
Abstract
Background
As total shoulder arthroplasty has emerged as the fastest growing joint replacement performed, optimizing surgical efficiency and patient outcomes is essential. The goals of the current study were to identify trends and factors affecting the operative time of total shoulder arthroplasty over a 10-year period.
Methods
The National Surgical Quality Improvement Program database was analyzed to determine the operative time and 30-day complications of total shoulder arthroplasty from 2008 to 2018. Factors affecting total shoulder arthroplasty operative time were also assessed. Multivariable linear regression was used to analyze operative time over years studied while controlling for patient demographics and comorbidities.
Results
A total of 20,587 total shoulder arthroplasty cases from 2008 to 2018 were included. Mean operative time in 2008 was 139.0 min, while in 2018, mean operative time decreased to 105.6 min (P < .001). Male sex, outpatient surgery, increased body mass index, and low preoperative hematocrit were associated with longer operative times, while elevated international normalized ratio, resident involvement, and elective surgeries were associated with decreased operative duration.
Discussion
Operative time for total shoulder arthroplasty has decreased from 2008 to 2018. Patient factors and comorbidities are associated with operative time, and such factors are important to consider in operative planning to ensure appropriate patient and surgeon expectations.
Introduction
Total shoulder arthroplasty (TSA) has become a widely utilized and reliable procedure in the treatment of end-stage glenohumeral arthritis. The popularity of TSA and its reverse counterpart have risen internationally and, in conjunction with advancements in surgical technique and implants, have made shoulder arthroplasty the fastest growing joint replacement performed in recent years.1–3 This high demand for shoulder arthroplasty has led to emphasis on optimizing surgical outcomes and operative efficiency.4,5
Various total joint arthroplasty studies have described the relationship between operative duration and complications.6,7 In shoulder arthroscopy, a 15-min increase in operative time has been associated with increased risk of venous thromboembolism, surgical site infection, and increased length of hospital stay. 8 Similarly, increased operative duration of shoulder arthroplasty has demonstrated significantly more complications, blood transfusions, nerve injuries, and urinary tract infections. 9 Operating time greater than 2 h is an independent predictor of complications in TSA. 10 While both modifiable and non-modifiable patient and surgeon factors play into operative time, understanding trends in operative duration as well as investigating factors affecting operative time is of paramount importance to identify high-risk patients and address risk factors associated with extended surgical time.
Prolonged operative duration does affect not only the outcomes but also the cost of patient care. A recent study cites operating room time costs at around $36 to $37 per minute, highlighting the substantial cost of operative time. 11 Decreases in surgical duration optimize efficiency and allow for surgeons and hospitals to maximize their case volumes, which is an important factor associated with improved TSA outcomes. 12 There remains a lack of data pertaining to the change in operative time of TSA procedures over recent years.
With a continued interest in optimizing surgical efficiency, factors that increase surgical duration and the related costs must be considered. Currently, there remains a paucity of large-scale analyses describing changes in operative duration of TSA over recent years. Therefore, the goals of the current study are to utilize a large nationwide database to identify trends in TSA procedures with a focus on operative duration, as well as to investigate factors affecting operative times. Our hypothesis is that the operative duration of TSA has decreased over the past 10 years in accordance with advancements in technique, implants, and surgeon experience.
Methods
Data source
The National Surgical Quality Improvement Program (NSQIP) database from the American College of Surgeons was utilized. This chart-based database contains variables including de-identified patient demographics, Current Procedural Terminology (CPT) codes, comorbidities, and 30-day complications. Over 700 medical centers contribute to the NSQIP, and clinical reviewers periodically audit the submissions. 13
Case selection
All cases with CPT code 23472 (arthroplasty, glenohumeral joint) performed between 1 January 2008 and 31 December 2018 were selected. Of note, this code includes both anatomic and reverse TSA. There were 1121 cases with operative time either greater than the 97.5th percentile (217 min) or less than the 2.5th percentile (47 min) that were excluded to remove potential bias from outliers. Additionally, any cases missing sex (n = 6), race (n = 2080), age (n = 131), BMI (n = 68), anesthesia method (n = 67), American Society of Anesthesiologists (ASA) Class (n = 16), postoperative length of stay (LOS, n = 12), or preoperative functional status (n = 138) were excluded (Figure 1). A modified Charlson comorbidity index (CCI) was calculated based on the available information in the NSQIP. For the calculation of CCI, a history of diabetes mellitus on oral therapy, ascites, chronic obstructive pulmonary disease, or congestive heart failure were all assigned 1 point. A history of end-stage renal disease or insulin-dependent diabetes mellitus were assigned 2 points. Disseminated cancer was assigned 6 points, and 1 point was assigned for decade of age over 49 (1 point for ages 50–59, 2 points for ages 60–69, etc.).
