
Abstract
Introduction
As the utilization of total shoulder arthroplasty (TSA) increases, it is essential to identify risk factors associated with postoperative complications. Urinary tract infection (UTI) is one such example. Our objective is to identify whether UTI is associated with increased rates of prosthetic joint infection (PJI) and determine whether its treatment reduces PJI rates.
Methods
Patients who underwent primary TSA for glenohumeral osteoarthritis between 2010 and 2019 with minimum two-year follow-up were identified in a national database (PearlDiver Technologies) using Current Procedural Terminology and International Classification of Diseases codes. These patients were stratified into two cohorts: those with preoperative UTI within two weeks of TSA and those without. The preoperative UTI cohort was stratified into those treated and those untreated prior to TSA. Univariate and multivariable analyses were performed.
Results
Following multivariable analysis, there were significantly higher odds of postoperative anemia, pulmonary embolism, and death in the UTI cohort. Comparing treated to untreated UTI, there were no significant differences in multivariable analysis for any 90-day medical or two-year surgical complications.
Discussion
This study showed that UTI was not associated with increased rates of PJI. UTI was, however, associated with postoperative medical complications that surgeons should be aware of.
Introduction
Prosthetic joint infection (PJI) is one of the most severe complications following total joint replacement, with direct consequences to patients including additional healthcare costs, time missed from work, long-term disability, and potentially death.1–3 In total shoulder arthroplasty (TSA), the incidence of PJI is ∼1% in primary replacements, with an increase to between 4% and 15.4% in revision arthroplasty.1,4–6 As the number of shoulder replacements performed each year increases, so too does the number of prosthetic joint infections. 7
To combat the growing clinical and economic burden associated with PJI, much of the existing literature has been aimed at identifying risk factors that predispose individuals to infection.1,8–10 One such example is urinary tract infection (UTI), whereupon hematogenous spread of microorganisms from the genitourinary system have the potential to seed the prosthetic joint, leading to infection and ultimately failure of the prostheses. 11 Close evaluation of this risk factor becomes especially important when considering the increasing number of older candidates for TSA. 12 Older adults have demonstrated to have an incidence of UTI as high as 32% for those aged 65–75 and 48% in those aged 75–85. 13 Given the increased incidence of UTI and the concurrent increase in TSA in this population, preoperative UTI as a risk factor for PJI is particularly worth investigating.
The current literature on preoperative UTI in TSA is sparse; with a more robust body of evidence focused on total hip arthroplasty (THA) and total knee arthroplasty (TKA). Many recent studies have focused on asymptomatic bacteriuria (ASB), rather than true, symptomatic UTI.14,15 Recent THA/TKA literature suggests that addressing ASB prior to joint replacement is unnecessary and that screening and treatment should be reserved for patients who exhibit symptoms of UTI.15,16 This recommendation, however, garnered a consensus vote of only 74% when voted upon by a panel of over 400 experts from various medical disciplines. 10 Despite a lack of conclusive evidence, some physicians continue to employ conservative measures such as antibiotic prophylaxis or routine urinary screening before electing to proceed with surgery. 17 Furthermore, because the existing literature focuses so heavily on THA/TKA, clinicians are often left to extrapolate these data to make clinical decisions regarding the TSA population.
To help fill this gap in the literature, the purpose of this paper is to (1) investigate whether UTI in the preoperative period is associated with PJI in patients undergoing TSA, (2) evaluate whether treatment of the UTI impacts two-year postoperative outcomes, and (3) determine what other complications may be anticipated in the following 90-day postoperative period in the setting of a preoperative UTI. We predict there to be no association between preoperative UTI and rates of PJI at two years following the index shoulder arthroplasty.
Methods
Patients who underwent TSA from the Mariner dataset of the PearlDiver database (PearlDiver Technologies; www.pearldiverinc.com, Colorado Springs, CO). The Mariner dataset includes all-payers claims information from 2010 to 2019 of over 120 million patients that are identified by International Classification of Diseases (ICD) codes and Current Procedural Terminology (CPT) codes. The dataset provides longitudinal follow-up based on a unique patient identifier. If a patient does not have activity based upon the follow-up window, they were assumed to be lost to follow-up and excluded from the study. Patients who underwent primary TSA were identified based on ICD 9/10 procedure codes and CPT codes (Appendix 1). These patients were then filtered into those who had a symptomatic UTI within two weeks of TSA and those that did not based on ICD 9/10 diagnosis codes (Appendix 1). The preoperative UTI cohort was further stratified into those who were treated preoperatively and those who were not. The treated cohort was defined as patients prescribed antibiotics within two weeks of TSA (Appendix 1).
Patients were excluded if they were <18 years of age, had a simultaneous or staged bilateral TSA or had TSA performed related to a diagnosis of cancer, trauma, or fracture. Staged or bilateral TSA was discerned based on whether the same patient had claims information for another TSA after the primary and was excluded to control for laterality for revision complications. Patients were included only if they underwent TSA for a diagnosis of osteoarthritis, as determined by ICD codes. Patients were also excluded if they did not have at least a two-year minimum follow-up. Exclusion and inclusion criteria are shown in Figure 1.
