
Abstract
Background
Elbow and forearm motion are thought to affect elbow load transmission, yet little empirical evidence exists to quantify the biomechanics.
Methods
Eight fresh-frozen human cadaver upper extremities were utilized. A 100 N axial force was applied across the elbow joint at elbow flexion angles of (0°, 30°, 60°, and 90°) and forearm rotation angles (0°, 45° supination, and 45° pronation). Pressure mapping sensors were placed in both the radiocapitellar and ulnotrochlear joints. Force distributions and contact areas were measured, and paired t-tests were used for comparison (p < 0.05).
Results
The average maximum loading percentage of the radiocapitellar and ulnotrochlear joint pressures were 57.8 ± 4.6% and 42.2 ± 4.6%, respectively. Elbow flexion angle and forearm rotation did not significantly affect the joint loading. There was no significant difference between the contact areas of each joint, although ulnotrochlear and radiocapitellar joints demonstrated an inverse relationship.
Conclusion
Our study is the only one to date to comprehensively evaluate loading mechanics throughout both functional elbow flexion and forearm rotation across both articulations. The load sharing ratio across the radiocapitellar and ulnotrochlear joints was 58%:42%, agreeing with previously reported ratios with limited parameters. A relationship may be present between increasing radiocapitellar and decreasing ulnotrochlear contact areas as elbow flexion increases.
Introduction
The complexity of axial load distribution from the hand, through the wrist and forearm, and across the elbow has yet to be fully defined. Force transmission through the forearm is a complex interplay of forearm position, wrist anatomy, radioulnar soft-tissue attachment, and elbow alignment. 1 A single milestone study published in the 1960s established that 57% and 43% of axial load was transmitted through the radiocapitellar and ulnotrochlear joints, respectively. 2
However, in the past 60 years, little additional attention has been given to load distribution across the elbow. A few research groups have focused on the effect of forearm rotation on force transmission across the radiocapitellar joint. Using a cadaveric elbow model, Morrey and Stormont 3 evaluated force transmission throughout forearm rotation at varying degrees of flexion, concluding that elbow extension transmits the greatest force across the radiocapitellar joint, and forearm pronation relays a higher load, independent of flexion. The Van Riet group found increased pressure across the radiocapitellar joint with forearm pronation. 4 Hwang et al. demonstrated the radial head is susceptible to injury in pronated positions. 5 However, in contrast to previous studies, comprehensive evaluation of loading mechanics across both the native ulnotrochlear and radiocapitellar joints simultaneously throughout the entire functional range of elbow flexion and forearm rotation to accurately represent in vivo conditions has not been conducted.
To our knowledge, there have been few studies to date that have fully assessed both ulnotrochlear and radiocapitellar joint loading biomechanics throughout the functional range of elbow motion and forearm rotation. The aim of this study was to quantify axial loading biomechanics across both the native radiocapitellar and ulnotrochlear joints as originally described by Halls and Travill 2 and establish force transmission and contact area biomechanics of forearm rotation across a comprehensive range of varying degrees of elbow flexion using a custom loading apparatus and pressure-sensitive film. We hypothesize that load distribution and contact area across the elbow will be directly affected by elbow flexion angle and forearm rotation.
Methods
Eight intact fresh-frozen human cadaveric arms from donors (four male/four female, age at death: 53 ± 15, height: 66 ± 3, Body mass index: 23.0 ± 3.9, race/ethnicity: four Caucasian, two African-American, two Hispanic) were thawed to room temperature. Skin, adipose, and muscle tissue were removed from the humerus to the wrist, and the humerus was cut 15 cm from the elbow joint and rigidly fixed in a custom potting jig. The hand was kept intact for the entire testing session to better replicate in vivo conditions. A small transverse anterior arthrotomy was made to enable the insertion of pressure sensors described below. A saline solution was used throughout testing to ensure the specimens remained moist.