14
Flowchart of inclusion criteria for study subjects. TSA: Total shoulder arthroplasty. rTSA: Reverse total shoulder arthroplasty. CPT: current procedural terminology; NSQIP: National Surgical Quality Improvement Program; BMI: body mass index; ASA: American Society of Anesthesia; LOS: length of stay.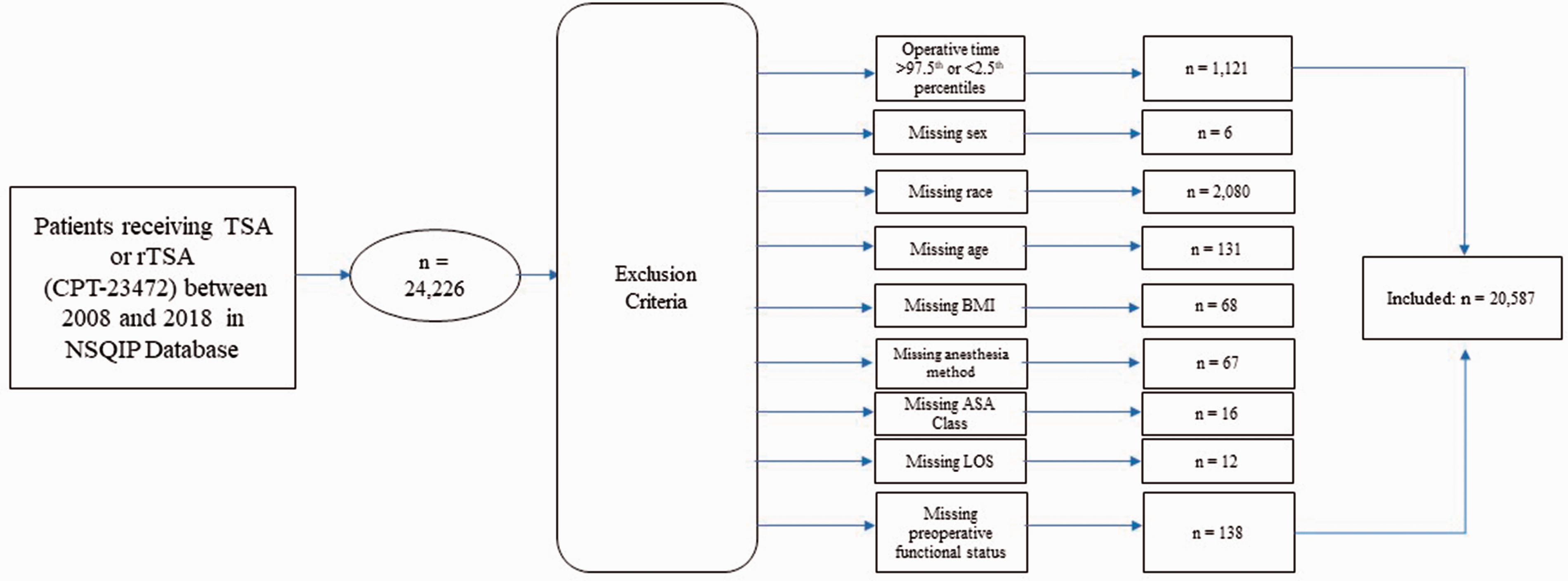
The primary outcome variables assessed were operative time and LOS. Additionally, several 30-day complications were assessed, including readmission to the hospital, return to the operating room (OR), superficial wound infection, deep wound infection, wound dehiscence, deep vein thrombosis (DVT), pulmonary embolism (PE), and sepsis.
Variables assessed for predictive value of case length included patient sex, race, age, body mass index (BMI), modified CCI, ASA class, preoperative functional status, smoking status, non-elective versus elective surgery, inpatient versus outpatient surgery, anesthesia method, history of a bleeding disorder, preoperative blood transfusion, and presence of a resident during surgery. Data on resident involvement were captured from 2008 to 2012, and data on elective surgery were captured from 2013 to 2018. Some patients also had preoperative laboratory values for hematocrit, white blood cell count, international normalized ratio (INR), creatinine, and platelets. As many patients were missing these values, we included a term for missing values to assess for any possible bias. These laboratory values were recoded into normal and abnormal ranges. A hematocrit less than 35 for women and less than 40 for men was defined as abnormal, as were white blood cells less than 4 K/µL or greater than 11 K/µL, INR greater than 1.1, creatinine greater than 1.1 mg/dL for women or 1.2 mg/dL for men, and platelets less than 150 K/µL.
Statistical analysis
Independent samples t-testing was performed to determine differences in operative time for both resident involvement and elective surgery as these variables were not collected for the entire length of the study. Both linear models and chi-squared testing were used to assess trends over time for operative time, LOS, and 30-day complications. Additionally, a multivariable linear model was created to analyze how operative time changed over the course of the study while controlling for patient demographics and comorbidities. SPSS Statistics V26.0 was used for analysis (IBM Corporation, Armonk, NY, USA). Statistical significance was set at P < .05.
Results
Patient demographics
Continuous variables for total shoulder arthroplasties performed from 2008 to 2018.