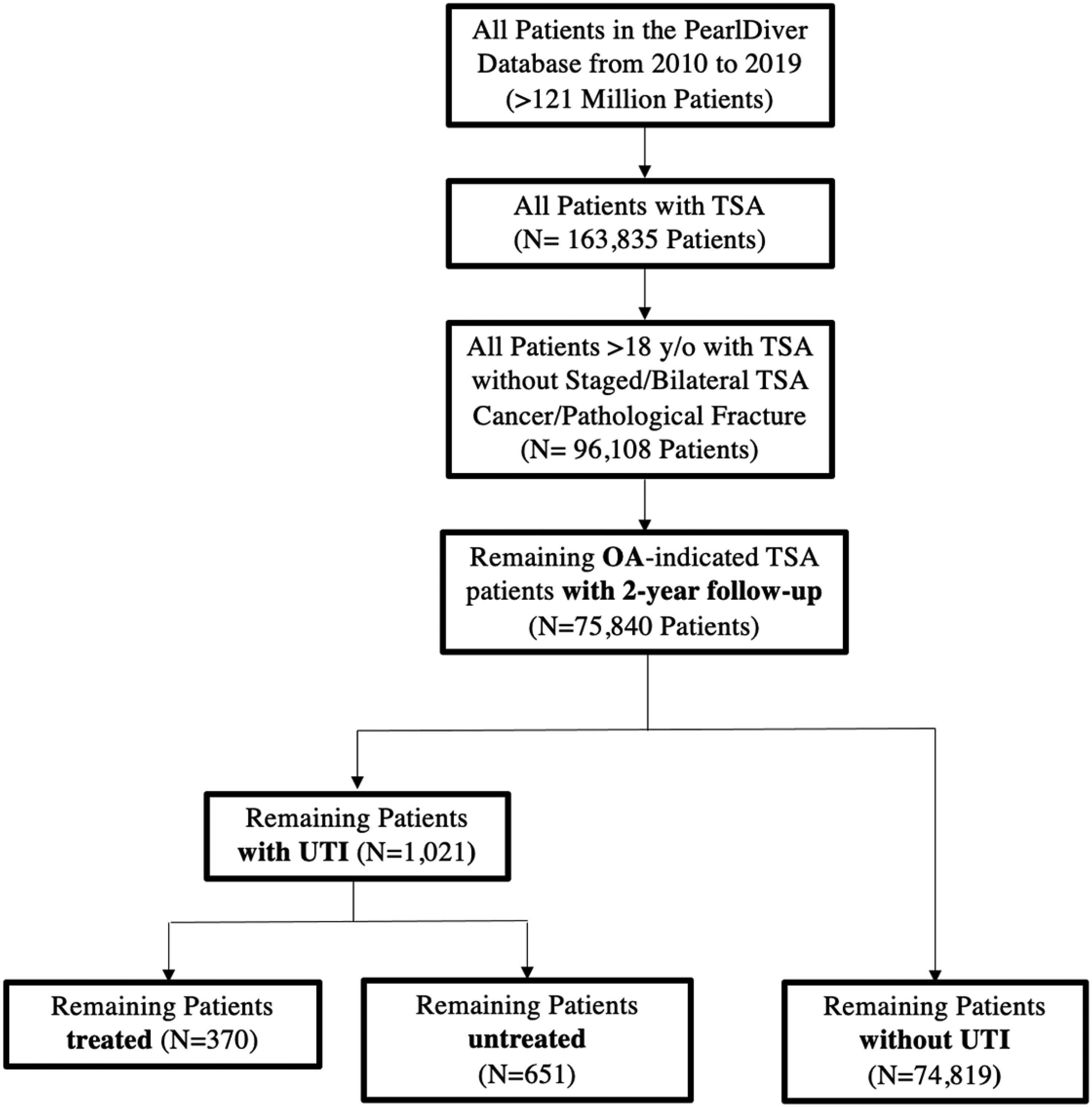
Inclusion and exclusion criteria for defined cohorts. Notes: Patients were stratified based on preoperative UTI diagnosis and whether treatment was received. Final analysis included 370 patients with treated UTI, 651 patients with untreated UTI, and 74,819 controls, with no UTI. OA: Osteoarthritis; TSA Total Shoulder Arthroplasty; UTI: Urinary Tract Infection; Treated: Treated for UTI; Untreated: Untreated for UTI
The demographic data collected included age, gender, and all Elixhauser comorbidities for each cohort. 18 Primary outcomes were two-year surgical complications including all-cause revision, periprosthetic joint infection (PJI), and manipulation under anesthesia (MUA). Revision and MUA were defined using CPT codes. PJI-indicated revisions were defined using the ICD 9/10 diagnosis codes for PJI at the same dates as the CPT code for revision TSA. Secondary outcomes were 90-day readmissions and medical complications of surgical site infection (SSI), renal failure, postoperative anemia, atrial fibrillation, arrhythmia without atrial fibrillation, bleeding complications, blood transfusion, pneumonia, stroke, death, deep vein thrombosis (DVT), heart failure, pulmonary embolism (PE), respiratory complications, and sepsis. All medical complications were defined using ICD 9/10 diagnosis codes. SSI differs from PJI in that PJI requires revision arthroplasty, with the infection penetrating the prosthesis. SSI is limited to the skin and typically does not require surgical intervention. These are discerned based on the ICD 9/10 diagnosis codes.
