
Abstract
Background
There is limited evidence about exercise performance during postoperative immobilization. This study aimed to quantify the muscle activity in the immobilized shoulder girdle in an abduction and neutral rotation position during a battery of contralateral activities and ipsilateral exercises of the upper limb in healthy volunteers and patients with unilateral shoulder pain (USP).
Methods
Thirty participants were included and grouped as without (N = 17) or with USP (N = 13). Muscle activity (percentage of maximum voluntary isometric contraction (%MVIC)) of the serratus anterior (SA), upper trapezius (UT), lower trapezius (LT) and infraspinatus muscles was assessed during five contralateral activities (during comfortable speed, fast speed and comfortable speed with additional load) and seven ipsilateral exercises.
Results
No differences in % MVIC were found between healthy volunteers and patients with USP on immobilized upper limb exercises and with the contralateral shoulder girdle. General muscle activity was low (<15% MVIC) to moderate (21–40% MVIC). This similarity was maintained at different speeds and with additional load. Adapted lawnmower exercise showed a favorable UT/LT activation ratio.
Conclusion
The study results support the use of all evaluated shoulder exercises, as they have shown low muscle activity, which is important for early rehabilitation phases.
Introduction
Shoulder pain is one of the most common musculoskeletal pain presentations 1 and results in over three million visits to physicians each year. 2 Of those visits, rotator cuff disease is the most common cause, 2 and a high percentage of patients require surgical repair and a rehabilitation process. 3 Shoulder immobilization is commonly used as a protective intervention for a period of days to weeks; however, it may result in muscle weakness and loss of normal neuromuscular control.1,4 The influence of postoperative rehabilitation on the healing and clinical results after arthroscopic rotator cuff repair has received increasing attention.5,6 Theoretically, the timing of shoulder motion and the progression of rehabilitation milestones may directly influence tendon healing following surgery, but this topic is still under investigation.7–11 Currently, there is no consensus on the best immobilization position,12–14 and the required optimal time for immobilization is still unknown.1,12 However, shoulder abduction is often used to prevent postoperative tears and promote healing of the repaired tendon.12,15–17
Advances in surgical techniques have contributed to the demand for treatment of rotator cuff injuries. In this regard, the evidence regarding the approach to post-surgical rehabilitation remains uncertain. 1 There is limited evidence about muscle activity during exercise, especially during the immobilization stage, except for the studies of Smith et al.18,19 The authors concluded that contralateral movements of the upper limbs at self-selected speeds are likely not detrimental to healing tissues. 18 They suggest clinicians prescribe specific movements of the contralateral upper limbs to facilitate early activation of the middle and lower trapezius (LT) muscles (cross-body reach, straight-forward reach and downward reach). 18 The authors recommended that scapular depression and protraction exercises could be performed safely after rotator cuff repair to facilitate scapulothoracic rehabilitation. 19 However, limitations should be considered: the sample size was small, only asymptomatic subjects were studied, and the exercises were performed with shoulder girdle immobilized in adduction and internal rotation, which is currently not the only recommended modality.
Exercise selection during rehabilitation is often based on the minimal load on the injured/repaired glenohumeral structures, combined with optimal activation of the scapulothoracic and rotator cuff muscles. 20 This is relevant for recovery due to the overactivity of the immobilized muscles during the acute healing phase. 5 Thus, it is critical to establish exercise selection criteria based on parameters derived from the electromyographic findings. Electromyographic activity levels lesser than 20% maximal voluntary isometric contraction (MVIC) are within the previously reported range of electromyographic activity for Neer Phase I supine and upright exercises. 18 These levels are often considered safe during the acute post-injury or postoperative period. 21 Other published reports suggested 15% MVIC.5,8,22,23 However, there is no precise recommendation on the optimal level for the immobilization stage.
In this study, we aimed to quantify the muscle activity in the immobilized shoulder girdle in abduction (20°) and neutral rotation during a battery of contralateral activities (during comfortable speed, fast speed and comfortable speed with additional load) and ipsilateral exercises of the upper limb, in patients with unilateral shoulder pain (USP) and healthy volunteers. The first hypothesis was that healthy volunteers and participants with USP would present similar muscle activity in all exercises and all muscles. The second hypothesis was that muscle activity during a contralateral exercise battery would be similar during slow, fast and resisted execution.
Materials and methods
Study design and participants
This is a cross-sectional study involving healthy volunteers and patients with USP. Participants with USP were recruited from a medical consultation and by invitation through social media. All participants received a verbal and written explanation of the study and written informed consent was obtained before inclusion. The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the bioethics research committee for human research of the Instituto Universitario Italiano de Rosario (number 19/18).
Sample size calculation
The one-tailed a priori sample size calculation used the effect size (ES) calculated based on the percentage electromyography (EMG) pairwise differences observed in a previous study. 24 The chosen variable was the infraspinatus muscle excitation during the press-up exercise. The accounted ES value was 1.33, with the α set at 5% and the expected power (1 - β) at 95%. The N1/N2 allocation ratio was set at 0.7. The analysis returned a minimal sample of 28 participants with an actual power of 0.96. The G-Power program (v3.1.9.7, Franz Faul, Universität Kiel, Kiel, Germany) was used to perform the sample calculation.
