
Abstract
Background
As no consensus exists on the optimal postoperative rehabilitation protocol in terrible triad injuries, we sought to characterize the reported protocols and relate them to postoperative range of motion (ROM) measures and Mayo Elbow Performance Score (MEPS).
Methods
A systematic review was performed by searching PubMed/MEDLINE, Embase, Web of Science, and Cochrane databases to identify articles on the operative treatment of terrible triad injuries reporting postoperative rehabilitation protocols were included. Included studies were descriptively summarized. Methodologic quality was assessed using the Methodological Index for Non-randomized Studies criteria. Meta-analysis compared postoperative ROM measures and the MEPS between patients initiating passive ROM exercises at ≤7 days vs. >7 days.
Results
Our review included 36 articles with 1123 elbows (66% male, mean age: 43 years, follow-up: 27 months). Of the studies reporting physical therapy protocols, it was most commonly initiated at 7 days postoperatively (6/36, 17%), passive ROM exercises at 7 days (3/25, 12%), and active ROM at 21 days (4/26, 15%). On meta-analysis, early passive ROM initiation was not associated with improved elbow ROM or MEPS.
Discussion
While rehabilitation protocols commonly advised passive ROM at one week post-operatively, meta-analysis did not support functional benefits of early passive ROM.
Study design
Systematic Review; Level of evidence, 4.
Keywords
Introduction
Terrible triad injuries are characterized by radial head or neck fracture, coronoid fracture, and concurrent elbow dislocation.
1
Injury occurs secondary to a combination of valgus, axial, and posterolateral rotary forces typically after a fall onto an outstretched hand that results in posterolateral humeroulnar dislocation.
2
This dislocation can cause abnormal forces on the coronoid process, radial head, olecranon, and/or collateral ligaments, which can lead to fractures and ligament injuries.
3
The bony and ligamentous disruption results in instability that routinely requires operative fixation or reconstruction to restore stability and function to the elbow.
4
Fixation of terrible triad injuries that are severe enough to warrant surgery involves stepwise repair or fixation of all injured structures including the lateral and/or medial collateral ligaments, the radial head or neck, and the coronoid process/anterior capsule.
5
Elbow stiffness, the loss of range of motion (ROM) typically below 100° in functional flexion-extension arc and rotational arc, has been reported to occur in up to 27% of patients after surgical fixation of terrible triad injuries
Despite the established benefit of rehabilitation in the postoperative course of terrible triad injuries, there is no consensus regarding the optimal protocol.9,10 Earlier ROM and shorter immobilization times have been suggested to decrease stiffness and improve function, however, specific regimens are sparse.11–13 While some literature recommends limiting immobilization and immediately beginning passive ROM exercises to limit the risk of elbow stiffness,3,12,14–16 others recommend immobilizing and delaying ROM for up to six weeks to ensure adequate fixation and to prevent recurrent instability.17–19 These differences in postoperative protocols may be a product of the variable need to ensure elbow stability and also heterogeneous level of detail in the reporting of rehabilitative milestones.18,20 This makes it difficult to create precise, evidence-based rehabilitation guidelines for surgeons to reference when educating patients on postoperative rehabilitation. Before a consensus regarding the optimal rehabilitation protocol can be reached, a comprehensive review of the literature is needed to inform future studies.
The purpose of this systematic review was to identify reported practices and highlight common trends in rehabilitation strategies, such as time to remove all restrictions and non-weight bearing (NWB) restrictions, active and passive ROM commencement, introduction of strengthening, physical therapy (PT) delivery modality, and immobilization duration after operative treatment of terrible triad injuries. Secondarily, we aimed to determine whether initiation of early passive ROM exercises was associated with improved elbow ROM, a quantitative measure to account for the common complication of elbow stiffness, or Mayo Elbow Performance Score (MEPS), the most commonly reported outcome measure in terrible triad injuries. 21 We hypothesized that there would be wide variation among rehabilitation regimens after operatively managed terrible triad injuries but an overall predilection for earlier ROM and strengthening exercises and shorter duration of immobilization. This information will be useful for researchers, orthopaedic surgeons, and physical therapists when deciding which protocols should be included in a postoperative rehabilitation strategy of terrible triad patients and will help facilitate future cross-study comparison.
Materials and methods
This systematic review was conducted under the guidelines set by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocols criteria. 22
Eligibility criteria
We included original studies reporting outcomes in patients with terrible triad elbow injuries managed operatively. Studies were excluded for the following indications: duplicate, non-English text, abstract only, review or meta-analysis, fewer than five patients, commentary or editorial, biomechanical or cadaveric study, studies including patients only treated nonoperatively, or if therapy protocols were not reported (Figure 1). Studies were not excluded in the overall screening if they were lacking ROM or outcome measures as long as the study still included rehabilitation protocols, but meta-analysis was performed on only studies that reported these outcomes.
