant–Murley Score (CMS), the American Shoulder and Elbow Surgeons (ASES) scores, the visual analogue scale (VAS) for pain, biceps cramping pain, bicipital groove pain, forearm supination and elbow flexion strength indices, and complications developed after each treatment.
Risk of bias in individual studies
The qualitative analysis was performed with the revised Cochrane risk-of-bias tool for randomized trials (RoB 2). 8 The tool contains five domains which assess the randomization, adherence to intended treatments, missing outcomes, measurement bias and reporting bias. Each study was assessed by two authors independently.
Quantitative synthesis
The quantitative synthesis was performed with the use of Stata/IC (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). The outcomes were estimated with the use of 95% confidence interval (CI), and a significant difference in outcomes was considered statistically significant if the P value was less than 0.05. The mean difference (MD) was used for estimating the treatment effect of continuous outcomes. The Hedges G standard mean difference (SMD) was used for estimating the effect on the postoperative strength indices due to potential variability in measurement among studies. The risk ratio (RR) was utilized for dichotomous outcomes. The meta-analytic models were based on random-effects with the use of the DerSimonian–Laird method as a heterogeneity variance estimator. If a study reported medians or ranges instead of means and standard deviations, the conversion formulas by Hozo et al. 9 were used.
Results
Study selection
The search strategy resulted in 936 articles of which 530 articles were excluded, thus leaving 406 articles for searching by titles and abstracts. A total of 378 articles were excluded, resulting in 28 articles eligible for full-text reviews. Of the 28 articles, 18 articles were excluded which resulted in nine eligible articles. All nine eligible studies were included in the qualitative and quantitative analyses. The PRISMA flowchart is displayed in Figure 1.
The search strategy flowchart.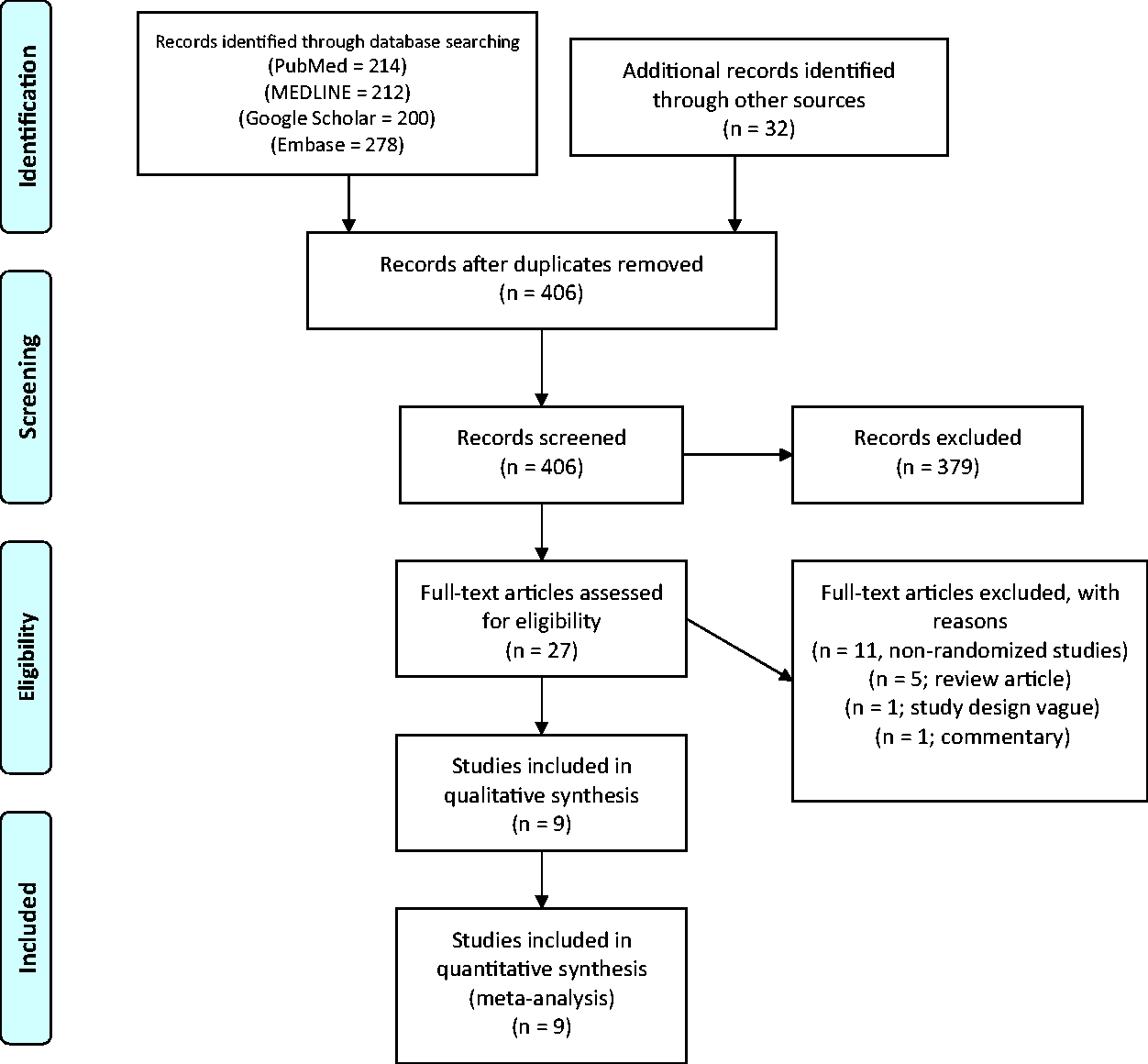
Study characteristics
Characteristics of included studies.
