
Abstract
Objective
To perform a systematic review and meta-analysis to compare the results of the Latarjet procedure performed using screws (S) or suture-button for coracoid graft fixation.
Methods
A systematic search in Pubmed, EMBASE, and The Cochrane Library databases was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Cohort studies comparing outcomes in the Latarjet procedure with screw fixation versus the Latarjet procedure with suture-button fixation were included.
Results
Five studies with 877 patients were included. There was a significantly lower rate of recurrent instability in those with S fixation compared to the suture-button fixation (1.5% vs 5%, p = 0.001). There was a significantly higher rate of reoperations with S fixation compared to suture-button fixation (4.3% vs 0%, p = 0.001). There were no significant differences between the groups regarding total complications (S: 7.5% vs suture-button: 3.6% p = 0.12) graft fracture (S: 0.8% vs suture-button: 0.5% p = 0.62) and symptomatic hardware (S: 2.7% vs suture-button: 0% p = 0.12).
Conclusion
The Latarjet surgery was associated with favorable results and a low rate of complications regardless of the type of fixation used. Screw fixation was associated with a significantly lower rate of recurrences, but greater reoperations due to irritation or pain after surgery.
Level of evidence
Systematic review and meta-analysis, level III.
Introduction
The Latarjet surgery, already described 70 years ago, has proven to be an effective procedure for the treatment of recurrent glenohumeral instability. 1 This technique, performed both openly and arthroscopically, has generally been reported to have good outcomes, with high rates of patient satisfaction, low rates of recurrent instability, and high rates of return to preinjury sports performance levels.2,3 However, this procedure is not exempt from complications, which have been reported in up to 15%–30% of the cases.4,5 One of the most frequent complications of this surgery, ranging between 6.5% and 46%, is related to the screws used to fix the graft. 6 Screw-related problems can present themselves in different ways. First, intra-articular screws can cause pain and accelerated wear of the humeral head cartilage with the consequent risk of early osteoarthritis. Second, screw pullout or loosening can lead to the inability to achieve a rigid stable initial fixation of the coracoid graft causing graft nonunion, fragmentation, or resorption. Thirdly, brachial plexus injury might occur as a result of the proximity of drilling lines of action and screw insertion and, if screws protrude too medially on the posterior side, the suprascapular nerve might also be at risk for injury.4,5,7 To avoid the complications mentioned above, some authors have proposed the use of suture-buttons (SBs) for graft fixation. 8 These devices are composed of strong sutures interwoven between 2 metal buttons that are tensioned through opposing bony cortices. This allows for compression through the suture and across the metal buttons. 9
Recent biomechanical studies have compared different systems of screws (S) and SB for fixation of the coracoid graft during the Latarjet procedure. The results have not been consistent.7,9–12 Some authors have found that the S and SB fixation techniques exhibited comparable biomechanical strength for coracoid bone block fixation.7,9,10 However, others have found that the cortical SB fixation did not withstand direct loads to the graft as much as traditional screw fixation and this could compromise the initial stability of the graft, causing graft migration and undesired early complications.11,12
Boileau et al. 8 were the first to publish a series of 76 patients treated with the arthroscopic Latarjet technique using SB for graft fixation. The authors reported 91% graft consolidation and 1.5% recurrences at 14-month follow-up on average. However, Metais et al. 6 described the first comparative results of coracoid fixation with S vs SB. Since then, different clinical studies have compared the results of Latarjet surgery using S vs SB as a method of fixation.13–16 The purpose of the following study was to perform a systematic review and meta-analysis to compare the results of the Latarjet procedure performed using S or SB for coracoid graft fixation.
Methods
Search strategy and study selection
Two independent reviewers searched in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and then analyzed the search results. In the event of disagreement, a senior author would intervene. The following were search terms that were used in The Cochrane Library, EMBASE, and Pubmed from their inception to June 2023: (Latarjet) AND (suture or SB or tight-rope or endo-button or dynamic or suspensory or cortical or screw or fixation)). Both the abstract and the title were reviewed for all identified studies, followed by a thorough review of each full text. Furthermore, references included in the studies identified were reviewed for additional studies that met the inclusion criteria.