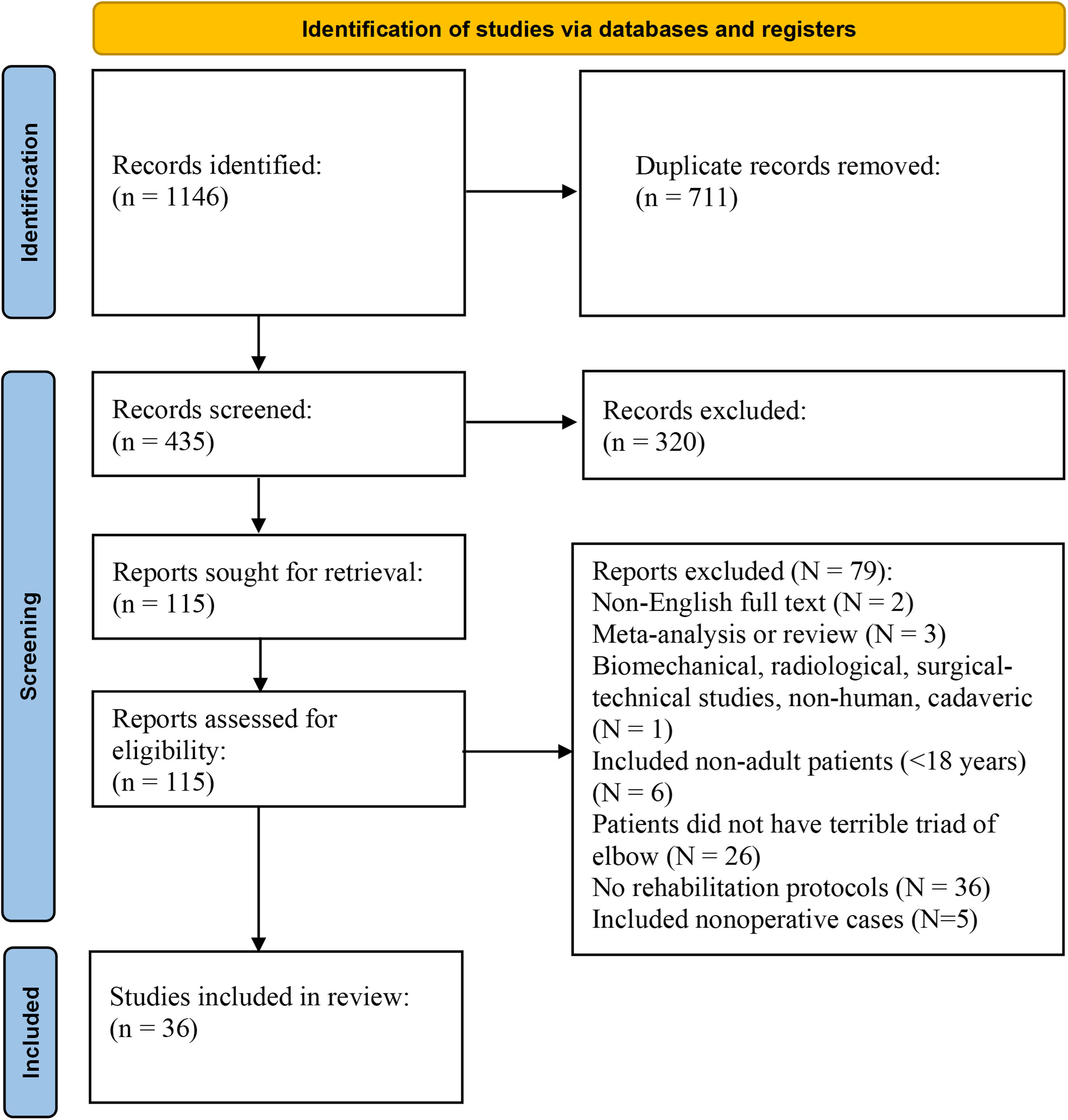
PRISMA flowchart of the study selection criteria.
Search strategy
PubMed/MEDLINE, Embase, Web of Science, and Cochrane Database, were searched in November 2022, including all articles since January 2010, a date set to include only recent literature, that assessed elbow fracture-dislocations. The search strategy included: (“terrible triad” OR “terrible-triad” OR “posterolateral rotatory”) OR (“elbow” OR “ulna*” OR “radi*”) OR (“fracture dislocation*” OR “fracture-dislocation*”). Articles were first screened by title and abstract for eligibility by multiple authors (J.L., K.M.H., L.W.). Authors included articles in the study if the inclusion eligibility was questionable. Subsequent full text screening was conducted by multiple authors (J.L., K.M.H., L.W., M.Q.B., R.L.J., and T.R.B.). A panel of senior shoulder and elbow surgeons provided expert opinion for any discrepancies.
Data extraction
Using a standardized data-collection form, data extraction was performed by three authors (R.L.J, M.Q.B., and T.R.B.). Several demographic variables were collected during the full-text review process, including country of origin, level of evidence, total number of patients and elbows, mean follow-up time, mean patient age, and proportion of females. Rehabilitation characteristics extracted included time for non-weight bearing status on the upper extremity (defined as an explicitly stated weight bearing restriction and separated from removal of all activity restrictions), time until full active or unlimited ROM, time to start passive and active ROM, time to start elbow strengthening exercises, time to start no restrictions, and whether a home exercise program was included postoperatively. To evaluate whether early passive motion was associated with reduced limitations in postoperative ROM and outcomes, we extracted elbow flexion, extension, flexion/extension arc, pronation, supination, and pronation/supination arc at final follow-up and the MEPS. 23 Methodologic quality of included non-randomized studies was assessed using the methodological index for non-randomized studies (MINORS) criteria. 24
Statistical analysis
Study characteristics were summarized descriptively. Weighted means, based on the number of elbows in each study, were calculated for study demographics and rehabilitation protocol characteristics of interest. Studies that involved injuries being managed with different strategies (e.g., nonoperative and operative cohorts) that utilized different post-injury rehabilitation protocols in each treatment group were recorded as separate cohorts. Weighted means and summary statistics were calculated for patient cohort demographics and rehabilitation protocol characteristics overall and stratified by injury management. Towards our secondary aim, meta-analysis was performed to compare postoperative elbow flexion, extension, flexion/extension arc, pronation, supination, and pronation/supination arc based on early versus late (≤7 days vs. >7 days postoperatively, respectively) initiation of passive ROM exercises. This cutoff was selected post-hoc based on an observed mode of studies reporting initiation of multiple aspects of rehabilitation at 7 days postoperatively. For these meta-analyses, studies included in the systematic review lacking either reporting of time to passive ROM initiation or the outcome of interest were excluded from the applicable meta-analysis. We anticipated that the design of the included studies and methodology involved in data collection would result in substantial heterogeneity; thus, we elected to use a random-effects model a priori. 25 The I2 statistic was used to assess the heterogeneity of results. The true effect size in 95% of the population (95% prediction interval) was calculated using the variance of true effects (T2) and the standard deviation of true effects (T). Meta-analysis was performed using the metafor package. 26 All statistical analyses were performed in R software (version 4.2.0, R Core Team, Vienna, Austria) with two-sided testing and an α = .05.
Results
Search results
Our search strategy returned 1146 publications, of which 435 were found to be unique following duplicate exclusion (Figure 1). We additionally excluded 320 articles during title and abstract screening, leaving 115 articles for full-text review. During full-text screening, 36 unique articles were found to meet inclusion criteria and were included.8,10,15,16,27–58 The average MINORS score for comparative studies was 22/24 and for non-comparative studies was 12/16. See Supplementary Table I for individual study characteristics and Supplementary Table II MINORS scores.
Study characteristics
The senior author on most included studies was from China in 14/36 (39%) studies. The most common continents were Asia in 19/36 (53%) studies, Europe in 6/36 (17%) studies, and South America in 5/36 (14%) studies. The studies consisted of 1/36 (2.8%) randomized controlled trial, 2/36 (5.6%) prospective case series studies, 4/36 (11%) retrospective cohort studies, and 29/36 (81%) retrospective case series studies.
Patient characteristics
A total of 1123 elbows were included, 34% of the patients were female, and the weighted mean age was 43 years old with follow-up of 30 months. Minimum follow-up ranged from 3–110 months.
Non-weight bearing
Time spent with strict NWB on the upper extremity was specifically reported for 1/36 (2.8%) studies, with a time of 42 days (Figure 2A) (Table 1).
