
Abstract
Introduction
Rotator cuff tendons are typically reattached to the proximal humerus using transosseous sutures or suture anchors. Their primary mode of failure is at the tendon–bone interface.
Methods
We investigated the addition of an adhesive, gelatin–resorcin–formalin (GRF) glue, to a single-row rotator cuff repair (RCR) on ex vivo sheep models. We hypothesised the addition of GRF glue would increase the repair construct strength. The study consisted of three groups of six sheep infraspinatus tendons with an inverted-mattress stitch, tension-band configuration. Group 1 was the control group where no glue was applied. Group 2 involved applying 2 × 2 cm of GRF glue to the infraspinatus footprint and a 2-min curing time. Group 3 allowed for a 15-min cure time.
Results
Failure occurred at the tendon–bone–suture interface in 6/6 of the control group, and 4/6 from groups 2 and 3. Failure occurred via the suture pulling out of the anchor in 2/6 of groups 2 and 3. No significant differences were noted between all three groups in ultimate failure load, repair stiffness or total energy to failure (p > 0.05).
Discussion
The addition of GRF glue to the tendon–bone–suture interface did not enhance RCR strength in an ovine model.
Introduction
Rotator cuff tears (RCT) can occur in any age group, with incidence increasing with age with an overall rate reported to be between 13% and 37%. 1 These tears cause pain and loss of function. Arthroscopic surgery is the gold standard for rotator cuff repair (RCR), and surgical techniques are constantly evolving. However, re-tear rates are a common complication ranging between 11% (partial isolated supraspinatus and infraspinatus tears) and 94% (larger, full thickness, retracted, multiple RCT). 2 The primary mode of re-tear is due to weakness in the suture–tendon interface whereby sutures cut through the tendon.3–5
To address the re-tear rate, some studies have examined the use of a biological adhesive to augment RCR. In particular, one study found that the use of frog glue significantly increased the load to failure, total energy required for failure and maximum energy at failure in three different repair techniques (p < 0.01). 6 The glue was noted to be strong, flexible and could set in water. Despite its success in the laboratory, the glue did not translate well clinically due to supply issues and difficulty creating a synthetic version. 6 However, this study supports the notion that a biologic adhesive can improve RCR pull-out strength and, in turn, reduce the re-tear rate.
We hypothesised that other adhesives might demonstrate a similar performance in an RCR model to frog glue. Fibrin glue has been used in orthopaedic surgery for many years and is primarily for haemostasis; however, it has been suggested that it may have other uses, for example, in healing of ACL grafts and meniscal repairs due to its biomechanical and physiological properties. 7 Arnoczky et al. found that a fibrin clot was associated with meniscal remodelling and subsequent healing in torn ex vivo dog menisci. 8 Furthermore, the same group later showed that torn in vivo dog menisci healed significantly better with a fibrin clot applied than the control. 9 In another study, isolated meniscal tear failure rate was 41% without an exogenous fibrin clot versus 8% with the exogenous clot. 10 Additionally, a study investigating hyaline cartilage healing with a fibrin clot showed significantly more organised and advanced healing short term in an ex vivo dog model. 11 Overall, fibrin glue may be a beneficial augment with a spectrum of advantages, including potential biomechanical strengths.
Another product that has been widely used is Microval gelatin–resorcin–formalin (GRF) glue (Saint-Just-Malmont, France). Its primary indication is for cardiothoracic surgery and has shown to have a promising 5-year survival rate (81.5%) in 138 patients with acute aortic dissection with intraoperative findings demonstrating haemostatic and adhesive properties. 12
Other studies have explored the potential of GRF glue for orthopaedic surgery. In a study by Szomor et al., 13 47 ex vivo sheep menisci were repaired using four different adhesives – cyanoacrylate, frog glue, GRF glue and fibrin glue. The results showed that the cyanoacrylate had the highest total strength to failure followed by the frog glue and GRF glue. Three glues (cyanoacrylate 150 N/m, frog 100 N/m, gelatin 40 N/m) were significantly stronger than the fibrin glue (20 N/m) (p < 0.0001).