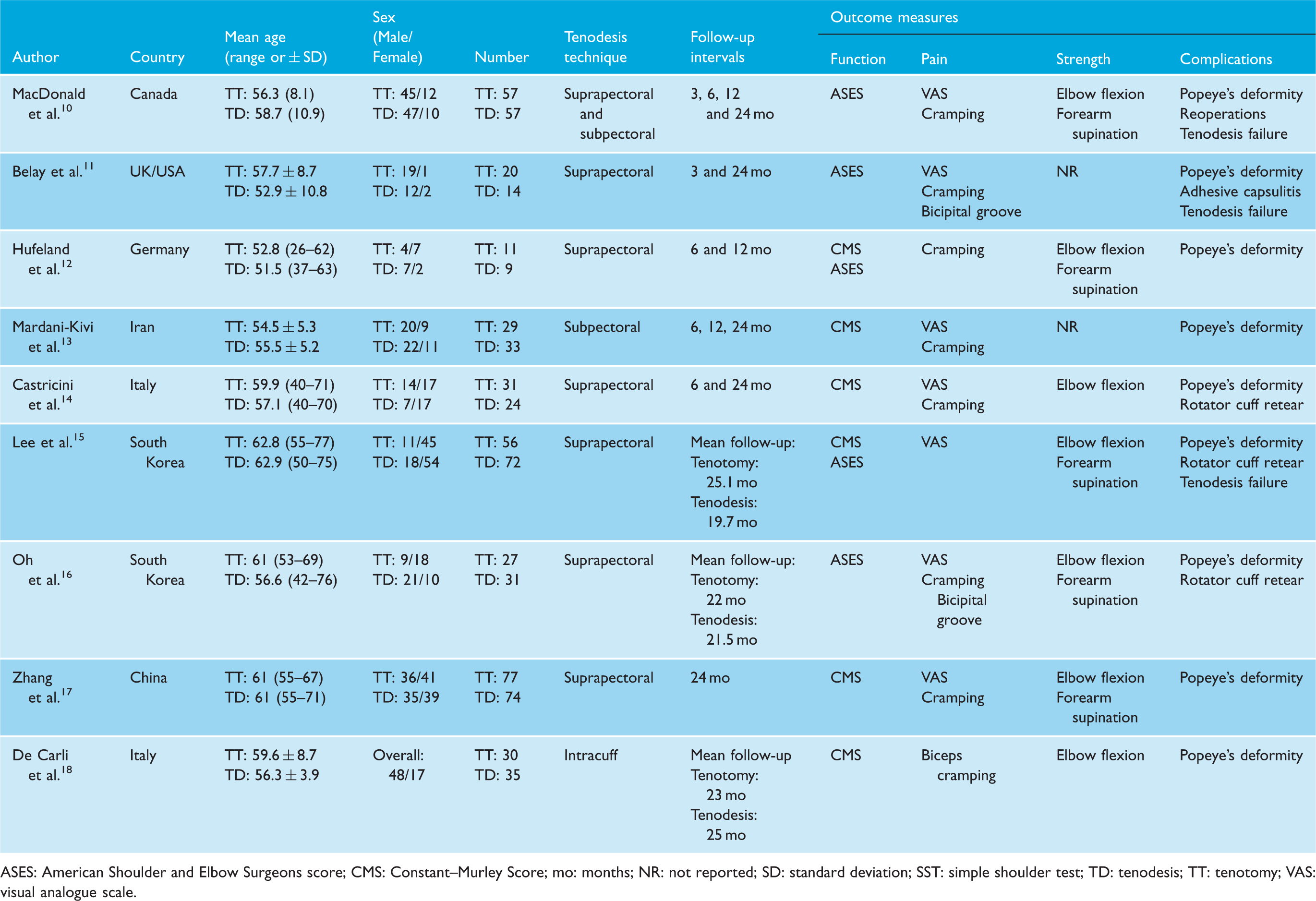
ASES: American Shoulder and Elbow Surgeons score; CMS: Constant–Murley Score; mo: months; NR: not reported; SD: standard deviation; SST: simple shoulder test; TD: tenodesis; TT: tenotomy; VAS: visual analogue scale.
