
Abstract
Aims
We aimed to evaluate the correlation between preoperative and postoperative resilience scores and postoperative outcomes at minimum 2-year follow-up after arthroscopic rotator cuff repair.
Methods
We prospectively enrolled 98 patients who underwent rotator cuff repair. We assessed resilience using the Brief Resilience Scale. Postoperatively, we obtained patient-reported outcomes measures including American Society of Shoulder and Elbow Surgeons scores, Single Assessment Numeric Evaluation, and Patient-Reported Outcome Measurement Information System Global Health-10 at minimum 2-year follow-up. We used Spearman correlation coefficients (r) to assess the relationship between variables.
Results
Ninety-one of 98 patients (93%) provided follow-up at an average of 32 months. Preoperative Brief Resilience Scale did not show a statistically significant correlation with American Society of Shoulder and Elbow Surgeons (r = 0.156; p = 0.142). However, preoperative Brief Resilience Scale showed statistically significant correlations with Patient-Reported Outcome Measurement Information System Global Health-10 (r = 0.290; p = 0.005) and Single Assessment Numeric Evaluation (r = 0.259; p = 0.014). Postoperative Brief Resilience Scale showed statistically significant correlations with American Society of Shoulder and Elbow Surgeons (r = 0.291; p = 0.005), Single Assessment Numeric Evaluation (r = 0.384; p < 0.001) and Patient-Reported Outcome Measurement Information System Global Health-10 (r = 0.515; p < 0.001).
Discussion
Resilience may be a valuable predictor of patients at risk of having suboptimal outcomes after rotator cuff repair and a target to improve surgical outcomes through non-surgical means.
Introduction
Historically, the orthopedic community identified the size of the cuff tear or the surgical technique used for repair as critical factors in patient outcomes after rotator cuff repair (RCR) surgery.1–3 More recently, researchers have identified numerous factors that may play a role in patient outcomes after RCR. Rather than using a purely biological framework to study patient outcomes after surgery, many authors have advocated for the adoption of the biopsychosocial model which recognizes “the impact of psychological and social factors on the development and outcomes of illness and disease.” 4
Numerous psychosocial factors may play a role in the outcomes after orthopedic surgery, and more specifically, RCR.4,5 While the link between states of emotional distress (e.g., anxiety and depression) and surgical outcomes has been repeatedly established,6–8 researchers have also begun to look for correlations between positive psychosocial factors and improved surgical outcomes. 9 Resilience, defined as the “ability to bounce back or recover from stress,” may play a critical role in determining patient outcomes after RCR. 10
In this study, we aimed to evaluate the correlation between preoperative resilience scores and postoperative patient-reported outcome measures (PROMs) after arthroscopic RCR. We also sought to evaluate the correlation between concurrent resilience and PROMs measured at a minimum 2-year follow-up. We hypothesized that (1) preoperative resilience and (2) concurrent resilience would correlate with patient-reported outcome measures at minimum 2-year follow-up after arthroscopic RCR.
Materials and methods
Study design
This study was a single-center prospective cohort study of patients who underwent arthroscopic RCR by one of three fellowship-trained sports medicine surgeons between September 2017 and October 2019. We prospectively enrolled 104 consecutive adult patients who were diagnosed with rotator cuff tear using magnetic resonance imaging and scheduled for arthroscopic repair. We later excluded six patients: four patients were found not to have rotator cuff tears and underwent isolated subacromial decompression, one had a massive tear and underwent superior capsular reconstruction, and one canceled her surgery for an unknown reason. Therefore, we ultimately included 98 patients for follow-up at a minimum of 2 years from surgery. Ninety of 98 patients provided full responses, and one patient provided a partial response to the questionnaires, for a follow-up rate of 93%. Short-term follow-up of this patient cohort has previously been published, but the data presented in the current study has not been published.
A clinical research coordinator (CRC) obtained informed consent for patient enrollment in accordance with standards set by the Institutional Review Board. Preoperative questionnaires, including Brief Resilience Scale (BRS), American Society of Shoulder and Elbow Surgeons (ASES) shoulder score, Single Assessment Numeric Evaluation (SANE), and Patient-Reported Outcome Measurement Information System Global Health-10 (PROMIS-10) were then obtained preoperatively from patients by the CRC and later populated into REDCap (Vanderbilt University, Nashville, TN, USA). Minimum 2-year follow-up was obtained by contacting patients via telephone to ascertain their preferred email address for questionnaire administration (BRS, ASES, SANE, and PROMIS-10). If patients did not use email or strongly preferred to complete questionnaires in a different method, we used postal mail or administered questionnaires by telephone. Eighty-two patients completed the questionnaires in a written format (76 by email (83.5%) and 6 by postal mail (6.5%)) while 9 completed the questionnaires over the telephone (10%). All of the questionnaires have been validated in written format. While other PROMs have been validated when administered via telephone, we are not aware of any literature validating the specific measures we used.