Recruitment criteria
Healthy volunteers were recruited from employees and students from the University of Gran Rosario, by a non-probabilistic convenience sampling. They were considered healthy if they exhibited a full, pain-free range of motion and no symptoms on physical examination. Volunteers were included in the USP group if they reported shoulder pain (>1 month during the last year, with a minimum pain intensity of 2/10 on the visual analogue scale) and if at least three of the following criteria were positive: positive Neer sign, positive Hawkins sign, positive Jobe's sign, Painful Arc sign and positive resistance test against external rotation. 25 Exclusion criteria were a history of dislocations or shoulder surgery, cortisone injections within the last 6 months, history of neurologic disorders, systemic disorders, cervical spine injuries or postural deformities, obvious scapular dyskinesis and unusually strenuous activity 48 hours before the testing session. The American Shoulder and Elbow Surgeons (ASES) scale was used to assess the extent of symptoms in the involved shoulder and as additional score to classify the participants into both groups. 26 The scapular movement pattern was evaluated using the “scapular dyskinesis test.” 27
Muscle activity recordings
Muscle activity was recorded using bipolar surface EMG using an amplifier with four channels (Miotec™, Biomedical Equipments, Brazil). EMG signals were amplified, filtered (Butterworth fourth-order, 20–450 Hz bandpass filter, 60 Hz notch filter), sampled (2 kHz) and digitalized (14-bit resolution) The EMG signals were recorded with surface Meditrace™ (Ludlow Technical Products, Canada) Ag/AgCl electrodes with a diameter of 1 cm and a centre-to-centre distance of 2 cm. Electrodes were placed in transverse orientation aligned with the underlying fibers on a muscle site. A reference electrode was placed on the lateral humeral epicondyle. Prior to EMG electrode placement, skin was cleaned with alcohol at 70% to eliminate residual fat, exfoliated with sandpaper for skin, and cleaned again with alcohol. The electrodes were positioned on the upper trapezius (UT) and LT, and serratus anterior (SA) muscle following Surface Electromyography for the Non-Invasive Assessment of Muscles (SENIAM) recommendations. 28 For the infraspinatus muscle, electrodes were placed following a previously published report. 29 The sEMG signals were normalized by the root mean square in μV maximum value obtained in three MVIC collected during manual muscular testing for each muscle. The EMG data for each muscle and each participant were averaged for each phase across the five repetitions.
Maximal voluntary isometric contraction
Three 5-second MVIC followed from each muscle were performed by each participant and were followed by 1 minute of rest for each tested muscle. The resistance was applied at the wrist. Standardized verbal commands (“start,” “force,” and “stop”) were used by the same rater for all test recordings. Before recording the first MVIC trial, the participants received an explanation about the position and the direction in which they should exert maximal effort. The mean among the MVIC trials was used to normalize the EMG signals. For the SA and UT muscles, the volunteers remained seated. For the SA muscle, the shoulder was flexed to 125°, while resistance was applied above the elbow, and the other hand was placed on the lateral scapula to stabilize it. 30 The volunteer was requested to perform an isometric contraction of shoulder flexion against the rater's manual resistance. For the UT muscle, the shoulders were placed in shrugged position and the arm along the side. Resistance was applied at the acromion. The volunteer was requested to perform an isometric contraction of the shoulder shrugged against the rater's manual resistance. 30 For the LT muscle, the participant was asked to lie in the prone position. The MVIC was collected with the shoulder fully extended with the scapula maximally retracted, while the resistance was applied against the fully flexed elbow on the distal humerus. 31 The participant was instructed to resist against the downward force. For the infraspinatus, the volunteers remained standing, and the shoulder was externally rotated with the elbow flexed at 90°. The volunteer was requested to perform an isometric contraction of shoulder external rotators against the rater's manual resistance. 29
Exercise description
A shoulder girdle immobilizer was placed in abduction (20°) and neutral rotation at a randomized side for the healthy volunteers. In participants with USP, the immobilizer was placed on the symptomatic side. Before data collection, the participants received familiarization sessions of the movements and the exercises to verify their understanding. Subjects completed one set of five consecutive repetitions of each activity (movements related to daily life) with the non-immobilized upper limb (Figure 1). All movements were conducted in a standing position, and for each one, five repetitions were conducted at a self-selected comfortable speed, five at a fast speed and the remaining five at a self-selected comfortable speed with additional load. The additional load was selected according to 8/10 on the Borg scale. Figure 2 shows the exercises with the upper limb immobilized (related to scapular rehabilitation) (Figure 2). All movements were completed in a standing position, and for each one, they completed five repetitions at a self-selected comfortable speed.