Pressure-sensitive film (Pressure Mapping Sensor 4041, 0.178 mm thickness, two separate 12.7 mm ×31.5 mm sensing areas, Tekscan, South Boston, MA) was first calibrated and preconditioned per manufacturer recommendations and then inserted into the radiocapitellar and ulnotrochlear joints to record pressure of the joints throughout testing. There are 90 sensels (individual units of pressure-sensitive ink) per tab (22.8 sensels/cm2), and the Tekscan sensor has been previously validated for contact pressure between two round surfaces with numerous areas of contact.6–9 A custom loading jig was used to hold the cadaveric specimens in 12 different configurations. At each of four elbow flexion angles (0°, 30°, 60°, and 90°), forearm rotation angles were fixed at 45° supination, neutral, or 45° pronation with the wrist extended at 90° (Figure 1). A 100 N compressive load was applied for 30 s (MTS, Eden Prairie, MN) while the pressure data were recording (50 Hz). Tests were performed in a random order for each specimen.
Experimental photos showing the entire setup (left) and a close up of the elbow joint with pressure sensors in the radiocapitellar and ulnotrochlear joints (right).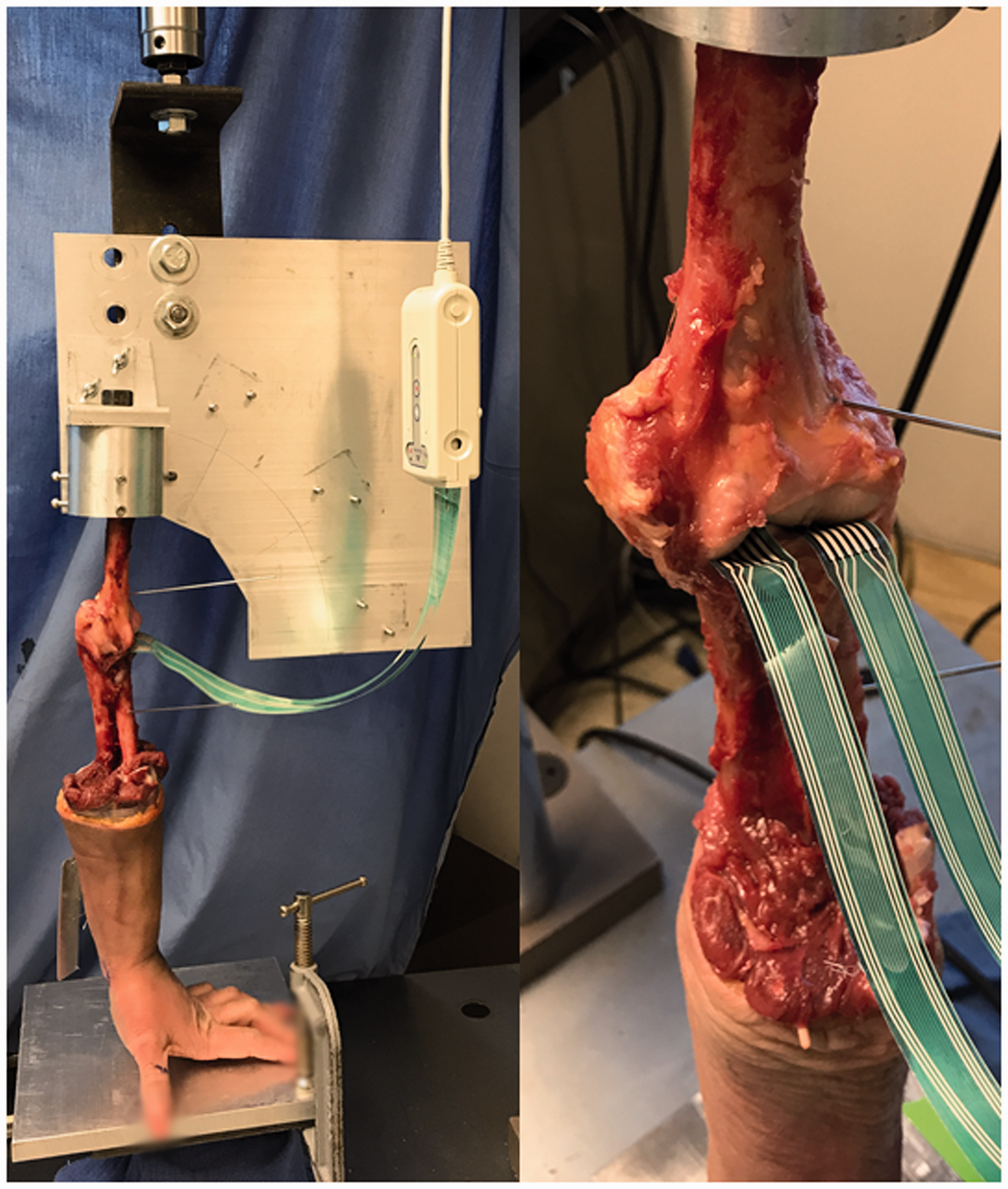
Data were exported to Excel (Microsoft, Redmond, WA). Via custom code (Matlab, Natick, NJ), mean forces were calculated for each joint and presented as a percentage of the total force recorded for both joints, and the contact area recorded during each frame of testing was averaged for each 30 s testing session for each joint. Two-way MANOVAs were used to determine differences between loading ratios and contact areas in the two joints due to flexion angles and wrist rotation angles (p < 0.05). Post hoc one-way ANOVAs and paired t-tests were used to compare data between flexion angles and wrist rotation angles. Because of the sample size and variable nature of cadaveric testing, it will be noted when p < 0.10.
