
Abstract
Background
The aim of the study was to assess if 3D CT-scan-based planification of distal filling ratio (DFR) is accurate when compared to postoperative DFR calculated on plain X-rays. A secondary aim was to investigate if an association between clinical outcomes and the degree of stress shielding (SS) exists.
Methods
Fifty patients with short-stem reverse shoulder arthroplasties, preoperative CT scans, and a minimum 24-month radiographic follow-up were included in the study. At 24 months follow-up, all patients were evaluated by assessing the postoperative filling ratios, the 3D DFRs, the simple shoulder test, Constant-Murley score, and visual analogue scale through a prospectively data collection and statistically analyzed.
Results
A correlation between the 3D DFR and SS onset (rs 0.54; P < 0.001), and between postoperative DFR and SS (rs 0.71; P < 0.001), was found. The 3D DFR and the postoperative DFR were correlated (rs 0.89; P < 0.0001). SS negatively affects the postoperative range of motion, decreasing the forward elevation of the shoulder.
Conclusion
The calculation of DFR based on 3D CT planning is a good predictor of humeral SS after short-stem RTAs. The presence of SS decreases clinical outcomes by lowering the anterior elevation of the shoulder.
Level of evidence
Case series.
Introduction
Reverse shoulder arthroplasty (RSA) is a well-established and efficient treatment for end stage glenohumeral osteoarthritis, rotator cuff dysfunction, and cuff tear arthropathy. Over the next decades, along with the increased indications, an increasing number of revisions are expected. 1 Proximal humeral resorption is among the causes of primary RSA failure in the long term, 2 while aseptic loosening is one of the most common long-term complications of a humeral stem. 3 Uncemented short-stem shoulder arthroplasty has the advantage of bone preservation and potential easier revision surgery when compared to conventional cemented or uncemented stemmed prostheses, even if it is associated with high levels of stress shielding (SS).4,5 Generally, surgeons determine the size of the humeral stem based on intra-operative testing, looking for the best fit through internal and external rotation of the component, the so-called “Twist test”. However, using this test, the surgeon is unable to evaluate the relationship between the stem and the metaphysis, nor can they assess the distal filling ratio (DFR) accurately. Furthermore, while some studies have found a correlation between DFR calculated with the method described by Schnetzke et al. and SS. 6 only a few authors have investigated the accuracy of the DFR with automated measurement based on CT scans. 7 Although SS is a frequent radiological complication in the long term, 8 its role in terms of clinical outcomes or related complications is still debated.4,9
Literature shows how a reduced filling ratio (<70%) is associated with a reduced SS without compromising stem stability in the early to mid-term follow-up.10,11
The first purpose of this study was to validate an automated measurement of the DFR based on CT-scan planification and its relation to the onset of SS. The second purpose of this study was to evaluate the role of the SS in terms of clinical outcomes at 2 years minimum follow-up after short-stem RSA. The hypotheses were that modern CT-scan-based measurements for DFR are accurate and that there would be no difference in functional outcomes between patients with or without SS.
Materials and methods
From March 2020 to September 2021, patients who underwent RSA with a short-stemmed implant were selected to participate to the present retrospective cohort study with 2-year follow-up. Preoperative and intra-operative data were collected retrospectively, while postoperative data were collected prospectively. Inclusion criteria were: (a) primary procedure using a humeral stem with metaphyseal stability, (b) age > 18 years at the operation, and (c) minimum 2 years of clinical and radiological follow-up. Approval for this study was provided by the Campus Bio-Medico Ethical Committee (study no. GR7009). The exclusion criteria were as follows: revision surgery, infection, and fractures. Indications for surgery were eccentric cuff tear arthropathy, concentric osteoarthritis, or nonfunctional irreparable cuff tears.