Statistical analysis
The data on patient demographics, comorbidities, and 90-day complications were first assessed using univariate analysis using R software (R Foundation for Statistical Computing, Vienna, Austria) provided by PearlDiver. Univariate analysis was conducted using chi-squared and student t-tests where appropriate. All 90-day outcomes and two-year revisions with a p-value <0.2 were included as dependent variables in the multivariable analysis. To control for potential confounding variables, all demographics, and comorbidities with a p-value <0.02 were included as independent variables in each multivariable analysis. Multivariable analysis was performed using logistic regression in R software provided by PearlDiver. P-value <0.05 was utilized as the level of significance.
Results
In total, 75,480 patients were included in this study. Of these, 1021 patients were diagnosed with preoperative UTI and 74,819 were not. Of the 1021 patients with preoperative UTI, 370 patients were treated with preoperative antibiotics and 651 patients were not.
Demographics and comorbidities
Patients with preoperative UTI prior to TSA were more likely to be older (p < 0.001), female (p < 0.001), and smokers (p = 0.033); more likely to have congestive heart failure (p < 0.001), arrhythmias (p < 0.001), valvular disease (p < 0.001), pulmonary circulatory diseases (p < 0.001), peripheral vascular diseases (p < 0.001), hypertension (p < 0.001), paralysis (p < 0.001), other neurological disorders (p < 0.001), chronic pulmonary disease (p < 0.001), diabetes mellitus (p < 0.001), hypothyroidism (p < 0.001), renal failure (p < 0.001), liver disease (p = 0.047), rheumatoid arthritis and collagen vascular diseases (p < 0.001), coagulopathy (p < 0.001), fluid and electrolyte disorders (p < 0.001), blood loss anemia (p < 0.001), iron deficiency anemia (p < 0.001), psychosis (p = 0.019), and depression (p < 0.001) when compared to the control cohort of those without preoperative UTI (Table 1).
Patient demographics and comorbidities for OA-indicated TSA: patients with UTI compared to those without UTI.
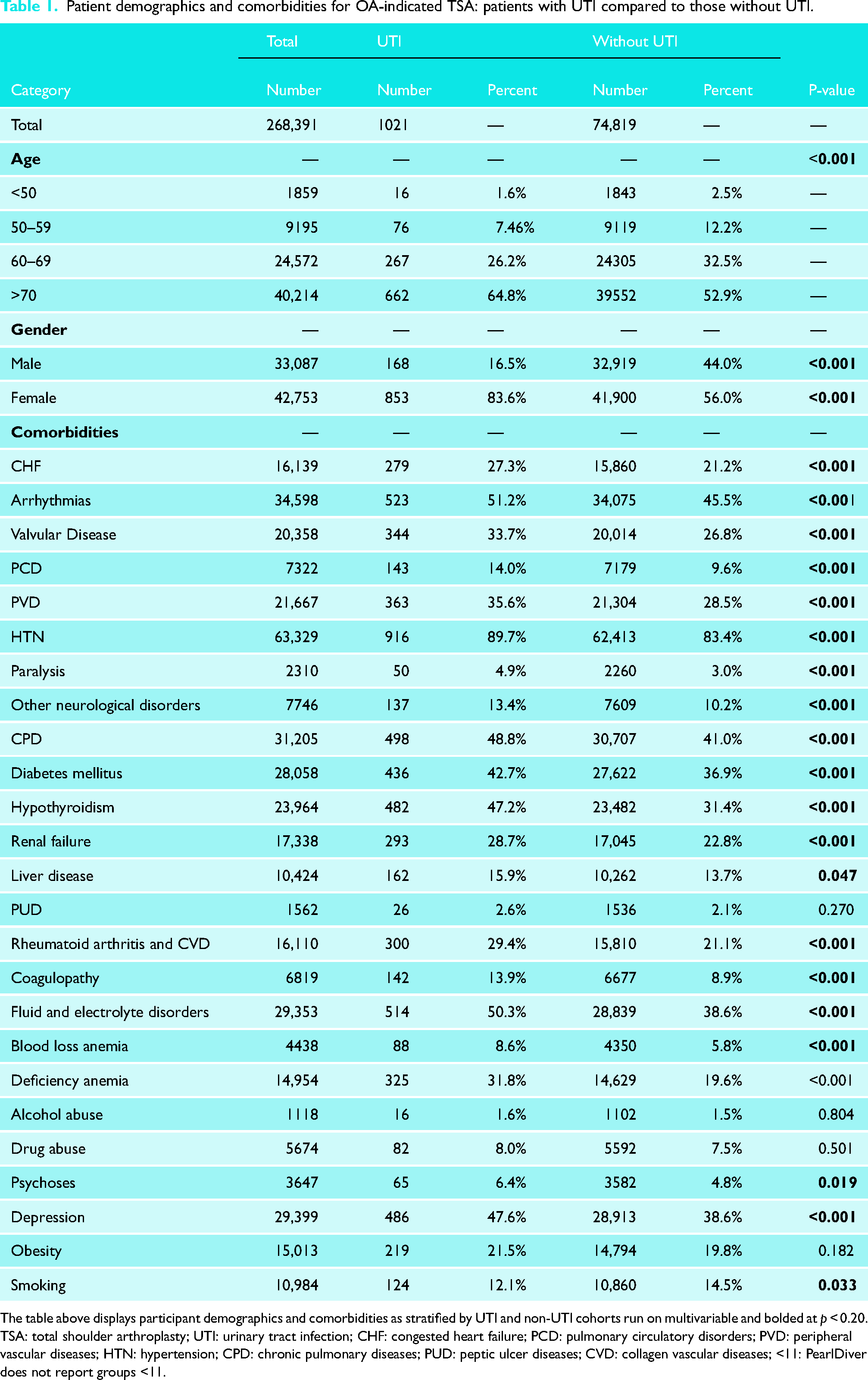
The table above displays participant demographics and comorbidities as stratified by UTI and non-UTI cohorts run on multivariable and bolded at p < 0.20.