Eligibility criteria
Inclusion criteria were as follows: (s) Clinical cohort studies comparing screw fixation and SB fixation for the Latarjet procedure, (b) published in a peer-reviewed journal, (c) published in English or full translation freely available, and (d) full text of studies available. All other studies were excluded.
Data extraction
Two independent reviewers collected all relevant information using a predetermined data sheet on Microsoft Excel. In the instance where required information was not offered in the text, authors were contacted via email. Level of evidence (LOE) was assessed using the criteria from the Oxford-Centre for Evidence-Based Medicine. Methodological quality of the evidence (MQOE) was assessed using the Newcastle-Ottawa scale, which is a 9-point scale where studies 7–9,4–6, and 1–3 points were identified as very good, good, satisfactory and unsatisfactory, respectively.
Outcomes analyzed and statistics
Statistical analysis was performed using Review Manager ((Revman) [Macintosh]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.) Heterogeneity between studies was quantified using the I2 statistic. Random-effects models were employed. Results were expressed as risk ratio (RR) for dichotomous outcomes and mean difference (MD) for continuous outcomes, with a 95% confidence interval (95% CI). A p-value of < 0.05 was considered to be statistically significant.
Results
Literature search
The initial literature search resulted in 758 total studies. Once duplicates were removed 478 studies were assessed for eligibility and full texts were reviewed. Five studies with 877 unique patients were included in this review (Figure 1).
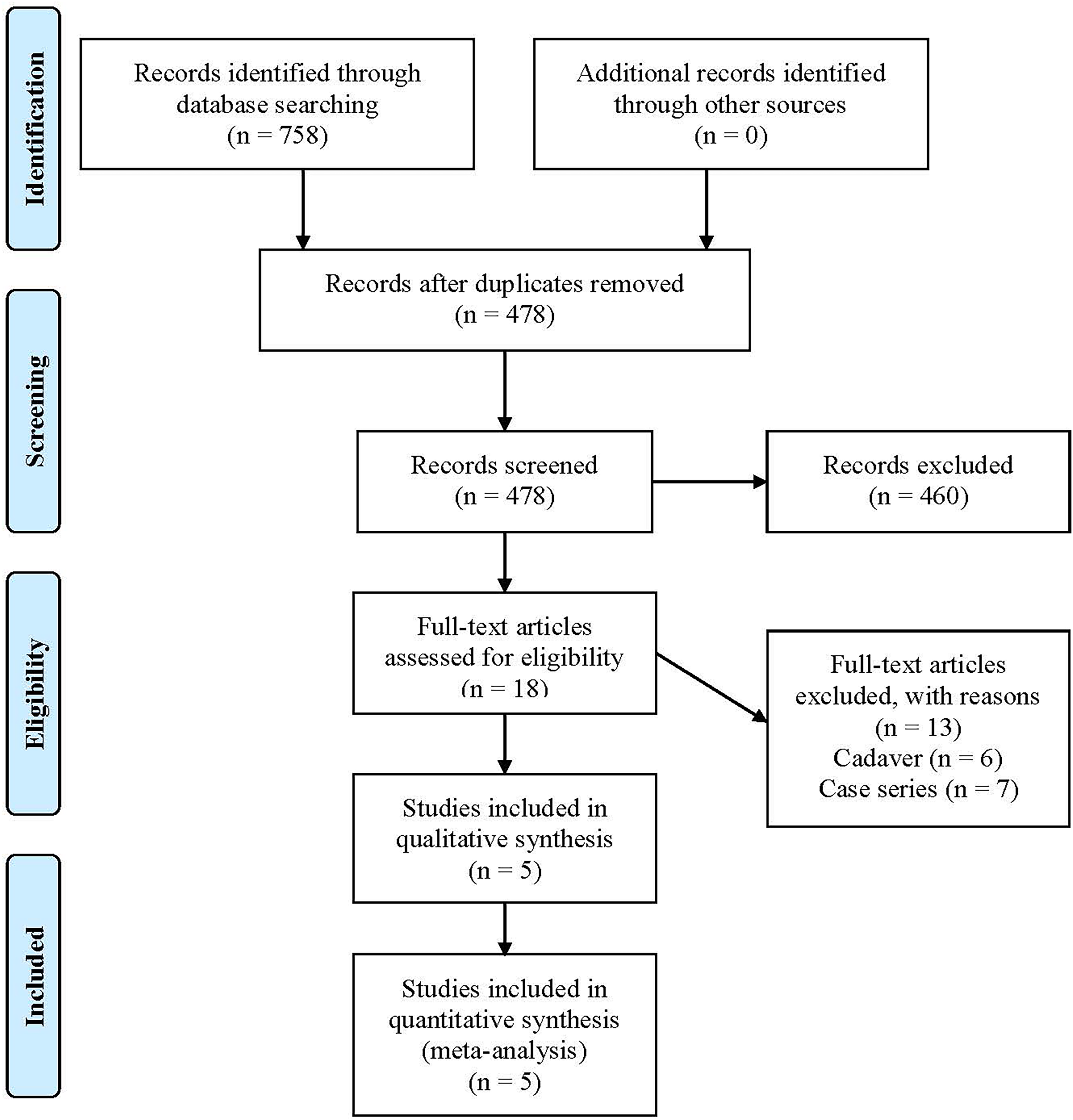
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Study characteristics and patient demographics
There were 5 studies included (LOE II = 1, LOE III = 4), with 657 patients treated with screw fixation and 220 with SB fixation. The mean MQOE was 7.4 (6–9). Overall, 85% of the patients were male with an average of 27.5 years old, and a mean follow-up of 32 months. The study characteristics and patient demographics are detailed in Table 1.
Study characteristics.
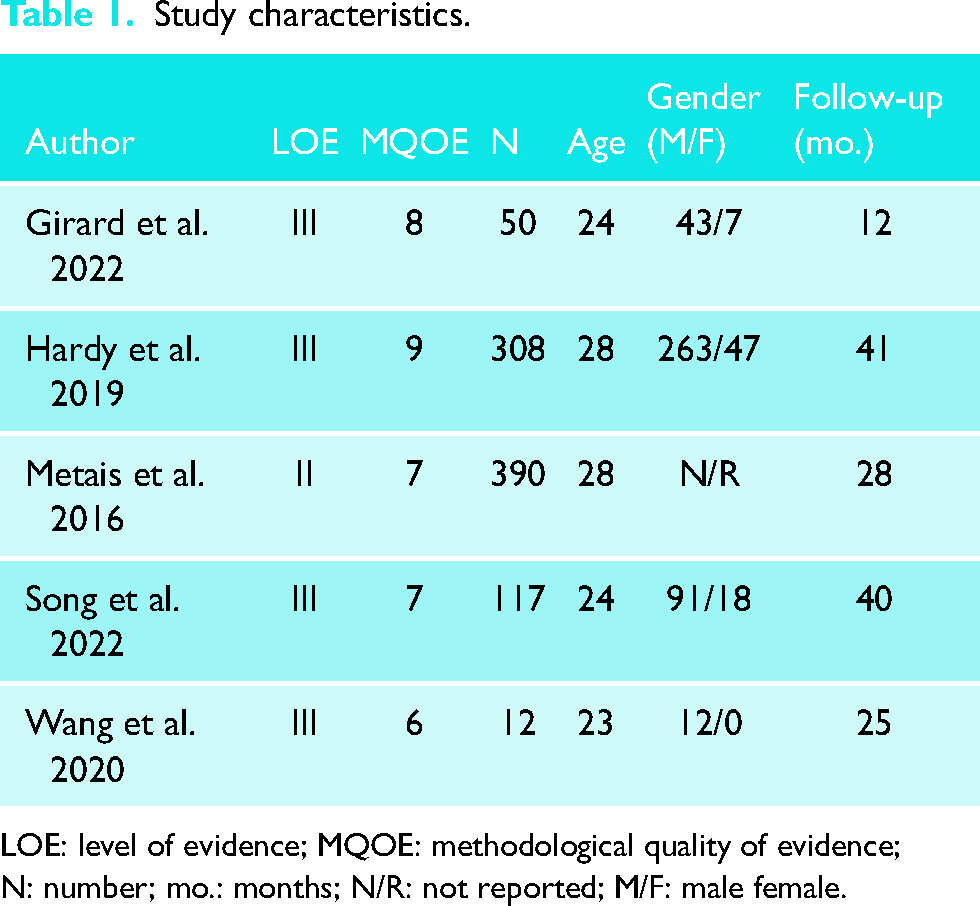
LOE: level of evidence; MQOE: methodological quality of evidence; N: number; mo.: months; N/R: not reported; M/F: male female.