Results
All specimens were able to withstand testing in all 12 configurations. However, accurate pressure data were not recorded for 15% of trials due to various experimental complications (sensors moving during testing and sensors malfunctioning), and those trials were excluded from the analyses.
Force distribution
With all testing conditions considered, statistically significant differences between the radiocapitellar and ulnotrochlear joints were found in the loading ratio (mean ± standard error: 57.8 ± 4.6% radiocapitellar and 42.2 ± 4.6% ulnotrochlear, p < 0.001).
The data were analyzed both with respect to differences in loading due to forearm rotation at each elbow flexion angle, and with respect to differences in loading due to flexion angle at each forearm rotation. Without considering elbow flexion angle, the loading ratio of the radiocapitellar vs. ulnotrochlear joint in the supinated, neutral, and pronated conditions was not affected by forearm rotation angle (p > 0.05). Similarly, without considering forearm supination angle, the loading ratio of the radiocapitellar vs ulnotrochlear joint was not significantly impacted by elbow flexion angle (Figure 2, p > 0.05). Post hoc paired comparisons found no significant difference in loading distribution between the two joints for any two flexion angles or two forearm angles (p > 0.05).
Radiocapitellar load distribution as a percentage of the total loading at each elbow flexion angle, grouped by forearm rotation angle (mean + standard error). No differences were found between any conditions (p > 0.05).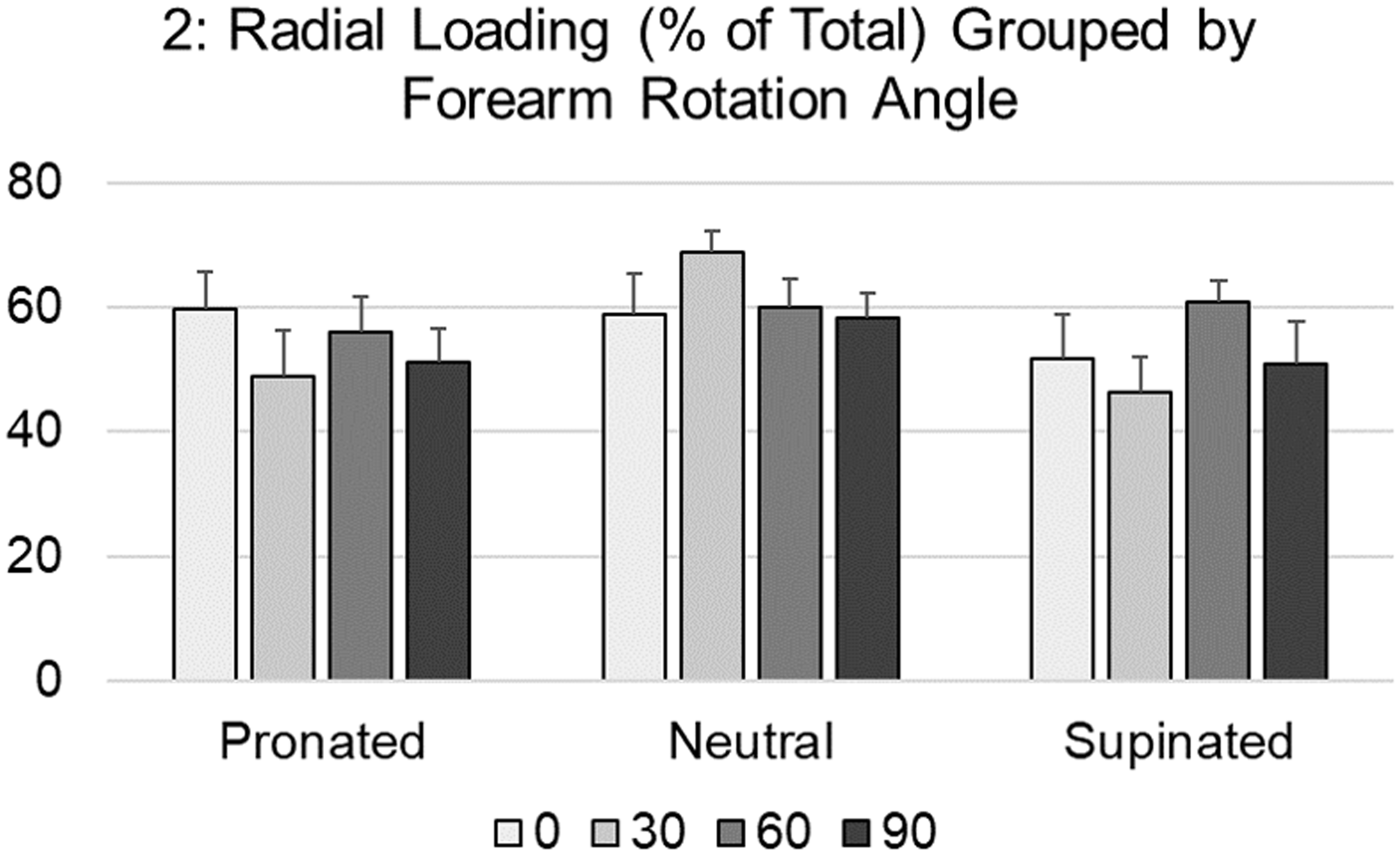
Contact area
With all testing conditions considered, no difference was found in the contact areas of the two joints (mean ± standard error: 76.0 ± 9.7 mm 2 radiocapitellar and 77.0 ± 11.8 mm 2 ulnotrochlear, p > 0.05).
Forearm rotation effect on contact area
No effects due to forearm rotation were found on the ulnotrochlear joint (Figure 3(a)). When data from all elbow flexion angles were combined, the radiocapitellar joint had a larger average contact area in forearm pronation (81.6 ±9.7 mm2) compared to supination (67.5 ± 6.8 mm2; p = 0.0483, Figure 3(b)). Specifically, at a 30° elbow flexion angle, the radiocapitellar joint experienced higher contact areas in pronation (87.8 ±10.4 mm2) compared to supination (65.2 ± 8.8 mm2; p = 0.050).
Ulnotrochlear (a) and radiocapitellar (b) contact area at each forearm rotation angle, grouped by elbow flexion angle (mean + standard error). With all flexion angles considered, the radiocapitellar joint had a 21% larger contact area in forearm pronation vs supination (p = 0.0483). *p < 0.05.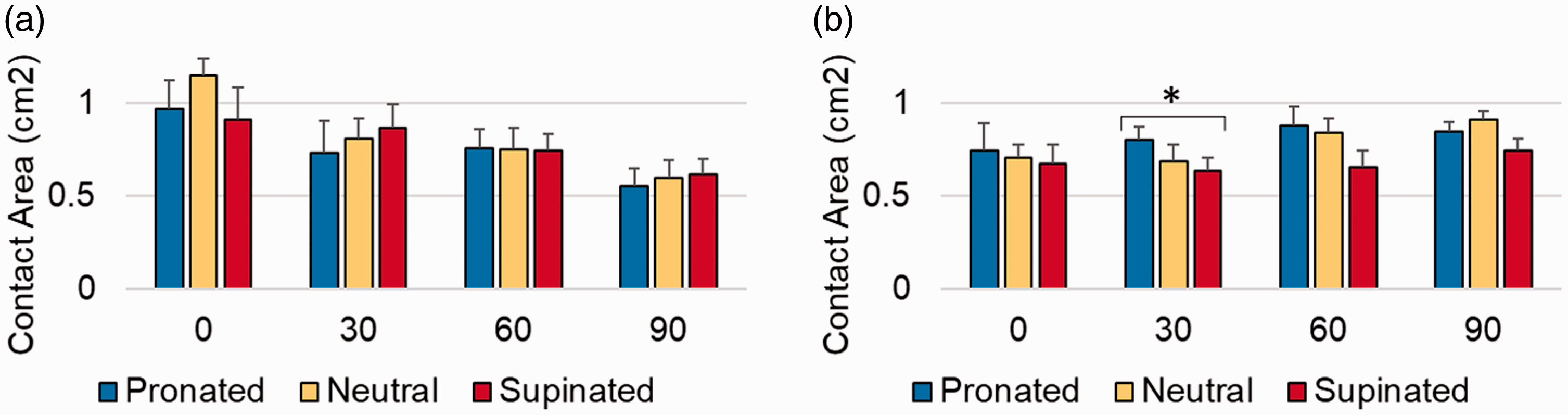
Elbow flexion angle effect on contact areas