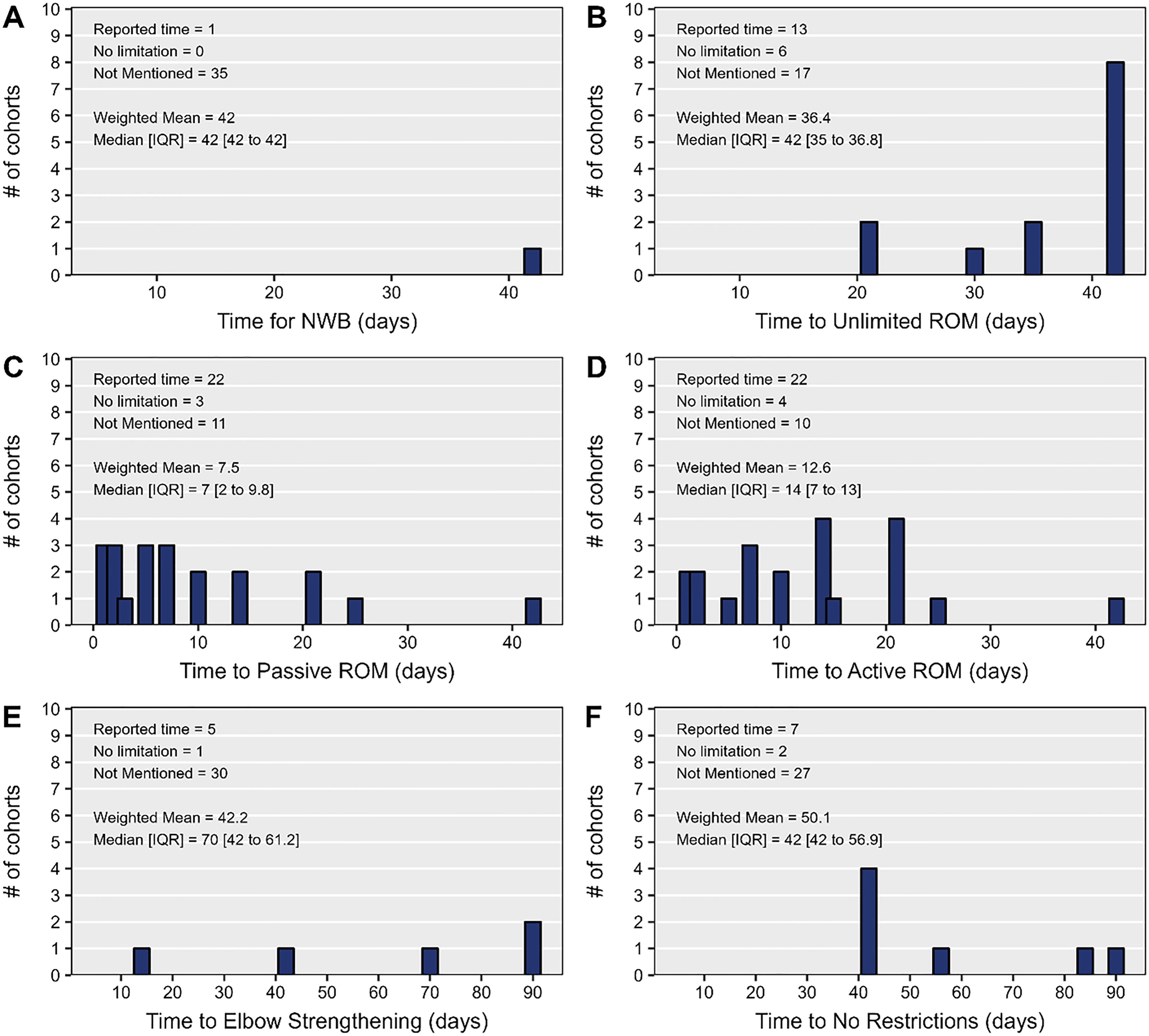
(A) time for non-weight bearing (NWB) status, (B) time to unlimited or full active range of motion (ROM), (C) time to passive ROM, (D) time to active ROM, (E) time to elbow strengthening, (F) time to no restrictions.
Most commonly reported timing of implementing rehabilitation characteristics.
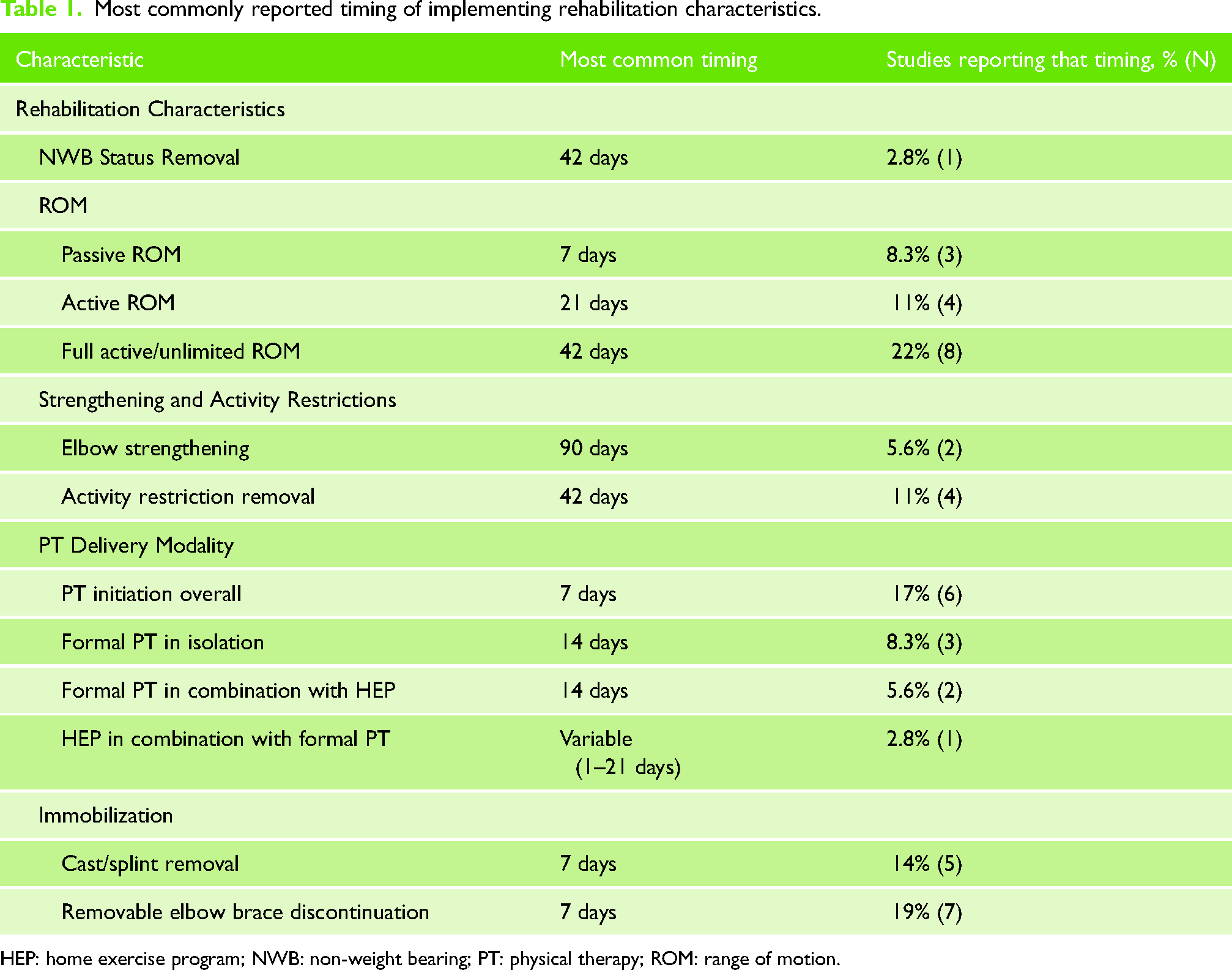
HEP: home exercise program; NWB: non-weight bearing; PT: physical therapy; ROM: range of motion.