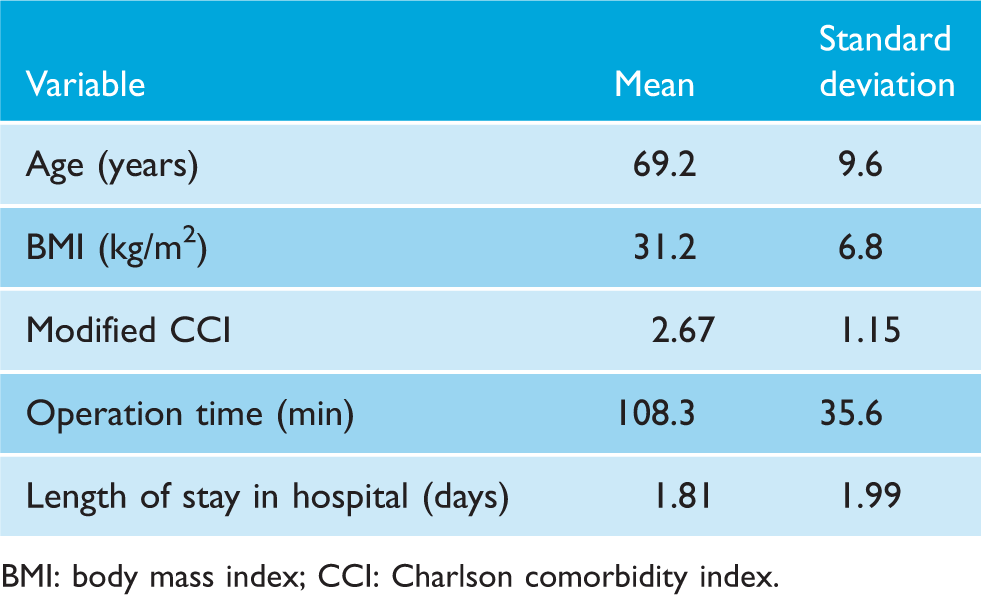
BMI: body mass index; CCI: Charlson comorbidity index.
Categorical variables for total shoulder arthroplasties performed from 2008 to 2018.
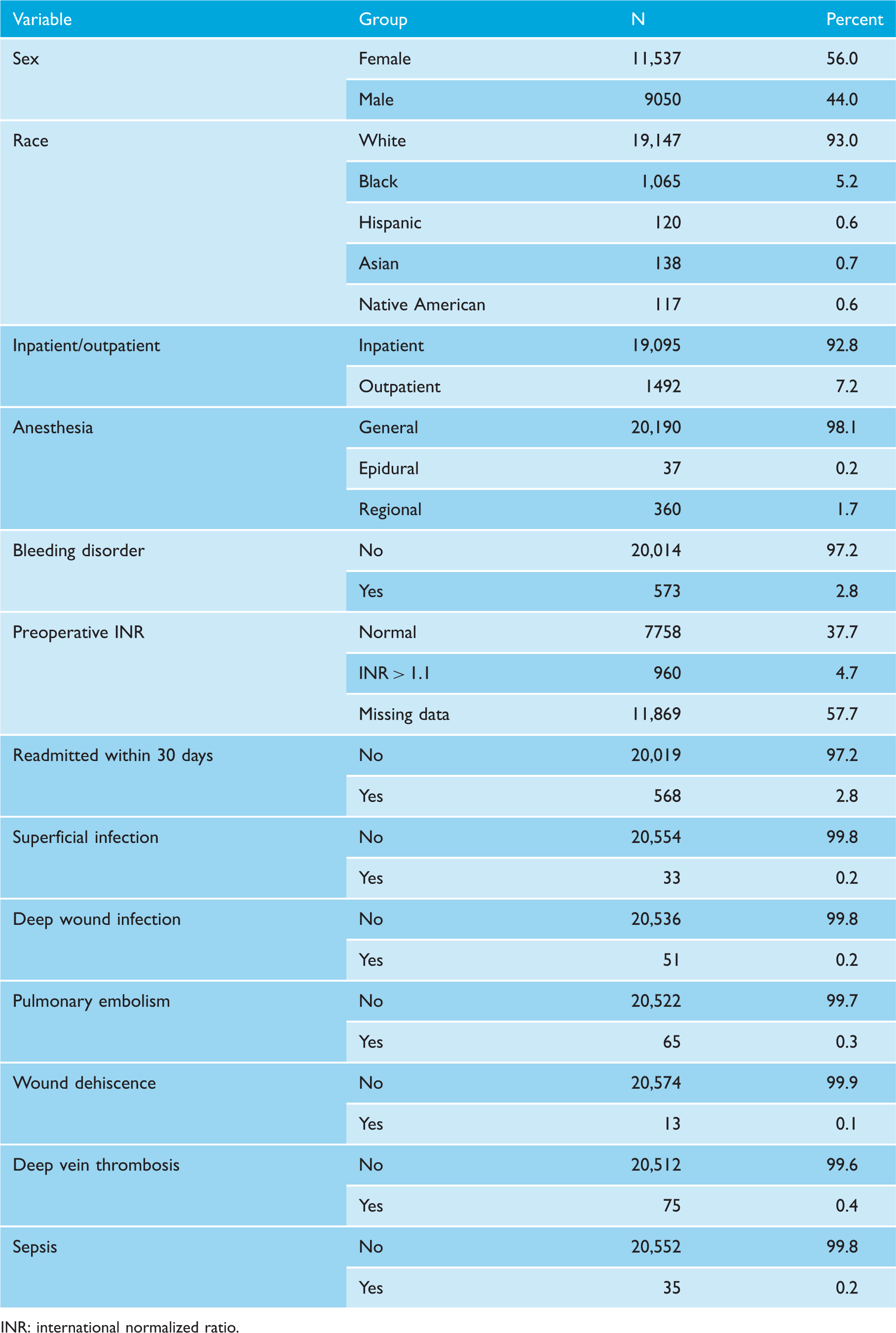
INR: international normalized ratio.
