
Abstract
Aim
This study aims to evaluate restoration of anatomy following Total Shoulder Arthroplasty (TSA) with the Mathys Affinis Short prosthesis.
Background
Over the last decade stemless shoulder arthroplasty has increased in popularity. One of the reported advantages of the stemless designs is the ability to restore anatomy following surgery. However, very few studies have evaluated restoration of anatomy following stemless shoulder arthroplasty.
Methods
The study included all patients who had undergone TSA using the Affinis Short (Mathys Ltd, Bettlach, Switzerland) prosthesis for primary osteoarthritis between 2010 and 2016. The mean follow up was 42.8 months (range 9.4 to 83.4 months). Pre and post-operative radiographs were assessed for Centre of Rotation (COR), Humeral Head Height (HHH), Humeral Head Diameter (HHD), Humeral Height (HH) and, Neck Shaft Angle (NSA) using the best fit circle method on PACS software. Measurements were scored and compared to assess the accuracy of the implant in restoring the native geometry, including the intraobserver variability. The same data was collected by another experienced observer to measure the interobserver variability.
Results
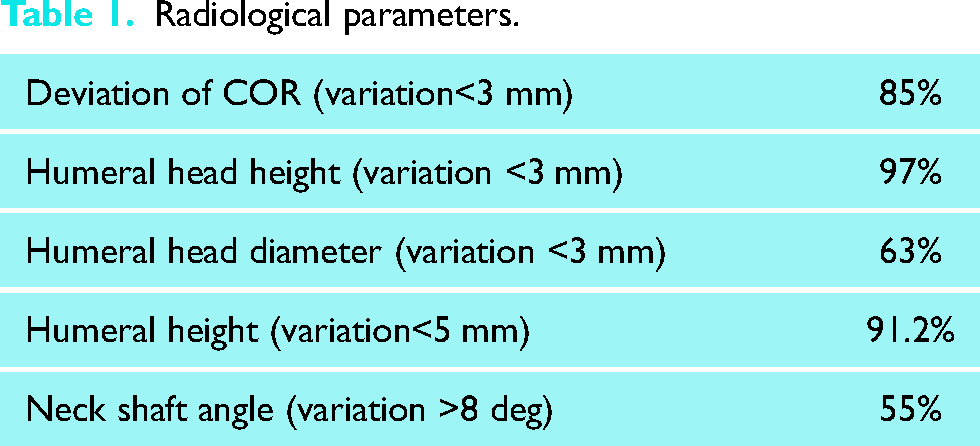
The deviation of COR of the prosthesis from the anatomical centre was less than 3 mm in 58 cases (85%). Humeral head height and humeral head diameter showed a variation of less than 3 mm in 66 cases (97%) and 43 cases (63%) respectively. Humeral height followed a similar trend, with 62 cases (91.2%) showing a difference of less than 5 mm. The neck shaft angle showed a variation of more than 8 degrees in 38 cases (55%), and 29 cases (42.6%) had a postoperative angle of less than 130 degrees.
Conclusion
Overall, stemless total shoulder arthroplasty with the Affinis Short prosthesis allows excellent restoration of anatomy confirmed by most of the measured radiographic parameters. The variability in neck shaft angle might be due to differing surgical techniques, with some surgeons preferring a slightly vertical neck cut to protect the rotator cuff insertion.
Introduction
Restoration of biomechanics is one of the most important goals in total shoulder arthroplasty. Results after shoulder arthroplasty in terms of functional outcomes and implant survivorship have improved possibly due to better restoration of anatomy with the newer implant designs. 1
Use of stemmed components can however lead to stem-related complications, such as bone loss secondary to stress shielding and humeral fractures.2–5 Stemmed implants rely on diaphyseal fixation, and the glenohumeral relationship is determined by the head position relative to the stem and the alignment of the stem within the humeral shaft. 6 Although the humeral component design has evolved, restoration of anatomy (humeral offset and centre of rotation) is not always achieved with the new modular designs.7,8
There is a theoretical advantage of better restoration of anatomy with stemless implants. Stem related complications are also eliminated. Since stemless implants are based on metaphyseal fixation, Glenohumeral relationship is not dependant on the relationship between the diaphysis and humeral head. 9 There is, however, more potential to vary the neck shaft angle. Modern concepts in shoulder arthroplasty have recently focused on exact restoration of the centre of rotation of the glenohumeral joint.10–16
Presently a number of stemless shoulder arthroplasty prostheses are available, 17 with limited clinical data showing encouraging results.18–22 Although a variety of different prostheses have been looked at, no study on the Affinis short implant has specifically evaluated the restoration of radiographic geometry.21–24
The purpose of this study was to evaluate the restoration of anatomy following Total Shoulder arthroplasty with stemless Affinis Short implant (Mathys, Bettlach) in patients with primary glenohumeral osteoarthritis.