When data from all forearm rotation angles were combined, the ulnotrochlear contact area significantly decreased as elbow flexion increased (0°: 101.0 ± 13.8 mm2, 30°: 80.0 ±10.5 mm2, 60°: 75.0 ± 10.1 mm2, 90°: 58.8 ± 7.4 mm2, p = 0.006, Figure 4(a)). Specifically, in the neutral forearm position, the ulnotrochlear contact area tended to decrease with increasing elbow flexion over all flexion angles (p = 0.058). Similarly, with a supinated forearm, the ulnotrochlear contact area was nearly 30% less at a 90° elbow flexion angle compared to a 30° elbow flexion angle (p = 0.044).
Ulnotrochlear (a) and radiocapitellar (b) contact area at each elbow flexion angle, grouped by forearm rotation angle (mean + standard error). With all forearm rotations considered, ulnohumeral contact area decreased with increasing elbow flexion (p = 0.006). Radiocapitellar contact area was only affected by elbow flexion angle in the neutral forearm position (p < 0.05). *p < 0.05 and †p < 0.10.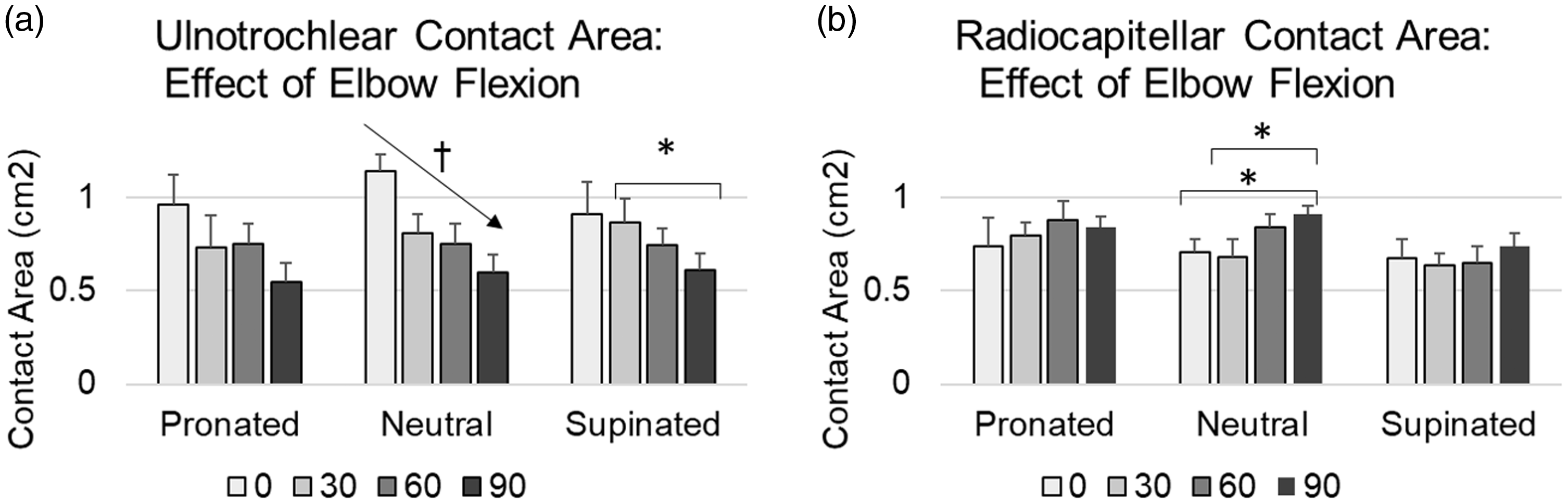
Conversely, when considered as a group, radiocapitellar contact area did not show a significant change due to flexion angle (p > 0.05, Figure 4(b)). However, in the neutral forearm position, the radiocapitellar contact areas were 50% greater at a 90° flexion angle compared to both the 30° (p = 0.062) and fully extended 0° conditions (p = 0.086).
