
Abstract
Introduction
Terrible triad injuries (TTIs) of the elbow have traditionally been reported to have poor outcomes, hence requiring surgical stabilisation. We identified and reviewed patients with TTIs treated non-operatively within our department.
Methods
We retrospectively reviewed patients with TTI treated non-operatively with standardised elbow-instability rehabilitation from 2010 to 2020. We used Mason and Morrey classifications for radial head and coronoid fractures, respectively. Non-operative indications included a congruent joint on CT, significant co-morbidities pre-disposing to high-risk surgery and/or patient preference. Outcomes included Oxford Elbow Score (OES), ROM and complications.
Results
Nineteen patients were included (mean age 49; 37% female). At an average of 6 years (range 2–11 years) post-treatment, mean OES was 46 ± 7. At last clinic review, mean 6 months (2–15), average ROM was 131 ± 11° flexion, 8 ± 10° extension, 85 ± 12° supination and 85 ± 13° pronation. One patient required arthrolysis and another had an incongruent ulnohumeral joint which developed clicking with a functional ROM.
Conclusion
Our report suggests non-operatively managed and appropriately rehabilitated TTI injuries can achieve good function and ROM. We recommend conservative management as a viable option in cases with joint congruency and no mechanical block in patients with significant co-morbidities or those refusing surgery but patients must be assessed on a case-by-case basis.
Introduction
Dislocation of the elbow with fracture of the radial head (RH) and coronoid was first described as a terrible triad by Hotchkiss in 1996 due to historically poor outcomes. 1 Traditionally, these injuries have necessitated surgical management to restore stability and early motion, with options including fixation or replacement of the RH, lateral collateral ligament (LCL) repair and fixation of the coronoid fragment if affecting stability. 2 Surgical complications are recognised, including loss of movement, stiffness, heterotrophic ossification, nerve injury and reoperation. 3
More recently, conservative management of a terrible triad injury (TTI) has become more of a consideration in certain circumstances. Matthew et al. 4 described four essential criteria that must be met when considering non-surgical treatment: post-reduction ulnohumeral and radiocapitellar joint congruency, a sufficiently stable elbow to allow extension up to 30°, a small undisplaced or minimally displaced RH or neck fracture which does not cause mechanical block to elbow movement and a small coronoid tip fracture. Utilising these indications, Chan et al. achieved good elbow function at a mean of 36 months follow-up in 12 patients with type 1 and 2 RH and coronoid fractures treated non-operatively. 5
Standard practice has been to treat TTI with surgical stabilisation. As a result, the published literature evaluating non-operative management of these fracture dislocations has been limited by small cohort numbers and short follow-up times. A retrospective review was undertaken to evaluate outcomes of TTI managed non-operatively within our department.
Methods
We performed a retrospective single-centre review of 19 patients with TTI managed non-operatively between 2010 and 2020. Patients were identified from the hospital database and each patient was contacted by telephone to consent for participation in the study. Both patients’ notes and imaging were reviewed using the online hospital records systems (Lorenzo and XERO viewer, respectively). Inclusion relied on radiological evidence of an elbow dislocation with both RH and coronoid fractures. The dislocations were reduced in the emergency department with confirmation of the reduction on repeat radiographs in an above-elbow plaster of paris backslab or high collar and cuff sling applied to maintain position, provide pain relief, and allow rest. Post-reduction computed tomography (CT) was performed on every patient to assess both fracture fragment configuration and joint congruency. The decision for conservative management was based on certain indications outlined by Mathew et al., 4 specifically joint congruency on post-reduction CT scan and movement without mechanical block but consideration was also given to those with significant co-morbidities pre-disposing to high-risk surgery or patients’ preference for treatment without surgery. Exclusion criteria included an open injury, previous fracture or dislocation of the ipsilateral elbow or pre-existing non-functional limb.