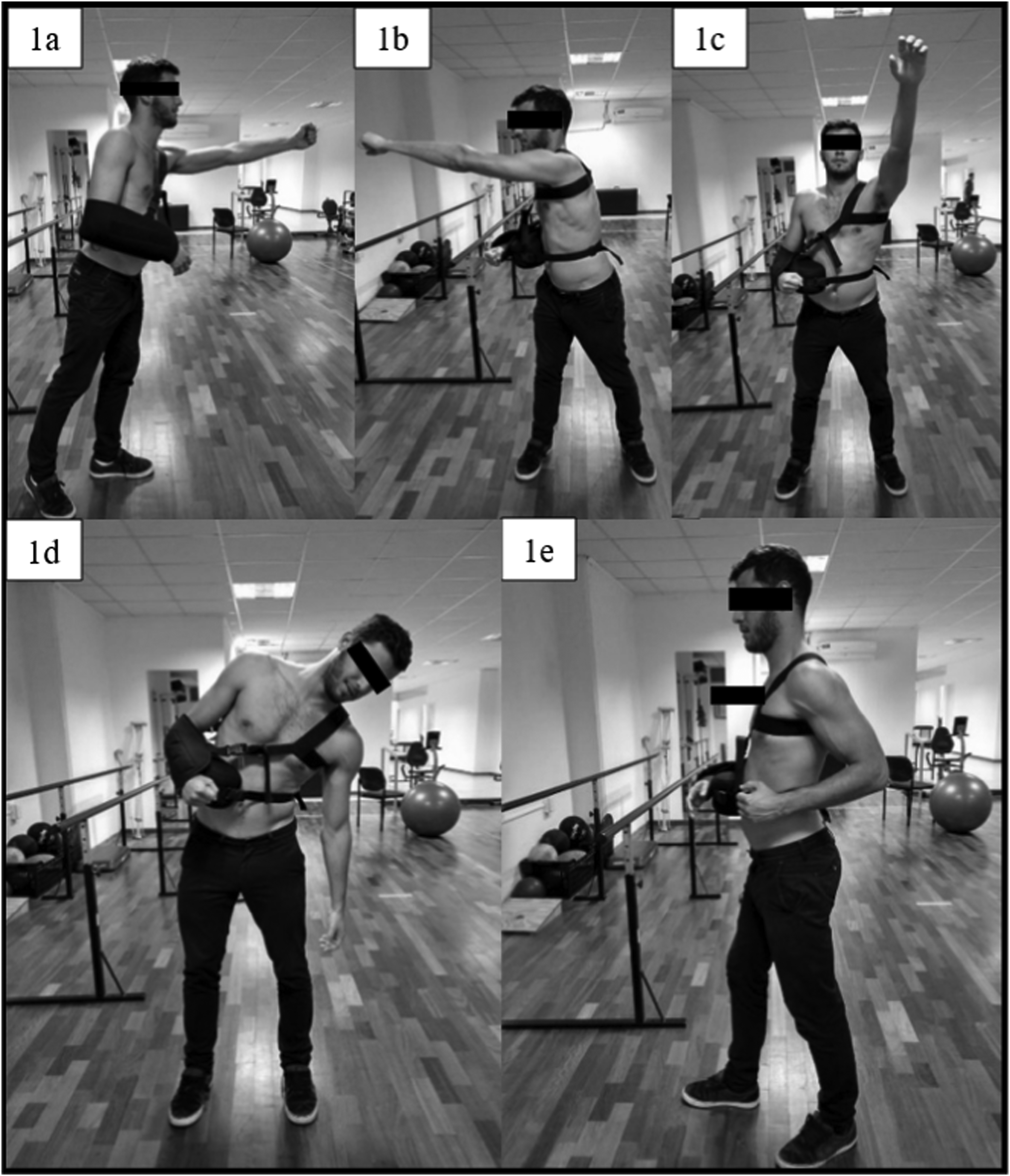
Contralateral activities and exercises. (1a) Straight-forward reach (Sfr), from a split stance position (the foot of the immobilized side was placed forward) with the hand of the non-immobilized side placed against the chest, the subject reaches directly forward to maximal upper limb extension. (1b) Cross-body reach (Cbr), similar to straightforward reach but the subject reaches maximally to the immobilized side. (1c) Upward reach (Ur), from a shoulder width stance with the non-immobilized elbow flexed and the hand adjacent to the left shoulder, the subject reaches maximally upward in the plane of the scapula. Downward reach (Dr), from a shoulder width stance with the non-immobilized arm at the side, the subject reaches down toward the left ankle in the coronal plane. (1d) Backward pull (Bp), from a split stance position (foot of the non-immobilized side forward) with the non-immobilized upper limb maximally extended straightforward, the subject rows backward producing maximal backward retraction of the non-immobilized upper limb so that the hand rests on the chest wall.
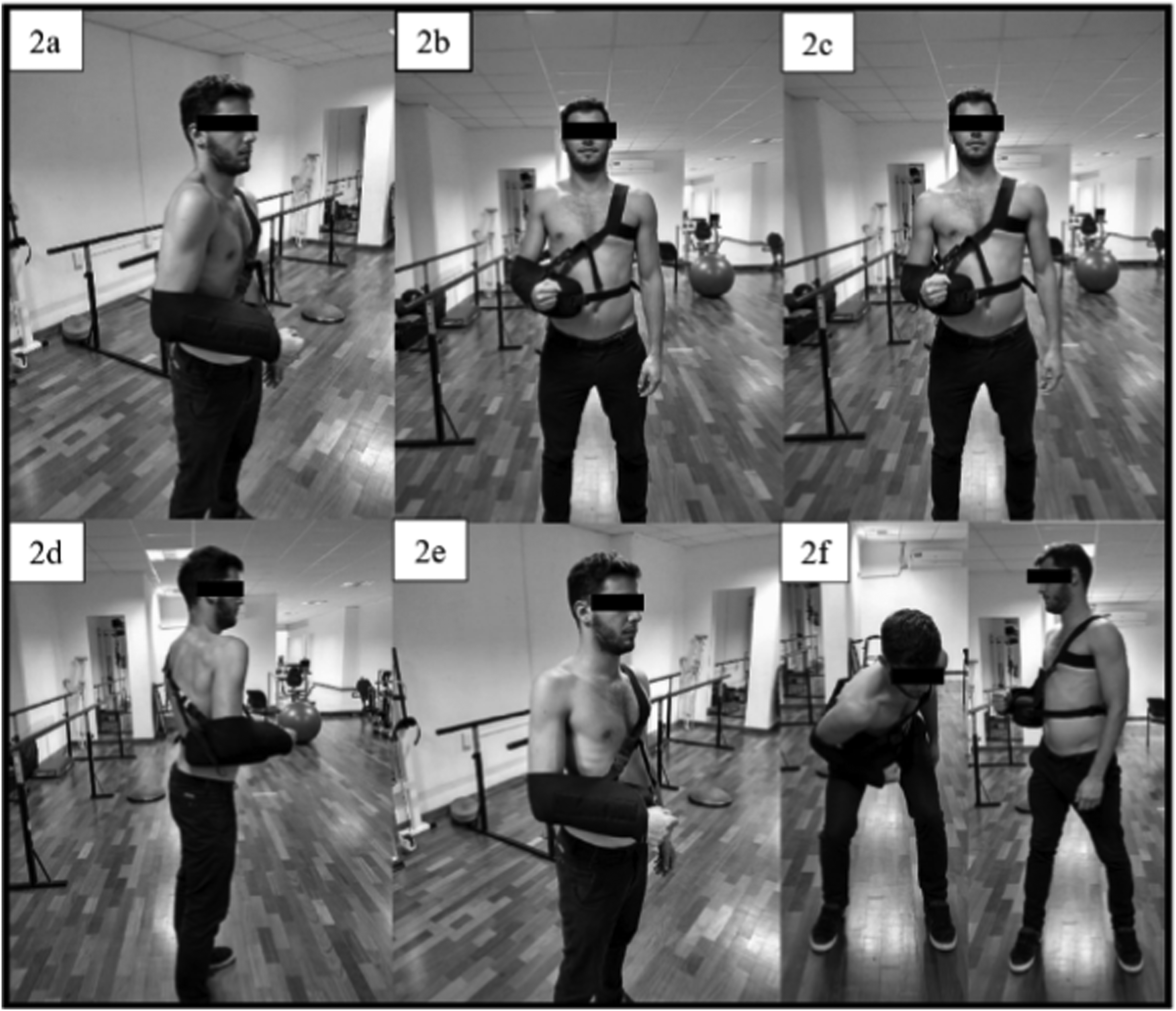
Ipsilateral activities and exercises. (2a) Scapular clock counterclockwise (Scccw), starting from resting neutral position, the subject moves the right shoulder forward, upward, backward and downward and then forward in a circumferential counterclockwise motion, scapular clock clockwise: similar to the scapular