TSA: total shoulder arthroplasty; UTI: urinary tract infection; CHF: congested heart failure; PCD: pulmonary circulatory disorders; PVD: peripheral vascular diseases; HTN: hypertension; CPD: chronic pulmonary diseases; PUD: peptic ulcer diseases; CVD: collagen vascular diseases; <11: PearlDiver does not report groups <11.
Patients with preoperative UTI treated prior to TSA were more likely to be female (p < 0.001) and smokers (p < 0.001); and more likely to have valvular disease (p = 0.043), coagulopathies (p = 0.019), when compared to those with untreated preoperative UTI (Table 2).
Patient demographics and comorbidities for OA-indicated TSA: patients with treated UTI compared to those with untreated UTI.
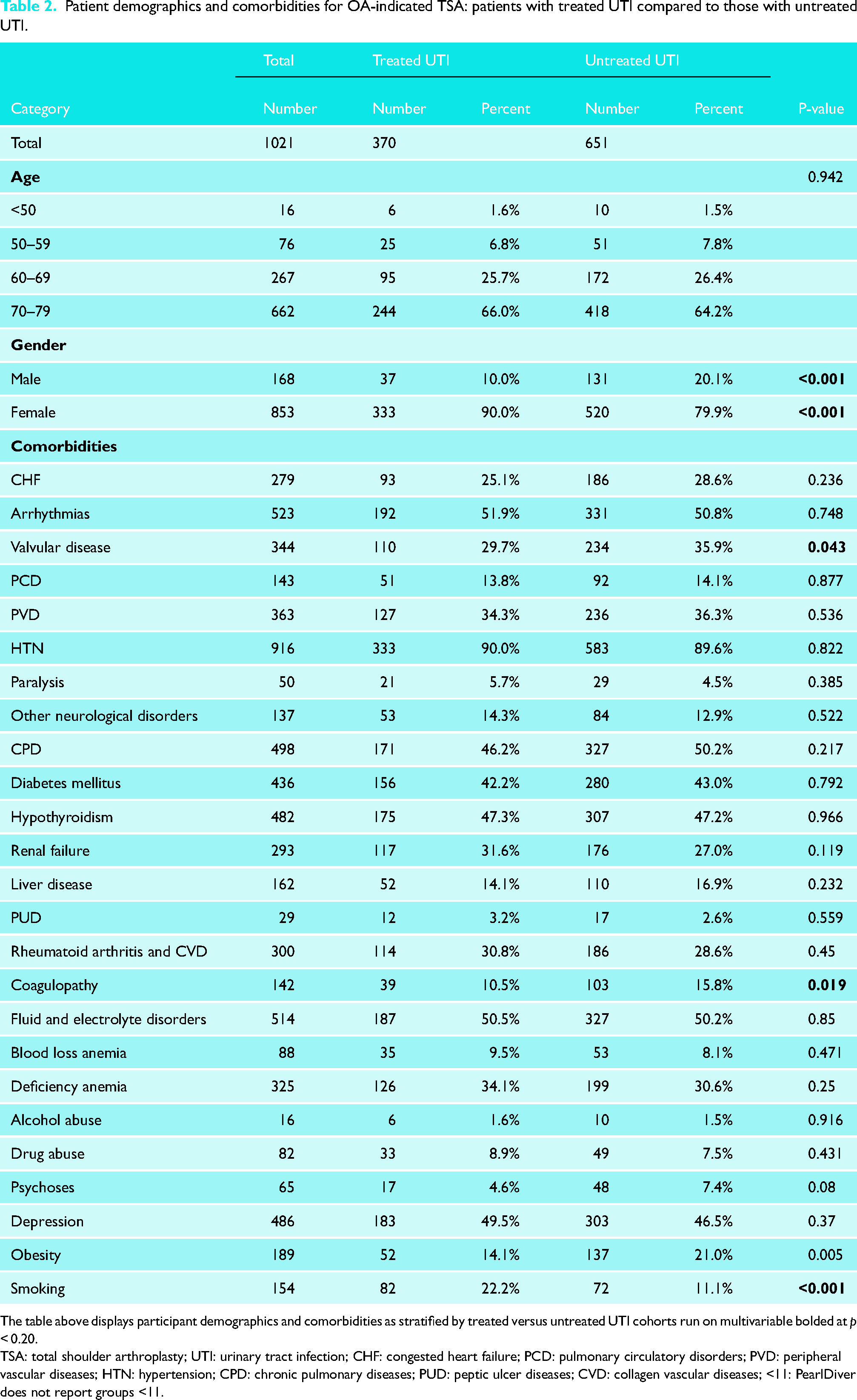
The table above displays participant demographics and comorbidities as stratified by treated versus untreated UTI cohorts run on multivariable bolded at p < 0.20.