All patients required close monitoring with regular follow-up, starting with initial review in a planned specialist shoulder and elbow fracture clinic within 1 week following initial management in the emergency department. On review in clinic, range of motion and mechanical block assessment were performed and radiographs were repeated to ensure the joint and fractures remained adequately reduced in a collar and cuff. Each patient received standardised elbow-instability rehabilitation which included removal of backslab if present at the first fracture clinic visit, high collar and cuff with physiotherapy to allow active movement from 90° to full flexion At 4 weeks ROM was increased from 60° to full flexion and then 30° to full flexion at 6 weeks, with radiographic and clinical evaluation performed at each review to ensure joint remained congruent with no evidence of instability. At 8 weeks following trauma, full ROM was allowed. Following this physiotherapy regime, stability and function were then assessed on further fracture clinic follow-up appointments.
Initial radiographs and CT were used to grade RH fractures using the Mason classification 6 and coronoid fractures according to the Morrey classification. 7 Our primary outcome measure involved assessment with the Oxford Elbow Score (OES). Secondary outcome measures included ROM and any clinical complications.
Results
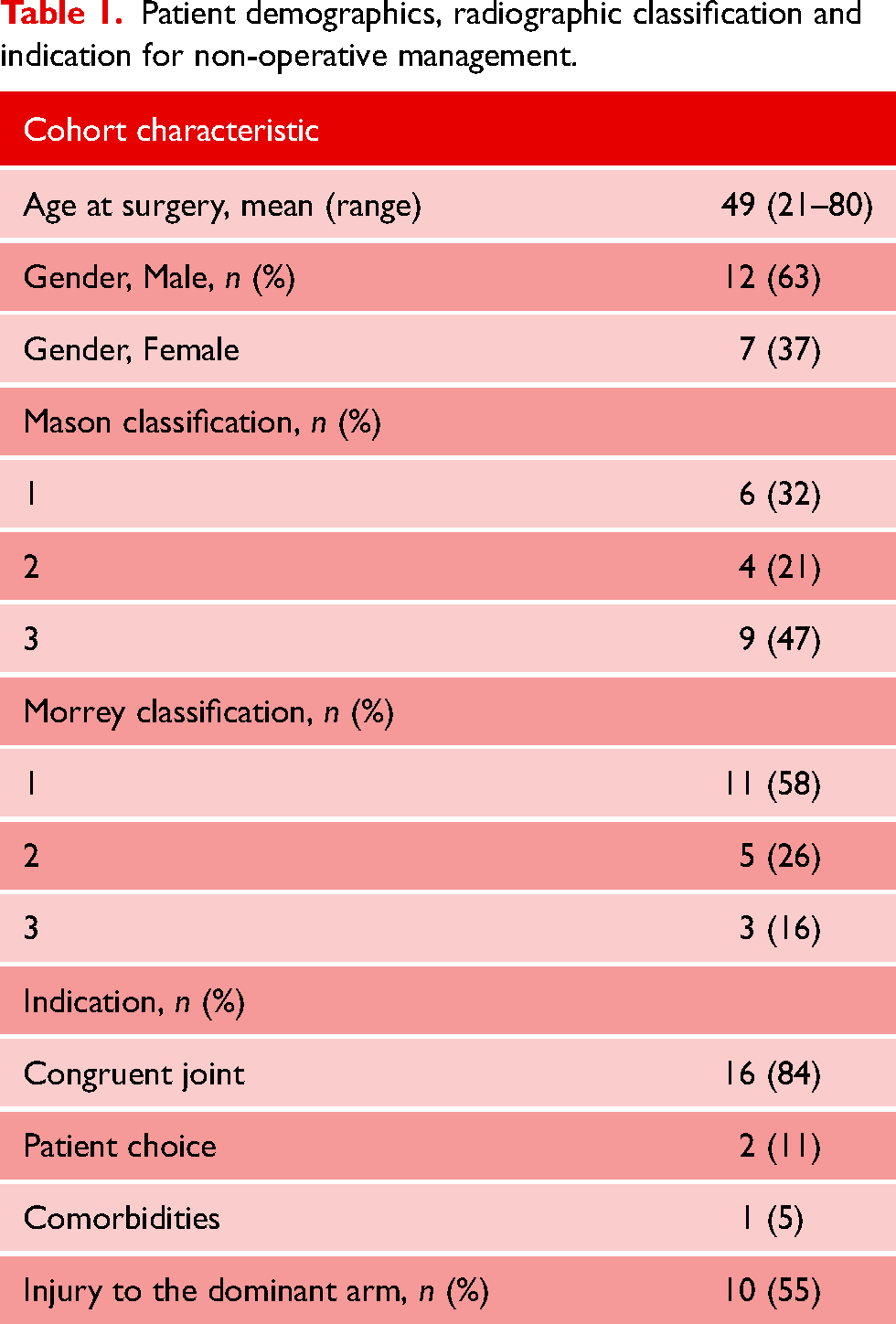
Nineteen patients who had a conservatively TTI, one patient, however, passed away prior to final follow-up from an unrelated cause. The mean age at the time of injury was 49 years and, of the cohort, seven (37%) were female. Patient demographics, radiographic classification and indication for non-operative management are summarised in Table 1.