clock counterclockwise but in the opposite direction (no figure). (2b) Scapular elevation (Se), from neutral position, the subject elevates (i.e. shrugs) the shoulder and then returns to the starting position. (2c) Scapular depression (Sd), from neutral position, the subject depresses the shoulder downward and then returns to the starting position. (2d) Scapular protraction (Sp), from neutral position, the subject protracts the shoulder and then returns to the starting position. (2e) Scapular retraction (Sr), from neutral position, the subject retracts the shoulder and then returns to the starting position. (2f) Adapted lawnmower (Lm), subjects began the exercise standing with their arm supported in a sling. They were instructed to flex the trunk and rotate it to the non-immobilized side. They were instructed to extend the hip and rotate the trunk toward the tested side in a vertical orientation while retracting the scapula to attempt to place an elbow in their back pocket position.
Data analysis and statistics
The Shapiro–Wilk test was used to assess the normality. Data were presented as means and standard deviation. Between-group differences in anthropometric characteristics were assessed using the independent sample t-test. The factorial analysis of variance (ANOVA) with repeated measures was used to rate within and between-group differences (“group”), and the factor (“condition”) was represented by speeds and load. All data were reworked using Holm's post hoc test to compare pairwise differences avoiding multiple comparisons. The standardized differences for the comparisons were analyzed using the partial eta squared ES (η2p). The magnitude of the η2p was qualitatively interpreted using the following thresholds: ∼0.01 (small), >0.09 (medium) and >0.25 (large). The significance was set at P < 0.05. All analysis was performed using the Jamovi software (version 1.2, the Jamovi project, 2020 (retrieved from https://www.jamovi.org)).
Results
Enrollment
A total of 13 participants with USP and 17 healthy volunteers were included in the study. Population characteristics are summarized in Table 1.
Participant's characteristics.
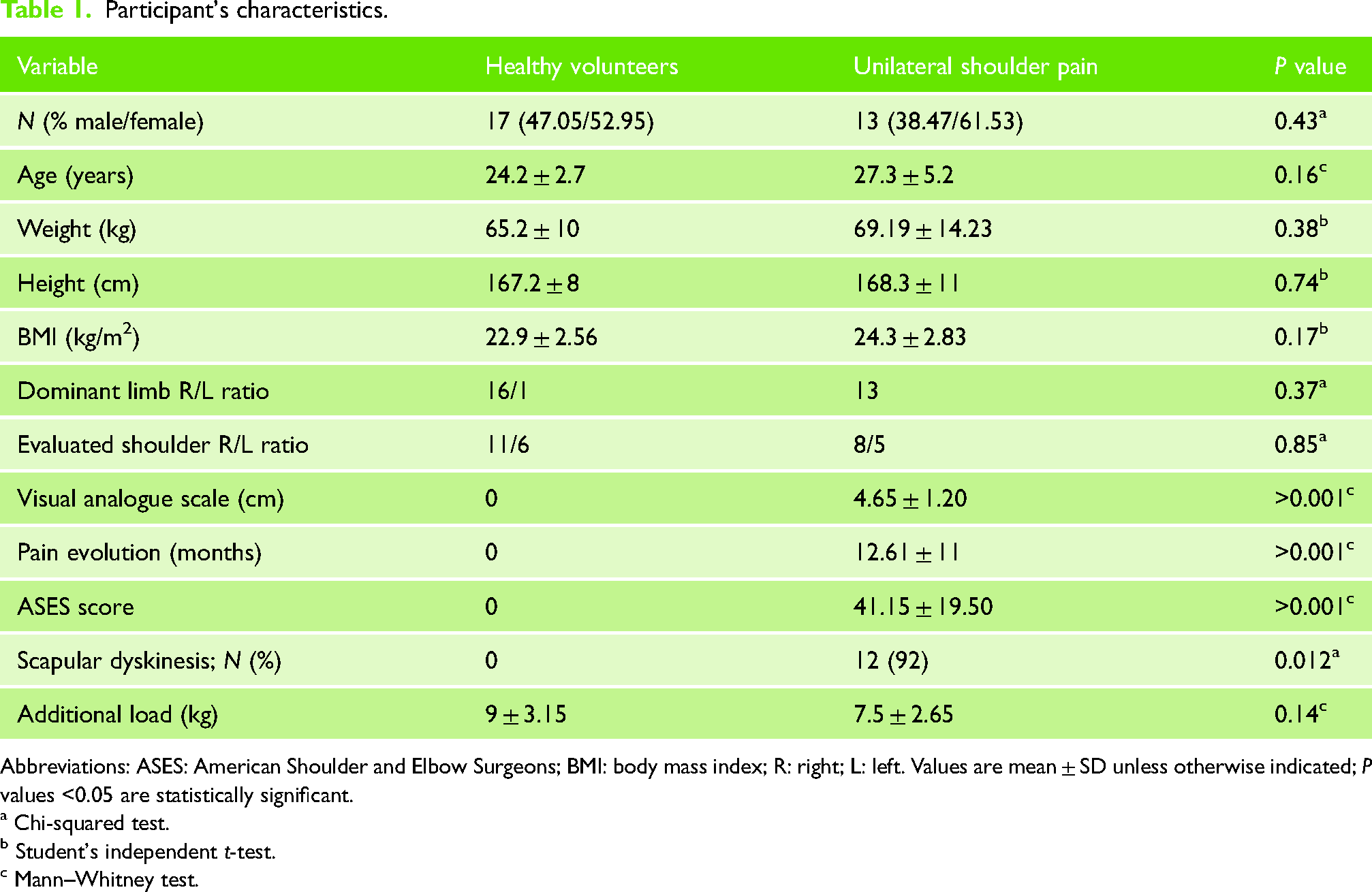
Abbreviations: ASES: American Shoulder and Elbow Surgeons; BMI: body mass index; R: right; L: left. Values are mean ± SD unless otherwise indicated; P values <0.05 are statistically significant.
a Chi-squared test.
b Student's independent t-test.
c Mann–Whitney test.
No differences in percentage MVIC were found between healthy volunteers and USP on immobilized upper limb exercises. General muscle activity was low to moderate (Table 2).
Independent sample t-test.
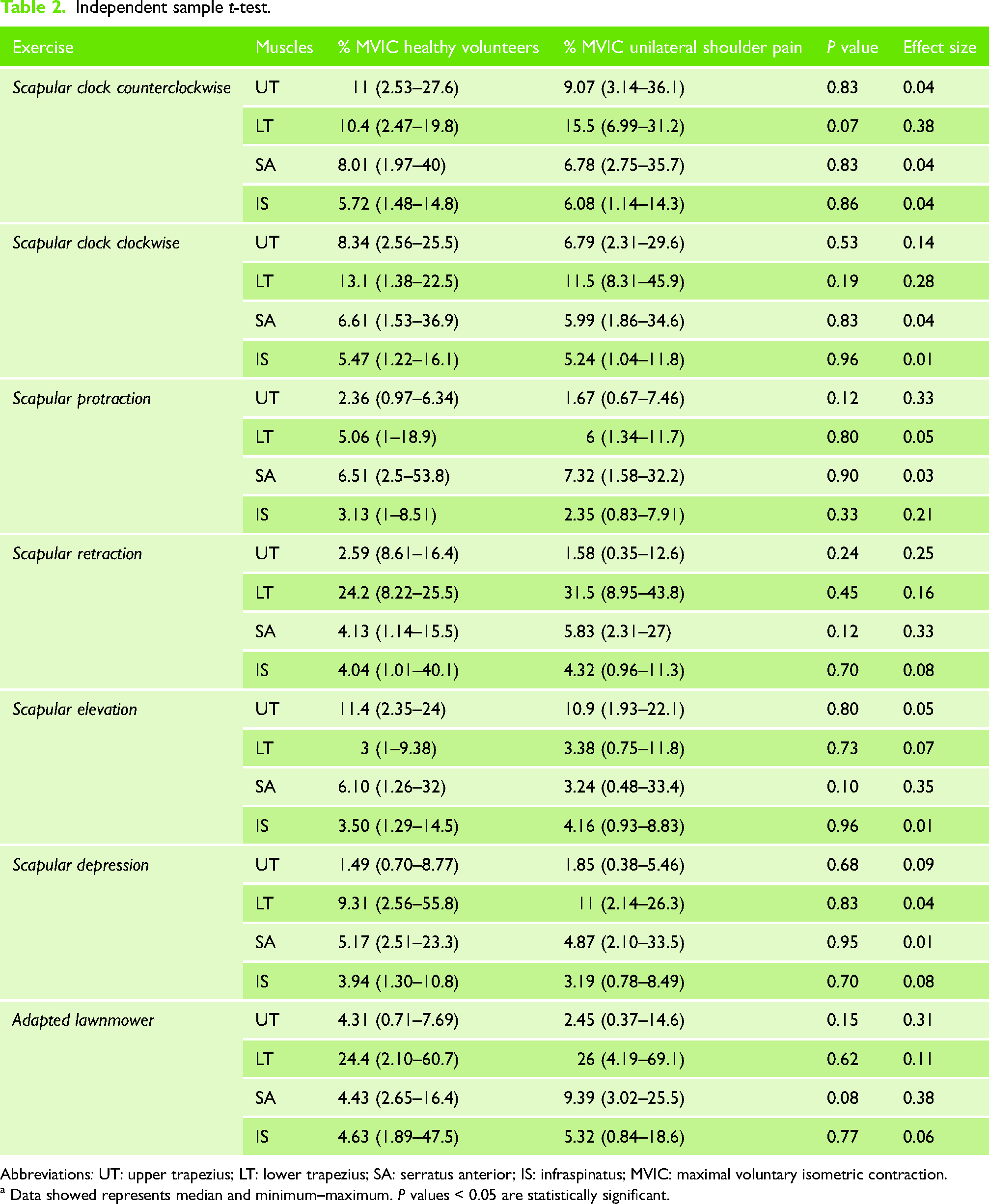
Abbreviations: UT: upper trapezius; LT: lower trapezius; SA: serratus anterior; IS: infraspinatus; MVIC: maximal voluntary isometric contraction.
a Data showed represents median and minimum–maximum. P values < 0.05 are statistically significant.