Questionnaires
We chose BRS as the resilience outcome measure because previous studies have demonstrated its validity and consistency. 10 The BRS is a 6-question Likert scale with 5 anchors per question, such that scores range between 6 and 30 (Figure 1). Patients with higher scores are considered more resilient. To evaluate shoulder pain and function, we used ASES and SANE scores. To evaluate general physical and mental health, we used PROMIS-10 because of its manageable length and strong correlation with legacy measures of physical and mental health.11,12
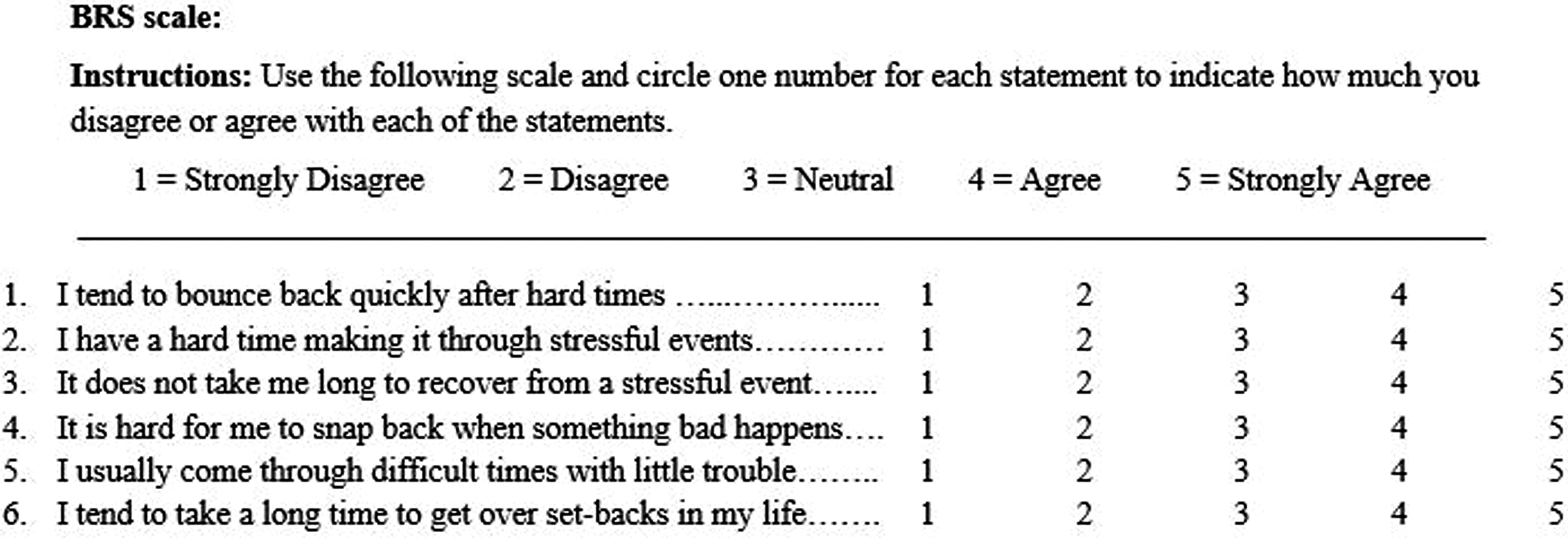
Depiction of the questions included in the Brief Resilience Scale.