Patient demographics, radiographic classification and indication for non-operative management.
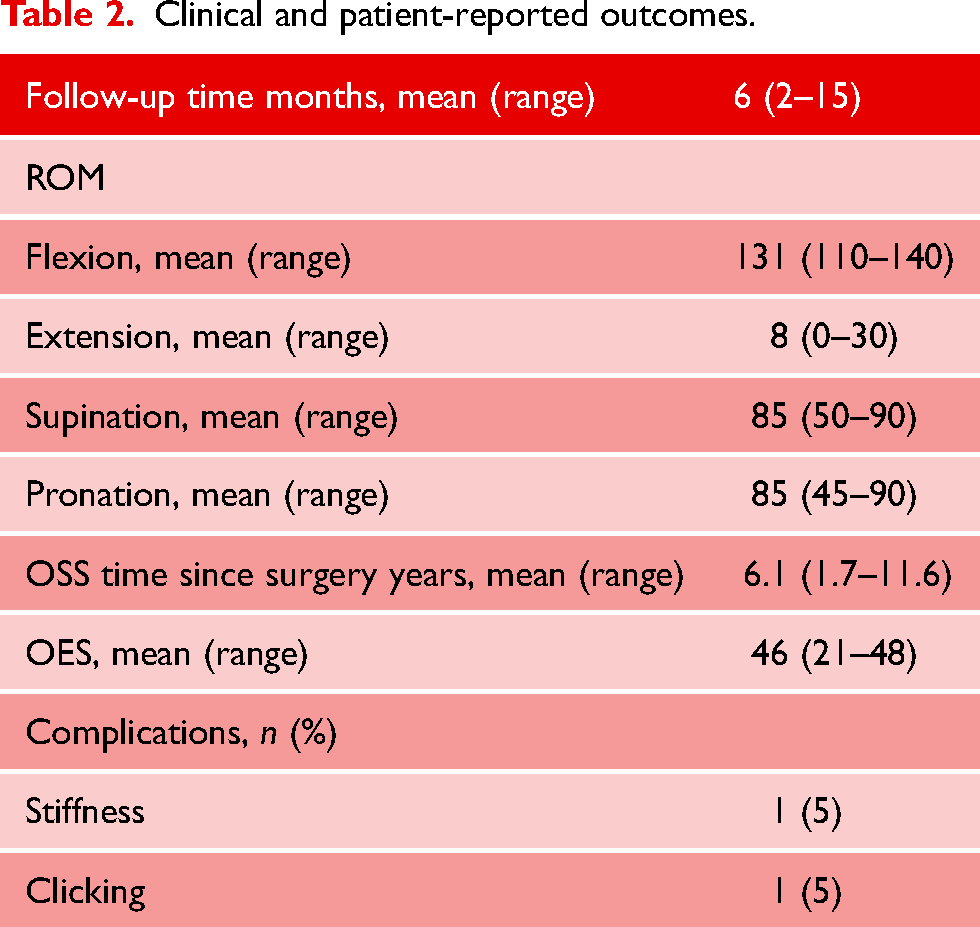
Clinical and patient-reported outcomes are summarised in Table 2. At a mean follow-up of 6 years (range 2–11 years), the mean OES of our cohort was 46 ± 7. This follow-up time was for collection of outcome scores via telephone, at time of collection further surgery and change in elbow function were asked. None of the patients felt the need for further face-to-face review following OES collection. The average clinical follow-up time was 6 months (range 2–15) months. On last clinical follow-up the mean ROM included 131 ± 11° flexion, 8 ± 10° extension, 85 ± 12° supination and 85 ± 13° pronation. Patients achieved a flexion–extension arc of 123° (90–140) and a supination–pronation arc of 170° (105–180). Lower OES were noted in the TTIs with both type 3 Mason RH and Morrey coronoid fractures achieving a mean OES of 34.5, compared with the average 45 OES score. Mean flexion–extension ROM in this group however was 10–135° with a mean supination–pronation arc of 145°. In all subgroups, numbers were too small to determine statistical significance.