Clinical outcomes
Recurrent instability
Overall
Recurrent instability was reported in all studies. Overall, 1.5% of patients treated with screw fixation and 5% of patients treated with SB fixation had recurrent instability. There was a statistically significant difference in favor of screw fixation (RR, 0.26; 95% CI, 0.11–0.59; I2 = 0%; p = 0.001) (Figure 2).
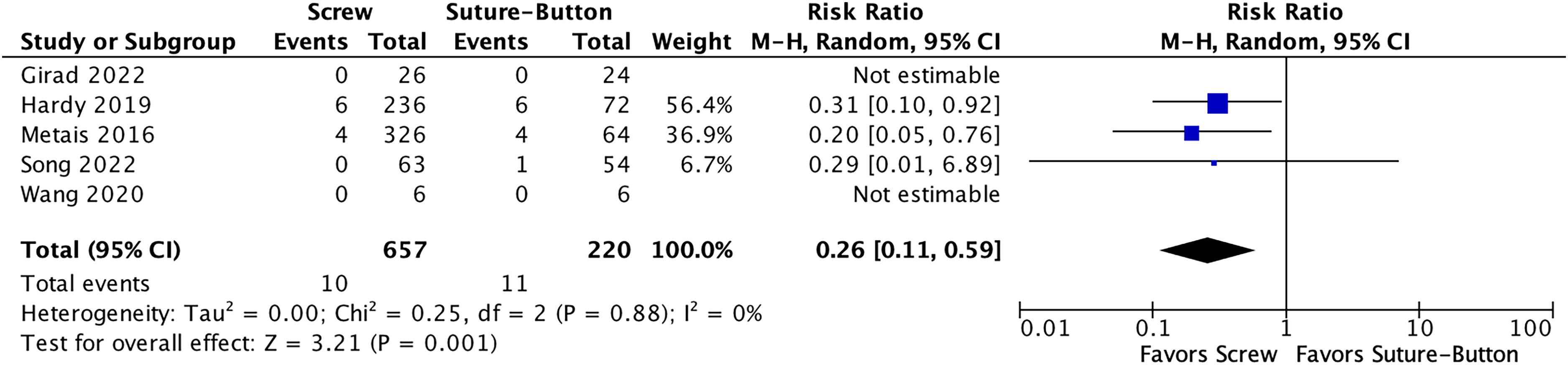
Forest plot of recurrent instability.