Range of motion
Time to start passive ROM was reported for 24/36 (67%) studies (Figure 2C). The most commonly reported time to start passive ROM was 7 days (8.3%, n = 3) (Table 1), but varied from 1-day post-intervention (8.3%, n = 3) to 42 days (2.8%, n = 1). The overall weighted mean was 7.5 days. Meta-analysis showed no effect of initiation of early (i.e., within postoperative day seven) passive ROM exercises on postoperative ROM measures (Figures 3 and 4) or the MEPS (Figure 5) evaluated at latest follow-up.
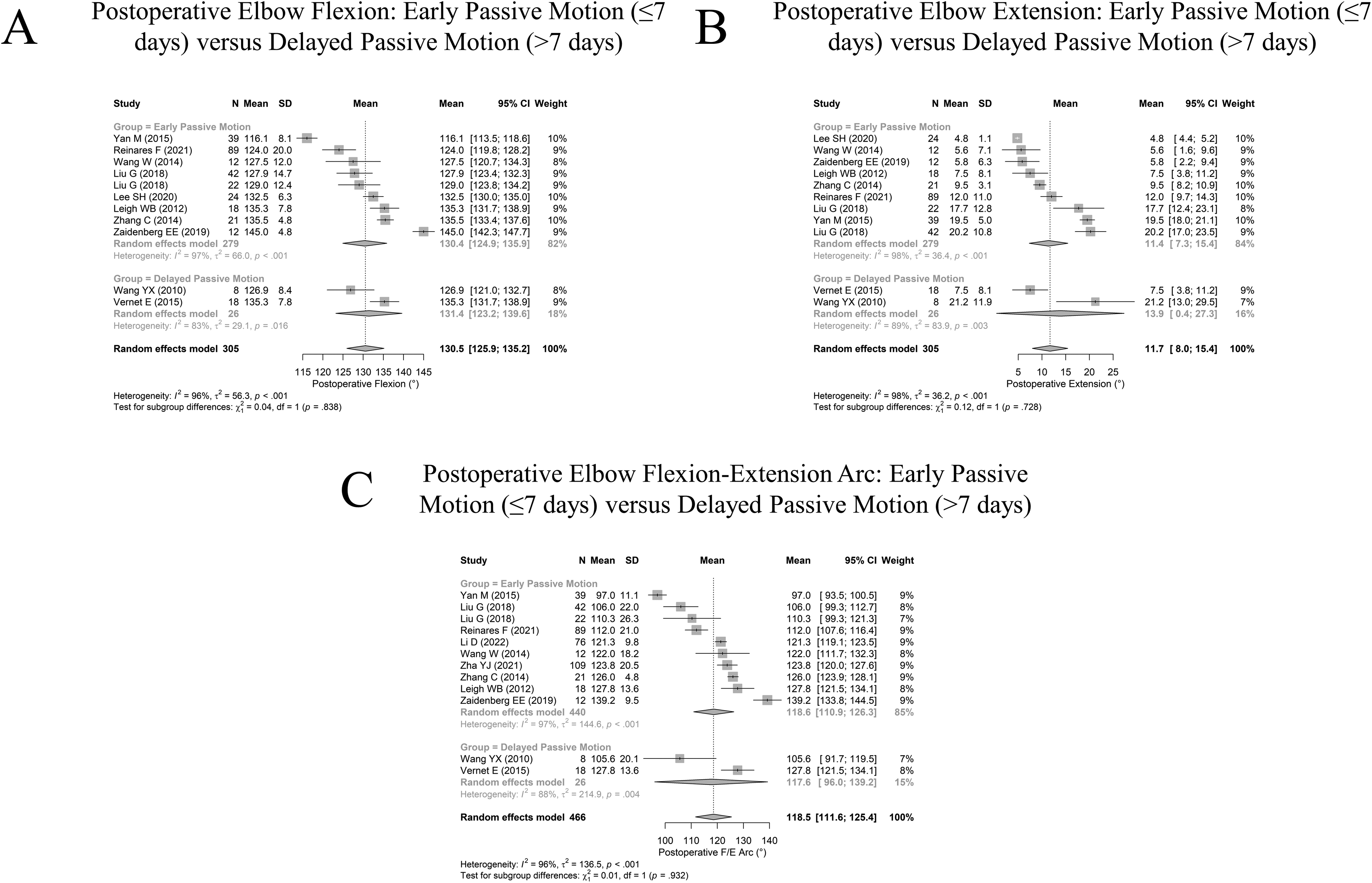
Comparison of postoperative range of motion measures based on early (≤7 days) versus late (>7 days) initiation of passive motion exercises (A) elbow flexion, (B) elbow extension, (C) elbow flexion-extension arc.