Trends over time
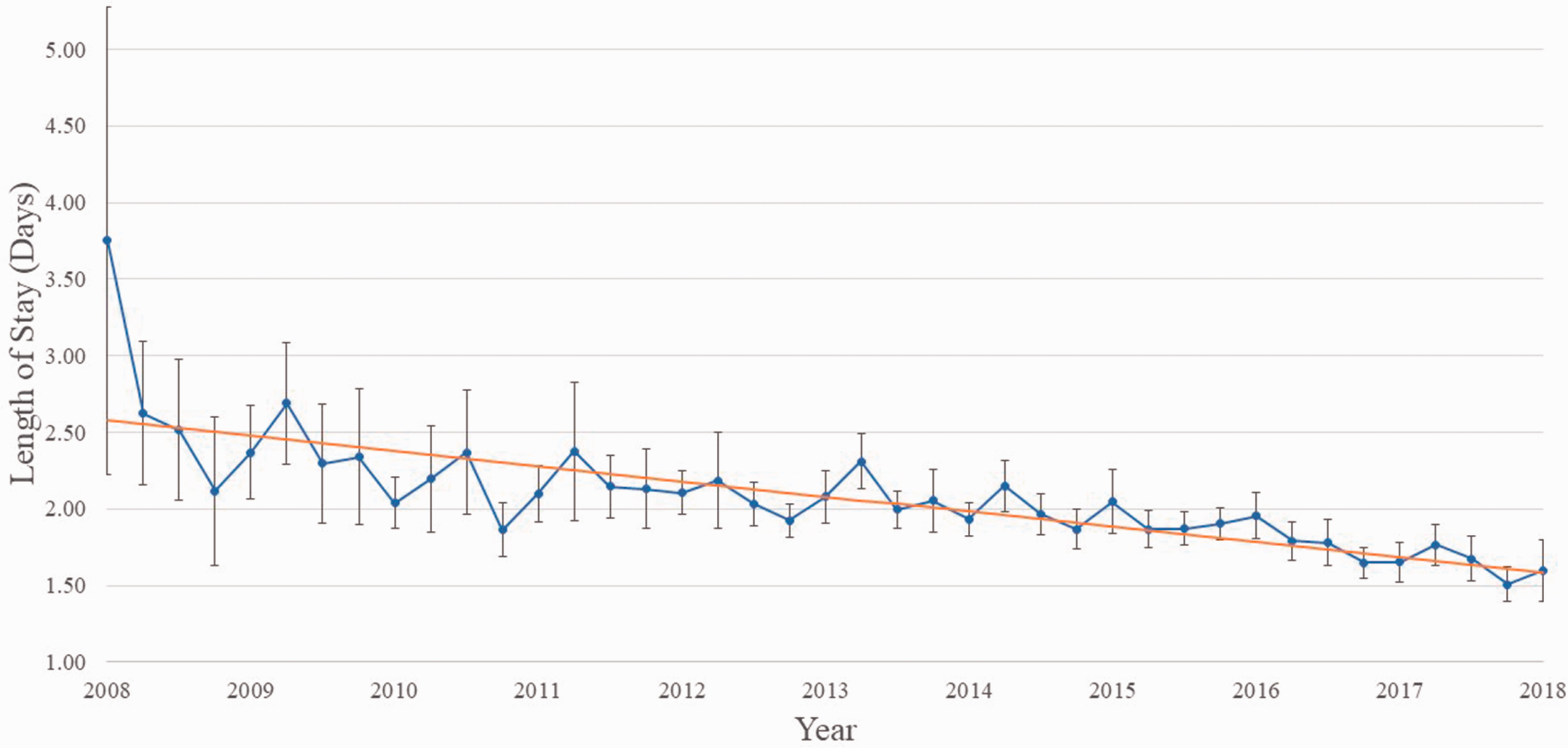
Both operative time (Figure 2) and LOS (Figure 3) decreased over the course of the study. The average operative time in 2008 was 139.0 min (95% CI, 131.5–146.6). In 2018, the mean operative time had decreased to 105.6 min (95% CI, 104.5–106.6) (P < .001). A single linear regression found an annual decrease of 1.5 min (95% CI, 1.3–1.7) per year. Similarly, the mean LOS in 2008 was 2.60 days (95% CI, 2.26–2.94) compared to 1.49 days (95% CI, 1.42–1.56) in 2018 (P < .001). There was a yearly decrease of .10 days (95% CI, .09–.11) for LOS under single linear regression (Figure 3).