Within-group differences were observed for UT, LT, SA and IS muscles for the “condition” factor considering all the contralateral activities, except for LT (F(2,56) = 0.08; P = 0.92; ηp2 = 0.00) and SA (F(2,56) = 3.08; P = 0.053; ηp2 = 0.09) in the downward reach activity and IS (F(2,56) = 0.71; P = 0.49; ηp2 = 0.02) for the backward pull activity (Table 3). No within-group differences were observed for UT, LT, SA and IS for the factor “condition × group” for all the contralateral activities, except for the SA muscles (F(2,56) = 3.37; P = .042; ηp2 = 0.10) (Table 3). No between-group differences were observed for UT, LT, SA, and IS (Table 3).
Repeated measures ANOVA.
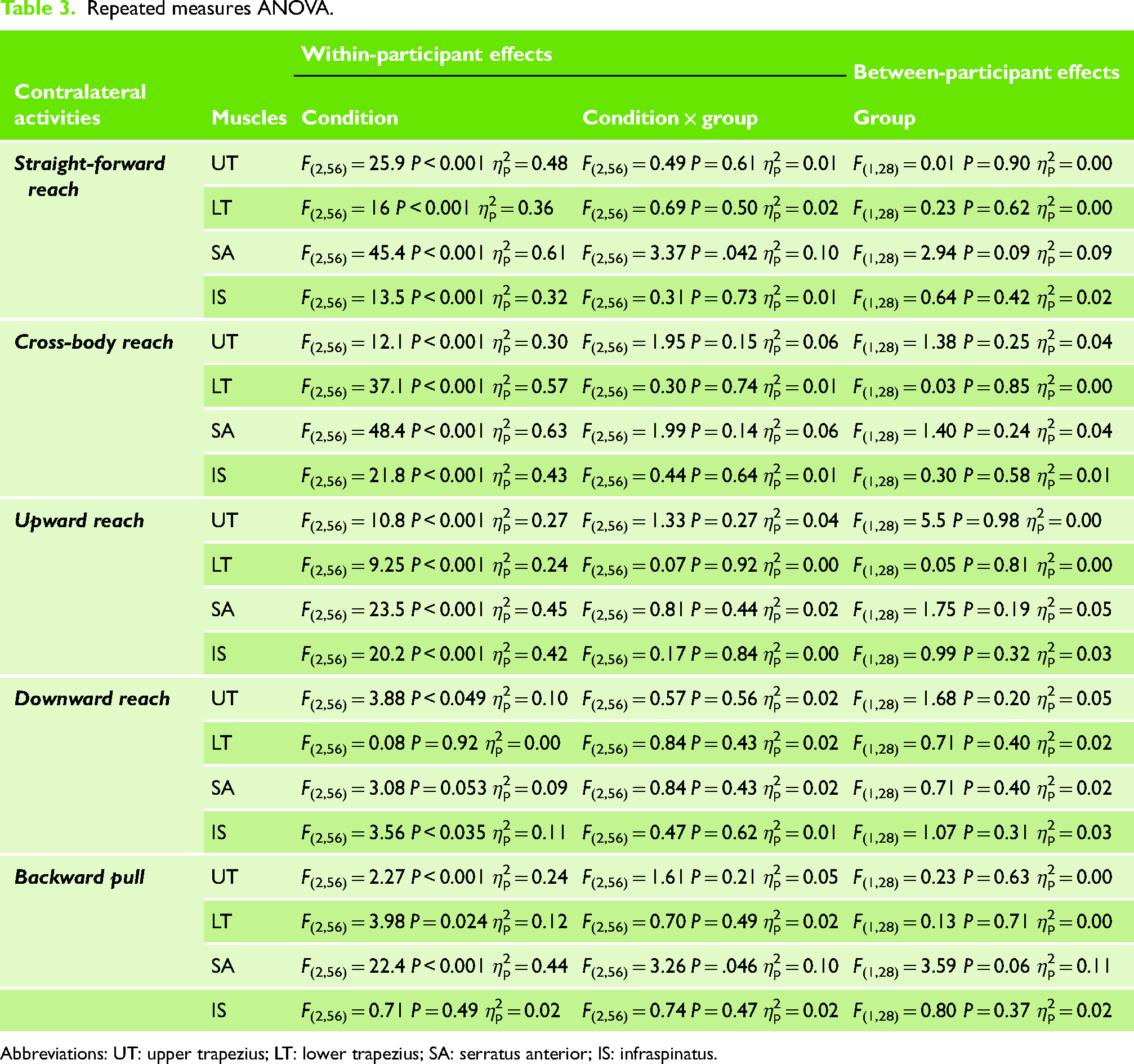
Abbreviations: UT: upper trapezius; LT: lower trapezius; SA: serratus anterior; IS: infraspinatus.
Post hoc comparisons
Straight-forward reach activity
For IS, UT, LT, and SA muscles for the “condition” factor showed significant differences (Pholm < 0.001). Additionally, for the SA muscle, the “condition × group” factor revealed significant differences for different conditions (Pholm < 0.001).
Cross-body reach and upward reach activities
Most muscles in the “condition” factor showed significant differences for the comfortable speed/additional load and additional load/fast speed comparisons (Pholm < 0.001). Except in the upward reach activity, for the LT, only the comfortable speed/additional load comparison yielded a significant difference in the “condition” factor (Pholm < 0.001).