The LHBT pathologies were degenerative tears, tenosynovitis, subluxation and SLAP lesions. Eight10,11,13–18 out of total nine studies included concomitant rotator cuff tears which were reparable, with only the study by Hufeland et al. 12 including SLAP lesions without rotator cuff tears. The status of the rotator cuff tear was variable among these studied ranging from high-grade partial-thickness tears to varying sizes of full-thickness tears (small to large).
The rehabilitation protocol in the included studies was variable. Eight of the included studies had rotator cuff repair which had a brief period of immobilization with an abduction brace for 3–6 weeks depending on the degree of rotator cuff tear. Gradual passive and active range of motion training were instituted after brace removal and strengthening began at 4–12 weeks following surgery. Return to sports and manual labour was permitted at six months. No immobilization was performed in the study by Hufeland et al. 12 as patients had isolated LHBT injuries.
Eight out of nine studies had no difference in rehabilitation between tenotomy and tenodesis. However, in the study by Zhang et al., 17 the tenodesis group was restricted with a return to elbow active range of motion allowed at six weeks postoperatively and unrestricted use of the biceps muscle at 16–20 weeks postoperatively. The tenotomy group had only elbow immobilization for one week in that study. The postoperative rehabilitation in the study by De Carli et al. 18 was not detailed.
Risk of bias within studies
With the use of the Cochrane RoB 2 tool, three studies were well designed with low risk of bias,10,12,14 three studies had some concerns,11,17,18 and three studies had a high risk for bias.13,15,16 **Figure 2 summarizes the risk of bias assessment across the five domains of bias.
The Cochrane risk of bias assessment.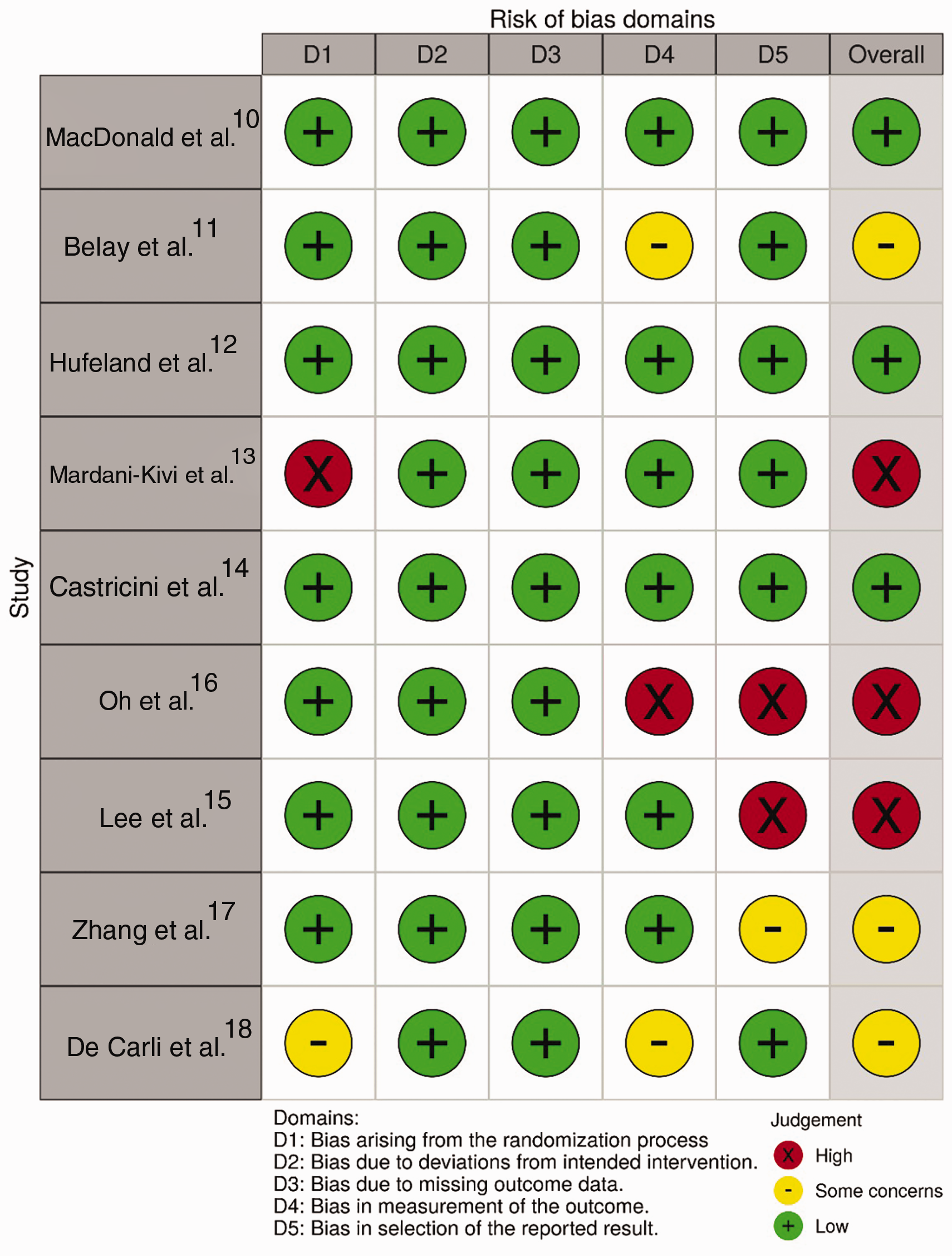
Results of individual studies
Shoulder function scores