To our knowledge, GRF glue has not been examined as a potential surgical adhesive in RCR.
Aim
The aim of this study was to determine if an augmentation technique using GRF glue added to a conventional single-row inverted-mattress suture technique for RCR improved biomechanical pull-out strength at the tendon-to-bone interface compared to a conventional inverted-mattress suture technique in an ovine model.
Materials and methods
Study design
The study consisted of 36 ovine ex vivo infraspinatus tendons. After measuring tendon width (anterior to posterior) and thickness, tendons were allocated to one of three groups of 12 tendons each to ensure there were no statistical differences between groups prior to testing (p > 0.05). Group 1 consisted of two single-row inverted-mattress suture anchor repairs, and acted as the control. Group 2 had two single-row inverted-mattress suture anchor repairs that were augmented with six drops of Microval GRF glue (Saint-Just-Malmont, France), applied in between the tendon-to-bone interface according to the manufacturer’s instructions (2 ml Gelatin–Resorcin polymer, 1 ml Formalin catalyst over 5 × 10 mm area). The glue was allowed to cure for 2 min before biomechanical testing. Group 3 was prepared identically to Group 2 except the glue was allowed to cure for 15 min before biomechanical testing. Group 3 was included as it was hypothesised in a wet-lab environment that curing time may be a confounding factor.
Ovine rotator cuff tear model
An ovine chronic rotator cuff tear ex vivo model was developed to simulate a torn rotator cuff in accordance with our institute’s previous studies. 14 Ovine infraspinatus tendon has been previously used in our laboratory as a well-established ex vivo model for assessing RCR techniques. 15 The infraspinatus from ovine shoulders were harvested and attached muscles were excised. In order to simulate in vivo human cuff repairs, there was imitation of debridement in actual surgery via 5 mm excision of torn tendon edges to create an even edge. All groups received two horizontal inverted-mattress sutures inserted 1 cm medial to the lateral edge of the tendon using a suture passer (Scorpion Suture Passer, Arthrex Inc., Naples, FL, USA) using #2 FiberWire (Arthrex Inc. Naples, FL, USA) with the suture limbs 4.5 mm apart. The tendons were then reattached to bone using 5.5-mm knotless suture anchors (SwiveLock C, Arthrex Inc., Naples, FL, USA), and then allocated to one of the three experimental groups.
After allocation and application of adhesive for groups 2 and 3, the constructs were pulled to failure using a mechanical tensile testing machine (Instron 8874, Instron Ltd, UK).
The glue
A 2 × 2 cm, 0.2-mm thick layer of Microval GRF glue (Saint-Just-Malmont, France) along with six drops of glue hardener was applied to the tendon-to-bone interface in all specimens in groups 2 and 3. Group 2 was allowed to cure for 2 min before biomechanical testing whereas group 3 cured for 15 min before testing.
Rotator cuff repair technique
The tension band repair was performed using two 5.5-mm knotless suture anchors (SwiveLock C, Arthrex Inc, Naples, FL, USA). Prior to placing the anchors, two inverted-mattress sutures (FiberWire) were passed through the infraspinatus 13 mm medial to the torn edge of the tendon using a suture passer (Scorpion Suture Passer, Arthrex Inc. Naples, FL, USA). Two pilot holes were created in the proximal humerus 5 mm lateral to the infraspinatus footprint with a 4.5-mm diameter punch (Arthrex Inc, Naples, FL, USA). The free ends of each inverted-mattress suture were delivered over the tendon and through an eyelet of a knotless anchor forming a tension band construct. Each knotless anchor was placed in the appropriate pilot hole and locked into bone. The suture was tensioned until the tendon was reduced over the bony footprint, then the anchor was screwed into the bone for fixation.
Biomechanical testing
After tendon repair to bone with or without application of adhesive, all tendons were kept moist with normal saline solution. The free ends of the tendons were clamped to the material testing machine. The clamps were lined with sandpaper to improve grip. Pull to failure tests were performed using a mechanical tensile testing machine (Instron 8874), as previously described in Andres et al. 5 Specimens were preloaded with 10 N for 30 s. Following this, specimens were pulled at 1.25 mm/s to failure with the data captured at 100 Hz on a computer. The modes of failure were recorded for each specimen using a charged-coupled device camera.