Demographic information
As part of a previous study on this patient cohort, we recorded preoperative demographic information on each patient including age, sex, body mass index, smoking status, and a dichotomized history of diabetes and mental health diagnoses (including anxiety, depression, personality disorders, cognitive impairments, or psychotic disorders) using the electronic medical record (Epic Systems Corporation, Verona, WI). We also recorded the size of the rotator cuff tear based on the surgeon's operative report classification, according to the method described by Cofield (small, medium, large, or massive). 13
Statistical analyses
We described sample characteristics using descriptive statistics. We used frequencies and percentages to describe categorical variables. We used the mean and standard deviations (or medians and ranges when appropriate) to describe continuous variables. We used a chi-square test to assess the association between categorical variables. We used a Wilcoxon rank-sum test to test for differences in scores between 2 groups and used a Kruskal-Wallis test to test for differences between three or more groups. We used a Spearman correlation coefficient (r) to assess the relationship between two continuous or ordinal variables. Spearman correlation coefficients range from −1 to 1, with 0 representing no correlation, and −1 and 1 representing perfect negative and positive correlations, respectively. The closer the correlation is to either −1 or 1, the stronger the correlation. Statistical significance was set to p-value < 0.05. A trained statistician performed all statistical analysis in SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic information
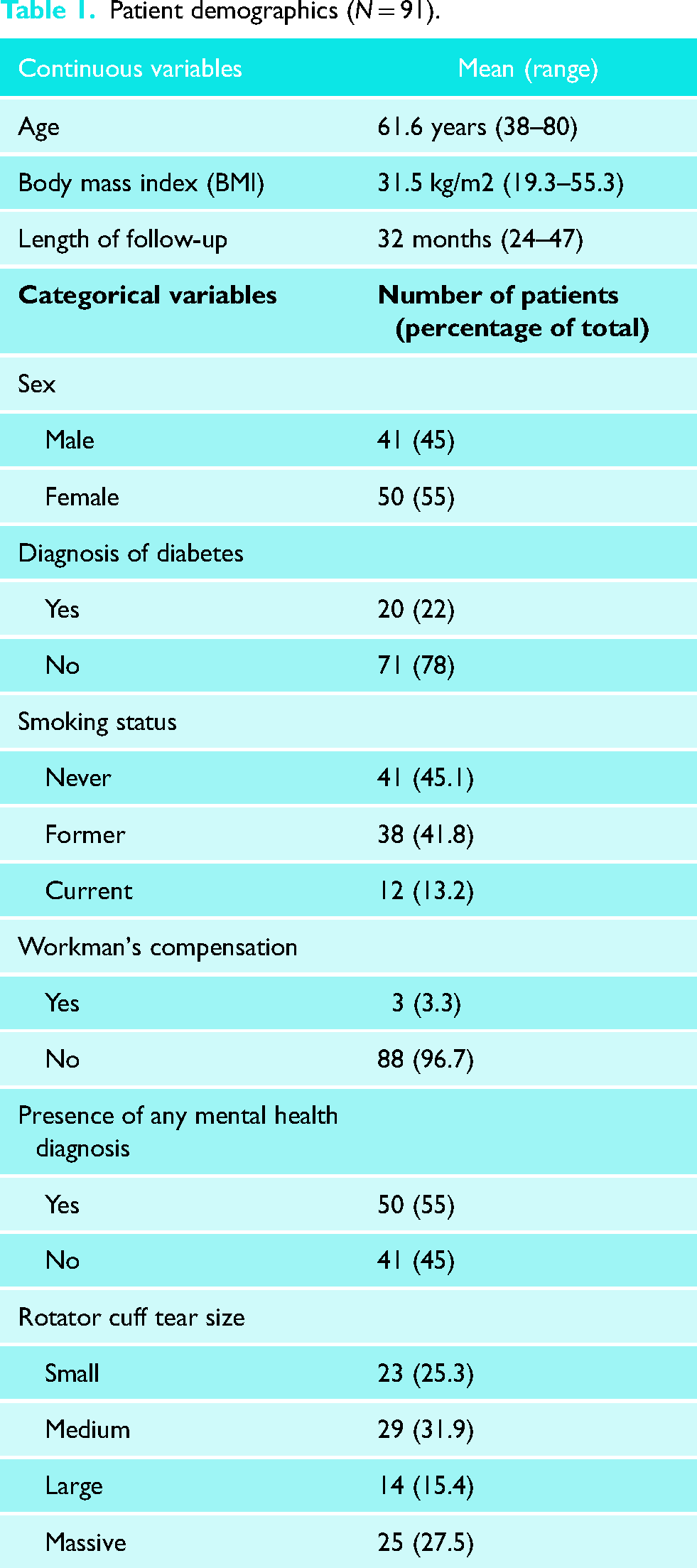
Table 1 depicts patient demographic characteristics. The average length of follow-up was 32 months (range of 24–47 months). Table 2 depicts the mean preoperative and postoperative BRS and PROM scores.
