
Abstract
Introduction
Indications for surgical management of displaced humeral shaft fractures are not clearly established, leading to variations in practice. The aim of this study was to determine the scale of these variations in the UK practice to help design a future national trial.
Methods
An online survey was sent to all surgeon members of British Elbow and Shoulder Society to help define humeral shaft fractures, fracture displacement as well as indications for operative and non-operative management. Patient and injury related factors considered important when managing humeral shaft fractures were investigated.
Results
The survey achieved a response rate of 32% (104/327). There was a lack of consensus on definitions for humeral shaft fractures and fracture displacement. A functional brace was the most common form of non-operative treatment (63%). Majority immobilise humeral shaft fractures for 4–8 weeks or until callus are visible (62%) with a similar number considering operative treatment if adequate signs of healing are not present at around 12–16 weeks. Around half of our respondents exclusively use plates with variations in preference of approach and a minority (2%) exclusively use intra-medullary nails.
Conclusion
The significant variation in management of displaced humeral shaft fractures in the UK suggests a clear need to evaluate clinical and cost effectiveness through a multi-centre randomised trial.
Introduction
Humeral shaft fractures (HSFs) are common injuries and account for approximately 3–5% 1 of all fractures and 20% of all humeral fractures in adults.1,2 Closed HSFs have traditionally been treated non-operatively with immobilisation in either a plaster or a functional brace.3–5 There has been a steady increase in the rate of surgery over last few decades for displaced fractures despite there being limited evidence to support superior outcomes over non-operative treatment.4,5
Surgery is generally indicated for polytrauma, 6 segmental fractures, 7 open fractures or those with a vascular injury. It may also be indicated for a progressive radial nerve palsy or when a trial of non-operative treatment has failed. There are also relative indications and various surgical options ranging from plating using anterior or posterior approaches and intra-medullary nailing. 8 It is unclear which displaced fractures are likely to suffer nonunion. The optimal surgical treatment remains controversial and there are benefits as well as limitations to each of the available options. 9 There remains considerable variation in current practice.
The aim of this survey was to identify current UK clinical practice relating to displaced HSFs. We were particularly interested in the proportion of patients that are treated surgically, what factors are important in surgical decision making and how the surgery is performed. These questions are increasingly important as the rate of surgery for HSFs continues to rise 10 despite the scarcity of good evidence and variations in practice can only be addressed once they have been recognised.
Methods
A survey was developed to meet the study aim to study the factors affecting variations in decision making of surgeons when treating patients with displaced humerus shaft fractures and to help define the different arms of a future randomised trial by including questions to help define HSFs, displacement and patient characteristics important for decision making.
Firstly shaft (middle third) of humerus fractures was defined using anatomical landmarks and the parameters for displacement were outlined (Supplementary material). Patient and injury related factors important in decision making for choice of operative and non-operative treatment were explored with a separate question which included options such as body mass index (BMI), macromastia, multiple long bone fractures, nerve or vessel injury, open fractures, patient choice, smoking and diabetes. To determine what is considered the standard non-operative treatment further questions were posed about mode of immobilisation used for non-operative management, variations in length of immobilisation and length of time clinicians prefer to immobilise when treating non-operatively before they would be classified as a non-union and surgery would be advised. In the next section we aimed to find out more about current surgical practice. To do this we asked about the proportion of patients with HSFs that they treat surgically and the approach as well as fixation method they commonly employ.
The survey was initially trialled within the department with four surgeon members of the upper limb team before submitting the survey for consideration to the British Elbow and Shoulder Society (BESS) scientific committee. Once approved, all surgeon members of the BESS were invited to participate in an online survey (Supplementary material) using the Qualtrics software. No minimum number of responses were required, and the response rate calculated based on number of responses and the BESS membership at the time. Duplicate answers were excluded automatically using the Qualtrics software. Qualtrics software tracks responses by IP address and the location of device used for the response and we have not noticed multiple responses from the same IP address or location. A post-hoc power analysis assuming a 15% rate of non-contactable members (out of a total 327 BESS surgeon members), confidence intervals of 80% and a type 1 error rate of 5% suggested the appropriate sample size to be between 104 and 106. Descriptive analysis was used to summarise findings of the survey. The invitation email was first distributed on 2 March 2018 and following reminders the survey closed on 30 June 2018. Ethical approval was not required for this study.