Functional assessment and radiographic analysis
The whole cohort function and range of motion was evaluated at final follow-up by assessing the simple shoulder test (SST), the Constant-Murley score (CMS), and the visual analogue scale (VAS) scale for pain. All patients underwent a preoperative computed tomographic (CT) evaluation and postoperative radiologic evaluation at the final follow-up. Radiologic evaluation was also performed at 1, 3, 6, 12, and 24 months. Preoperative CT scans and immediate postoperative X-rays of all eligible patients were reviewed by one fellowship-trained shoulder surgeon (EF) and two orthopedic residents (PG and GP) to collect the predicted DFR (Figure 1) and the resulting DFR after surgery (Figure 2) 6 in DICOM (Digital Imaging and Communications in Medicine) format or using Horos (Pixmeo, Bernex, Switzerland). The predicted DFR refers to the DFR calculated using the 3D planning software based on the size of the stem implanted in the patient. In particular, at the time of the investigation, the 3D DFR (Figure 1) was evaluated using Blueprint Digital Platform (Stryker) to assess its reliability compared to the measurement obtained from postoperative radiographs (2D DFR) (Figure 2). In this phase, patients were excluded only if the software was unable to calculate the DFR, typically due to issues with the quality of the CT scan. On radiographs performed at final follow-up (24 months), the presence of humeral radiolucencies condensation lines, cortical thinning and osteopenia, and spot welds was evaluated and classified into humeral zones according to Nagles et al. 12 (Figure 3). The grade of SS was defined according to Celik et al. 13 and studied in relation to two different groups of patients: group A with DFR < 70% and group B with DFR ≥ 70% based on the X-ray postop. calculation. Humeral loosening was defined as a radiolucent line of 2 mm or greater in three or more contiguous zones.

Distal filling ratio (DFR) evaluation using the planning software. The predicted DFR was highlighted with a red circle.
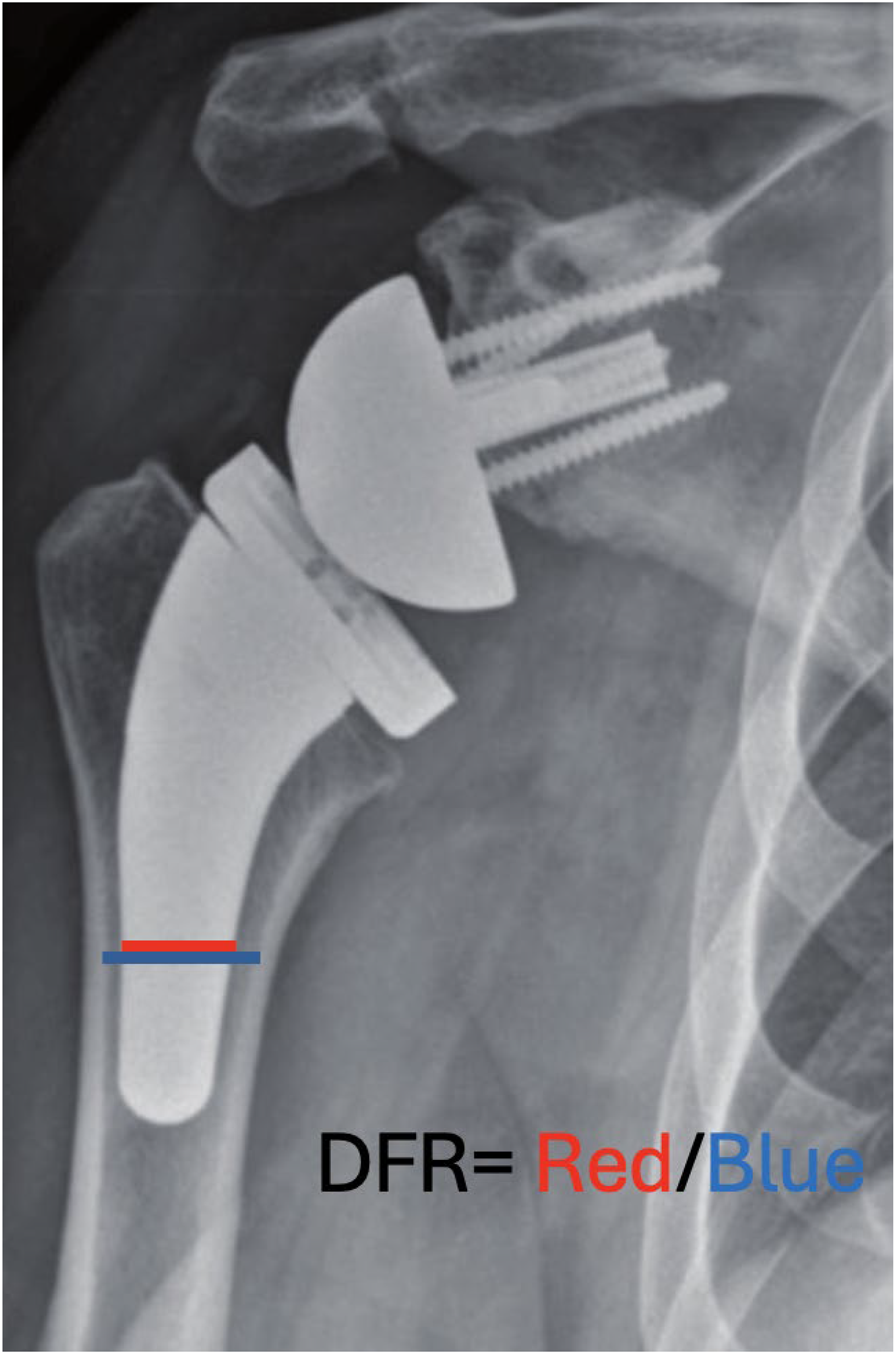
Distal filling ratio (DFR) calculation method on a postoperative X-ray. The result, coming from a millimeter measuring, is then converted to percentage (%).