TSA: total shoulder arthroplasty; UTI: urinary tract infection; CHF: congested heart failure; PCD: pulmonary circulatory disorders; PVD: peripheral vascular diseases; HTN: hypertension; CPD: chronic pulmonary diseases; PUD: peptic ulcer diseases; CVD: collagen vascular diseases; <11: PearlDiver does not report groups <11.
Univariate complications
Within 90 days postoperatively, patients with preoperative UTI had a significantly higher incidence of renal failure (2.4% [24] vs. 1.4% [1018]; p = 0.007), postoperative anemia (4.7% [48] vs. 2.5% [1903]; p < 0.001), atrial fibrillation (8.6% [88] vs. 7.0% [5209]; p = 0.039), blood transfusion utilization (2.0% [20] vs. 1.2% [914]; p < 0.001); death (0.5% [<11] vs. 0.1% [77]; p < 0.001), DVT (1.8% [18] vs. 1.0% [717]; p = 0.009); PE (1.9% [19] vs. 0.8% [591]; p < 0.001), when compared to the control cohort of those without preoperative UTI (Table 3). In terms of two-year surgical complications, there were no significant differences between the two cohorts in the rates of PJI, revision surgery, or MUA. There were no significant differences in two-year surgical complications or 90-day medical complications when comparing those with treated preoperative UTI to those with untreated preoperative UTI (Table 4).
Two-year surgical and 90-day medical complications for OA-indicated TSA: univariate analysis of patients with UTI compared to those without UTI.
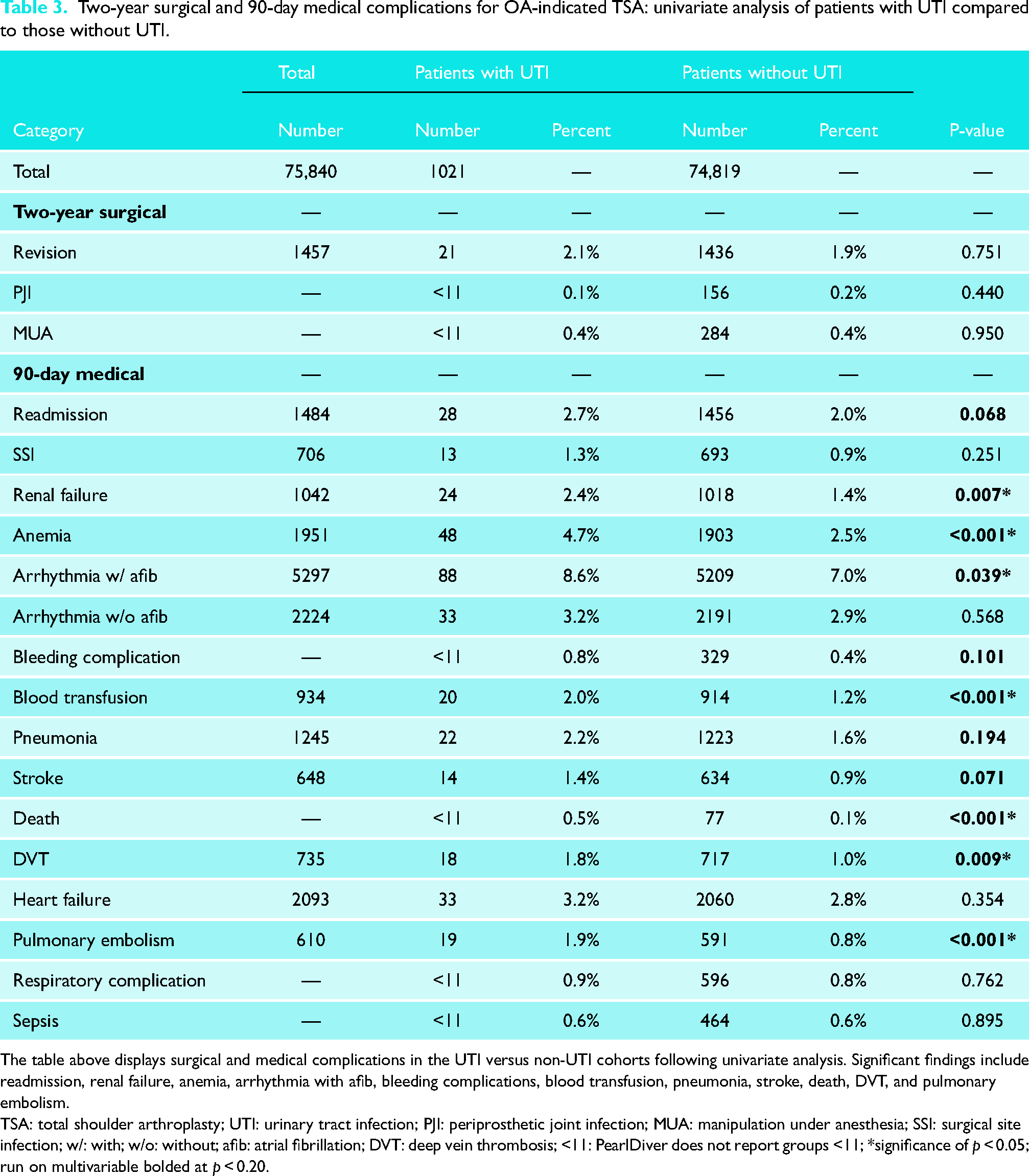
The table above displays surgical and medical complications in the UTI versus non-UTI cohorts following univariate analysis. Significant findings include readmission, renal failure, anemia, arrhythmia with afib, bleeding complications, blood transfusion, pneumonia, stroke, death, DVT, and pulmonary embolism.