Annual mean operative time and linear regression model of operative time based on year for total shoulder arthroplasty. Annual mean length of stay and linear regression model of operative time based on year for total shoulder arthroplasty.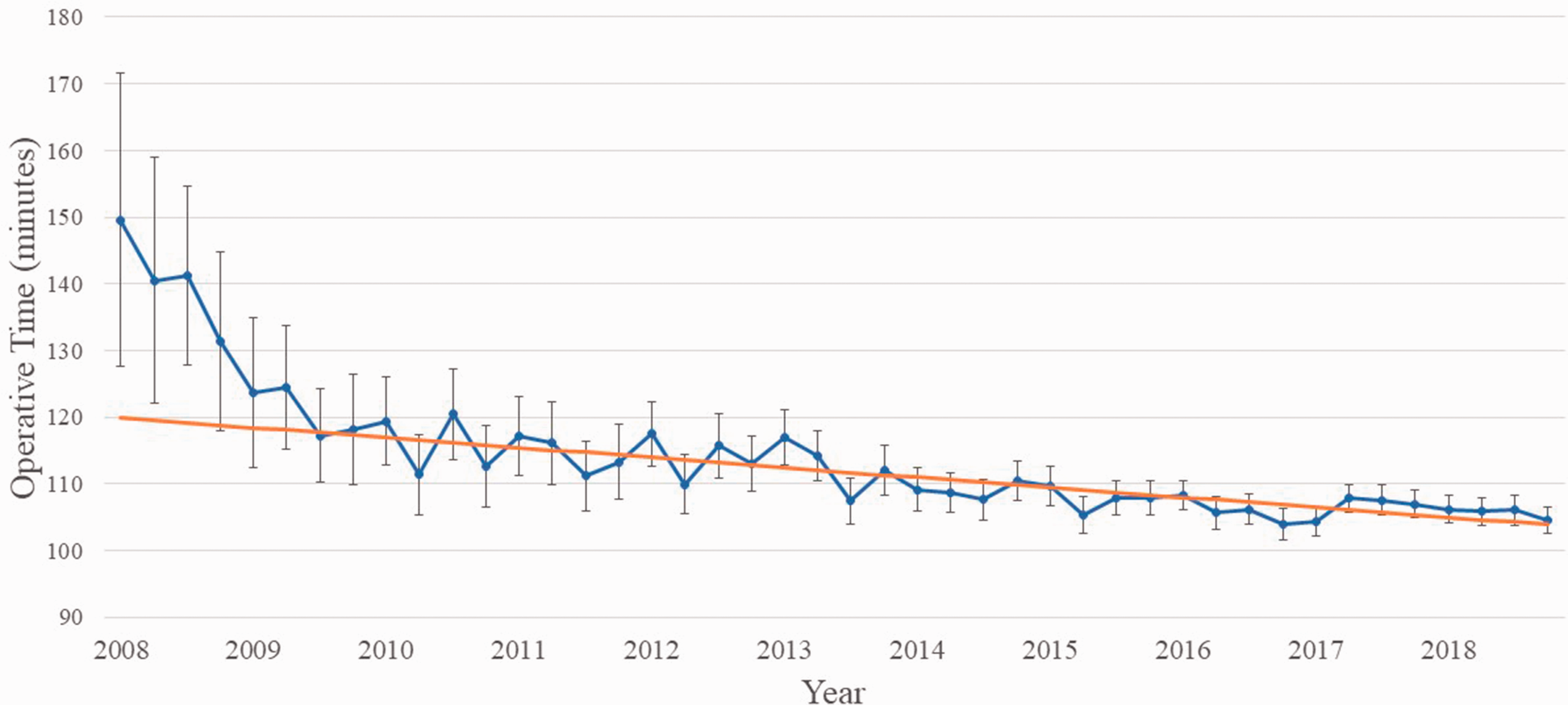
Generalized linear model of operative time as predicted by patient and surgical characteristics for total shoulder arthroplasty.
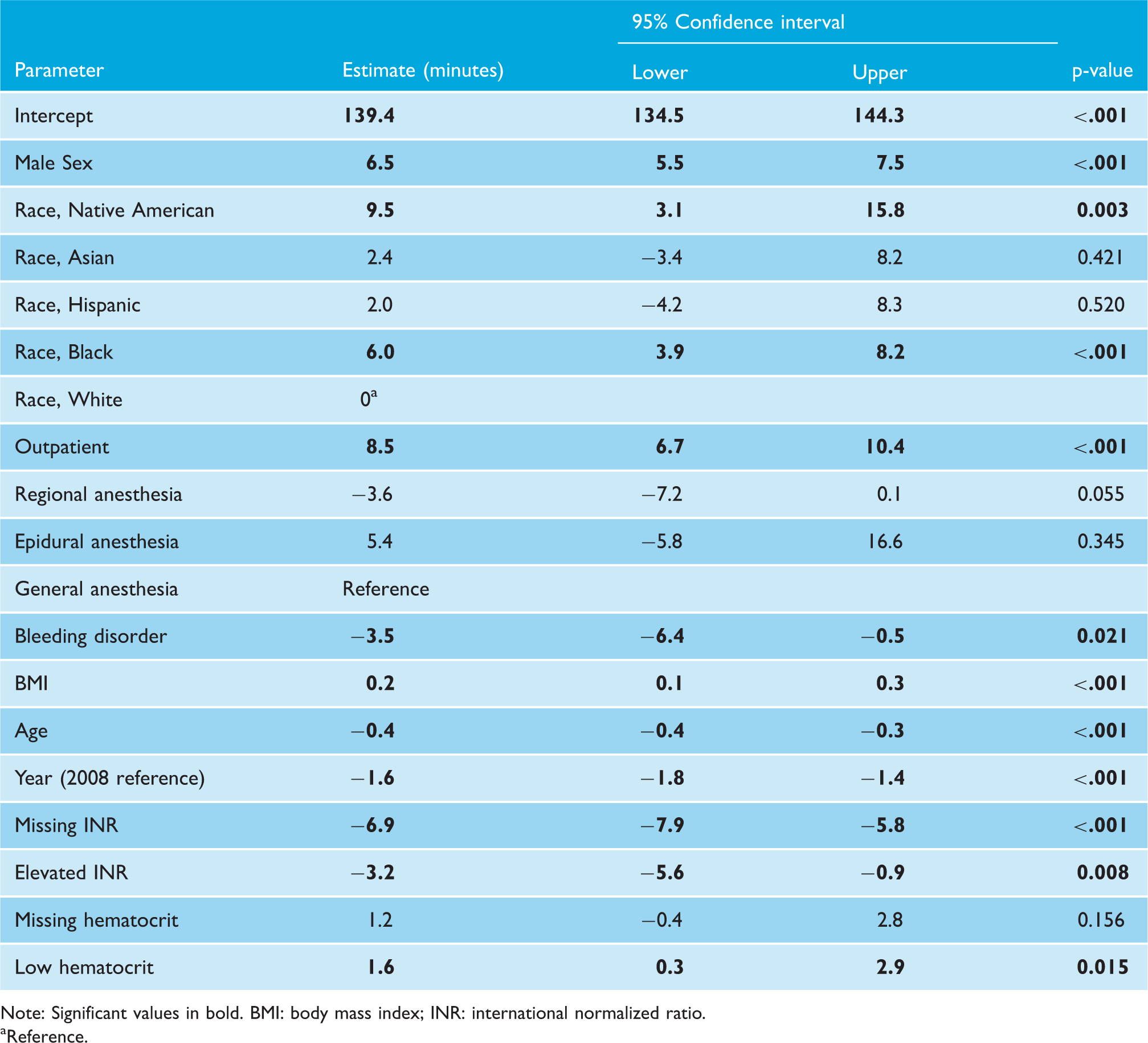
Note: Significant values in bold. BMI: body mass index; INR: international normalized ratio.
Reference.
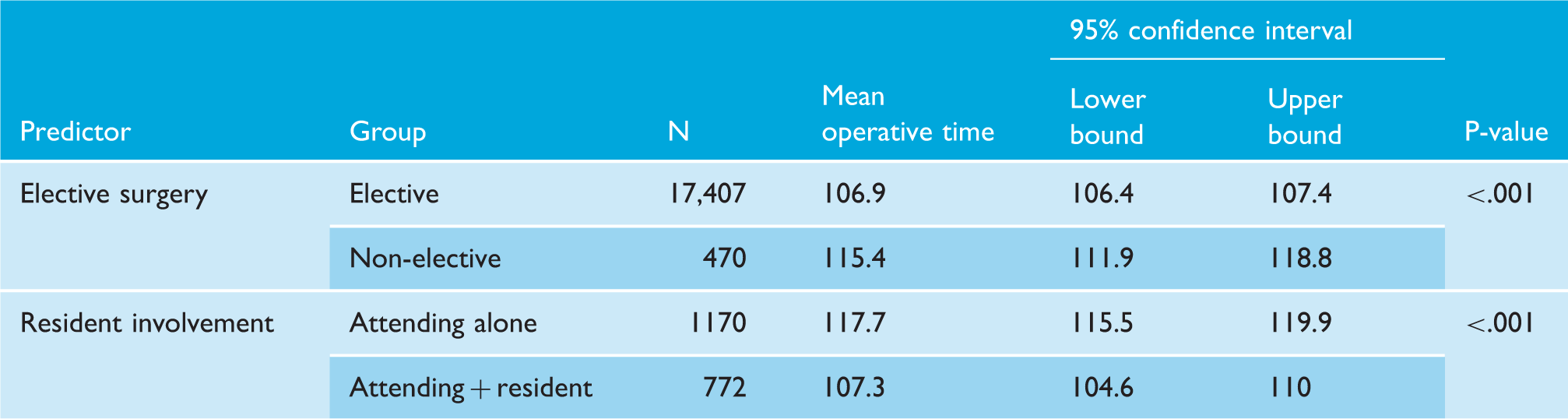
Although both resident involvement and elective versus surgery were only captured for part of the sample, both variables showed significant trends over time. Non-elective TSAs were 8.5 min longer than elective TSAs (115.4 vs. 106.9 min, P < .001). Cases performed with both an attending surgeon and a resident were 10.4 min shorter than cases performed by an attending without resident assistance (107.3 vs. 117.7 min, P < .001).
30-day complications
The all-cause 30-day readmission rate was 2.8% (Table 2). The most common 30-day complication was deep venous thrombosis (.4% of all cases), while the next most common 30-day complication was wound dehiscence, which occurred in .4% of cases. PE occurred in .3% of cases. Superficial infections, deep wound infections, and sepsis occurred at a rate of .2%. Wound dehiscence occurred in .1% of cases. Using both linear regression and chi-squared analysis, there was no significant change over time in any of these complications.