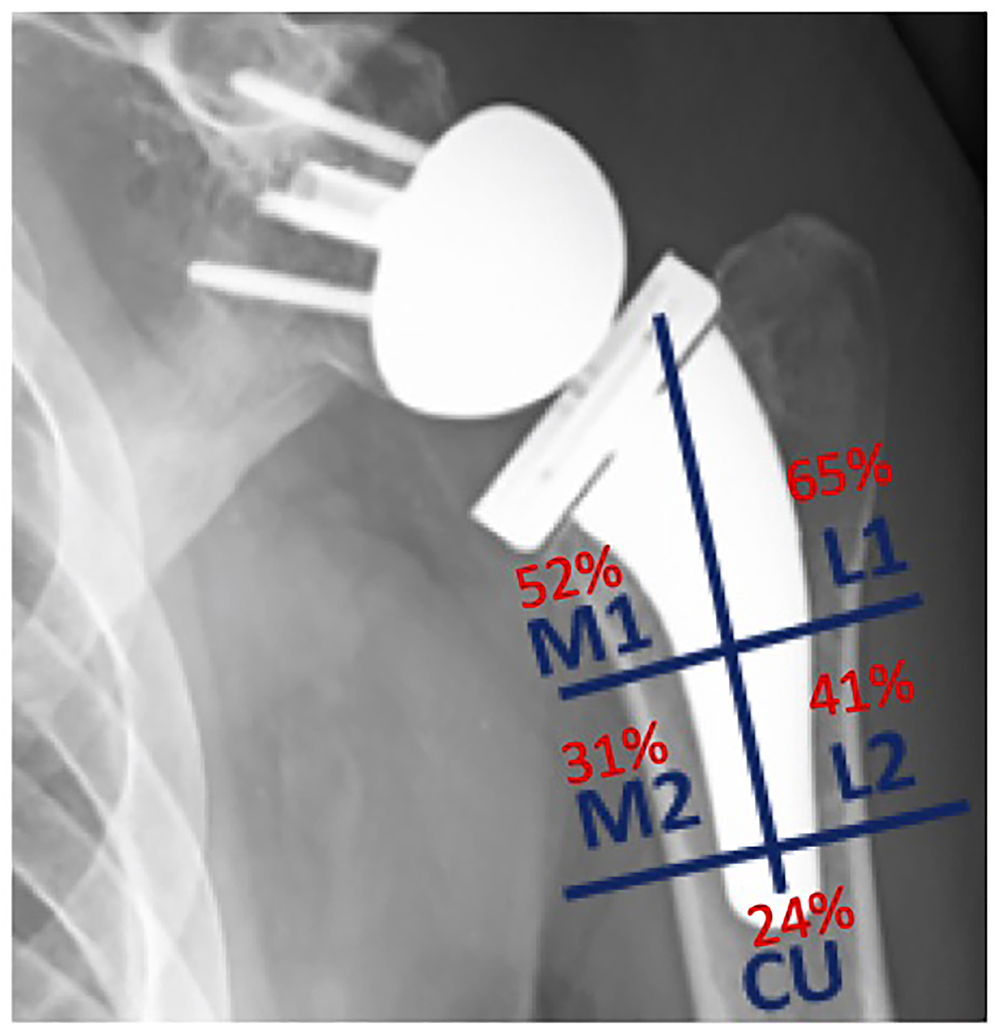
Distribution of stress shielding prevalence into zones according to Nagles et al.