The functional outcomes reported were the CMS in six studies12–15,17,18 and ASES in five studies.10–12,15,16 The functional outcomes were not statistically different between LHBT tenotomy and tenodesis at 6, 12 or 24 months in all randomized trials reporting shoulder function.
Pain outcomes
The VAS score for pain was reported in seven studies out of nine. Zhang et al. 17 found a significant reduction in pain in the tenotomy group at two weeks (P < 0.001) postoperatively with no difference at four weeks. At longer follow-up points, only the study by Mardani-Kivi et al. 13 showed significantly improved pain at 12 and 24 months in favour of tenotomy. However, other studies did not report any significant difference at 6, 12 and 24 months.10,11,14–16
Subjective biceps cramping pain was reported in seven studies out of nine.10–14,16,17 No significant differences were found in all included studies in terms of the subjective cramping pain except in the study by Mardani-Kivi et al., 13 which reported cramping in 31% of patients who had tenotomy versus 0% in tenodesis (P < 0.001).
Bicipital groove tenderness was reported in two studies, and no significant difference was reported between LHBT tenotomy or tenodesis.11,16
Elbow flexion and forearm supination strengths
The elbow flexion strength was reported in seven studies.10,12,14–18 No differences were found in elbow flexion strength indices at 6, 12 and 24 months. However, Hufeland et al. 12 found that tenodesis achieved significant improvement in elbow flexion at six months, despite no significant difference detected at 12 months.
The postoperative forearm supination strength was reported in five studies.10,12,15–17 Only the study by Oh et al. 16 reported superior supination strength for LHBT tenodesis at 24 months, whereas the other four studies found no significant difference between tenotomy and tenodesis.
Complications
Summary of postoperative complications.