Materials and methods
This was a retrospective study of all patients who had undergone Total Shoulder Arthroplasty (TSA) using the Affinis Short prosthesis for primary osteoarthritis (OA) between 2010 and 2016. The Affinis Short prosthesis is an uncemented metaphyseal anchoring humeral stemless prosthesis, with a Titanium humeral component coated with bioactive calcium phosphate and a ceramic head.
Inclusion criteria were patients with primary OA who had undergone stemless total anatomic shoulder arthroplasty. Patients with post-traumatic OA, bone-stock insufficiency, revision, previous surgeries, inflammatory arthropathies (eg. Rheumatoid arthritis) or stemmed humeral implants were excluded. All procedures were performed by fellowship trained shoulder surgeons.
A total of 72 patients were recruited in the study. However, 2 patients were excluded due to poor quality of radiographs. Mean age of the study group was 70 years (range 55–84 years) at the time of surgery, with a mean follow up of 42.8 months. The surgery was performed using the deltopectoral approach. All patients underwent the department's standard postoperative rehabilitation protocol, and were reviewed at 6 weeks, 3 months and 1-year follow up, and subsequently every year.
True anteroposterior radiographs with neutral rotation of the humerus and axillary radiographs were obtained at each follow up visit.
Radiological analysis was performed on the AP radiograph using the Picture Archiving and Communication System (PACS). One independent observer carried out all radiographic measurements to calculate the baseline and intra observer variability. The same set of measurements was carried out by another observer to calculate the inter observer variability. Premorbid humeral head anatomy was estimated by a best-fit circle method according to previous studies18,25 The premorbid Centre of Rotation (COR) was assessed using the best fit circle method using the PACS software. The importance of three bony landmarks: lateral cortex of the greater tuberosity (GT), the medial edge of the GT at the supraspinatus insertion and the medial calcar at the inflection point where the calcar meets the articular surface, have been well described. 25 Importantly, they are not altered by the osteoarthritic articular surface.
The pre and postoperative radiographs were assessed for deviation of Centre of Rotation (devCOR), Humeral Head Height (HHH), Humeral Head Diameter (HHD), Humeral Height (HH), and Neck Shaft Angle (NSA) (Figure 1). As described by Alolabio et al., 18 a deviation of more than 3 mm was considered as being clinically significant. The various parameters have been described in Table 1.

Radiographic measurements performed preoperatively (left) and postoperatively (right). Humeral Height (HH); Humeral Head Height (HHH); Humeral Head Diameter (HHD); deviation of Centre of Rotation (devCOR); Neck Shaft Angle (NSA).
Radiological parameters.
Premorbid humeral head anatomy was measured by a best-fit circle in the anteroposterior (AP) view. The small arrows in the figure represent non articular landmarks. The anatomic neck was defined as the line between the small arrow markers on the humeral head. The Centre of Rotation (COR) was then identified and the distance to anatomical neck calculated in millimetres (deviation of COR). Humeral head height (HHH) is defined as the perpendicular linear distance from the anatomic neck to the apex of the circle. Neck-shaft angle (NSA) was measured as the angle between a line perpendicular to the anatomic neck and long axis of humeral diaphysis. Humeral height (HH) was defined as the distance between the top of greater tubercle and the highest point on the humeral head
Post-operative radiographic measurements included the same parameters. The Centre of Rotation (COR) was identified by fitting a circle to the curvature of the humeral head prosthesis, and the distance to the lower margin of the prosthetic head was calculated in millimetres (deviation of Centre of Rotation (devCOR). Humeral head height (HHH) was measured from the lower margin of the prosthetic head to the top of the prosthetic humeral head. Neck-shaft angle (NSA) and Humeral height (HH) were measured in the same way as pre-operative measurements.