Surgical technique and implant
All the surgeries were performed by two fellowship-trained senior surgeons (EF and RP). The type of prosthesis used was Tornier Aequalis Ascend Flex reverse prosthesis (Tornier, Houston, TX, USA). All patients were operated under general and loco-regional combined anesthesia. The operative procedure was conducted through a deltopectoral approach. A humeral stem with a neck shaft angle of 145° was used. The stem is available in eight different sizes. The Reverse II glenoid system was used for the glenoid and lateralized with a BIO-RSA technique according to Boileau et al.14,15 All patients followed the same postoperative rehabilitation program with the assistance of a specialized physiotherapist. Postoperatively, the shoulder was immobilized in a sling which was progressively discontinued after 4 weeks.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, Version 28.0. Differences were considered significant at the P < 0.050 level. Data of continuous variables were presented as mean values ± standard deviation (SD). Median values with inter-quartile ranges were provided for non-normally distributed variables. Analysis of variance (Student's t-test) for normally distributed variables was performed according to gender; otherwise, the nonparametric Mann–Whitney U H test was adopted. The two-tailed Fisher exact test was used for dichotomous variables.
The correlation between continuous variables was tested using the Spearman's rho correlation analysis. The inter-rater agreement on calculating the DFR was tested using the nonparametric Kendall's concordance coefficient W, while the intraclass correlation coefficient (ICC) was calculated to evaluate the intra-rater reliability.
Multivariable linear regression analyses were adopted to assess the association of SS and age, sex, and all those variables which differed significantly (P < 0.050) in univariate models, including both the planned, and postoperative DFR. Variables with abnormal distribution were analyzed after log transformation.