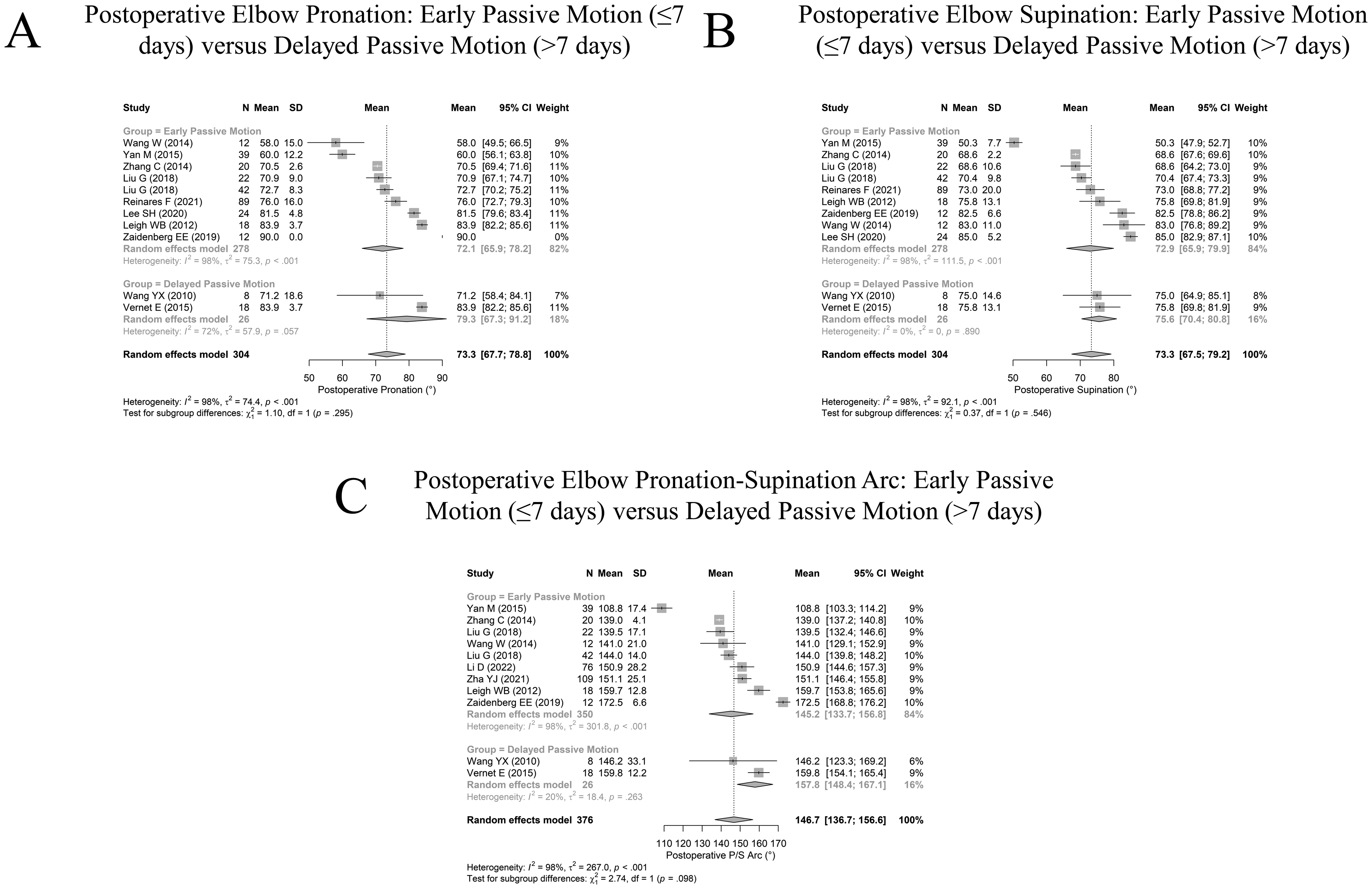
Comparison of postoperative range of motion measures based on early (≤7 days) versus late (>7 days) initiation of passive motion exercises (A) elbow pronation, (B) elbow supination, (C) elbow pronation-supination arc.
Time to start active ROM was reported for 25/36 (79%) studies (Figure 2D). The most commonly reported time to start active ROM was 21 days (11%, n = 4) (Table 1), but varied from 1-day post-intervention (5.6%, n = 2) to 42 days (2.8%, n = 1). The overall weighted mean was 12.6 days.
Time to start full active or unlimited ROM was reported for 19/36 (53%) studies, with 6 studies reporting no standardized limitations to reaching this milestone (Figure 2B). The most commonly reported time to start full active or unlimited ROM was 42 days (22%, n = 8) (Table 1), and varied from 21 days post-intervention (5.6%, n = 2) to 42 days (22%, n = 8). The overall weighted mean was 36.4 days.
Strengthening and activity restrictions
Time to start strengthening was reported for 6/36 (17%) studies (Figure 2E). The most commonly reported time to start strengthening was 90 days (5.6%, n = 2) (Table 1), but varied from 14 days post-intervention (2.8%, n = 1) to 90 days (5.6%, n = 2). The overall weighted mean was 42.2 days.
Time to remove all restrictions was reported for 9/36 (25%) studies (Figure 2F). The most commonly reported time to restriction removal was 42 days (11%, n = 4) (Table 1), but varied from 42 days post-intervention (11%, n = 4) to 90 days (2.8%, n = 1). The overall weighted mean was 50.1 days.
Physical therapy
Time to start PT was reported for 36/36 (100%) studies (Figure 6A). The most commonly reported time to start PT was 7 days (17%, n = 6) (Table 1), but varied from 1-day post-intervention (11%, n = 4) to 23 days (2.8%, n = 1). The overall weighted mean was 8.3 days.
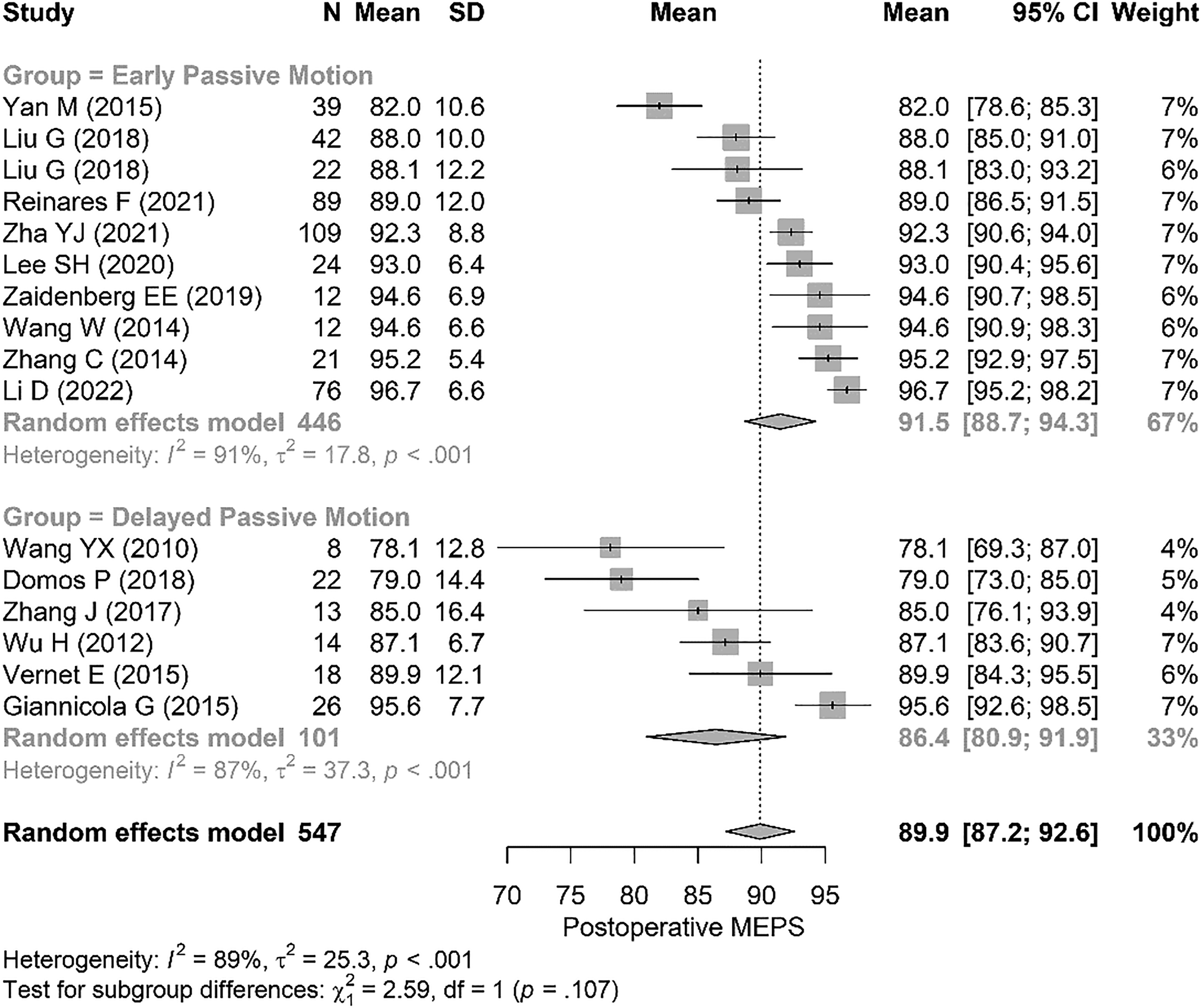
Comparison of postoperative Mayo elbow performance scores (MEPS) 23 based on early (≤7 days) versus late (>7 days) initiation of passive motion exercises.