Patient demographics (N = 91).
Preoperative and postoperative scores.
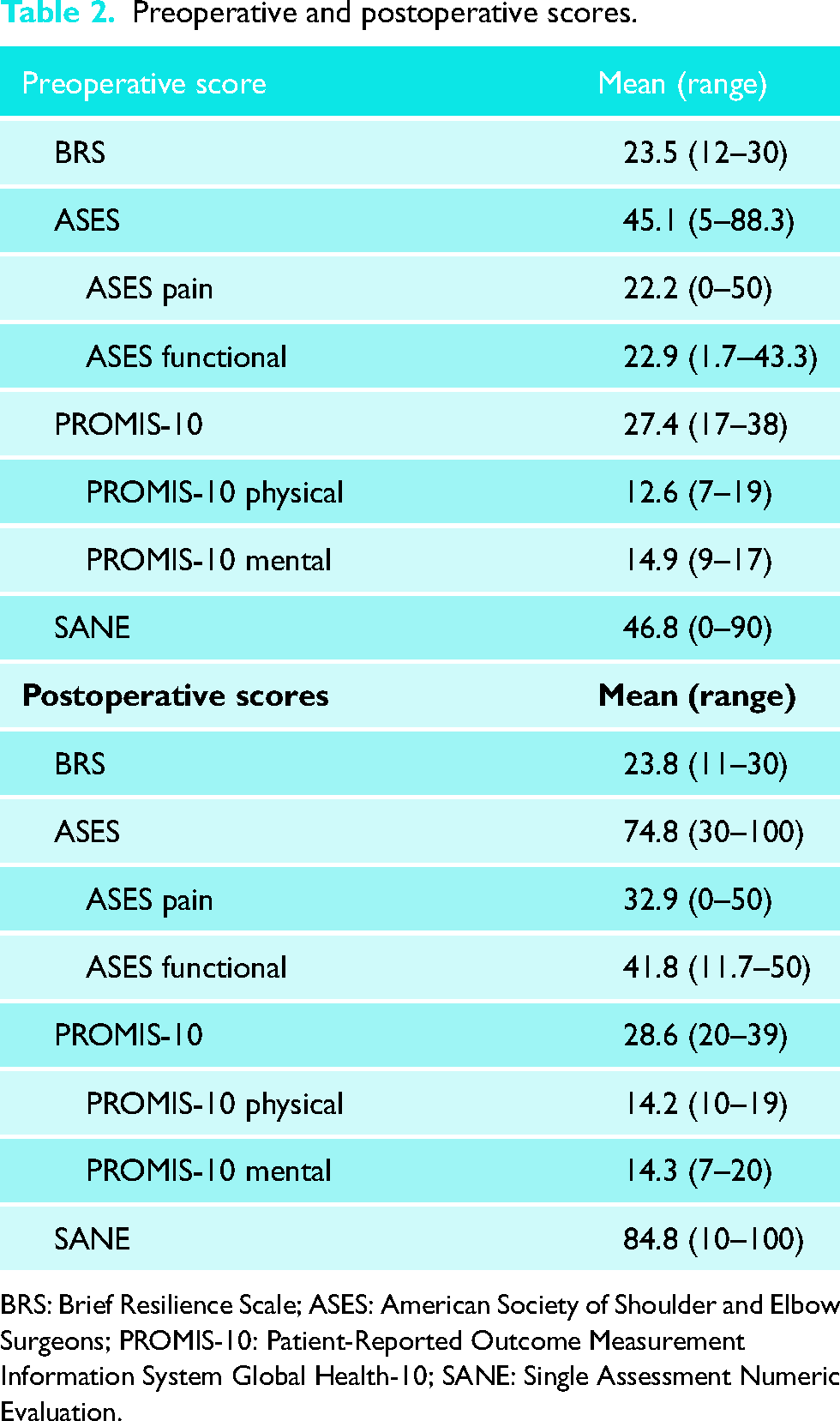
BRS: Brief Resilience Scale; ASES: American Society of Shoulder and Elbow Surgeons; PROMIS-10: Patient-Reported Outcome Measurement Information System Global Health-10; SANE: Single Assessment Numeric Evaluation.