Clinical and patient-reported outcomes.
There were no cases of conversion to surgical fixation in our non-operative cohort. During the study period, the predominant treatment of TTI was surgical fixation which was performed in 51 cases. Within the non-operative cohort, there were two complications. A 61-year-old female (patient 6) fell from standing and sustained a coronoid tip fracture and a displaced radial neck fracture as part of her TTI. After reduction of the ulnohumeral joint dislocation, the RH remained displaced posteriorly but despite gross incongruence of the radiocapitellar joint, the patient refused surgery. She developed painless clicking within the elbow joint but, with a focused rehabilitation pathway, went on to achieve a full ROM and an OES of 48 and required no other intervention. The other complication involved a 45-year-old female (patient 12) who sustained a TTI with Mason type 3 RH and Morrey type 3 coronoid fractures after being hit by a bus. Initially managed non-operatively due to patient choice, the joint was stiff with their flexion–extension arc limited from 60 to 130° at 8 months follow-up and functional deficit. The patient underwent arthrolysis, successfully improving flexion from 20–140° and supination–pronation arc to 110°. We had no other incidence of non- or delayed union, infections, nerve injury or instability.
Discussion
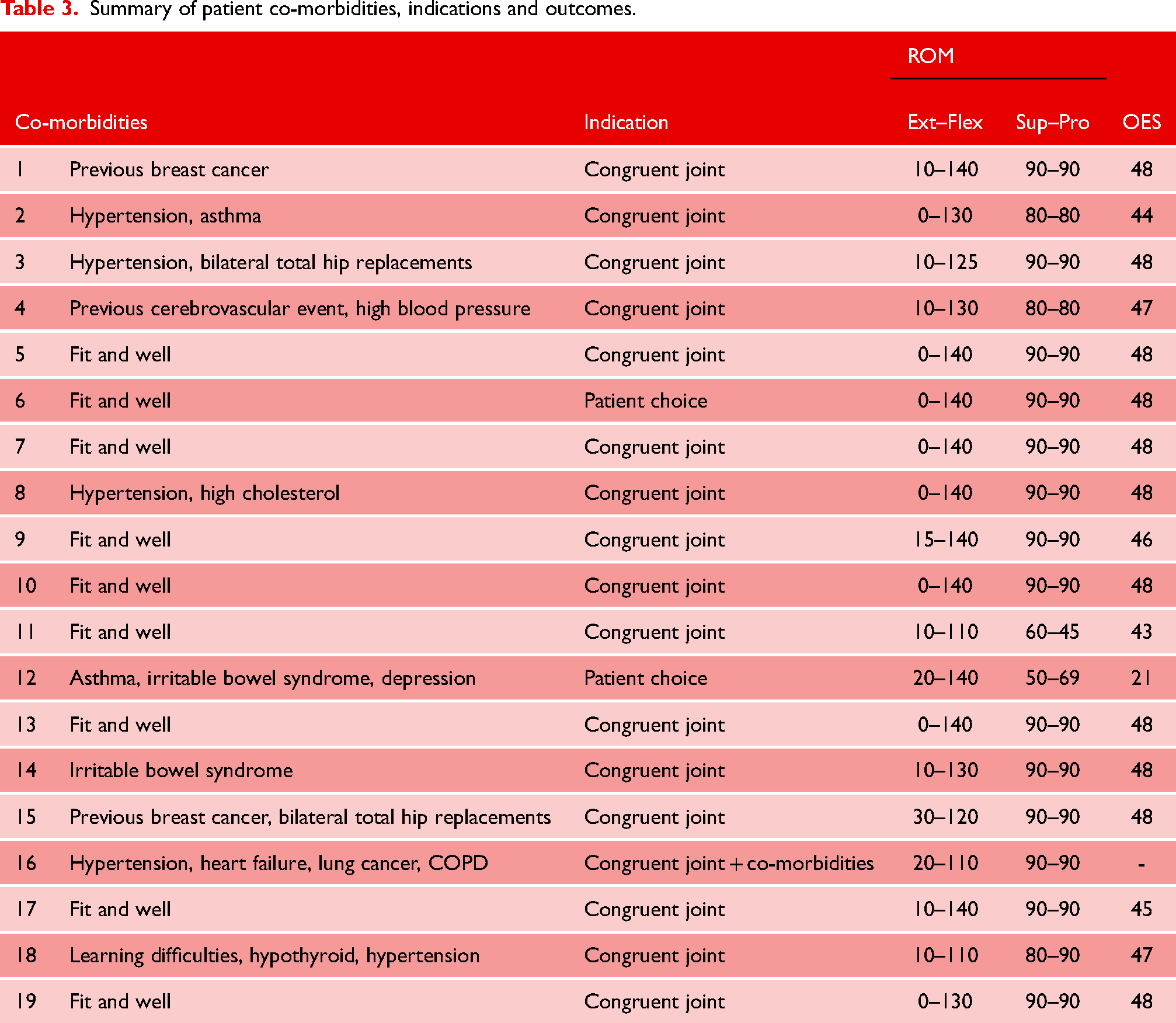
The inherent instability associated with TTI has meant surgical intervention is often the preferred method of treatment in order to allow safe and early movement. 1 Due to this, there is a paucity of data published on both indications and outcomes for non-operative management of these fracture-dislocations (Table 3).