We found two reported PT delivery modalities, formal PT used in isolation and a combination of formal PT and a home exercise program (HEP). The combination approach was further stratified by which modality was initiated first, formal PT or HEP.
Time to start formal PT used in isolation was reported for 14/36 (39%) studies (Figure 6B). The most commonly reported time to start formal PT in isolation was 14 days (8.3%, n = 3) (Table 1), but varied from 1-day post-intervention (2.8%, n = 1) to 28 days (2.8%, n = 1). The overall weighted mean was 12.2 days.
Time to start the formal PT component when used in combination with HEP was reported for 4/36 (11%) studies (Figure 6C). The most commonly reported time to start this aspect of PT was 14 days (5.6%, n = 2) (Table 1), but varied from 5 days post-intervention (2.8%, n = 1) to 18 days (2.8%, n = 1). The overall weighted mean was 12.6 days.
Time to start the HEP component when used in combination with formal PT was reported for 4/36 (11%) studies (Figure 6D). Each study reported a different time to start this aspect of PT, with varied times from 1-day post-intervention (2.8%, n = 1) to 21 days (2.8%, n = 1) (Table 1). The overall weighted mean was 8.3 days.
Immobilization
Time spent with the upper extremity immobilized in a cast or splint was reported for 23/36 (64%) studies (Figure 7A). The most commonly reported time spent immobilized was 7 days (14%, n = 5), but varied from one day (5.6%, n = 2) to 28 days (2.8%, n = 1) (Table 1). The overall weighted mean time was 11.2 days.
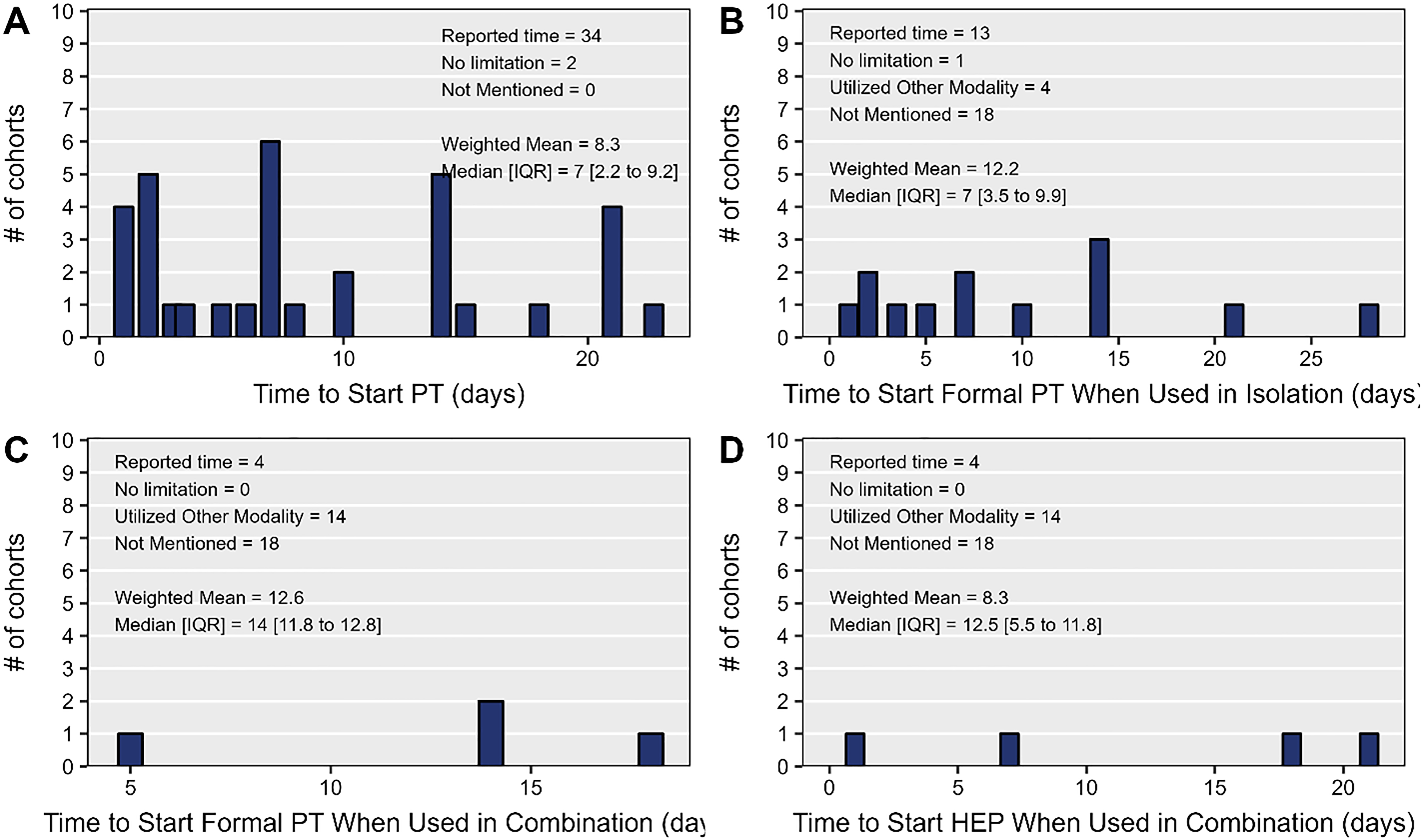
(A) Time to start physical therapy (PT), (B) time to start formal PT when used in isolation, (C) time to start formal PT when used in combination with a home exercise program (HEP), (D) time to start HEP when used in combination with formal PT.