Correlation between preoperative BRS scores and postoperative PROMs
Preoperative BRS did not show a statistically significant correlation with ASES (r = 0.156; p = 0.142). However, there was a statistically significant correlation with the ASES functional component (r = 0.223; p = 0.035). Preoperative BRS also showed statistically significant correlations with PROMIS-10 (r = 0.290; p = 0.005) and SANE (r = 0.259; p = 0.014; Table 3).
Correlation between preoperative BRS and outcomes at final follow-up.
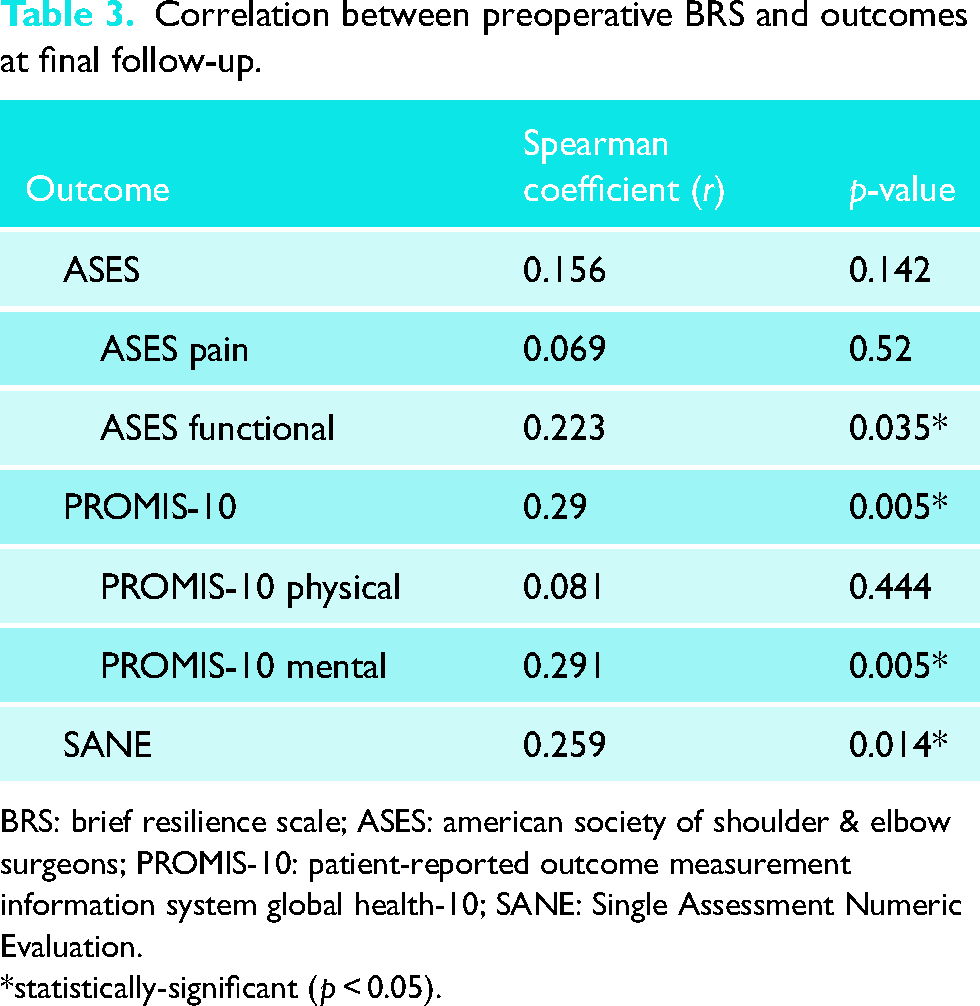
BRS: brief resilience scale; ASES: american society of shoulder & elbow surgeons; PROMIS-10: patient-reported outcome measurement information system global health-10; SANE: Single Assessment Numeric Evaluation.
*statistically-significant (p < 0.05).
Correlation between concurrent BRS scores and PROMs
When obtained at minimum 2-year follow-up, BRS more strongly correlated with ASES, SANE, and PROMIS-10. In fact, 2-year BRS showed statistically significant correlations with ASES (r = 0.291; p = 0.005), SANE (r = 0.384; p < 0.001), and PROMIS-10 (r = 0.515; p < 0.001; Table 4).
Correlation between postoperative BRS and outcomes at final follow-up.