Statistical analysis
Statistical analysis was performed using the paired t- test for comparison between pre and post-operative geometrical measurements. Descriptive analyses were reported as means, standard deviation(SD) and ranges. A statistical review was conducted by a biomedical statistician.
The intraclass correlation coefficient (ICC) (with 95% confidence interval [CI]) was used to evaluate the intra and interobserver variability.
Results
The various radiological parameters assessed on pre and post op radiographs using the best fit circle method were deviation of Centre of Rotation (devCOR), Humeral Head Height (HHH), Humeral Head Diameter (HHD), Humeral Height (HH) and Neck Shaft Angle (NSA). The variations between pre and post op values are depicted in percentage in table below.
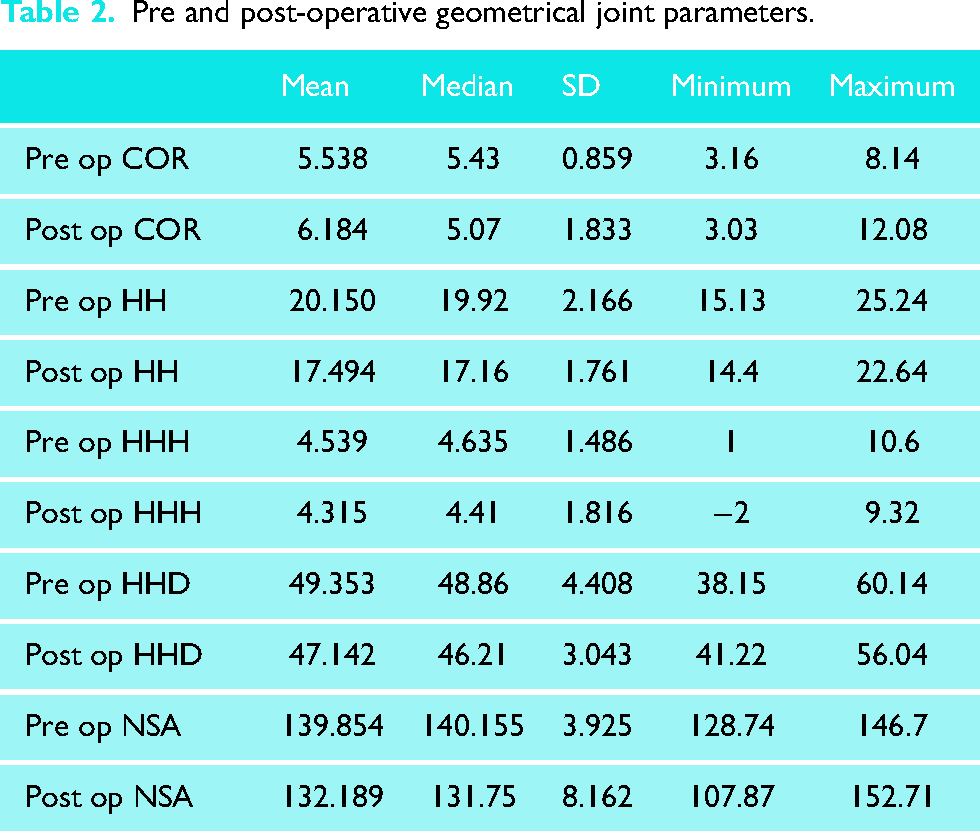
As seen in data from Table 1 and 2, the preoperative versus postoperative radiographs demonstrated no significant differences in COR (5.538 vs 6.184, p value = 0.9977), HHH (4.539 vs 4.315, p value = 0.1031). However, HHD (49.353 vs 47.142, p value<0.05), NSA (139.854 vs 132.189, p value <0.05) and HH (20.150 vs 17.494, p value<0.05) showed significant variation between pre and postoperative measurements (Table 3).
Pre and post-operative geometrical joint parameters.
Radiological pre and post-operative shoulder measurements.