TSA: total shoulder arthroplasty; UTI: urinary tract infection; PJI: periprosthetic joint infection; MUA: manipulation under anesthesia; SSI: surgical site infection; w/: with; w/o: without; afib: atrial fibrillation; DVT: deep vein thrombosis; <11: PearlDiver does not report groups <11; *significance of p < 0.05; run on multivariable bolded at p < 0.20.
Two-year surgical and 90-day medical complications for OA-indicated TSA: univariate analysis of patients with treated UTI compared to those with untreated UTI.
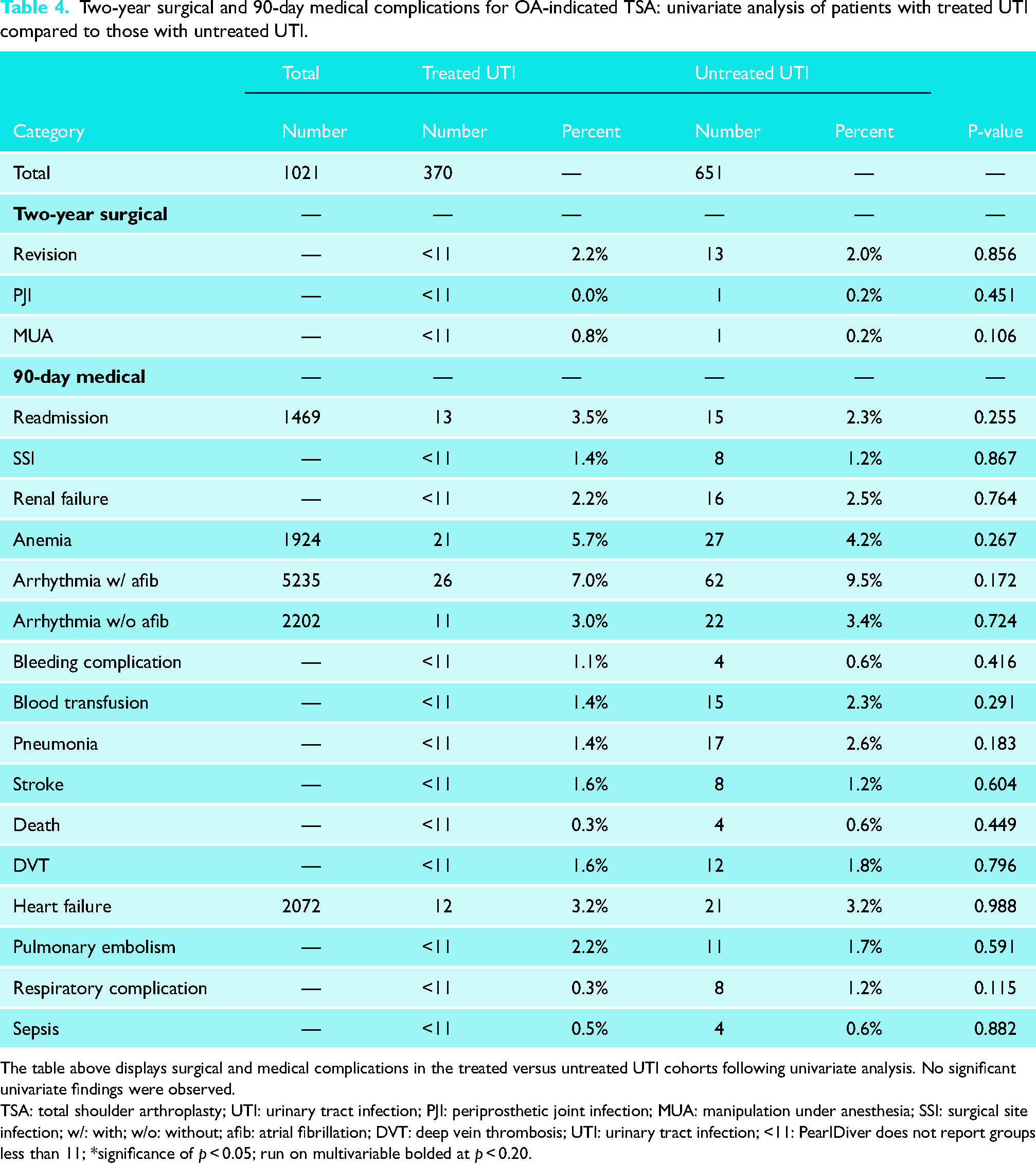
The table above displays surgical and medical complications in the treated versus untreated UTI cohorts following univariate analysis. No significant univariate findings were observed.