Results
A total of 104 (32%) responses were received from 327 (2017–2018) surgeon members of BESS. No demographic data about the responders were collected. A number of questions allowed multiple answers and therefore the number of responses for some questions were higher than 104. In terms of defining the fracture of middle third of the humerus there was a lack of consensus between our responders. The most common definition selected (n = 36, 35%) was that a fracture anywhere between the surgical neck to 5 cm above the elbow joint would be defined as fracture of shaft of humerus. The second most selected definition by 29 respondents (28%) was a fracture between the lower border of pectoralis major tendon attachment to a line drawn 5 cm above the elbow joint. The other definitions were less commonly selected with 19 respondents (18%) selecting superior border of pectoralis major to 7 cm above the elbow, 16 respondents (15%) considering it extending from the superior border of pectoralis major to a line 5 cm above the upper border of olecranon fossa and another 16 (15%) defining shaft fractures according to Müller’s squares. This is where the shaft lies between the proximal and distal segments of long bones which themselves are considered to lie inside a square with sides being the same length as the widest part of the epiphysis. 11
The second question about what constitutes a displaced HSF also garnered a variety of responses with 104 respondents returning 217 responses. Fifty-seven per cent of respondents considered displacement to be when there was no contact between the proximal and distal fracture fragments. In transverse fractures, diastasis amounting to the thickness of the humeral cortex was considered displaced by 15% of respondents, half the width of humerus by 26% and the full width by 57%.
Forty per cent of respondents treat between 20 and 50 patients with HSFs a year and another 40 per cent treat less than 20 a year. Only a small number (13%) treat between 50 and 75 fractures a year. This data will help estimate the possible recruitment rate per site for feasibility planning in a multi-centre national trial. The next question dealt with the proportion of patients with displaced HSFs that are treated operatively. Around half of the respondents operate on less than 25% of these patients with displaced fractures but there is variation amongst surgeons as a quarter of them responded that they are operating on more than 50% of displaced fractures (Figure 1).