Stiffness of the repair was calculated from the linear section of the load–displacement curve with MATLAB software (R2009; The MathWorks, Natick, MA, USA). Tendon displacement was obtained from clamp-to-clamp displacement. The total energy to failure was calculated from the area under the load displacement curve. This area is calculated by the use of trapezoid numerical integration with MATLAB software (R2009).
Statistical analysis
Differences between groups were analysed using unpaired Student’s t-tests for continuous variables.
Results
Footprint dimensions and tendon thickness
Specimens in the three repair groups were well matched in footprint dimensions and tendon thickness. In comparison between groups, Student’s unpaired t-tests revealed no significant difference between each group (p > 0.05).
The mean anterior–posterior length of the specimens used in the control group was 20 mm (SEM ± 0.99 mm) and the mean medial–lateral length was 12 mm ( ± 0.73 mm).
The mean anterior–posterior length of the specimens used in the 2 min glue group was 21 mm (SEM ± 0.54 mm) and the mean medial–lateral length was 13 mm ( ± 0.51 mm).
The mean anterior–posterior length of the specimens used in the 15 min glue group was 22 mm (SEM ± 0.43 mm) and the mean medial–lateral length was 13 mm ( ± 0.23 mm).
Biomechanical testing
The primary mode of failure for the control group was via the suture cutting through the tendon (6/6, 100%). In both groups 2 and 3, 33% (2/6) failed via the suture pulling out of the anchor and 67% (4/6) failed via the suture cutting through the tendon.
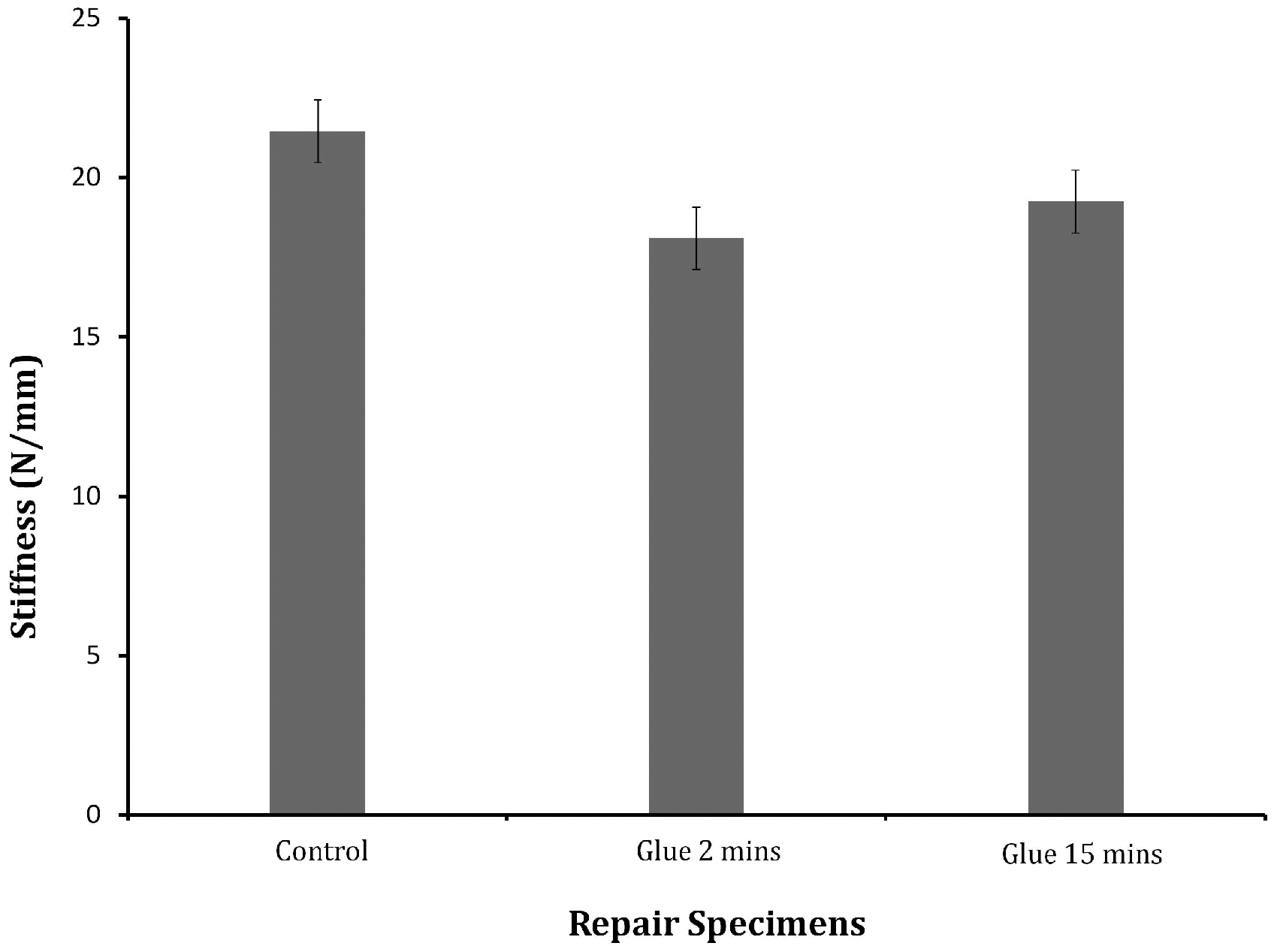
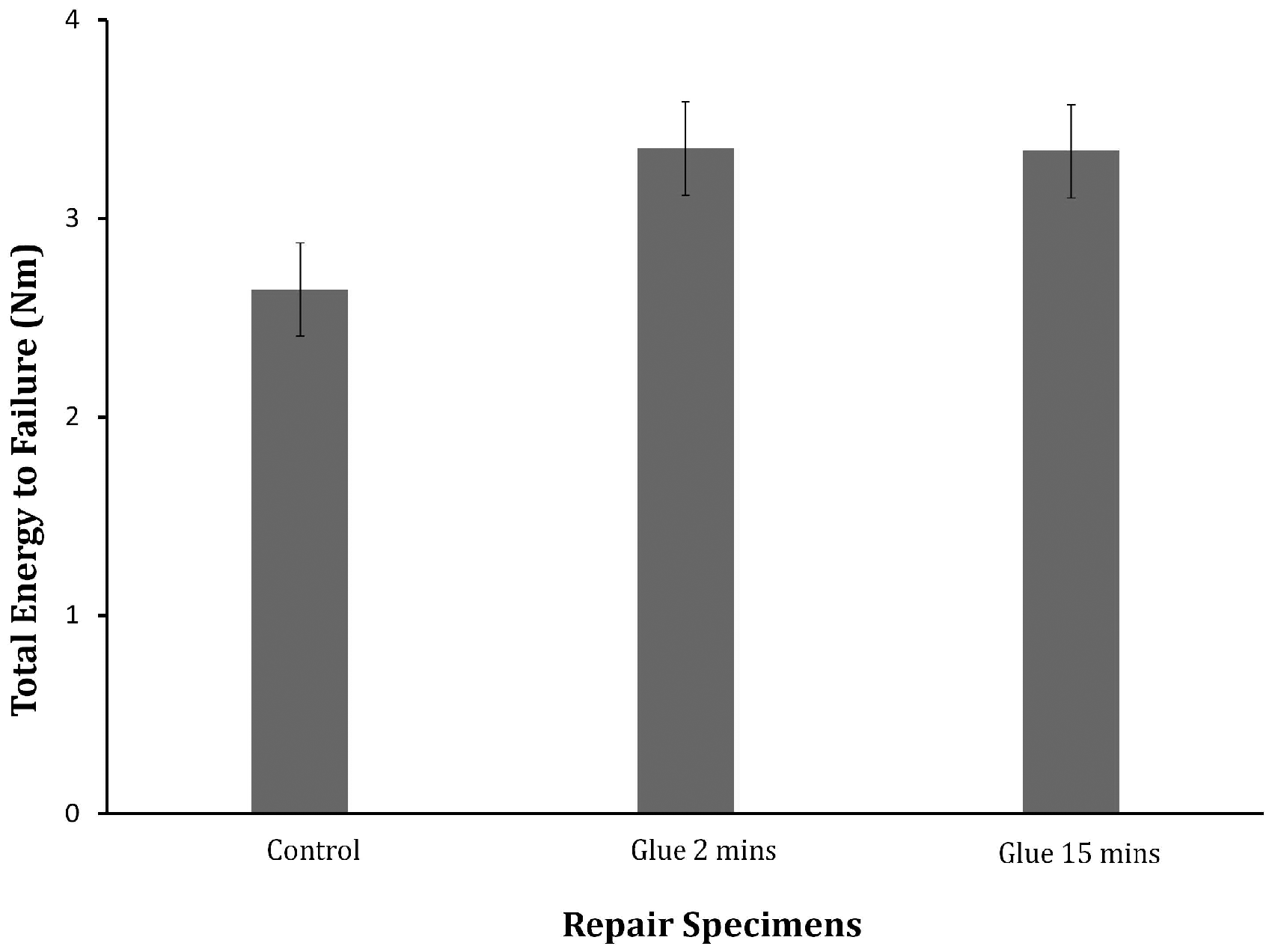
No significant differences were noted between all three groups in ultimate failure load with the highest load being group 2 (216 ± 31 N, p > 0.05) (Figure 1), in repair stiffness with the highest stiffness occurring in the control group 1 (21 ± 3 N, p > 0.05) (Figure 2), or in total energy to failure with the highest value occurring in group 2 (3 ± 1 N; p > 0.05) (Figure 3).
Ultimate failure load (N). Graph showed mean ± SEM (unpaired Students’ t-test). Repair stiffness (N/mm). Graph showed mean ± SEM (unpaired Students’ t-test). Total energy to failure (Nm). Graph showed mean ± SEM (unpaired Students’ t-test).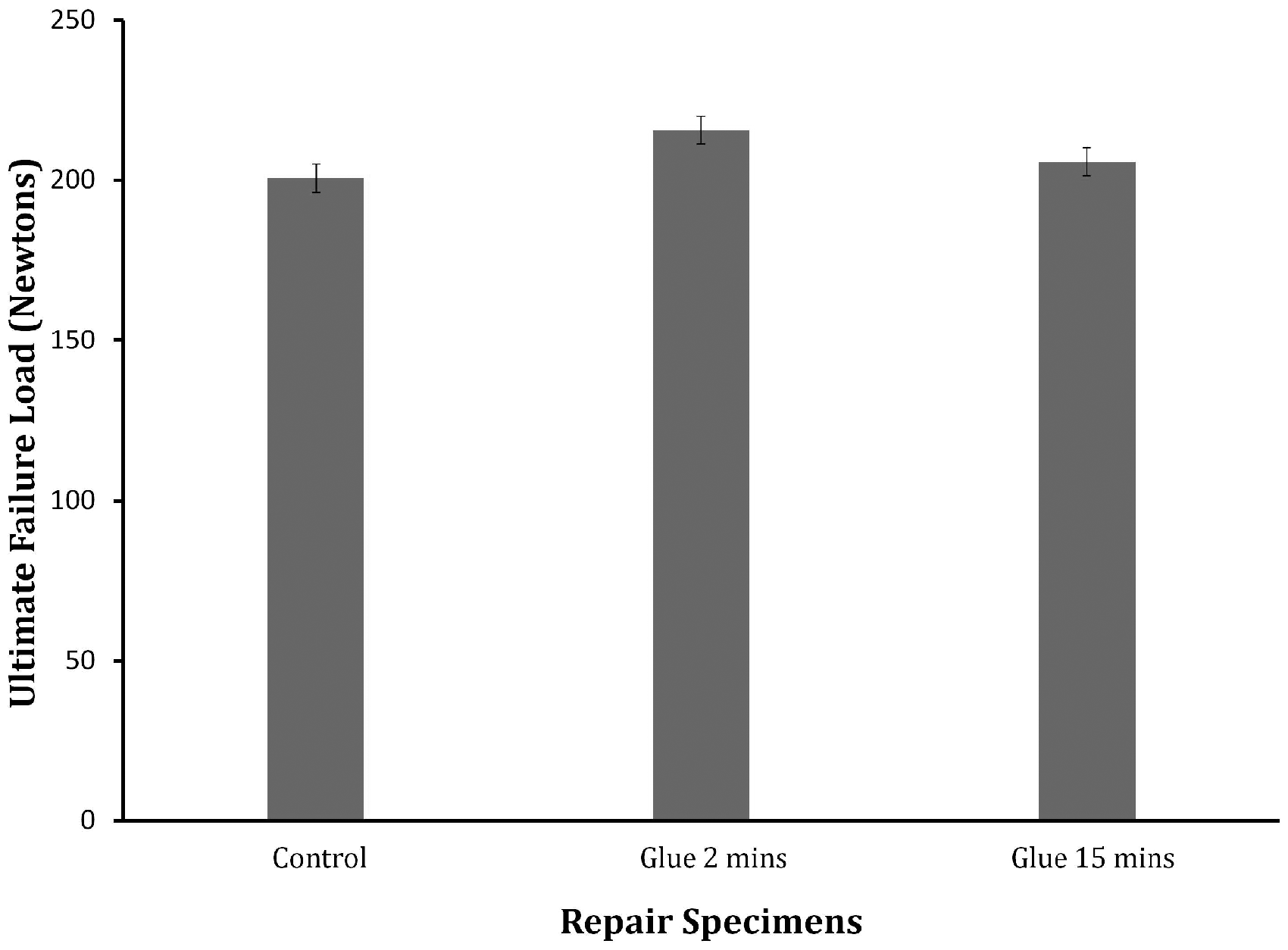
Discussion
This study explored the use of a biological adhesive to augment a conventional RCR and its effects on repair pull-out strength. The results demonstrated no significant difference between augmented repairs and the control group.