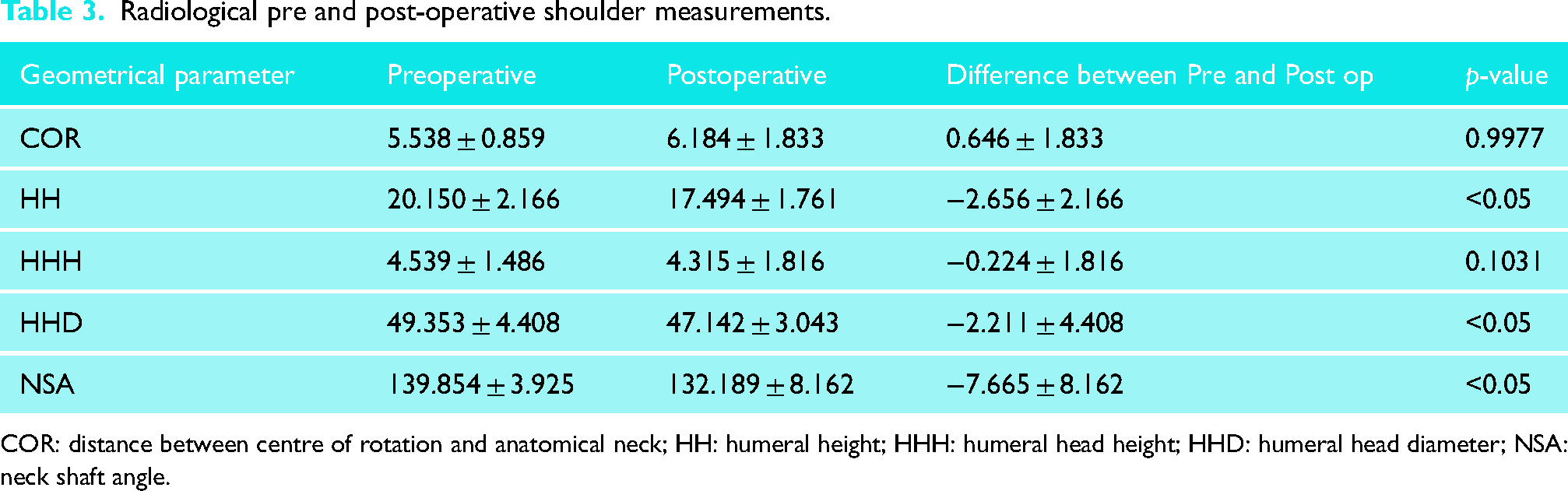
COR: distance between centre of rotation and anatomical neck; HH: humeral height; HHH: humeral head height; HHD: humeral head diameter; NSA: neck shaft angle.
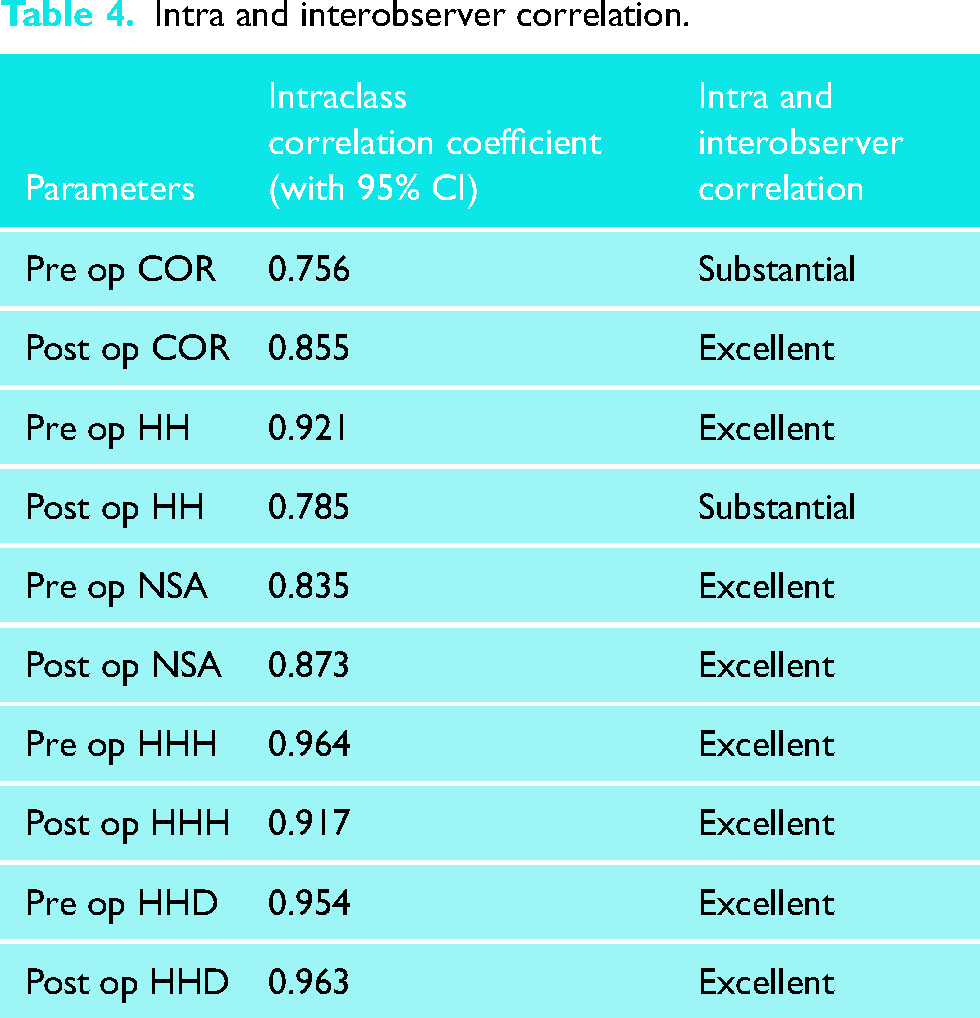
The intraclass correlation coefficient (ICC) (with 95% confidence interval [CI]) was used to evaluate the intra and interobserver variability. For the ICC, a value of 0.00 to 0.20 was considered slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, excellent. 9 All the parameters showed a value in substantial to excellent range demonstrating very low variability (Table 4).
Intra and interobserver correlation.
Discussion
Humeral replacement was originally described by Neer 26 who pioneered the development of implants and surgical techniques. Proximal humeral anatomy, including humeral head size, version, offset, and inclination, varies widely.27–29 Current humeral components are available in a wide range of sizes and include a greater range of modularity between the stem and head to accommodate variability in proximal humeral anatomy. 6
Accurate restoration of the glenohumeral anatomy is essential for the success of Total Shoulder Arthroplasty.1,19,20,30 The anatomic reconstruction of the glenohumeral joint, specifically the humeral head, restores physiological motion, muscle alignment, glenohumeral contact position, and bone stress distribution and prevents glenoid loosening via eccentric glenoid loading. 31 Coracoacromial impingement and rotator cuff damage can occur with malpositioning of the prosthetic head. 32 In stemless arthroplasty, post-osteotomy, the arthritic humeral head is replaced with a concentric implant. In stemmed implants, an appropriately sized head may need to be eccentrically dialled to restore the native anatomy.