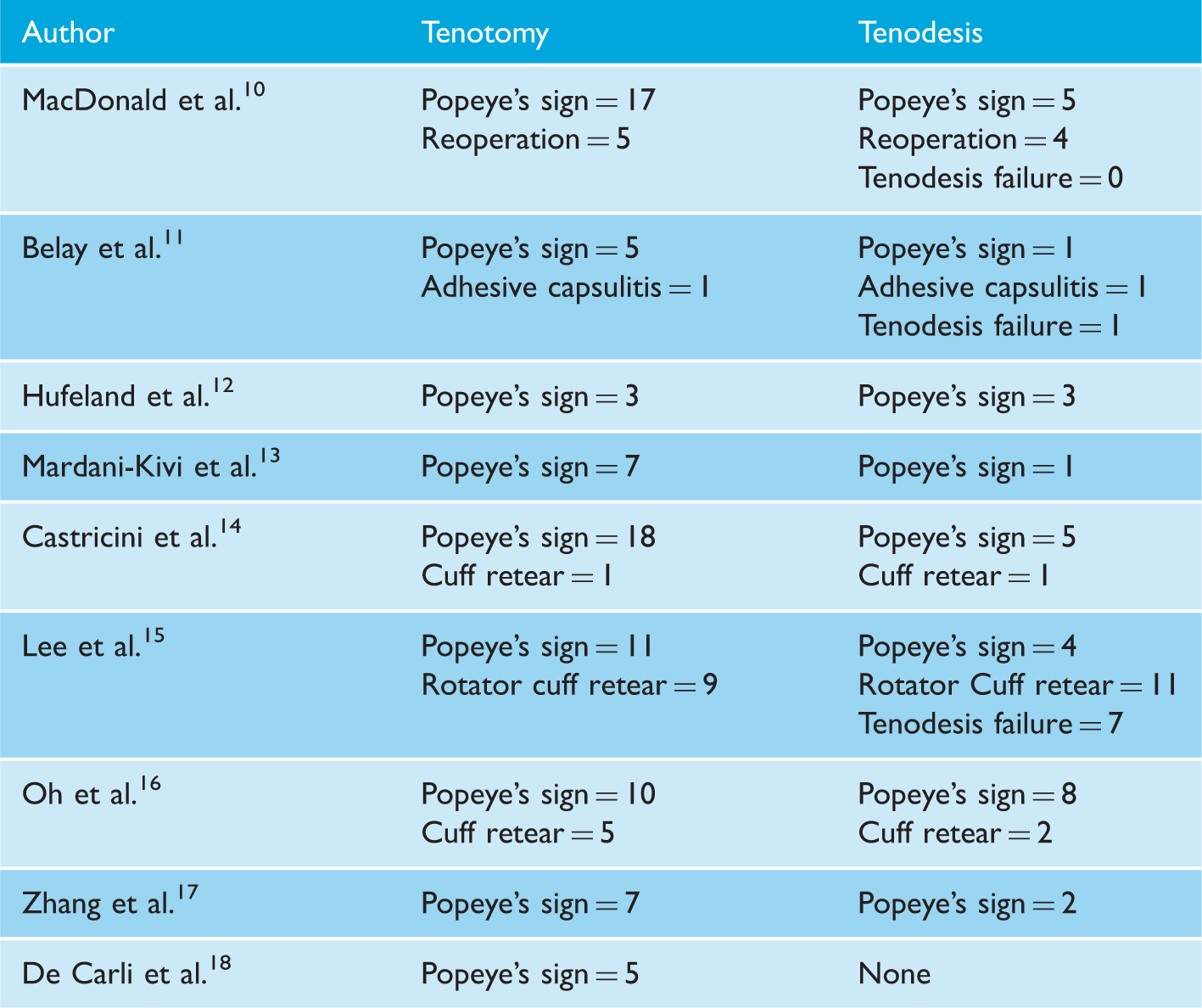
Three studies reported tenodesis failure rate at 24 months’ follow-up. Lee et al. 15 reported that 7 out 72 (10%) patients had failure of the LHBT tenodesis, Belay et al. 11 reported one case of tenodesis failure in 14 patients and MacDonald et al. 10 reported no tenodesis failures in 54 patients.
Revision surgeries were only reported by MacDonald et al. with no difference between tenotomy (five cases) and tenodesis (four cases). In all studies, no differences were detected retears for concomitantly repaired rotator cuffs.
Synthesis of results
Constant-Murley Scores
The comparison was performed on three studies12–14 at six months, two studies at 12 months,12,13 and four studies13,14,17,18 at two years postoperatively (Supplementary File 1). The meta-analytic comparison between tenotomy and tenodesis resulted in an MD of −0.67 points (95% CI −3.75, 2.4; P = 0.67; I2 = 22%) at six months; −5.08 (95% CI −14.02, 3.87; P = 0.27; I2 = 73.05%) at 12 months and −1.13 (95% CI −1.9, −0.36; P = <0.001; I2 = 0.00%) at two years.
The American Shoulder and Elbow Surgeons scores
The comparison was performed on two studies at 6 and 12 months,10,12 and on three studies at two years11,16 (Supplementary File 2). The meta-analytic comparison between tenotomy and tenodesis resulted in an MD of −5.36 (95% CI −26, 15.34; P = 0.61; I2 = 78.5%) at six months; −7.59 (95% CI −26.39, 11.21; P = 0.43; I2 = 80.5%) at 12 months and 0.26 (95% CI −3.7, 4.22; P = 0.9; I2 = 6.48%) at two years.