Summary of patient co-morbidities, indications and outcomes.
Chan et al. 5 advocated considering conservative management in elbows with joint congruency, no mechanical block, a stable ROM and Morrey type 1 or 2 coronoid fractures. They achieved good function and restored stable ROM but only reviewed 12 patients and included no type 3 RH or coronoid fractures. Within our 19-patient cohort, we demonstrated greater variety in complexity and severity of injury patterns, including nine RH Mason type 3, three coronoid Morrey type 3 and two having both type 3 RH and coronoid fractures, all achieving good function and ROM at long-term follow-up. This series is more representative of the full spectrum of TTI and hence may provide a greater understanding of this pathology.
Biomechanical studies have shown that the minimum range of flexion required for activities of daily living is from 30° to 130°, with 50° each for pronation and supination. 8 From the available literature, surgical treatment for TT achieves mean post-operative ROM of 130 ± 7° flexion, 15 ± 6° extension, 66 ± 10° supination and 69 ± 11° pronation.9–16 Sixteen of our patients treated without surgery achieved a functional ROM, adequate for their activities of daily living (ADL). Our outcomes demonstrate managing these injuries non-operatively in selective cases results not only in similar flexion–extension arcs to operative management but improved prono-supination, while additionally negating the risks of an anaesthetic and complications directly related to surgery.