Proportion of patients with displaced HSFs treated operatively.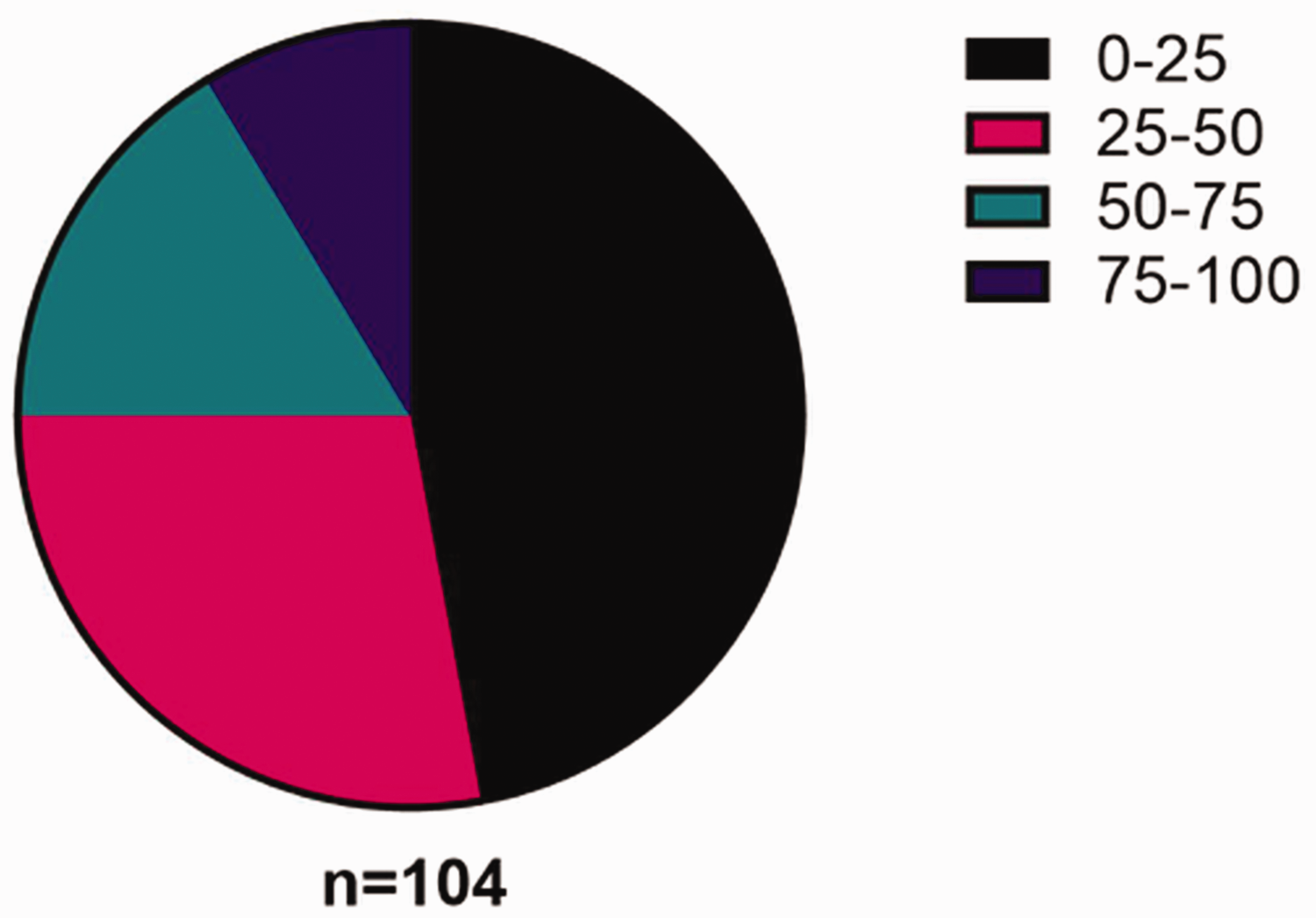
The most important factors considered by our respondents when recommending surgery were open fractures (97%), polytrauma (92%), associated nerve or vessel injury (87%) and patient choice (68%). With multiple selections allowed we had 562 responses for factors deemed important in deciding between surgery and non-operative management. Other factors such as a high BMI and macromastia were also considered to be relatively important (Figure 2).
Factors considered important in surgical decision making for humeral shaft fractures.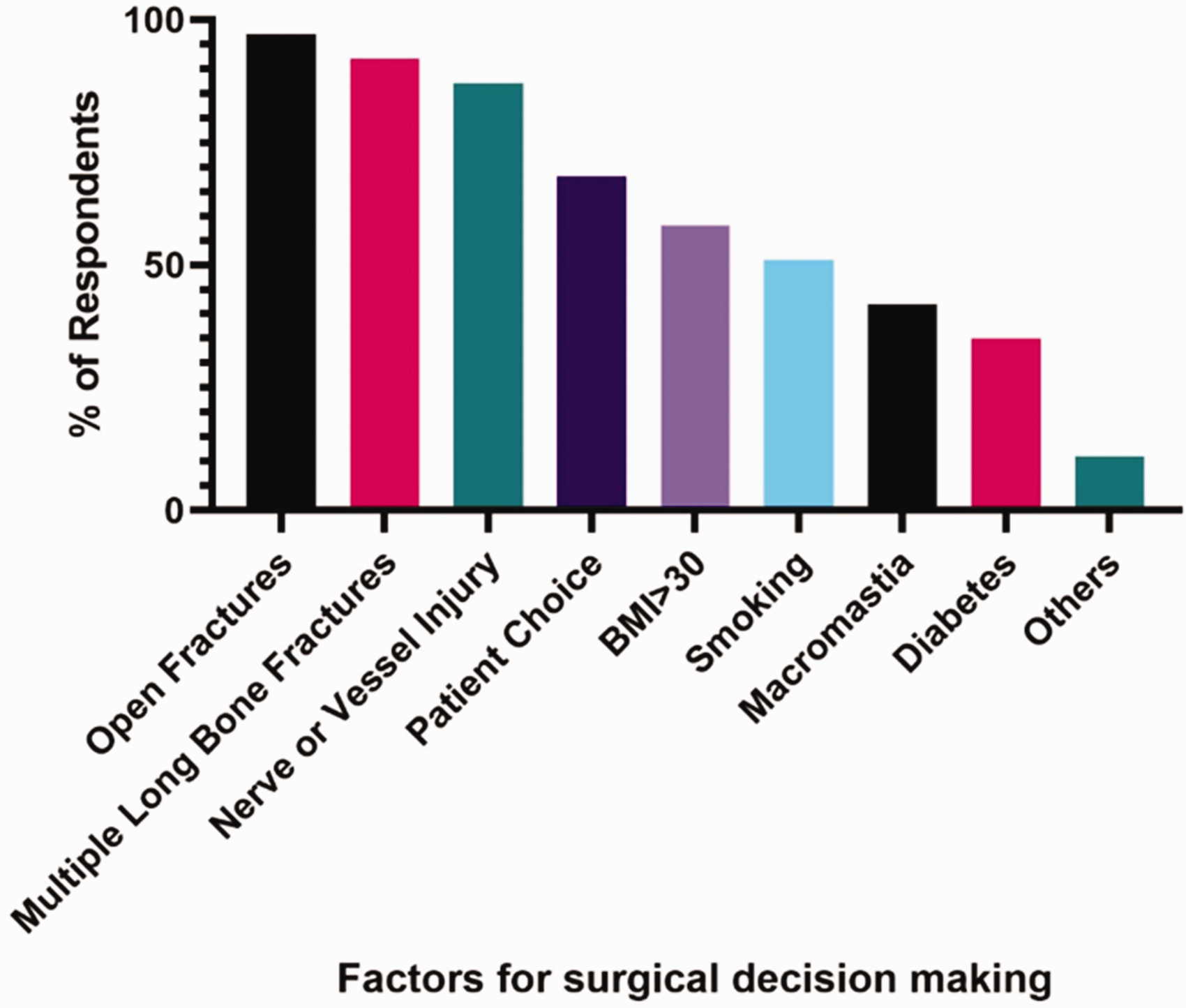
Most respondents when treating HSFs non-operatively would choose to use a humeral brace alone (n = 65, 63%) whilst the remaining chose to initially treat with plaster immobilisation followed by a brace (n = 35, 34%). The preferred length of immobilisation once again highlighted variations in practice with no single response taking the majority. The most common response was immobilisation for 4–8 weeks (n = 34, 33%) closely followed by immobilisation till callus being visible on radiographs (n = 30, 29%; Figure 3).