TSA: total shoulder arthroplasty; UTI: urinary tract infection; PJI: periprosthetic joint infection; MUA: manipulation under anesthesia; SSI: surgical site infection; w/: with; w/o: without; afib: atrial fibrillation; DVT: deep vein thrombosis; UTI: urinary tract infection; <11: PearlDiver does not report groups less than 11; *significance of p < 0.05; run on multivariable bolded at p < 0.20.
Multivariable analysis of complications
Following multivariable analysis, patients with UTI had an increased likelihood of having postoperative anemia (OR = 1.4, 95% CI, 1.1–1.9; p = 0.019), PE (OR = 1.9, 95% CI, 1.1–3.0; p = 0.008), and death (OR = 3.2, 95% CI, 1.1–7.3; p = 0.013), when compared to the control cohort of those without UTI (Figure 2).
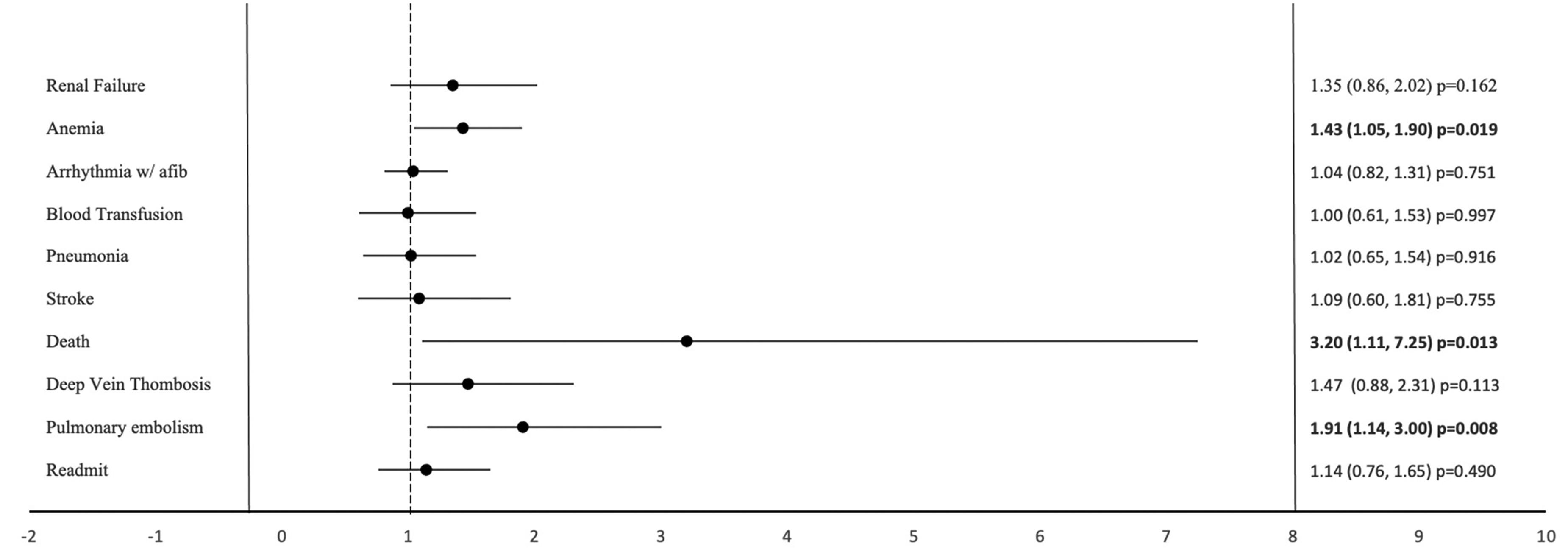
Two-year surgical and 90-day medical complications for OA-indicated TSA: a multivariable analysis of odds ratios for patients with UTI compared to those without UTI. Notes: Figure displays odds ratios comparing surgical and medical complications in the UTI vs non-UTI cohorts, bolded for p-values <0.05. Significant findings include increased rates of anemia, death, and pulmonary embolism in the UTI cohort.
Discussion
In the present study, we found no significant differences in two-year postoperative outcomes, including PJI, revision, and MUA when comparing the UTI cohort to the non-UTI cohort. There were, however, notable differences in 90-day complications between these cohorts. Namely, the rate of postoperative anemia, PE, and mortality was more common among the UTI cohort compared to the non-UTI cohort. When comparing the treated to untreated UTI cohorts, there were no significant differences in all two-year revisions, regardless of indication, or any 90-day medical complications.