Anatomical restoration after shoulder arthroplasty can generally be assessed in two ways, either by comparing anatomy of the operated shoulder with the contralateral side or with its premorbid anatomy.18,25 Youderian et al. demonstrated that premorbid HH size and COR in the arthritic shoulder can be accurately predicted from preserved non-articular bony landmarks by a best-fit sphere or circle fitted to the proximal humerus. 25
One of the first stemless implants with metaphyseal fixation, with the aim of complete elimination of humeral stem was introduced in 2004. 33 Apart from prevention of stem related complications like periprosthetic fractures, preserving bone stock; the stemless implants should also provide other potential benefits including the ability to perform anatomic reconstruction regardless of the posterior offset of the proximal humerus.21,34
Our study with a stemless prosthesis highlights the approximation of the native anatomy of the shoulder. The results depicted excellent restoration of the anatomy using the various radiological parameters like deviation of Centre of Rotation (devCOR), Humeral Head Height (HHH), Humeral Head Diameter (HHD), Humeral Height (HH), and Neck Shaft Angle (NSA).
The preoperative versus postoperative radiographs demonstrated no statistically significant differences in COR and HHH.
Kadum et al. 23 performed a geometrical analysis of 70 stemless TSAs using AP radiographs, finding the COR within 1 ± 2 mm; HHH, 1 ± 3 mm; and HNA, 3 ± 12. Using computed tomography for a similar assessment of 66 shoulders, they found a closer re-creation of the preoperative anatomy, with the COR within 0 ± 2 mm; HHH, 1 ± 2 mm; HNA, 2 ± 10; and LHO, 1.3 ± 5 mm. The similarities between these radiographic measures and those in our study are encouraging.
Further similar studies18–20 have shown a deviation of Centre of Rotation of more than 3.0 mm to be detrimental and leads to overstuffing and poor functional outcomes.