Downward reach activity
The “condition” factor did not show significant differences for all the muscles.
Backward pull activity
For the UT, the “condition” factor showed significant differences for the comfortable speed/additional load (Pholm < 0.001) and additional load/fast speed (Pholm = 0.002). For the LT, the “condition” factor showed significant differences for the comfortable speed/additional load (Pholm = 0.020). For the SA, the “condition × group” showed significant differences for the pain-comfortable speed/pain additional load and pain/fast speed–pain/additional load, respectively (Pholm < 0.001).
No differences in percentage MVIC were found between healthy volunteers and patients with USP for all the muscles, conditions and activities (Table 4).
% MVIC in contralateral activities.
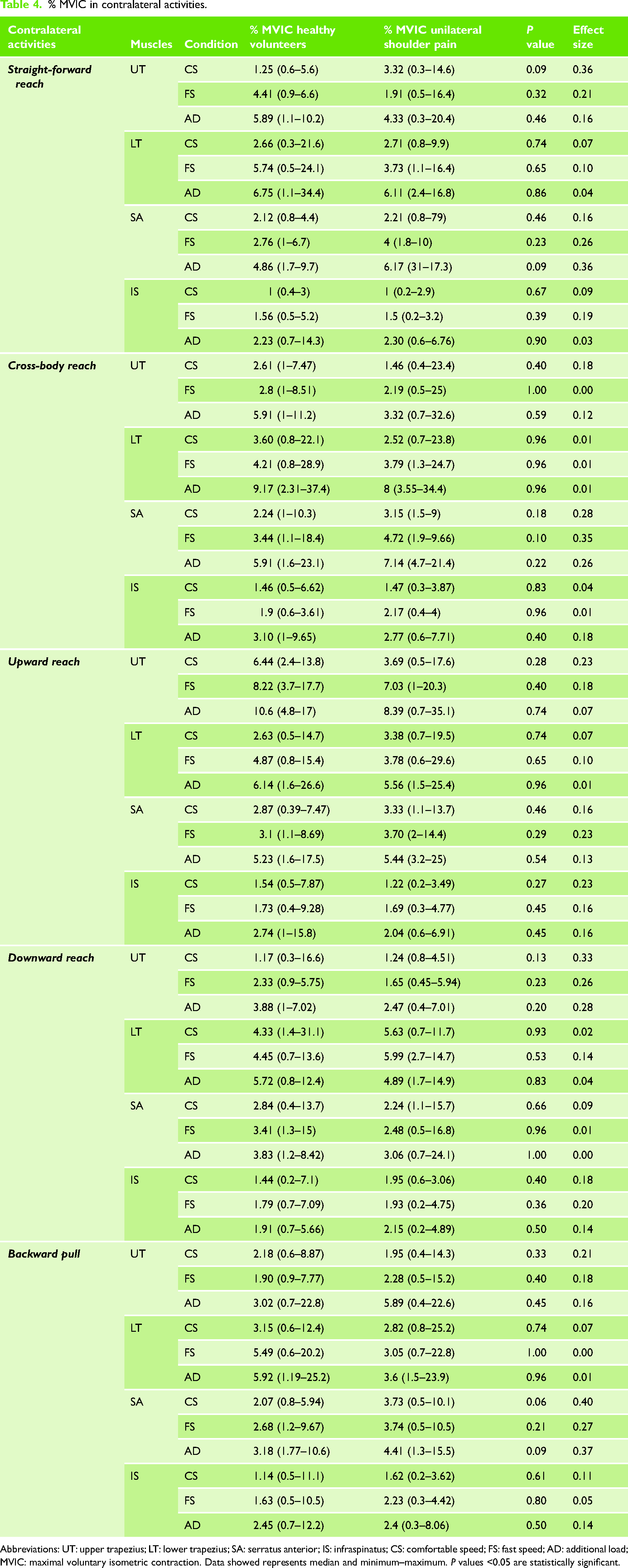
Abbreviations: UT: upper trapezius; LT: lower trapezius; SA: serratus anterior; IS: infraspinatus; CS: comfortable speed; FS: fast speed; AD: additional load; MVIC: maximal voluntary isometric contraction. Data showed represents median and minimum–maximum. P values <0.05 are statistically significant.
Discussion
The main objective of this study was to assess the muscle activity of the UT, LT, SA and IS muscles in healthy volunteers and patients with USP. The results showed no significant differences in electromyographic activity between the groups. The activity was similar in the exercises with the immobilized limb and the movements of contralateral shoulder girdle. This similarity was maintained at different speeds and with additional load. On the other hand, the global activity of the infraspinatus muscle was always very low, indicating that physiotherapists and physicians could prescribe this type of exercise in the early phases of rehabilitation.
Beyond the injury, immobilization can generate negative changes in the upper extremity. 32 Immobilization has shown a 35% loss of strength in elbow extension coupled with a decrease in upper arm girth following a 5-week immobilization by using a fiberglass elbow cast extended from the shoulder to the hand. 33 Furthermore, it revealed that significant bone mineral density loss occurred in the proximal humerus after 6 weeks of immobilization. 33 Those findings support the use of exercises in the early phases of rehabilitation to avoid the adverse effects of immobilization.