Reoperations
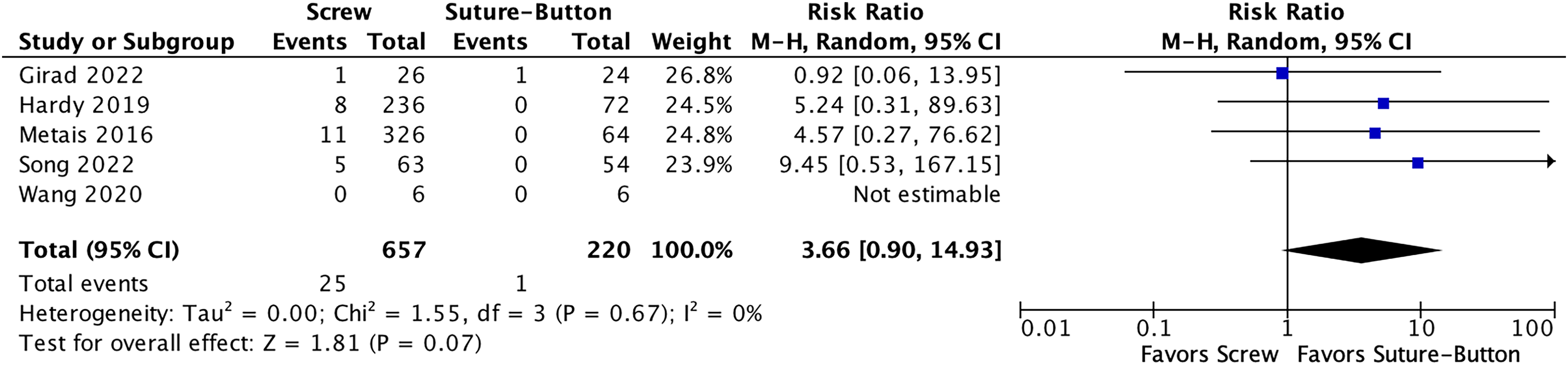
Reoperations, other than for recurrent instability, were reported in all studies. Overall, 4.3% of patients treated with screw fixation and 0% of patients treated with SB fixation had a reoperation. There was a statistically significant difference in favor of SB fixation (RR: 4.88; 95% CI, 1.12–21.17; I2 = 0%; p = 0.03) (Figure 3).
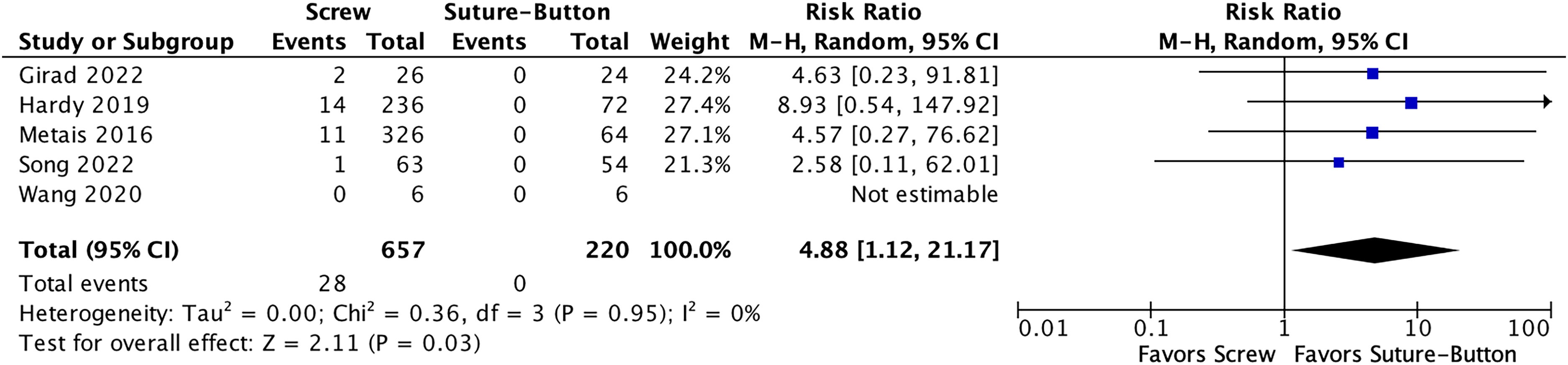
Forest plot of reoperations.
Complications
Complications were reported in all studies. Overall, 7.5% of patients treated with screw fixation and 3.6% of patients treated with SB fixation had a complication. There was no statistically significant difference (RR, 2.18; 95% CI, 0.81–5.90; I2 = 24%; p = 0.12) (Figure 4).