Prior to our study, the current literature remains unconvincing in its findings on the effects of preoperative UTI on arthroplasty outcomes. While some authors have successfully opted to continue with surgery despite preoperative UTI status, others are more conservative in their approach—first ensuring eradication of the infectious organism. 19 Recently, Schmitt et al. 15 examined data from the National Surgical Quality Improvement Program database to argue that postoperative UTI did significantly increase the risk for PJI in patients undergoing THA/TKA, while preoperative UTI did not. Similarly, from 2001 to 2006 Pulido et al. 9 prospectively collected data on 9245 patients undergoing THA or TKA and identified postoperative UTI as an independent risk factor for PJI. Based on their finding, they began preoperative UTI screening to identify and eradicate infection before proceeding with arthroplasty. Their study followed the assumption that postoperative UTIs can be prevented with preoperative treatment. However, there are many elements unique to the postoperative setting that may not be applicable to preoperative UTIs, regardless of preoperative screening and treatment. For example, patients with extended postoperative lengths of stay may be predisposed to nosocomial UTI. Inherently, acquiring a UTI in the hospital represents a different demographic of patients and likely a more resistant population of microorganisms when compared to preoperative, community-acquired UTI. Further, a longer postoperative inpatient period may represent innate characteristics within the patient that cannot be predicted solely by preoperative UTI screening.
The results of this study suggest that to delay total shoulder replacement in favor of treating preoperative UTI is unlikely to reduce rates of PJI, which may reduce the need for preoperative UTI screening in asymptomatic patients. This shift would ideally lessen the economic burden of UTI screening, limit the prescription of unnecessary antibiotics, reduce the incidence of lost operating room time, lessen patients’ frustrations, and most importantly result in quicker restored function in these patients with chronic shoulder impairment. In 2012, Bailin et al. 20 implemented an intervention in which surgeons decreased their UTI screening and treatment practices prior to THA/TKA and found no increase in the rates of SSI or PJI—corroborating our stance.
While we did not find preoperative UTI predictive of two-year PJI, we did find it to be associated with higher rates of certain medical complications within the 90-day postoperative period. With respect to anemia, both blood loss and iron deficiency anemia were found to be significantly higher in the preoperative UTI cohort when compared to the non-UTI cohort. As such, it is likely that the increased finding of postoperative anemia in the UTI group is attributable to these already increased preoperative rates. With regard to PE and DVT, the UTI cohort demonstrated higher rates of congestive heart failure, arrhythmias, hypertension, and diabetes mellitus—all potential cardiovascular risk factors which, when combined with the vascular trauma associated with major surgery, may have the potential to incite an embolic event.21–23 Of note, the significance of DVT in the UTI group became negligible when the cohort was stratified into patients who underwent UTI treatment—suggesting that resolution of UTI may be beneficial in reducing the number of postoperative DVTs. Smeeth et al. 24 performed a case series on 7278 DVT patients and 3755 PE patients, which revealed a significantly increased risk in patients after the diagnosis of UTI was made. The risk then returned to baseline over the following months—further supporting the notion that one benefit to preoperative UTI screening is a reduction in postoperative DVT/PE risk. 24 Still, the reasonings behind our postoperative findings are undoubtedly multifactorial and future studies should be aimed at exploring these complications in further detail.
This retrospective study has several limitations. Patients were stratified into cohorts based on ICD and CPT coding from multiple providers and facilities. The validity of our findings is dependent on the accuracy and completeness of data entry, which may not be standardized across such a wide variety of sources, and thus may be a potential source of misclassification bias. Although urine culture results would more accurately determine patients with a UTI, the Pearldiver database does not include the results for tests performed. Thus, we are limited to the coding of UTIs based on ICD 9/10 diagnosis codes. Additionally, for those with PJI, we cannot discern what species of bacteria grew (Gram+ or Gram−) and whether the species were different in the treated versus untreated groups. For the antibiotic cohort, although we observed the utilization of antibiotics following UTI and before TSA, we cannot determine from the database the exact indication for the antibiotic. Thus, this is a limitation in the treated cohort. Additionally, the database cannot discern what antibiotics were being used perioperative as prophylaxis for the surgery as it lacks perioperative medication data. Another limitation to the use of these billing codes is the less specific information. The CPT code 23472 was used to identify those that underwent TSA but cannot discern between reverse and anatomic TSA. In addition, using routinely collected data that was not created to answer a specific research question may limit the reliability of our results. Conversely, one strength in utilizing routinely collected data is in the large size of our research cohort. In total, 75,480 patients across the U.S. were included in our final analysis, which increases the diversity of our study population and improves the generalizability of our findings. Although our analysis was well powered, we could not look at longer-term outcomes beyond two years to maintain the power for the treated versus untreated analysis. Future works with larger sample sizes can observe longer-term outcomes in this population.
Conclusion
The results of this study indicate that the presence of preoperative UTI and its treatment prior to TSA did not alter the rates of revision surgery, PJI, or the need for MUA at the two-year mark following the index arthroplasty surgery. Preoperative UTI was associated with an increased risk of cardiopulmonary complications within 90 days of surgery. These findings may suggest that in the case of UTI, adopting a less conservative approach to surgical planning may lead to a reduction in associated costs and a more rapid return to function in these patients in need of shoulder arthroplasty, but further studies are needed to confirm this.
Footnotes
Authors’ Note
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article