Discussion
Optimizing surgeon efficiency in large joint arthroplasty remains an area of ongoing interest, and a greater understanding of the surgical factors that influence cost and outcomes, such as operative duration, is necessary. Efficiency in the operating room is important to optimize patient care, surgical workflow, and minimize the cost of care; yet recent trends in operative time of shoulder arthroplasty remains an area of uncertainty. Our results demonstrate that both operative time and hospital LOS have decreased in patients undergoing TSA between 2008 and 2018. Rates of readmission, return to the operating room, surgical site or deep wound infection, deep venous thrombosis, PE, and sepsis after TSA did not change over the study period. Factors including BMI, age, INR, gender, race, inpatient versus outpatient surgery, and anesthesia type were all associated with TSA operative time. Elective cases and those with resident involvement were both associated with significantly decreased operative time for TSA. Understanding how these variables affect surgical time may provide valuable information in initial patient consultation, risk stratification, and surgical planning.
Contrary to a recent report of operative duration trends in total hip arthroplasty (THA), our analysis demonstrates that surgical time for TSA has decreased over the past 10 years. 15 TSA has been growing in utilization at a faster rate than other large joint arthroplasty procedures, and such an increase in demand results in higher surgical volume and should lead to optimization of surgeon efficiency over time. 2 In an analysis of several fellowship-trained arthroplasty surgeons, Testa et al. reported that recent fellowship graduates performing TSA at high volumes demonstrate an initial steep learning curve, followed by a substantial decrease in operative times after up to 86 cases. 16 This trend, in the context of our results, may be apparent in surgeons at a population level and is one element contributing to the decrease in TSA surgical duration over time. Moreover, the advances in implant technology and technique are readily apparent over the past decade and may contribute to improved operative speed by improving surgical efficiency and eliminating unnecessary surgical steps. 17 Reverse TSA (rTSA) is also a relatively new procedure in some countries, as it was only approved for use in the United States in 2004. Its popularity and surgical indications have increased substantially over recent years and, as such, surgeons have likely become more comfortable and efficient performing reverse TSA over the more recent years captured by our analysis.
While the overall operative duration of anatomic and reverse TSA has decreased between 2008 and 2018, our study concomitantly observed no change in the 30-day complication rate (i.e., surgical site infection, DVT, PE) or hospital readmissions following such procedures. Increased shoulder arthroplasty operative time has previously been associated with higher complication rates, including more blood transfusions, nerve injuries, and urinary tract infections. 9 Anthony et al. described an operative time of greater than 2 h as being an independent predictor of complications in TSA. 10 Our results demonstrate that, while shoulder arthroplasty surgeons have improved their efficiency by over 30 min on average from 2008 to 2018, no concominant reduction in complication rate was observed. This finding was unexpected in the face of the previously discussed literature and may be related to the increase in the utilization of rTSA over the studied time period. Reverse TSA has been shown to have widely variable complication rates, ranging from 0% to 75% depending on the series studied. 17 With the rise in rTSA prevalence, more surgeons may also still be operating within the surgical learning curve, prior to the threshold after which complication rates after rTSA are reduced. 17 As advancements in surgical technique and implants for shoulder arthroplasty continue to evolve, it will be interesting to continue to observe both operative time and complication rates to elucidate any further relationship between these important factors as longer time periods and greater surgical volume can be studied.
Providers and hospital entities are growing increasingly interested in reducing unnecessary hospital stays and decreasing patients’ LOS after various arthroplasty surgeries. Various patient factors such as increasing age, female sex, medical comorbidities, or low-volume surgeons are associated with extended LOS following TSA.18,19 Moreover, inpatient admission after TSA is an independent risk factor for complications. 20 The results of the current study confirm those of several prior studies that have described a decrease in the average LOS of TSA patients over recent years.21,22 Prior studies have also elucidated a relationship between TSA surgical time and hospital LOS. Dunn et al. found a relationship between operative time greater than 174 min and longer hospital stays in TSA patients. 21 The decrease in LOS mirrors the trends observed in operative duration over the 10 years studied. Possible explanations include improved perioperative multimodal pain management and optimization of preoperative patient factors associated with increased LOS. 22
Bivariate analysis of elective vs nonelective surgery and resident involvement versus operative time for total shoulder arthroplasty.
As surgical providers continue to focus on high-value care, outpatient total joint arthroplasty has increased in interest and poses an opportunity to optimize the surgical experience for the patient and surgeon alike. Shoulder arthroplasty is 40% less expensive when performed in the outpatient setting and is typically performed in patients who are younger and healthier.19,24 However, in order to perform outpatient arthroplasty, it must be proven that it can be done safely. Interestingly, in our analysis, outpatient TSA took significantly longer to perform, requiring over 8 min more operative time than traditional inpatient TSA. One possible explanation for this finding may be related to the need for more meticulous hemostatic control given placement of a drain, for example, is less ideal in a patient being discharged home on post-operative day zero. Moreover, there is limited opportunity to closely monitor the patient in the immediate hours to days following surgery, where early surgical complications can be easily and safely identified. This is an otherwise unexpected finding; patients undergoing outpatient TSA are typically younger and healthier, a cohort which in general was identified by our study to have shorter average operative times. Bean et al. found both outpatient and inpatient TSA to have similar surgical times in a retrospective cohort analysis of 61 patients, which is contrary to our findings. 25 Further research into the surgeon and patient-specific characteristics (e.g., specific patient pathology/diagnosis, implant system, geographic setting) leading to prolonged operative time in outpatient TSA would provide interesting insight into this unexpected finding.