Length of immobilisation for non-operative treatment.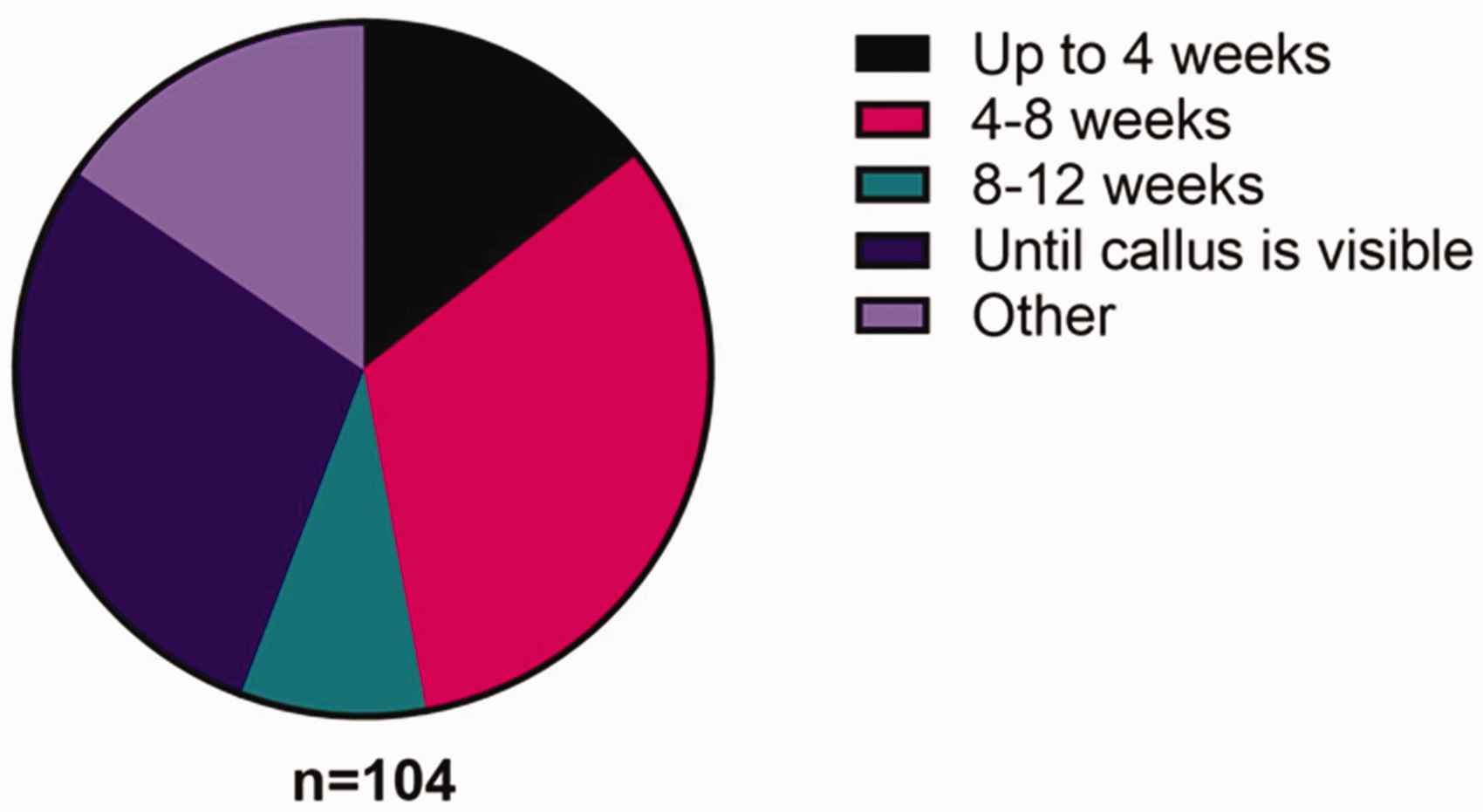
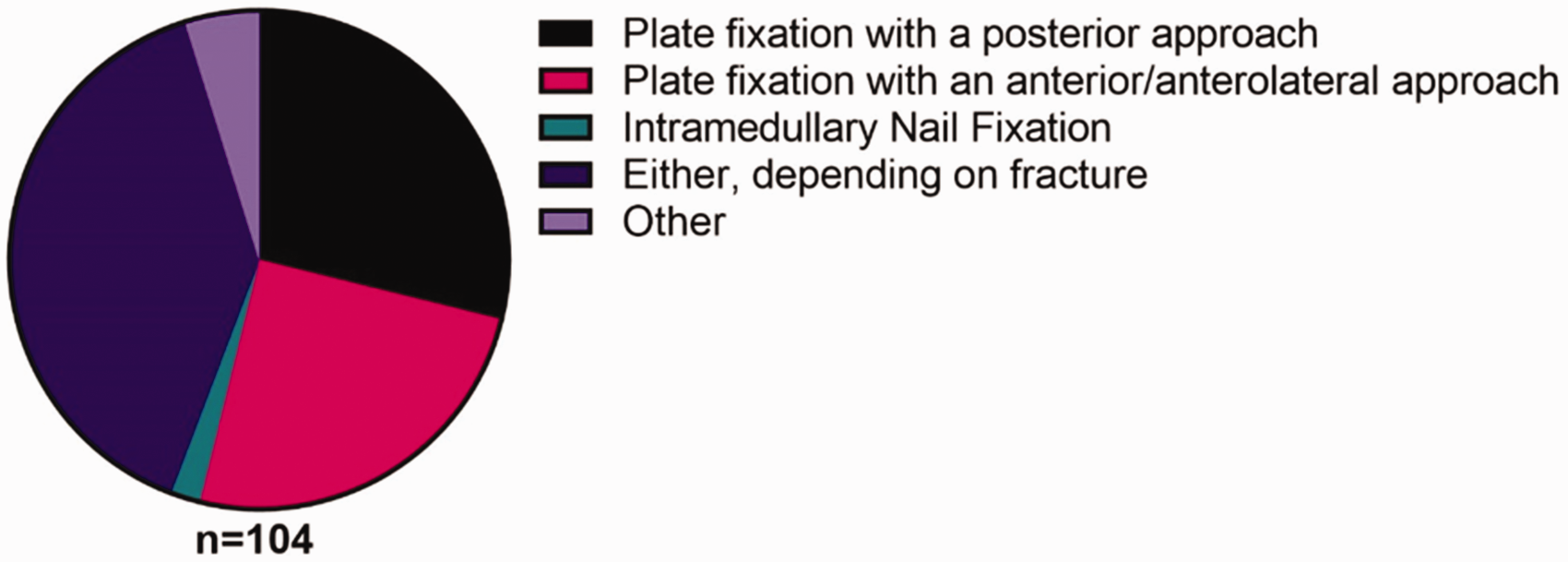
Most of our respondents (n = 63, 61%) considered recommending surgery for HSFs when there are inadequate signs of union at 12 and 16 weeks. Very few would consider surgery at 8 weeks (5%) or leave it for as long as 24 weeks (13%; Figure 4). In terms of operative approach and method of fixation 41 (39%) respondents chose to be flexible based on the nature of fracture. Most would exclusively use plates with either an anterior/anterolateral or posterior approach (n = 56, 54%) and only a small minority would exclusively use nails for HSFs (2%; Figure 5).
Length of non-operative treatment before recommending surgical intervention for delayed union. Approach and method of fixation for displaced humeral shaft fractures.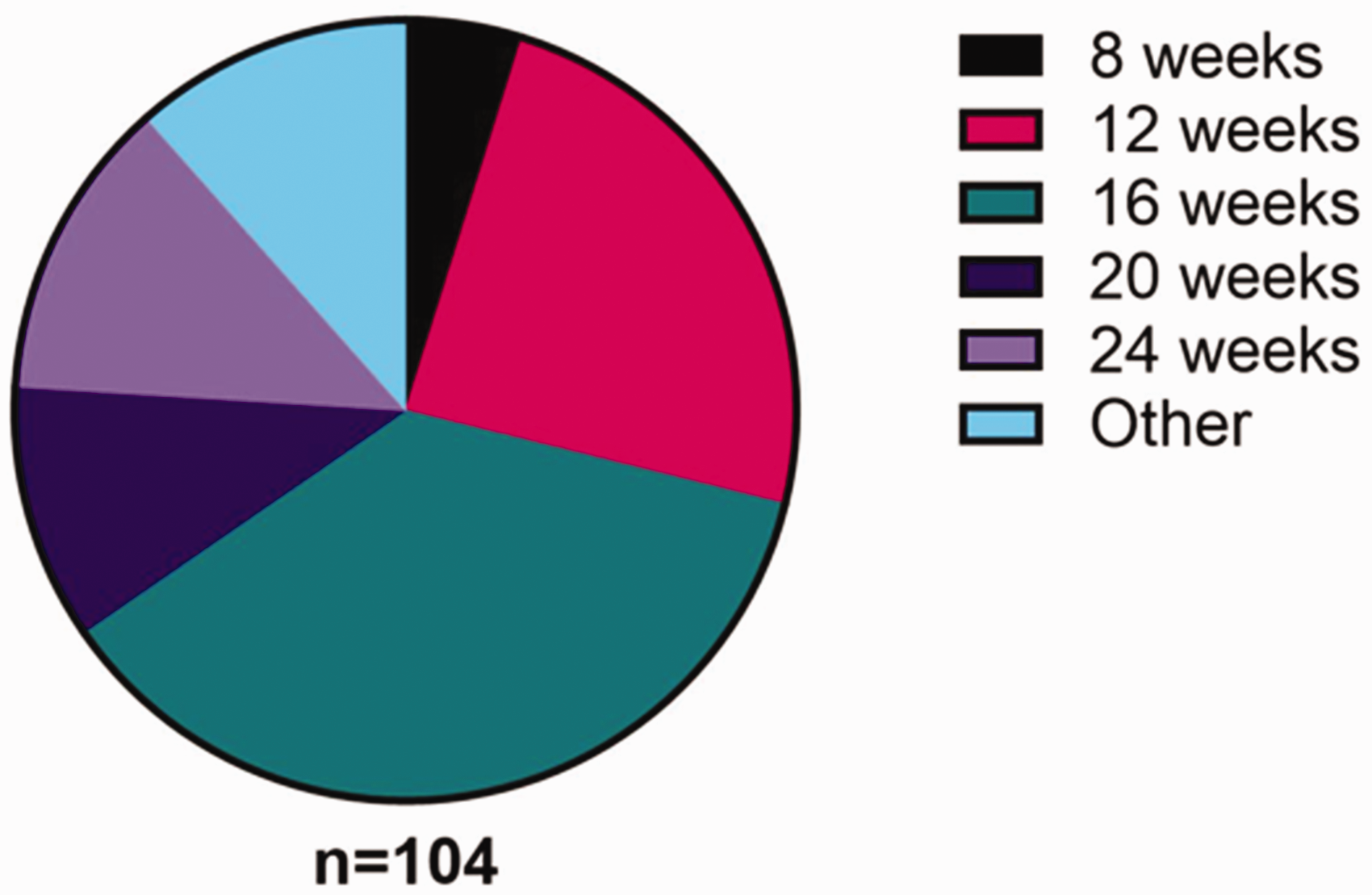