Postoperative pain
The VAS for pain comparison was performed on three studies13,14 at six months, two studies10,13 at 12 months and four studies11,13,14,16 at two years (Supplementary File 3). The comparison between tenotomy and tenodesis resulted in an MD of 0.17 (95% CI −0.16, 0.51; P = 0.3; I2 = 1.02%) at six months; an MD of −0.25 (95% CI −1.10, 0.61; P = 0.57; I2 = 56.21) at 12 months and an MD of −0.16 (95% CI −0.57, 0.25; P = 0.44; I2 = 43.79%) at two years.
In addition, the incidence subjective cramping pain was pooled in six studies. The RR for tenotomy when compared with tenodesis was 1.43 for subjective cramping pain at the latest follow-up point (95% CI 0.57, 3.58; P = 0.44; I2 = 38.48%) (Supplementary File 4).
Postoperative strength
Comparison of elbow flexion strength and forearm supination strength between long head of biceps tendon tenodesis versus tenotomy.
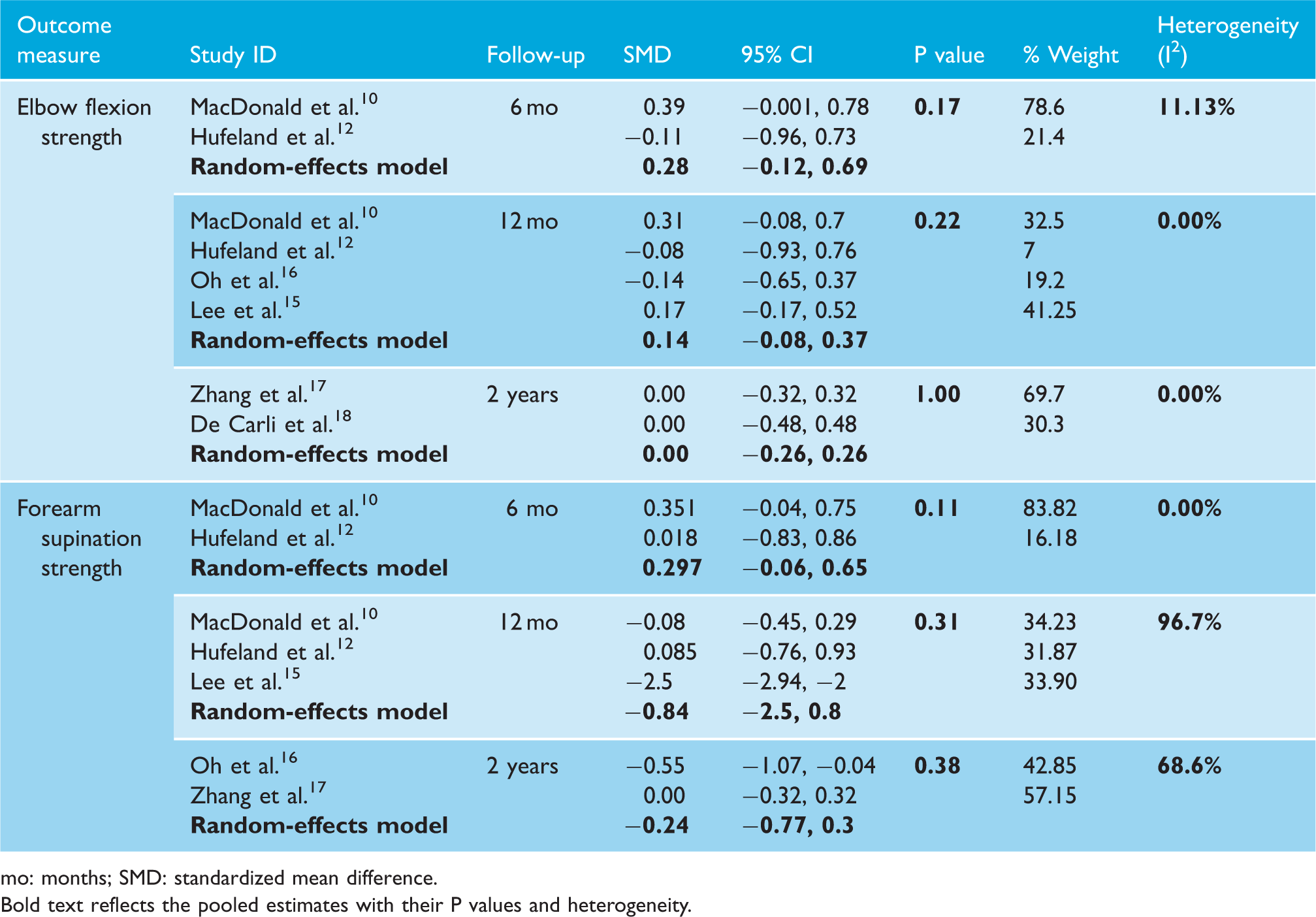
mo: months; SMD: standardized mean difference. Bold text reflects the pooled estimates with their P values and heterogeneity.