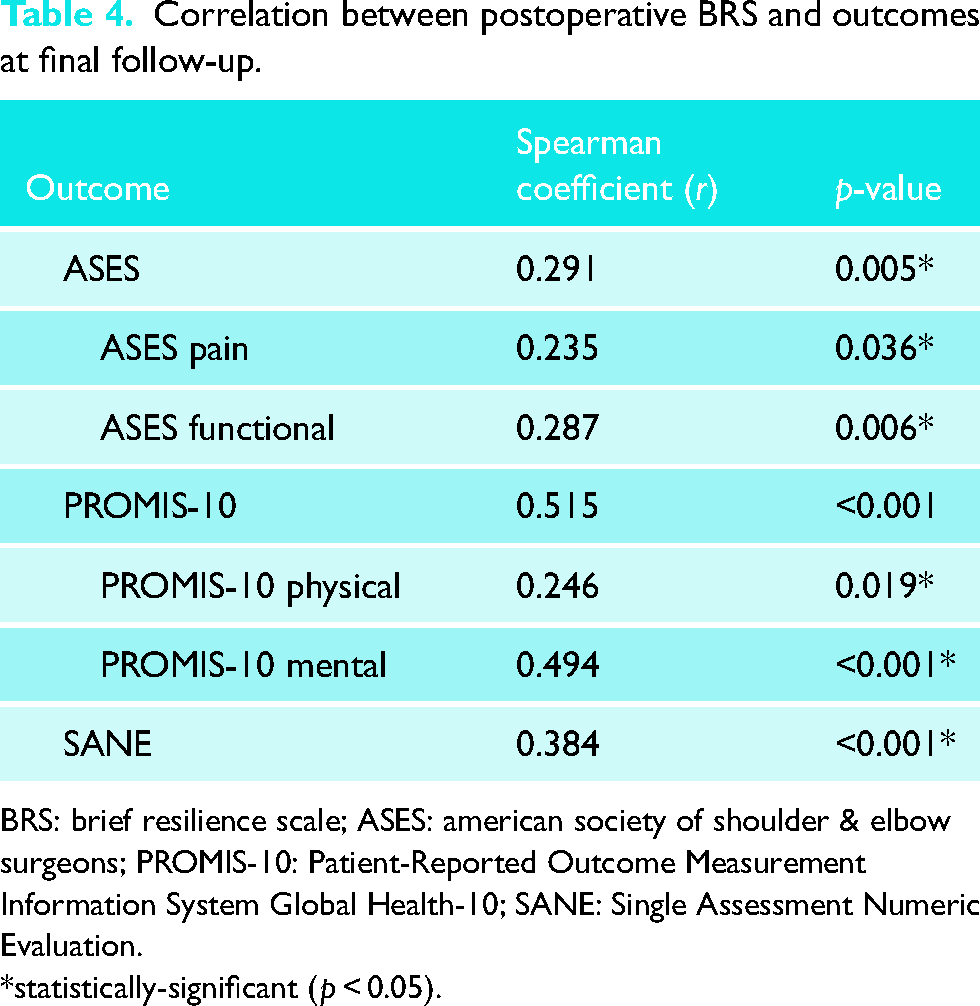
BRS: brief resilience scale; ASES: american society of shoulder & elbow surgeons; PROMIS-10: Patient-Reported Outcome Measurement Information System Global Health-10; SANE: Single Assessment Numeric Evaluation.
*statistically-significant (p < 0.05).
Discussion
In this study, we sought to study the relationship between patient resilience and outcomes after arthroscopic RCR. We found that preoperative resilience, as measured by the BRS, correlates with several postoperative PROMs, including PROMIS-10 and SANE. When measured concurrently at minimum 2-year follow-up, we found that BRS correlates with ASES and SANE and more strongly correlates with PROMIS-10.
We have shown that preoperative resilience has a correlation with PROMIS-10 and SANE after RCR. Other authors have published similar findings in a variety of orthopedic populations. In a prospective cohort of patients who underwent total knee arthroplasty, resilience was found to predict postoperative knee function and general physical health, but not mental health, at 3-month follow-up. 14 Recall of pre-fracture psychological resilience has been shown to correlate with physical function in older adults after hip fracture surgery. 15 Drayer et al. 16 found patients with high preoperative resilience had significantly higher postoperative outcomes scores in domains of knee pain and function, and mental health following arthroscopic knee surgery.