Immobilization protects the tendon from excessive force and prevents re-tearing after surgery. 15 However, re-tear after rotator cuff repair is still frequent. Evidence reports a prevalence of 20% to 90% postoperative re-tears.15,34 There are two modifiable factors that surgeons might be aware of: the surgical technique and the postoperative activities.4,35 Although the optimal time of immobilization is unknown, generally for the first 6 weeks, the shoulder is immobilized with a sling.1,4,8 Delayed movement onset may increase the risk of postoperative shoulder stiffness and muscle atrophy, impairing functional recovery. 4 Based on this information, some surgeons opt for early mobilization in order to improve shoulder function and avoid tissue stiffness.1,15,17 Moreover, mechanical tension plays an important role of organizing the tissue healing process at the repaired tendon site. 15 The force transmission across the healing interface may promote the organization of collagen deposition through biochemical changes in tenocytes. 15
Our first hypothesis was that healthy volunteers and patients with USP would present similar muscle activity in all movements and exercises in all muscles. The results showed no differences between groups in the muscle activity of the analyzed muscles, in any movement, exercise or condition. On the other hand, the global activity of the IS muscle was always very low, indicating that physicians could prescribe this type of exercise in the early phases of rotator cuff surgery rehabilitation. This inference derives from muscle activity below 15% MVIC in all exercises.5,22
One of the most differential aspects of the previous literature was the excitation levels of the scapular muscles (UT and LT muscles).18,19 The previous studies described activation levels greater than 50% MVIC in the UT muscle during the backward pull. 18 Thus study showed less than 15% MVIC for the same exercise, with 31.5% MVIC for the highest value during scapular retraction in patients with shoulder pain in the LT muscle, which was much lower compared to the value above 70% reported by Smith et al. 18 Our findings showed a considerably low overall muscle activation compared to the studies by Smith et al.18,19 where the electrical activity was above 50$ to 60% MVIC. Neither the cross-body or downward reach movements with the contralateral limb nor the scapular depression and protraction with the ipsilateral limb generated high IS muscle activity. This is why these movements can be considered as safe.
Some movements (scapular retraction and adapted lawnmower) generated an activation of the LT muscle greater than 20% MVIC with a favorable ratio to the UT muscle. Thus, safe strengthening in the scapular musculature may take place. Previous studies showed that moderate levels of muscle activation (20–40% MVIC) are considered adequate to retrain neuromuscular control of the scapular girdle.30,31
Cross-body rotations were the best exercise to achieve early activation of the SA muscle, being more selective at lower levels. 36 This premise encouraged the analysis of the lawnmower exercise described by Kibler et al. 30 who found that this exercise produced greater than 20% MVIC activation of the UT, LT and SA muscles. We propose a novel approach by adapting this exercise to patients with a sling. The subject performs a squat to approximate the immobilized shoulder with the opposite knee; after that he/she ascends and performs a scapular retraction and depression rotating the trunk toward the immobilized side. Unlike Kibler et al., 30 our findings show that the activity of the UT and SA muscles was less than 20% MVIC, so the TS/TI activation ratio is favorable to make it an exercise that could be used in the early stages of immobilization to strengthen the LT muscle, and pain would not be a limitation because muscle activity was similar between groups. The coordination between the movement of the lower part of the body and the gesture of the upper part did not produce major changes in the activation of the scapular muscles but could favor the preservation of motor and/or sports gestures after surgery.
Regarding the second hypothesis, the additional load in straight-forward reach, cross-body reach, upward reach, downward reach and backward pull did not cause changes in muscle activation levels. The absence of differences between the groups is an important finding, as it suggests the benefits of the current exercise in achieving exercise goals for both groups, meaning that people with shoulder pain were able to achieve the same levels of muscle arousal in each level, even with an additional load. It should be noted that the addition of load to the movements was performed with a variable load and a participant-perceived sensation of effort of 8/10. Unlike other studies that incorporated a fixed load using free weights, 18 we used a pulley device to execute these movements.
In our work, the analysis of the different conditions (comfortable speed, fast speed and comfortable speed with additional load) showed intra-subject changes in the other conditions except in the downward reach movement concerning the SA and LT muscles and in the backward pull movement for the IS muscle. The findings associated with intragroup changes (healthy volunteers or patients with USP) only showed changes in the SA muscle in the straightforward reach and backward pull. The comparison between groups yielded no differences, suggesting that participants with USP would not show changes in their muscle activation in various performance conditions. This should be considered when indicating exercises to patients with pain or post-surgical immobilization. Moreover, the speed of execution and the load should be contemplated as a progression variable.
Some limitations of the current study should be considered. First, we did not evaluate the muscular activity of the supraspinatus, subscapularis and biceps due to technical limitations, as well as other muscle groups that might influence the data correlation with compensatory movements during the standing position. This could be important in patients with surgical repair of these muscles. Second, the movements and exercises were not performed in random order. Third, the convenience sample was constituted by young adults, so results must be interpreted in this age range. The strengths include the sample size, the inclusion of mixed-sex participants and the presence of a group with shoulder pain. Other studies on shoulder girdle EMG only included healthy subjects, not reflecting the performance in symptomatic patients. Furthermore, all exercises were performed with the shoulder girdle immobilized in abduction, which is currently the most recommended position. Finally, our study proposes a safe alternative for strengthening the SA and LT muscles which can be used as part of a comprehensive rehabilitation program to restore shoulder function.
Conclusion
The study results support the use of all evaluated shoulder exercises for early phases of rehabilitation. There were no differences in muscle activity between healthy volunteers and patients with USP. Furthermore, different conditions, such as speed and load, did not modify muscle excitation. Adapted lawnmower exercise is an alternative to the preservation of motor and/or sporting gestures after surgery.
Footnotes
Acknowledgements
The authors thank all participants for their contribution to this study and Carolina Ten for their contribution language help.
Contributorship
LI was responsible for study conception, design, data acquisition, analysis, and interpretation, and drafted the article. IL, IR and CM were involved in study design, data acquisition and interpretation. IL was involved in study design and data interpretation. AWB and DJM were involved in data analysis and interpretation. All authors provided critical revision and approval of the final article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Instituto Universitario Italiano de Rosario (number 19/18).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
LI.
Informed consent
Yes.