The stabilisers of the elbow have been well described with the ulnohumeral joint and collateral ligaments providing primary stability and the RH being one of the secondary restraints. 17 Closkey et al. 18 performed resection of the coronoid in a six-cadaver case series. When axial load was applied to the elbow, a deficit of greater than 50% of the coronoid process allowed posterior dislocation more readily. As described by Morrey, the coronoid is the most important articular stabiliser and provides stability regardless of the integrity of the other articular components. 17 In our cohort, the fact that all our coronoid fractures remained reduced and ulnohumeral joints were congruent, from initial reduction through to final follow-up, maybe a contributing factor in producing stability and good function, regardless of their Morrey grading, with non-operative management.
As part of the spectrum of posterolateral rotatory instability (PLRI), the ligamentous deficit and RH fracture in a TTI often renders the joint unstable and hence these structures, as a minimum, usually need reconstruction surgically. Chemama et al. found that even with operative management, a Mason type 3 RH fracture as part of a TTI was a negative prognostic factor resulting in reduction of range motion. 12 Our outcomes demonstrate 86% of patients with a Mason type 3 RH fracture and Morrey type 1 coronoid fracture achieved full prono-supination, a minimum extension–flexion range from 20–110° and an average OES of 47 (43–48). This group included one of our two complications, where the RH remained displaced posteriorly after reduction of the ulnohumeral dislocation (Figure 1). After refusing surgery and undergoing rehabilitation, the ulnohumeral joint remained anatomically reduced providing stability and range with regards to flexion and extension but, despite a severely incongruent radiocapitellar joint, prono-supination was maintained with the only symptom being a painless clicking. In this case, forearm rotation was unaffected perhaps because of the RH being displaced out of the zone of the radiocapitellar axis of rotation as well as it remaining ununited and non-adherent to the radial neck.

Left elbow terrible triad treated non-operatively. (a) Pre-reduction lateral radiograph. (b) Lateral and anteroposterior post-reduction radiographs. (c) Computed tomography (CT) post-reduction sagittal image of ulnohumeral joint. (d) CT post-reduction axial image. (e) CT post-reduction sagittal image of radiocapitellar joint. (f) Post-injury anteroposterior and lateral radiographs at final follow-up.
While we had no Mason 3 RH fractures with Morrey 2 coronoid fractures, patients with a Mason 3 RH fracture combined with a Morrey 3 coronoid fracture demonstrated predictably reduced function despite maintaining a functional ROM. One patient from this group achieved 60–130° of flexion only, requiring arthrolysis to successfully improve range. In our cohort, a Mason type 3 RH fracture was not a predictive marker for poor function or reduced ROM with either flexion or forearm rotation, even without surgery.
There are limitations to this study, including that associated with the retrospective nature of the review. We have no pre-injury scores and no comparisons with the contralateral uninjured limb. Due to our selected cohort, our review may be affected by selection bias. Despite this being a small cohort study, it is still the largest of its kind in the available published literature and with the longest-term outcomes scores following treatment. Clinical follow-up time is short, average 6 months, however, telephone follow-up did not reveal any additional patient or surgeon concerns warranting further review. The outcomes of non-operative TT injuries seen in this study are similar to operative outcomes. Hence, we feel there is scope for a randomised controlled trial comparing the two treatment modalities for certain patients, depending on post-reduction congruency and clinical examination.
Conclusion
Non-operatively managed and appropriately rehabilitated TTI can achieve good or satisfactory function and ROM. We believe the maintenance of coronoid reduction and ulnohumeral joint congruence, regardless of Mason RH fracture grading, is key to achieving desirable outcomes in this group of patients. We recommend that conservative management is a viable option with a congruent joint and no mechanical block to forearm rotation in patients with significant co-morbidities or those refusing surgery. However, patients must be assessed individually with regular follow-up to ensure close monitoring and provided with advice making them aware of the possibility of ongoing instability and progressive arthritic change due to incongruency.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from all patients.
Contributorship
SB conceived the study and supervised the project. MB and AEB were involved in data collection and patient consent. MB, AEB, KG and SB were involved in literature research and data analysis. MB wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.