Our study demonstrated that the presence of a resident was associated with a decrease in operative time with an average case time of 107.3 min in those which involved a resident versus 117.7 min in cases where no resident was involved. Such findings mirror those by Romeo et al. who also demonstrated decreased TSA operative time when a resident was present (113.6 min vs. 121.3 min). 26 Furthermore, these authors demonstrated decreased LOS following TSA when a resident was present for the case and found no significant difference in medical or surgical complications postoperatively. 26 The observed decrease in operative times in the present and aforementioned studies is in contrast to what has been observed for other arthroplasty procedures, such as THA and total knee arthroplasty (TKA), where resident involvement is associated with increased operative times. 27 Such a discrepancy can be explained by both the nature of the operations as well as the medical setting in which they are performed. Hip and knee reconstructions are frequently performed in “Total Joints Centers of Excellence” which is a designation that is given to hospitals based on multiple criteria related to surgical volume, implementation of evidence-based practices, and other patient outcome metrics to improve patient care and decrease health-care spending.28,29 Many of these centers implement structured protocols which focus on efficiency to reduce operative times and the associated costs. At such centers, a resident may play less of a role in assisting the primary surgeon. 30 Conversely, the annual volume of TSA is currently less than that of TKA and THA, and therefore non-physician surgical staff may be less knowledgeable and comfortable in assisting with the procedure compared to a resident physician.
When examining the relationship between the modality of anesthesia and operative time, our results demonstrated operative times to be, on average, 3.6 min faster when regional anesthesia was used in comparison to general anesthesia (P = .055). However, general anesthesia was used much more frequently, in 98.1% of the cases in comparison to regional anesthesia (1.7%). As more procedures are being performed on an outpatient basis and reimbursements become more frequently adjusted based on patient outcomes and quality of care, it is paramount to consider all factors related to the surgical experience, patient outcomes, satisfaction, and overall cost of care. Regional anesthesia use in TSA patients is becoming increasingly common as it has multiple benefits when compared to general anesthesia. Such benefits include superior muscle relaxation, improved intraoperative hemodynamic stability, reduced hospital LOS and time spent in the post-anesthesia care unit, reduced in-hospital complication rates, reduced readmission rates, improved pain control, and higher patient satisfaction.31–34
Finally, when investigating patient-specific factors that influenced the total operative time, our results demonstrated male sex, higher BMI, and lower preoperative hemoglobin to be associated with longer operative times. Such increases are likely multifactorial, but it can be hypothesized that this increased time may be spent during the surgical approach. For example, males tend to have more muscle mass and higher BMIs, both of which are known to result in more difficult surgical exposures. Additionally, surgeons may be more likely to spend more time on hemostasis in patients who have lower preoperative hemoglobin to minimize the need for blood transfusion. Conversely, the mean operative time was shown to be less for older patients, patients with a history of a bleeding disorder, and an elevated preoperative INR. For similar reasons, in these patients, surgeons may be more motivated to minimize operative time to decrease anesthesia-related risks in an older population as well as minimize blood loss in those at increased risk for such loss. The data above are essential to consider preoperatively when counseling patients, planning for the case, and maximizing patient optimization preoperatively.
Despite the large cohort of patients analyzed, our study contains several limitations. Inherent to all database studies, our data are dependent on accurate coding, and thus data may be either missing or incorrect. However, we believe that our large sample size mitigates these errors and prevents substantial changes to the observed outcomes. Additionally, the NSQIP database does not display data related to multiple factors that are likely related to operative time, including surgeon experience, the performed surgical technique/approach, and finally, the type of implant used. An important limitation to the current study is the lack of unique CPT codes for rTSA and TSA, resulting in our data acquisition encompassing both procedures. Using a recent study evaluating the utilization of TSA in the United States using a National Inpatient Sample, Rabinowitz et al. demonstrated a large shift in the performance of shoulder arthroplasty from anatomic to reverse over recent years, with approximately 62% of TSA cases performed being rTSA in 2018. 35 Given rTSA utilization is increasing at a greater rate relative to anatomic TSA over recent years in the United States, and that surgeons may perform one procedure more quickly than the other, these are variables that could not be accounted for which may ultimately impact operative speed.36,37 However, we believe that our data present vital information for surgeons; understanding such data can help surgeons anticipate which patients may require increased operative time and may benefit from further preoperative optimization and planning. Finally, this information can assist surgeons when choosing which patients are ideal candidates for outpatient TSA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval from our institution was not required to perform and publish the attached research. Informed consent was not required given no patient identifiers were not accessed in this database analysis.
Guarantor
EJT.
Contributorship
EJT researched the literature, conceived the study, performed data collection and interpretation, and prepared the manuscript. LTL performed data collection and analysis as well as manuscript preparation. NJL performed data interpretation and manuscript preparation. SDF performed data interpretation and manuscript preparation.