Although the geometric parameters, HHD and HH, reported statistically significant differences between pre and postoperative measurements, the actual values restored post operatively were within previously described acceptable ranges (less than 3 mm and 5 mm respectively)35,36
Post-operative HHD was on average 2.21 mm less than the pre-operative measurement. Pinto et al. showed a similar reduction in HHD −1.7 mm, identifying a tendency to slightly undersize the humeral head in stemless implants. A difference of less than 3 mm was deemed to be acceptable, Undersizing, is preferable to an oversized head and subsequent overstuffing.
In our study, NSA was 139 ± 4 deg pre-operatively compared with 132 ± 8 deg post-operatively. There were 30/70 (43%) shoulders with post-operative NSA <130 deg, which shows a tendency to put the prosthesis in varus. Kadum et al. 23 showed similar findings with a reduction in NSA post-operatively and a significant proportion of implants in a slight varus inclination. The humeral osteotomy for the Affinis short prosthesis is at the surgeon's discretion and not determined by the use of intra-medullary alignment jigs. The aim is to replicate the natural orientation of the native humeral neck without violating the cuff insertion. Efforts to protect the cuff insertion superiorly may predispose to favouring a steeper or more varus cut. The Centre of Rotation, however, appears to be maintained despite a varus inclination (Figures 2 and 3).
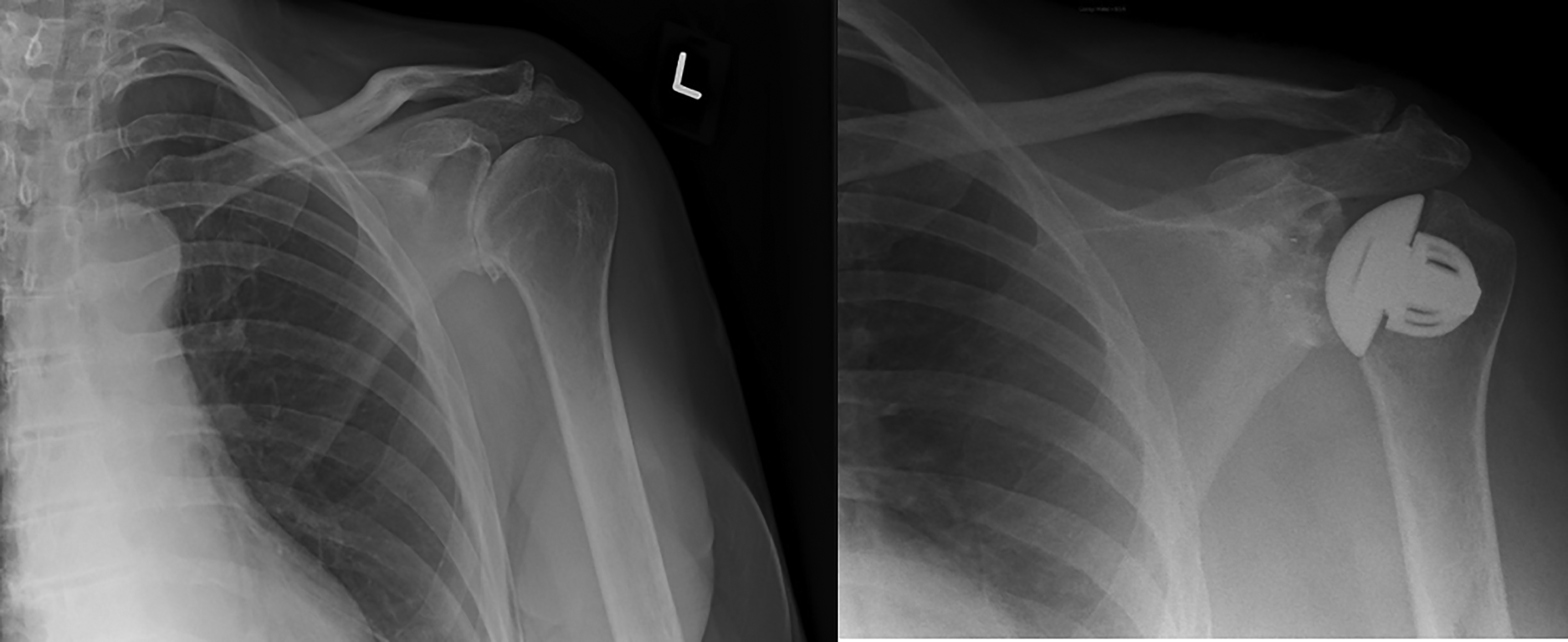
Pre and post-operative radiograph showing varus positioning of the implant. Difference in deviation of COR was still less than 3 mm.