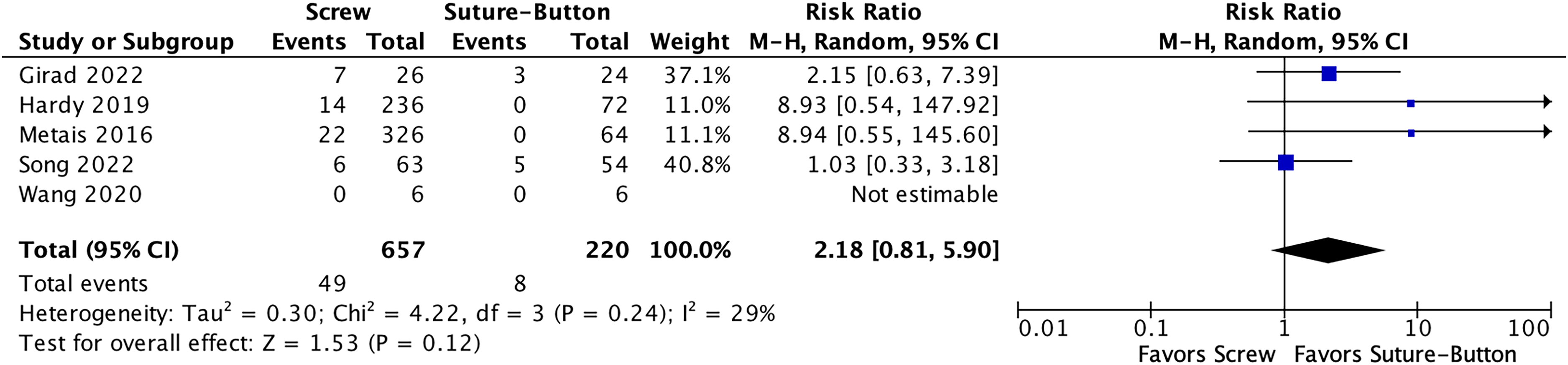
Forest plot of complications.
Graft Fracture
Graft fractures were reported in all studies. Overall, 0.8% of patients treated with screw fixation and 0.5% of patients treated with SB fixation had a graft fracture. There was no statistically significant difference (RR, 1.52; 95% CI, 0.28–8.15; I2 = 3%; p = 0.62) (Figure 5).
Forest plot of graft fractures.
Symptomatic Hardware
Symptomatic hardware was reported in all studies. Overall, 2.7% of patients treated with screw fixation and 0% of patients treated with SB fixation had symptomatic hardware. There was no statistically significant difference (RR, 3.81; 95% CI, 0.70–20.76; I2 = 0%; p = 0.12) (Figure 6).
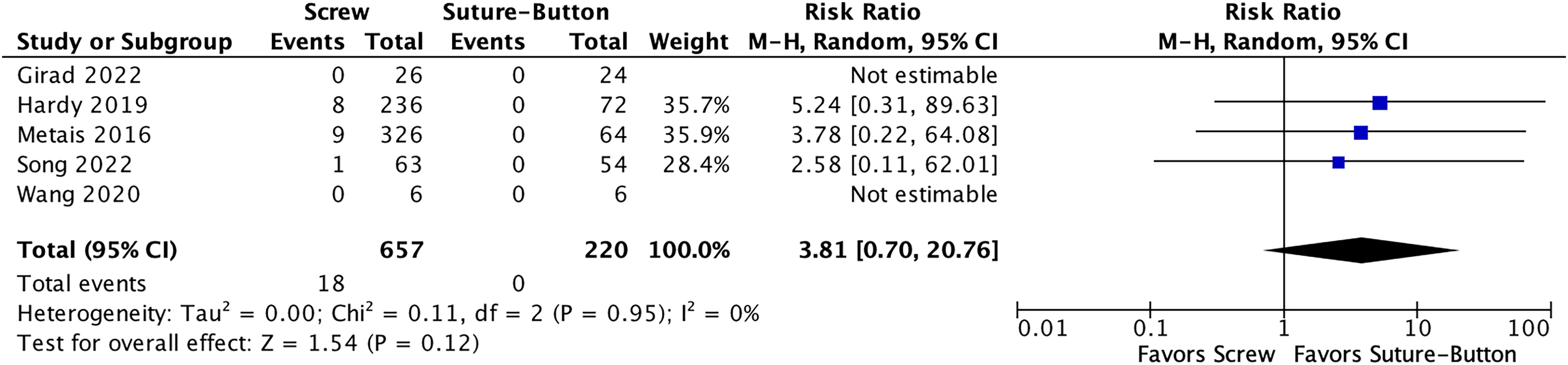
Forest plot of symptomatic hardware.