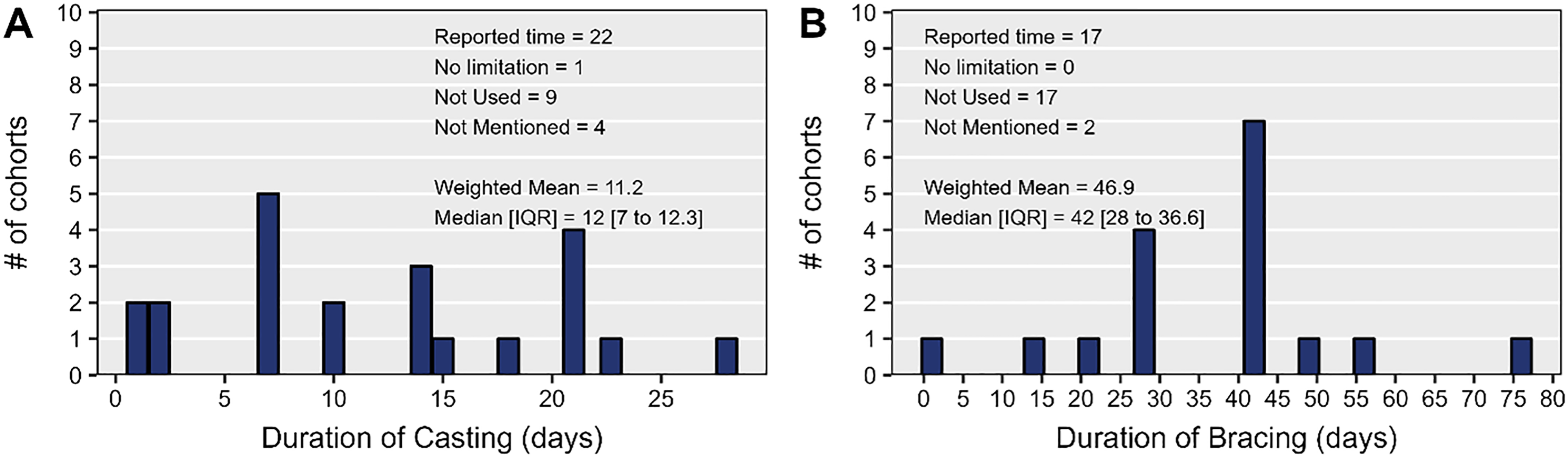
(A) Time spent in a cast or splint. (B) Time spent in a brace.
Time spent with the upper extremity in a removable elbow brace was reported for 17/36 (47%) studies (Figure 7B). The most commonly reported time spent braced was 42 days (19%, n = 7) (Table 1), but varied from one day (2.8%, n = 1) to 76 days (2.8%, n = 1). The overall weighted mean time was 46.9 days.
Discussion
There is a great deal of heterogeneity in the implementation and reporting of rehabilitation protocols used in the postoperative management of terrible triad injuries of the elbow. The purpose of this systematic review was to report the most commonly used rehabilitation strategies documented in the literature, with the goal of ultimately facilitating more standardized reporting of rehabilitation strategies. Passive ROM exercises were mostly initiated at one week postoperatively, active ROM at three weeks, and unrestricted ROM at six weeks. Initiation of early passive ROM within one week postoperatively did not confer a functional benefit in this meta-analysis. Immobilization in a cast/splint was most commonly discontinued at one week postoperatively, with PT most commonly beginning thereafter. Removable bracing was most commonly discontinued at six weeks, which coincided with the most common timing of strengthening initiation. Reporting of these rehabilitation characteristics was highly variable and was commonly omitted in the reviewed articles.
In this study, we found that the most reported rehabilitation protocol characteristic was time to active ROM (70%) followed by passive ROM (68%), unlimited ROM (51%), no restrictions (24%), and elbow strengthening (14%) (Figure 2). The most reported PT delivery modality included was formal PT (97%), with 38% reporting an isolated formal PT approach and 11% reporting a combination of formal PT and HEP (Figure 6). Sixty-five percent of studies reported a period of postoperative casting, and 52% of studies reported a period of postoperative bracing (Figure 7). These aspects of postoperative rehabilitation being reported more consistently would allow for improved investigation and possible improvement of rehabilitation protocol recommendations. For example, 97% of studies herein reported utilizing formal PT during the course of rehabilitation, and this PT delivery modality has been reported as the modality of the highest efficacy compared to HEP alone.59,60
Progression of elbow ROM milestones varied considerably among the included studies signifying heterogeneity among postoperative ROM protocols. Time to allow for passive ROM had an overall weighted mean time of 7.5 days, which ranged from 1 to 42 days (Figure 2C). Active ROM was slightly delayed with a weighted mean time of 12.6 days, ranging from 1 to 42 days (Figure 2D). Five included studies reported no limitations in ROM;30,39,40,47,53 however, the average time to remove ROM restrictions was 36.4 days, ranging from 3 to 6 weeks post intervention in our study (Figure 2B). A prior systematic review by de Haan et al. 61 analyzed outcomes after simple elbow dislocation and found earlier return to work and more rapid return of functional motion with early initiation of ROM exercises. While early motion may be beneficial in simple elbow dislocations, extrapolation is required to apply this to unstable elbow fractures. A systematic review by Harding et al. 62 analyzed early mobilization after operatively and non-operatively managed simple elbow fractures. The authors found a non-significant trend between early motion and improved post-intervention ROM with no adverse effects compared to prolonged immobilization. Contrarily, when studying outcomes after surgical treatment of complex elbow instability, Giannicola et al. 63 recommended an early rehabilitation program as they found the initial six months to be the critical period for rehabilitation, as rate of improvements in ROM diminished after this period. Early motion after operative treatment of terrible triad injury should be considered to prevent stiffness and possibly improve functional outcomes; however, specific timing of passive, active, and removal of ROM restrictions warrants further study.