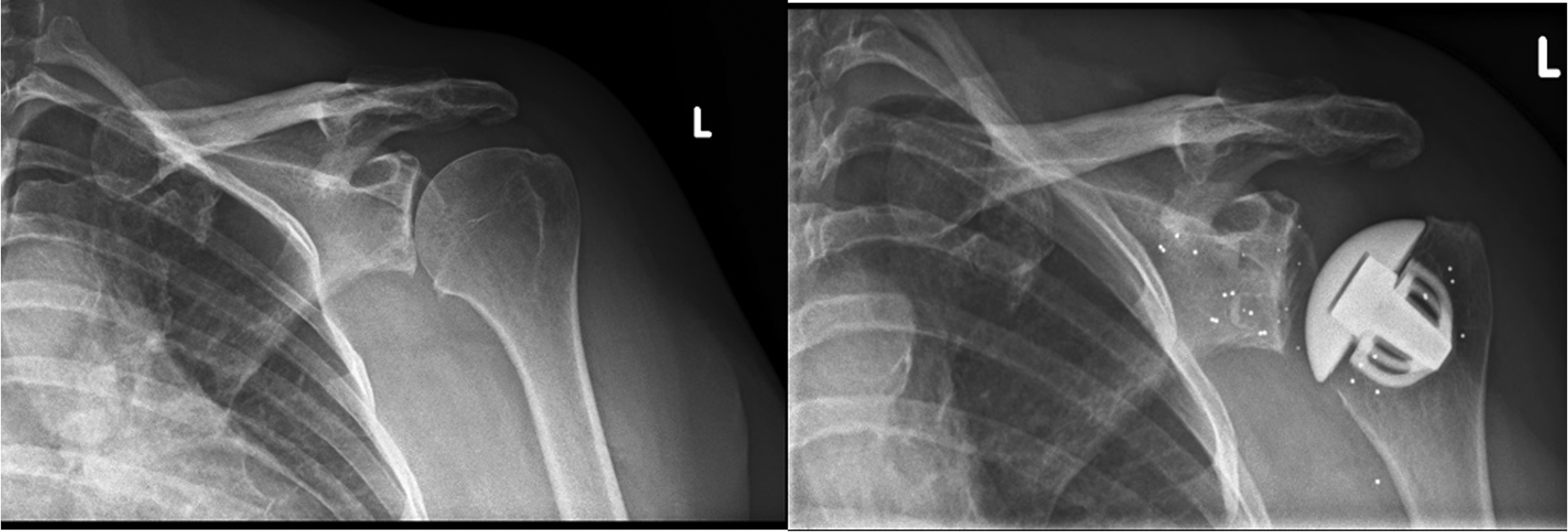
Pre and post-operative radiograph showing minimal variation in neck shaft angle compared to preoperative measurement. Difference in deviation of COR was less than 3 mm. Note presence of RSA beads in post-op Xray.
Our findings show the Affinis Short prosthesis reliably restores the humeral head into an acceptable anatomic position. The generally accepted most important factors are ensuring that the deviation of Centre Of Rotation is less than 3 mm and change in Humeral Head Height is less than 5 mm.20,23,37 Our results show that the Affinis Short prosthesis achieves this in the majority of cases (85%).
We acknowledge that our study had some limitations. The radiographic measurements were measured on plain X-ray, which could be subject to projection errors
Clinical correlation with the radiological measurements would have been preferable but was outwith the scope of this purely radiological evaluation project. However, mid-term outcomes for this prosthesis have been reported by our unit, with little evidence of aseptic loosening of either component. 38
Conclusion
Overall we have shown that stemless TSA using the Mathys Affinis implant seems to accurately re-produce the native glenohumeral joint anatomy. In particular, deviation of Centre of Rotation and Humeral Head Height, the most important measurements with regards to function and clinical outcomes in other studies, seem to be within the desired range in the majority of cases. A tendency for a varus neck shaft angle due to avoidance of the superior cuff insertion has been noted. This did not, however, appear to affect the other measured parameters.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.