Postoperative complications
The incidence of Popeye’s deformity was reported in all studies, and the RR was 2.46 when comparing tenotomy to tenodesis at the latest follow-up point (95% CI 1.66, 3.64; P < 0.001; I2 = 1.77%) (Supplementary File 5). The overall tenodesis failure occurred in 2.3% (8 out of 346 tenodesis cases). The overall complication rate was not pooled due to the heterogeneity of the complications reported across studies.
Discussion
This systematic review was conducted to compare LHBT tenotomy versus tenodesis due to the controversial results in the recent literature. Our findings have shown that both treatments achieved satisfactory patient-reported outcomes on the CMS. No significant difference was detected at 12 months; however, there was a statistically significant difference in favour of tenodesis at two years postoperatively (MD = −1.13; 95% CI −1.9, −0.36). It is important to acknowledge that this difference is not clinically relevant since the minimally important clinical difference for the CMS has been reported to be between 10 and 15 points. 19 All of the RCTs12–15,17 comparing both treatments and most comparative cohort studies20–22 have found no difference in CMS up to two years of follow-up.
Furthermore, in this systematic review there were no significant differences detected in the ASES scores at 6 months, 12 months and two years of follow-up. Despite that each pooled follow-up point had only 2–3 studies, our findings were similar to the findings of each trial individually.10–12,15,16
The LHBT has been notable as a source for anterior shoulder pain. 1 Both tenotomy and tenodesis have been effective in achieving improvement in pain relief. However, tenotomy has been associated with subjective cramping pain in up to 20% in a case series on 104 patients. 23 Authors favouring tenodesis have argued that the prevalent pain following tenotomy can lead to delay in returning to work and less than optimal outcomes with individuals with high functional demands. 24 We found no significant difference between both treatment regarding pain on the VAS at a follow-up of two years. Moreover, the presence of subjective cramping pain was statistically insignificant between both treatments with most of the cramping resolving or improving within a period of 2–24 months postoperatively.14,16,17 However, MacDonald et al. 10 found that the cramping pain was relatively unchanged over time with a follow-up period of 24 months.
Several studies have found that tenodesis achieves superior forearm supination and elbow flexion strength. In the trial by Lee et al., tenodesis had significantly stronger supination (P = 0.02). Moreover, another study on 35 patients demonstrated that tenotomy had significantly larger decrements in supination peak torque. 25 In the case series by Kelly et al., 26 38% of patients who underwent tenotomy had biceps fatigue discomfort after resisted elbow flexion. Hence, tenodesis has been recommended for younger individuals with high occupational or recreational demands. On the contrary, most RCTs on this matter refuted such findings. This meta-analysis did not demonstrate any superiority of one treatment over the other in forearm supination or elbow flexion strength at 6, 12 and 24 months postoperatively.
Regarding cosmetic outcomes in the management of the LHBT, tenotomy has been associated with significantly higher risk of Popeye’s deformity reaching up to 43%. 27 Therefore, biceps tenodesis has been recommended for reducing the cosmetic deformity. However, several surgeons have suggested techniques to circumvent the high rate Popeye’s deformity in tenotomy by minimizing the LHBT distal retraction. Such techniques described include releasing part of the superior labrum along with the LHBT 28 or by using a compressive wrap around the arm. 29 It is noteworthy that tenodesis does not eliminate the risk of Popeye’s deformity. In the trial by Oh et al., both treatments had no significant difference in the development of Popeye’s deformity with a rate of 37% for tenotomy and 26% for tenodesis. This can be attributed to tenodesis failure or inappropriate tension at the site of tenodesis. We found that tenotomy had 2.5 times the risk for developing a Popeye’s deformity compared to tenodesis which was statistically significantly.