Pain
Pain was reported in 3 studies, with 305 patients treated with a screw fixation and 132 with a SB fixation. Overall, the mean VAS score for pain for both screw and SB fixation was 1.3. There was no statistically significant difference (MD, 0.01; 95% CI, −0.34 to 0.36; I2 = 0%; p = 0.95) (Figure 7).

Forest plot of pain.
Rowe Score
The Rowe score is a scale ranging from 1 to 100 designed to evaluate patients who have undergone surgery for instability and assesses mobility, stability, pain, and overall performance in work and sports activities. The Rowe Score was reported in 3 studies, with 92 patients treated with a screw fixation and 79 with a SB fixation. Overall, the mean Rowe Score for screw fixation was 94.6 and 93.8 in patients treated with SB fixation. There was a statistically significant difference in favor of screw fixation (MD, 0.74; 95% CI, −1.49 to 2.96; I2 = 0%; p = 0.52) (Figure 8).

Forest plot of the Rowe score.
Walch-Duplay
The Walch-Duplay score is a scale ranging from 1 to 100 designed to evaluate patients who have undergone surgery for instability and assesses mobility, stability, pain, return to sports and daily activities. The Walch-Duplay Score was reported in 3 studies, with 265 patients treated with a screw fixation and 97 with a SB fixation. Overall, the mean Walch-Duplay Score for screw fixation was 83.5 and 81.3 in patients treated with SB fixation. There was no statistically significant difference (MD, 2.17; 95% CI, −1.83 to 6.17; I2 = 0%; p = 0.29) (Figure 9).

Forest plot of the Walch-Duplay score.
Discussion
There were three main findings in this meta-analysis. First, regarding recurrences, S fixation was associated with a significantly lower rate of recurrences than SB fixation. Second, although there was no significant difference in the overall complication rate, significantly more patients in the S fixation group required reoperation due to implant-related problems. Third, we found no significant differences in functional scores or postoperative pain between patients treated with the two techniques.
Latarjet surgeries performed with either screws or SBs have shown low recurrence rates in this meta-analysis. However, the rate of recurrences was significantly lower in the group treated with S (1.5%) than in those patients fixed with SB (5%). This difference could be due to different factors. From a biomechanical perspective, some authors have reported that the initial stability provided by SB is less than that provided by screw fixation.7,16 This could lead to recurrent instability due graft displacement, osteolysis or bone-block resorption, or non-union. Finally, non-union of the graft could occur due to insufficient fixation stability, which could lead to residual pain or apprehension. Unfortunately, the studies analyzed did not evaluate whether the patients with recurrence had any of these complications. Therefore, the reasons why the patients fixed with the SB system had more recurrences can only be hypothesized.