Not all studies show a correlation between preoperative resilience and postoperative outcomes. In patients who underwent RCR, resilience did not correlate with shoulder pain and function at 3- and 6-month follow-up. 17 Similarly, resilience did not correlate with 3 or 6-month Boston Carpal Tunnel Questionnaire scores after carpal tunnel release. 18 In contrast to the study by Drayer et al., Chavez et al. 19 found that in patients who underwent arthroscopic knee surgery, resilience did not correlate with postoperative pain and functional scores at 3 and 6-months. Similarly, we found that preoperative resilience did not correlate with the overall ASES score.
When measured concurrently, we found that resilience generally showed a stronger correlation with postoperative outcomes. Other authors have reported similar findings. Resilience was shown to correlate with shoulder functional scores in patients 2 years after total shoulder arthroplasty. 20 In a recent study, resilience, assessed using the Life Orientation Test, showed a correlation with ASES scores four years after RCR. 21 Low resilience scores were shown to be independently associated with greater functional disability in a cohort of patients with neck and low back pain. 22
In a prospective cohort of patients who underwent total knee arthroplasty, there was no significant correlation between preoperative resilience and one-year postoperative knee functional scores. However, there was a significant correlation between concurrent resilience and postoperative scores. 23 Similarly, in patients who underwent arthroscopic RCR, concurrent resilience was found to more strongly correlate with physical and mental health when compared to preoperative resilience. 17 While resilience may play a role in predicting patient recovery after surgery, it is also possible that resilience is not a static personality trait, but dynamic, and subject to the influence of a patient's recent experiences.
While identification of resilience attributes may be useful to help physicians stratify those patients at risk of poor surgical outcomes, the ultimate goal when illuminating a correlation between psychosocial factors and postoperative outcomes is to improve outcomes by modifying the factor of interest. This begs the question: can we foster resilience in our patients? The answer is unknown. Thought leaders in orthopedics have editorialized about whether it is possible to increase one's grit (a similar trait to resilience). 24 They encourage deliberate effort, perseverance, and development of specific goals. Similarly, other authors encourage mindfulness and fostering one's passions.25,26 However, these encouragements are all in the context of growing resilience traits and preventing burnout in healthcare workers. While some psychotherapists have outlined ways to foster resilience traits in patients, we still need significant research to show whether orthopedic surgeons can have a meaningful impact on our patients’ positive cognitive processes and thereby improve surgical outcomes.27,28 Cognitive behavioral therapy has been shown as an effective modality in improving patient resilience and reducing anxiety and depression. 29 It remains to be seen whether such interventions could translate to improved surgical outcomes, but this is an area of potential future study.
Limitations
Our study has a number of limitations. The BRS only focuses on one aspect of resilience—an individual's ability to recover from stressful events. Social or psychological support systems may also contribute to a patient's resilience. In addition, we did not measure all of the myriad psychosocial factors that may affect surgical recovery. Trying to account for all such factors would be untenable, so we elected to pursue a focused research scope, but doing so could fail to account for the effect of other important psychosocial factors. Finally, 10% of the follow-up questionnaires were obtained via telephone administration, a method that has not been formally evaluated for the specific instruments we used.
Conclusions
In conclusion, our study adds to the growing body of literature that psychosocial factors, such as resilience, play a role in determining patients’ recovery and ultimate outcome after surgery. We hope that this information may eventually be used to improve surgical outcomes via non-surgical means.
Footnotes
Acknowledgments
The authors would like to thank Dr. Robert Reeve and Dr. William Hamilton for allowing their patients to be enrolled in the study and for performing surgery. We would also like to thank Hope Gonzales, Spencer Rose, and Elizabeth Campbell for their consistent efforts as clinical research coordinators.
Contributorship
CDW, BNR, KAPH, and BDW conceived and designed the study. CDW and BDW did the initial literature review and wrote the protocol for review by the institutional review board, with oversight and input from BNR. Enrollment in the study was performed by rch coordinators. CDW and LJV obtained follow-up questionnaires. KAPH performed the data analysis. CDW, LJV, BDW, KAPH, and BNR all contributed to the manuscript writing and review. CDW performed the manuscript minor revisions.
Guarantor
Charlie Wilson.
Ethical approval
Ethical approval was provided by Baylor Scott & White Research IRB (Project ID: 020-329, Reference Number: 350477).
Informed consent
Written and signed informed consent was obtained for each of the patients enrolled in this study. Written informed consent was obtained for their anonymized information to be published in this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.