Several limitations exist for this meta-analysis. First, the intrinsic risk of bias within the included studies cannot be adjusted. For example, two included randomized trials had a level of evidence of 2 which reduces the overall strength of this study. Second, included studies did not utilize similar outcome measures which prevented pooling more data for the CMS score and have prevented meta-analytic comparisons of other validated outcome measures. For example, our analysis at two years for the CMS score was statistically significant but not clinically relevant. This could have resulted in a clinically meaningful difference had we been able to pool more data. Third, due to limited number of studies we could not conduct meta-regression analyses based on the technique of biceps tenodesis such as suprapectoral or the subpectoral techniques, which could influence the functional outcomes or complication rates. 30 In a recent retrospective review of 1526 LHBT tenodesis cases, subpectoral tenodesis had high risk of revision when compared to tenodesis in the suprapectoral position. Moreover, soft tissue tenodesis had higher anterior shoulder pain and subjective weakness when compared with implant-based tenodesis. 31 Fourth, the length of follow-up of two years might not be sufficient to detect a difference in outcomes between both treatments.
The strength of this systematic review is that it is the first of its kind on RCTs only, thereby offering a higher level of evidence on this matter. Our results have found no significant difference on functional outcomes between both treatments which is different than previous meta-analyses. All previously published meta-analyses reported superior results in favour of LHBT tenodesis, and all were based on mixed cohort and randomized studies.5,6 Another strength to this study is that we were able to analyse functional outcomes at different time intervals from six months and up to two years of follow-up.
In conclusion, LHBT tenodesis and tenotomy are both well-established techniques that similarly yield satisfactory outcome in the treatment of LHBT pathologies. There was no difference between both techniques in terms of shoulder functional outcomes. Moreover, no difference between both techniques was found in terms of pain, elbow flexion or forearm supination strength indices. Biceps tenotomy had 2.5 times the risk for developing Popeye’s deformities when compared to tenodesis. With the current evidence, we recommend either technique for the management of the LHBT tenotomy. Given that tenodesis has shown a statistically significant but clinically irrelevant improvement in CMS at two years, further large prospective comparative studies are warranted to determine whether tenodesis truly leads to superior functional outcomes as demonstrated.
Supplemental Material
sj-pdf-1-sel-10.1177_1758573220942923 - Supplemental material for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-1-sel-10.1177_1758573220942923 for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials by Abdulaziz F Ahmed, Ammar Toubasi, Shady Mahmoud, Ghalib O Ahmed, Mohammed Al Ateeq Al Dosari and Bashir A Zikria in Shoulder & Elbow
Supplemental Material
sj-pdf-2-sel-10.1177_1758573220942923 - Supplemental material for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-2-sel-10.1177_1758573220942923 for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials by Abdulaziz F Ahmed, Ammar Toubasi, Shady Mahmoud, Ghalib O Ahmed, Mohammed Al Ateeq Al Dosari and Bashir A Zikria in Shoulder & Elbow
Supplemental Material
sj-pdf-3-sel-10.1177_1758573220942923 - Supplemental material for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-3-sel-10.1177_1758573220942923 for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials by Abdulaziz F Ahmed, Ammar Toubasi, Shady Mahmoud, Ghalib O Ahmed, Mohammed Al Ateeq Al Dosari and Bashir A Zikria in Shoulder & Elbow
Supplemental Material
sj-pdf-4-sel-10.1177_1758573220942923 - Supplemental material for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-4-sel-10.1177_1758573220942923 for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials by Abdulaziz F Ahmed, Ammar Toubasi, Shady Mahmoud, Ghalib O Ahmed, Mohammed Al Ateeq Al Dosari and Bashir A Zikria in Shoulder & Elbow
Supplemental Material
sj-pdf-5-sel-10.1177_1758573220942923 - Supplemental material for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-5-sel-10.1177_1758573220942923 for Long head of biceps tenotomy versus tenodesis: a systematic review and meta-analysis of randomized controlled trials by Abdulaziz F Ahmed, Ammar Toubasi, Shady Mahmoud, Ghalib O Ahmed, Mohammed Al Ateeq Al Dosari and Bashir A Zikria in Shoulder & Elbow
Footnotes
Contributorship
AFA and AT researched the literature. AFA performed the statistical analysis and wrote both the method and result sections. AT wrote the introduction section and submitted the manuscript through the journal portal. SM and GOA assisted in editing the discussion section. MAA and BAZ conceived the study and provided overall supervision of conducting this review. All authors reviewed and edited the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Review and Patient Consent
Not applicable.
Guarantor
AFA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.