There was significant interest amongst our respondents for taking part in a national randomised trial with 44 BESS members providing their contact details for further information. They were willing to randomise patients to nonsurgical and surgical arms as this was considered to be an important clinical question. The survey also helped estimate the required recruitment rate to help us in planning and ensuring feasibility of a multi-centre national trial. It could be estimated from the submitted number of patients treated at each centre that on average 1.5 potentially eligible patients present to each recruitment site each month which would provide a conservative recruitment rate of 0.8 patients per centre per month.
Discussion
HSFs have traditionally been treated non-operatively with good clinical outcomes, but in recent decades surgical treatment is becoming increasingly utilised which may represent a significant public health burden. 12 The concern is nonunion leading to a later need for surgery. In our survey we found a significant number of respondents treating around half of their patients with displaced fractures surgically. This is despite lack of high-quality evidence to support surgery over non-operative management.4,5 A recently published randomised trial from Finland by Rämö et al. 5 with around 80 patients failed to show any differences in clinical outcomes between the operative and non-operative arms of the study. They did find a significant cross-over (30%) from the non-operative treatment arm to surgery. Given the relatively small number of patients in each arm, the results may need to be interpreted with caution and there is a good argument for a larger randomised trial. Other trials have attempted to compare various forms of operative treatment such as conventional and minimally invasive humeral plating as well as intra-medullary nailing.13,14 Recent meta-analyses comparing operative with non-operative treatments are still not able to agree on the optimal management of HSFs.4,15 They do show that non-union rates can be reduced with surgery, but with greater risks of infection and possibly nerve injury the ideal treatment is not clear.