Discussion
Understanding the loading biomechanics of the elbow has long been an area of interest. Previously, it has proved difficult to accurately assess dynamic loading pressures across the joint surfaces throughout the range of functional elbow flexion and forearm rotation. With improved technology and established techniques, we were able to more fully assess joint loading and load sharing across the radiocapitellar and ulnotrochlear joints of the elbow.
Load sharing
The load sharing ratio across the radiocapitellar and ulnotrochlear joints throughout the range of elbow flexion and forearm rotation was 58 ± 4.6%:42 ± 4.6%, respectively. Our results regarding load distribution agree with prior studies in elbow extension and neutral forearm rotation.2,5 There was no difference in load distribution across either joint throughout varying degrees of elbow flexion or forearm rotation (p > 0.05).
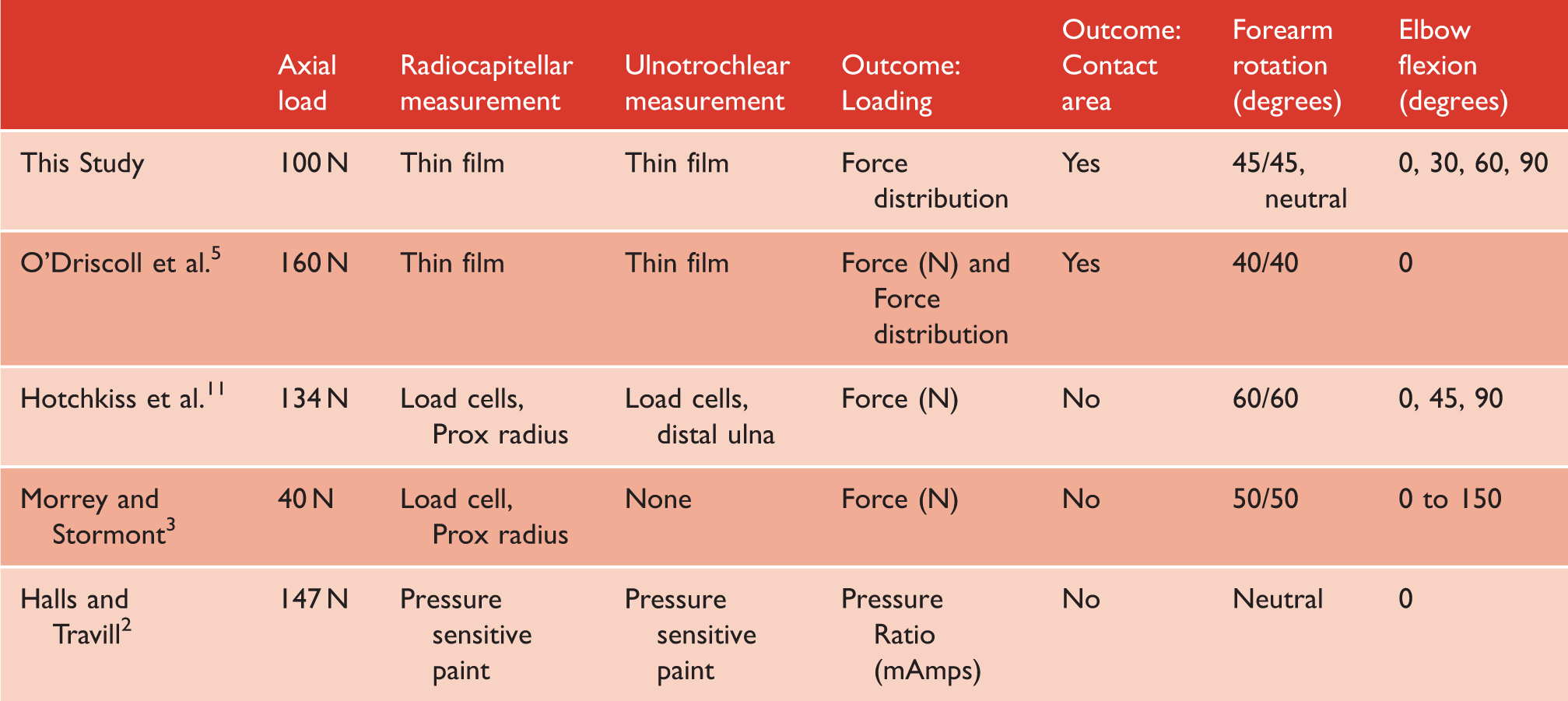
Summary of relevant studies that explore loading of the radiocapitellar and ulnotrochlear joints.