It is important to note that although in the present meta-analysis the SB fixation group had significantly more recurrences, in part this difference could also be due to other confounding factors. For example, Hardy et al. 14 compared 236 patients with S fixation and 72 with SB fixation at a mean follow-up of 3.4 years and found that recurrent dislocation was significantly lower in the S group: 2.5% compared to 8.3% in the SB group, p = 0.02. Interestingly, the authors reported that the mean time from Latarjet to recurrent dislocation was 3 years in the SB group. This calls into question the possibility that the recurrences were due to inadequate initial fixation, since complications such as fragmentation, resorption, or initial displacement of the graft tend to occur in the first months after surgery.4,5 Thus, it is likely that other risk factors for recurrence have influenced the difference found in the present meta-analysis in addition to the fixation method. Future prospective randomized studies where the only factor that varies between groups is the fixation method would help to define more clearly whether the differences in recurrences can be attributed to the fixation method or whether other factors are involved. Moreover, it would also be important for future studies to describe the timing of recurrences and analyze whether patients with recurrences have any complications related to the graft that could explain the relationship between recurrence and the fixation method.
On the other hand, an important aspect to take into account is the definition of recurrences used in the different studies. Unfortunately, only the study by Hardy et al. specified that “recurrence was defined as a new episode of dislocation that required reduction by someone else.” 14 In contrast, the other 4 studies did not specify how recurrences were defined. This is an important aspect to consider due to the fact that the way recurrences are defined can significantly influence the outcomes. In a recent systematic review of the literature, Kennedy et al. 17 reported that recurrences varied from 10% if only dislocations were assessed, to 16.5% if dislocations, subluxations and painful apprehension were considered.
Regarding the total rate of complications, we did not find any significant differences between the groups analyzed. It is important to highlight that the overall complication rates found (7.5% in the S group and 3.6% in the SB group) were lower than those reported in the literature.4,5 This could be due to the fact that the two studies that contributed the largest number of patients to this meta-analysis6,14 were multicenter studies in which expert surgeons with extensive experience in the technique participated. It is important to note that although in the following meta-analysis, 39% of the patients (340 of the 877 patients) were operated on arthroscopically, none of the studies reported the surgeons’ previous experience with the arthroscopic technique; therefore, it was not possible to analyze the influence that the surgeons’ learning curve may have had on the results found. However, previous studies showed that the arthroscopic Latarjet procedure has a high learning curve and the rates of complications, especially at the beginning, can be high.18
Regarding reoperations, it is important to highlight that there was a significant difference between the groups, with a 4.3% rate in the S group and 0% in the SB group. This difference was mainly due to the number of patients for whom it was necessary to remove the screws due to pain and irritation. For example, in the study by Hardy et al., 57% of the reoperations were for screw removal. 14
Finally, this study confirms that the Latarjet surgery is associated with very good functional results. The most frequently used scores in the evaluated studies were the Rowe and Walch-Duplay scores, which were reported in three studies each. The mean Rowe Score was 94.6 and 93.8 for S and SB fixation, respectively, and the mean Walch-Duplay Score was 83.5 and 81.3 for S and SB fixation, respectively, without any significant differences between the groups. In addition, the final VAS was 1.3 in both groups, reflecting virtually no pain. Unfortunately, return to sport could not be meta-analyzed because it was only reported in one of the studies. Girard et al. 13 evaluated 50 patients (24 fixed with S and 26 with SB). They reported 86% and 87% return to sports at 12 months follow up. Future comparative studies should include return to sport as an important outcome variable to take into account since many of these patients are young athletes who intend to compete again.
This study has several limitations and potential biases, including the limitations of the included studies themselves, as this is a systematic review. First, with all of the included studies being retrospective in nature, the lack of prospective studies is a weakness. Second, there was a mixture of both open and arthroscopic approaches, which may impact the outcome. Third, in most of the studies evaluated, the definition of what was considered a recurrence was not described adequately. However, there was 0% heterogeneity across almost all of the included outcome measures indicating that there was consistency regardless of the approach, and variance may simply be due to the fixation method.
Conclusion
The Latarjet surgery was associated with very good functional results and a low rate of complications regardless of the type of fixation used. Screw fixation was associated with a significantly lower rate of recurrences. However, this was at the expense of a greater number of patients who required S removal due to irritation or pain after surgery. Regarding postoperative pain and functional outcomes, there were not significant differences between S and SB fixation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The category in which the manuscript is being submitted is Systematic review—meta-analysis. The paper is not based on a previous communication to a society or meeting.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.