In any clinical study it is important to define inclusion criteria depending on the type of fracture. The aim of our survey was to look for consensus amongst surgeons on how a future randomised trial should look like so we would increase the willingness of surgeons to recruit to such a trial. This survey has highlighted that site of fracture definition can mean different things to different surgeons. Our responses did not show one dominant choice, and this would mean that any large trial, for the results to be universally accepted, would need to clearly define which fractures are included to help with the screening process. Fracture displacement was another area that highlighted disagreement and unless this is also addressed in the trial protocol the heterogeneity in what is classified as displaced may lead to selection bias in a randomised study.
Non-operative management is the primary treatment option for most HSFs and is known to result in good long-term outcome. 3 There is considerable debate on what constitutes a displaced fracture, but conservative treatment is generally either a coaptation plaster splint followed by a functional humeral brace or a humeral brace alone. We found that brace only treatment was more commonly used and is certainly a good option to allow early range of motion of both shoulder and elbow. Brace treatment works through a concept of soft-tissue compression creating a hydraulic cylinder. Success is based on patients staying upright, daily tightening of straps and non-weight bearing. If a sling is used for pain relief then this can affect fracture alignment and should be considered during follow-up radiographs. Contraindications include soft tissue or bone loss, an uncooperative patient, a very proximal or distal fracture as well as failure to get satisfactory alignment with brace tightening. In our survey there was a preference for immobilising patients for 4–8 weeks (33%) or until fracture callus was present (29%). Brace treatment would allow patients to continue with daily activities whilst the fracture heals.
Nearly all our respondents would consider open, neurovascular and multiple injuries as important factors when an early surgical management would be advisable so these could be useful exclusion criterion for the future trial. Patient choice and BMI were also considered important by over half our respondents. Although patient choice is an important factor, shared decision making is largely based on using the best available evidence and applying it to the patient in your clinic. Bias can creep into these discussions particularly if the evidence for one treatment over another is not strong. Patient habitus can have an impact on decision making as larger patients may be more difficult to treat with functional bracing.
Another area of contention in the literature is the use of plates over intramedullary nailing. There are certain cases where humeral plating would be preferred such as an established non-union or an associated neurovascular injury, but the evidence is yet to show superiority of one method of fixation over another. 16 Meta-analyses do not show a significant difference in outcome but only pool together a limited number of low quality studies. 17 A Cochrane review in 2011 18 and a more recent meta-analysis 8 suggested similar clinical outcomes, but a greater risk of impingement and metalwork removal with intramedullary nailing. This survey has highlighted variations in how patients are treated operatively with a comparable number preferring posterior plating (28%) and anterior/anterolateral plating (25%). Interestingly only a small number would exclusively use nails in HSFs. The majority would base their choice of method of fixation and approach on the location of the fracture. Based on the survey results and current literature there is unlikely to be complete consensus and a trial should allow a variety of surgical treatments based on a surgeon’s preference as this would ensure greater participation in a trial.
The main limitation of this survey is the potential for responder bias as we had a relatively low response rate of around 32% from the BESS membership. The response rate is not dissimilar to other survey-based studies in the literature. 19 Our power analysis assumed that 15% of BESS members would be non-active or non-contactable. If this number is lower than 15% then our study is at risk of being under-powered. When considering the response rate with the interest we have had towards a national trial we may have attracted responses from participants who are generally more research oriented. More research orientated members are also more likely to complete surveys in the first place and the responses may not be representative of the wider upper-limb surgical community. Responses to surveys may also not be an accurate reflection of the participants’ actual practice at their institution. Despite the limitations our responses have allowed us to get a glimpse of current UK practice, which appears to consist of significant variation in how we treat HSFs.
There is a significant need for conducting a high quality randomised controlled trial to not only compare clinical outcomes between operative and non-operative management, but to also look at the cost effectiveness and risk profiles of both interventions for displaced humerus shaft fractures. The lack of consensus on how we define HSFs and displacement will need to be addressed in the trial protocol. In addition, due to variations in how we treat HSFs a certain degree of pragmatism may need to be adopted to allow greater participations from UK centres.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.