Previously, a study examining augmentation of RCR with frog glue improved pull-out strength (Millar et al. 6 ). However, this adhesive has yet to be developed commercially in a sustainable, biocompatible form. Our study aimed to recreate the adhesive effects of frog glue using a product already approved for use in humans. Despite being safe and readily available, the GRF glue lacked the higher degree of adhesion seen in frog glue.
Another study examined the effect of increased footprint contact pressure on RCR integrity (Andres et al. 5 ). They found that an increased footprint contact pressure, along with strength of suture configuration, improved outcome of RCR. Our study only investigated pull-out strength of the repairs; however, it is possible that the glue played a role in augmentation of footprint contact pressure and priming of the tendon–bone interface for healing. Further study is needed to determine the role glue might play in altering footprint contact pressure.
The strengths of this study were a standardised methodology including protocol for dissection and preparation of ex vivo sheep specimens, instrumentation in preparing specimens, a standardised glue application technique, measuring pull-out strength, and blinded repairs and random sampling to reduce researcher bias.
The limitations of this study were that we were using ex vivo sheep models which are not live, human shoulders. Secondly, these specimens were absent of healing processes and coagulative processes seen in live subject shoulders.
In conclusion, it is clear from previous studies that augmentation of RCRs with glue can be an effective method for improving pull-out strength of a repair at time zero; however, currently the only statistically efficacious glues tested are cytotoxic or unavailable for logistical reasons. Our study examined the effect of augmentation of RCR using GRF glue as it is non-toxic to the body and readily available. Results revealed that repairs augmented with glue did not have superior biomechanical pull-out strength to conventional repairs. Further study is required to examine the role of GRF glue in regards to other properties important for successful RCR such as capacity to propagate healing and enhancement of footprint contact pressure. Concurrently, identifying other potential adhesives for augmentation of RCRs may be helpful in reducing RCR failure rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Review
This was an ex vivo animal study and does not require ethics approval in our healthcare system.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
WJM.
ORCID iDs
William J McNamara https://orcid.org/0000-0002-7524-2325 Patrick H Lam https://orcid.org/0000-0001-6196-1794 George AC Murrell ![]()