To this end, regarding postoperative elbow ROM and MEPS values, we found no significant benefit to early versus late initiation of ROM exercises. This is a similar finding to that reported by Kamel et al. 13 who investigated the endpoint MEPS in studies initiating mobilization exercises early or late in the postoperative course. Of note, these authors defined early versus late mobilization by the initiation of active ROM exercises before or after 14 days postoperatively while the protocol herein utilized the initiation of passive ROM exercises before or after 7 days postoperatively. Kamel et al. 13 found a statistically significant, but not clinically significant, improvement in functional outcomes with early postoperative mobilization, while we found no such significant improvements. Thus, in light of the aforementioned prior findings of improved ROM with earlier mobilization, an investigation of a higher level of evidence would be necessary to guide future practice guidelines in this space.13,62,63
PT along with other modalities, such as bracing and manual mobilization, have been proposed for the treatment and prevention of complications such as stiffness and heterotopic ossification after trauma.64–67 After terrible triad injury, PT is routinely utilized to guide rehabilitation efforts and achieve the most robust outcome. Though some providers prescribe a HEP without formal guidance, multiple studies have found improved pain, ROM, and patient-reported outcome measures with formal PT when compared to an unsupervised HEP.59,60 When analyzing formal PT, a survey on rehabilitation practice patterns after elbow fracture by physical therapists found strong homogeneity in modalities utilized. 68 In the acute phase, defined as the first six weeks after elbow fracture, active ROM was utilized by 86% of therapists; whereas in the functional phase, defined as 6–12 weeks, 99% utilized active ROM activities in addition to strengthening and functional activities in 97%. Thus, a high percentage of physical therapists utilize early ROM exercises, which, when examined in conjunction with the findings of other studies, could minimize elbow stiffness.3,11,12,14–16
Immobilization duration after surgical management of terrible triad injuries must balance maintenance of bony fixation while minimizing scar tissue formation which could ultimately lead to limitations in elbow ROM. Myden & Hildebrand 69 found a 12% incidence of elbow joint contracture requiring surgical intervention after traumatic elbow injury. This risk is likely higher with prolonged immobilization due to proliferation of fibroblasts and scarring.70,71 In various synovial joints, including elbows, wrists, fingers, hips, knees, and ankles, early mobilization has been shown to be superior to immobilization in terms of outcomes in postoperative and conservatively managed injuries.71–75 The FuncSiE trial was a multicenter randomized controlled trial that evaluated 100 patients with simple elbow dislocations and randomized to early mobilization versus three weeks plaster immobilization after reduction. 76 They found that patients who began early mobilization had faster return to work, higher functional scores using the Quick-Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) score, 77 and larger arc of motion at six weeks without increased complication risk; however, despite these early benefits there were no long-term advantages at one year. Other studies have found similar findings but none looking specifically at complex elbow fracture dislocations.61,65,71 While early mobilization shows clear benefit in other settings, further investigation is needed to determine the extent of immobilization time required postoperatively for complex elbow fractures.
To enable cross-study comparison of terrible triad treatment outcomes, more consistent postoperative protocol reporting is required. Key protocol points include the delivery modality, immobilization time, time to initiate ROM exercises of varying types (passive, active, and removal of ROM-based restrictions), and time to initiate strengthening. Standardizing the reporting of these rehabilitation protocol characteristics may enable future studies to determine how surgeons can improve the reproducibility of patient outcomes after operative management of terrible triad elbow injuries and may also facilitate cross-study comparison.
It is important to consider the limitations of this review. To achieve the most comprehensive and robust review we decided not to set a minimum level of evidence and 34/36 included studies were Level III and IV evidence with only one study being Level I quality. This unfortunately lessens the quality of the systematic review, but also enlightens the paucity of evidence in the literature. There is a possibility that some pertinent articles were missed in our review despite extensive review across multiple databases. As with all systematic reviews, there is a risk of publication bias and compounded reporting bias, especially given the high number of retrospective studies. It is likely that many studies varied in reporting or timing of rehabilitation milestones due to differences in follow-up timing rather than true differences, in protocol. It is also possible that differences in surgical approach, health care systems, and patient populations could have contributed to the observed heterogeneity. Therefore, future studies are needed to compare outcomes in treatment cohorts to establish more standardized rehabilitation protocols.
Rehabilitation strategies after terrible triad elbow fracture dislocation have been widely debated especially regarding early mobilization for decreasing stiffness versus delayed mobilization to allow adequate time for fracture and ligamentous healing. Examining the influence of rehabilitation protocol characteristics, such as timing of ROM, strengthening, physical therapy, and immobilization duration, may help to standardize and improve treatment of terrible triad injuries; however, there is substantial heterogeneity in reporting of postoperative rehabilitation protocols. Importantly, PT was most commonly begun at one week postoperatively, at which time immobilization devices were removed and ROM exercises were initiated. More, high-level evidence is needed to ensure safety of early initiation of passive ROM, especially given the fact that our meta-analysis found no significant difference in postoperative elbow ROM with early mobilization. Standardization of postoperative protocol reporting is needed in this challenging patient population and more research is needed to elucidate the most optimal rehabilitation regimen.
Supplemental Material
sj-docx-1-sel-10.1177_17585732241269807 - Supplemental material for Characteristics of rehabilitation protocols following operative treatment of terrible triad elbow injuries and the influence of early motion: A systematic review and meta-analysis
Supplemental material, sj-docx-1-sel-10.1177_17585732241269807 for Characteristics of rehabilitation protocols following operative treatment of terrible triad elbow injuries and the influence of early motion: A systematic review and meta-analysis by Joseph Larwa, Timothy R Buchanan, Rachel L Janke, Madison Q Burns, Logan Wright, Kevin A Hao, Robert J Cueto, Keegan M Hones, William R Aibinder, Thomas W Wright, Bradley S Schoch and Joseph J King in Shoulder & Elbow
Supplemental Material
sj-docx-2-sel-10.1177_17585732241269807 - Supplemental material for Characteristics of rehabilitation protocols following operative treatment of terrible triad elbow injuries and the influence of early motion: A systematic review and meta-analysis
Supplemental material, sj-docx-2-sel-10.1177_17585732241269807 for Characteristics of rehabilitation protocols following operative treatment of terrible triad elbow injuries and the influence of early motion: A systematic review and meta-analysis by Joseph Larwa, Timothy R Buchanan, Rachel L Janke, Madison Q Burns, Logan Wright, Kevin A Hao, Robert J Cueto, Keegan M Hones, William R Aibinder, Thomas W Wright, Bradley S Schoch and Joseph J King in Shoulder & Elbow
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.A.H. has a consultancy agreement with LinkBio Corp. W.R.A. is a consultant for Exactech, Inc. T.W.W. is a paid consultant and receive royalties from Exactech, Inc. B.S.S. receives royalties from Exactech, Innomed and Responsive Arthroscopy. J.J.K. is a paid consultant for Exactech, Inc. and LinkBio Corp. The other authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.