Contact area
No significant difference was observed in contact areas between each joint. With respect to all positions of forearm rotation, the ulnotrochlear contact area decreased with increasing elbow flexion. We postulate this may be a result of difference in articular morphology. Radiocapitellar contact area was 21% greater with forearm pronation relative to other positions. This finding agrees with previous studies that found increased contact area with increasing forearm pronation1,5 specifically with the influence of forearm rotation on fracture patterns in traumatic elbow injuries. 13 At 90° of elbow flexion, the greatest radiocapitellar contact area occurred in neutral rotation, which corresponds to the results of Shannon et al. 14 Forearm rotation had no effect on the ulnotrochlear contact area. Furthermore, an association may be present between increasing radiocapitellar and decreasing ulnotrochlear contact areas as elbow flexion increases. Many previous studies have focused evaluation on limited areas of flexion, rotation, or loading of the elbow. This study further expands on those results by using a more complete cadaveric model.
Strengths and limitations
Strengths of this study include the use of intact native cadaveric elbows including the entire distal extremity in order to more accurately replicate physiologic loading from the hand, through the forearm, and across the elbow. This contrasts previous studies where the extremity was amputated through the radiocarpal or carpometacarpal joints and potted. 5 Additionally, an olecranon osteotomy was not performed, and the elbow joint was not manipulated with the exception of an anterior capsular arthrotomy for sensor insertion.
Our cadaveric study has inherent limitations. Firstly, the cadaveric model is a close replica but tissue characteristics in vitro behave differently than in vivo. Also, the low sample size common in cadaveric studies may result in insufficient power to detect a significant difference in various testing conditions. The sensors utilized which allowed for dynamic assessment retain limited pliability and thus may not anatomically conform to joint surfaces or adequately capture the entire surface contact areas. Finally, due to the anatomy of the elbow articulations, it is plausible that the sensors may experience minor amounts of migration or position changes throughout testing.
Conclusion
In conclusion, our study agrees with and builds upon previous investigations examining the load sharing ratio of 58%:42% for the radiocapitellar and ulnotrochlear joints. However in contrast to previous studies which have evaluated limited aspects of elbow loading mechanics with regard to elbow flexion or forearm rotation, this investigation was the first conducted to comprehensively evaluate the loading mechanics across both the native ulnotrochlear and radiocapitellar joints simultaneously throughout the entire functional range of elbow flexion and forearm rotation in order to accurately represent in vivo conditions. Establishing a compendious baseline of loading parameters across the native elbow articulations enables accurate comparison for further work evaluating the effects of surgical procedures altering native elbow structure. Future work should evaluate the biomechanical impact of radial head arthroplasty and other common surgeries involving the radiocapitellar and ulnotrochlear joints, including load distribution and contact area.
Footnotes
Acknowledgements
The authors would like to thank BC for his assistance in facilitating this study.
Contributorship
SA assisted with study conception, design, specimen preparation, and trialing. KS and JS performed literature review, specimen preparation, and trialing. ES was responsible for study protocol, trialing, and data analysis. All authors reviewed and edited the manuscript and contributed to revision and approval of the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Funding
Acumed educational grant: K002704-00-S002 and NIH grant P20GM125503.
Guarantor
SA.