Eventually, the same multivariable linear model was adopted to test the possible association of SS with the Constant score, as well as the subitems of this scale.
Results
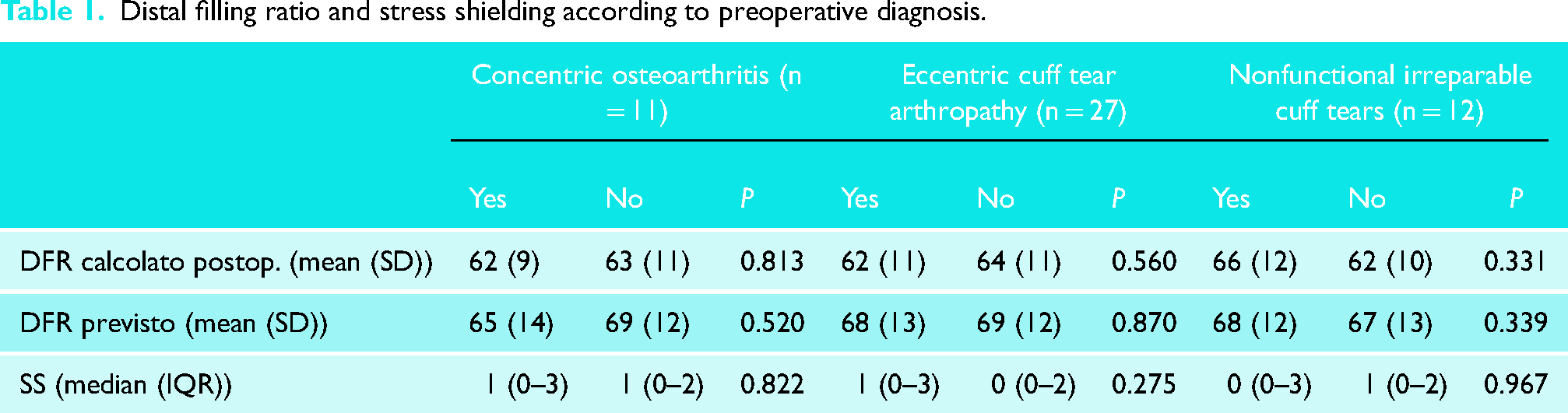
Sixty-five patients met the inclusion criteria. Two patients were excluded because the quality of the CT scan did not allow the software to extract the 3D DFR. Of the remaining patients, 50 completed the follow-up and represented our final cohort. There were 37 female (74%) and 13 male (26%) patients, with a mean age of 71 ± 10 years and a body mass index of 27.0 ± 3.4 kg/m2 for men and 73 ± 9 years a body mass index of 26.3 ± 5.4 kg/m2 for women. The median follow-up was 29.5 months (IQR 26–42). No surgical or medical complications were reported. There was a positive correlation between: the 3D DFR and 2D DFR (rs 0.89; P < 0.001), SS and the DFR 3D > 70% (rs 0.54; P < 0.001), and the correlation between the SS and the postoperative DFR > 70% (rs 0.71; P < 0.001). Also, there was a negative correlation of the SS and the postoperative total Constant score (rs −0.33; P = 0.018), as well as the subitem CS pain (rs −0.49; P = 0.002), CS mobility (rs −0.45; P = 0.006), CS DLA (rs −0.34; P = 0.042), and CS strength (rs −0.36; P = 0.029). No significant correlation was found between the SS and VAS pain and the SST, nor with age, BMI, or gender. Differences in DFR and SS according to preoperative diagnoses are showed in Table 1. There was a good concordance across raters (Kendal's W 0.83, P = 0.017). Also, the ICC score was 0.893, indicating excellent intra-reliability.
Distal filling ratio and stress shielding according to preoperative diagnosis.
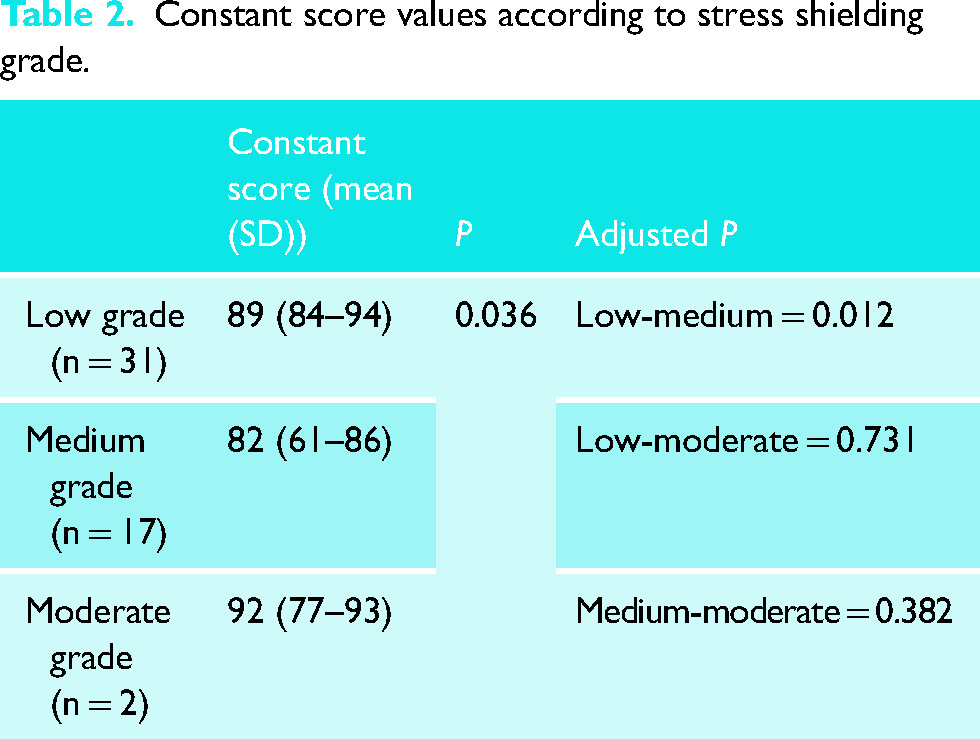
The Kruskal–Wallis test indicated a significant difference in the CS between the SS grades (Table 2); post hoc analysis showed only a difference between the low and the medium grade (Table 2).
Constant score values according to stress shielding grade.
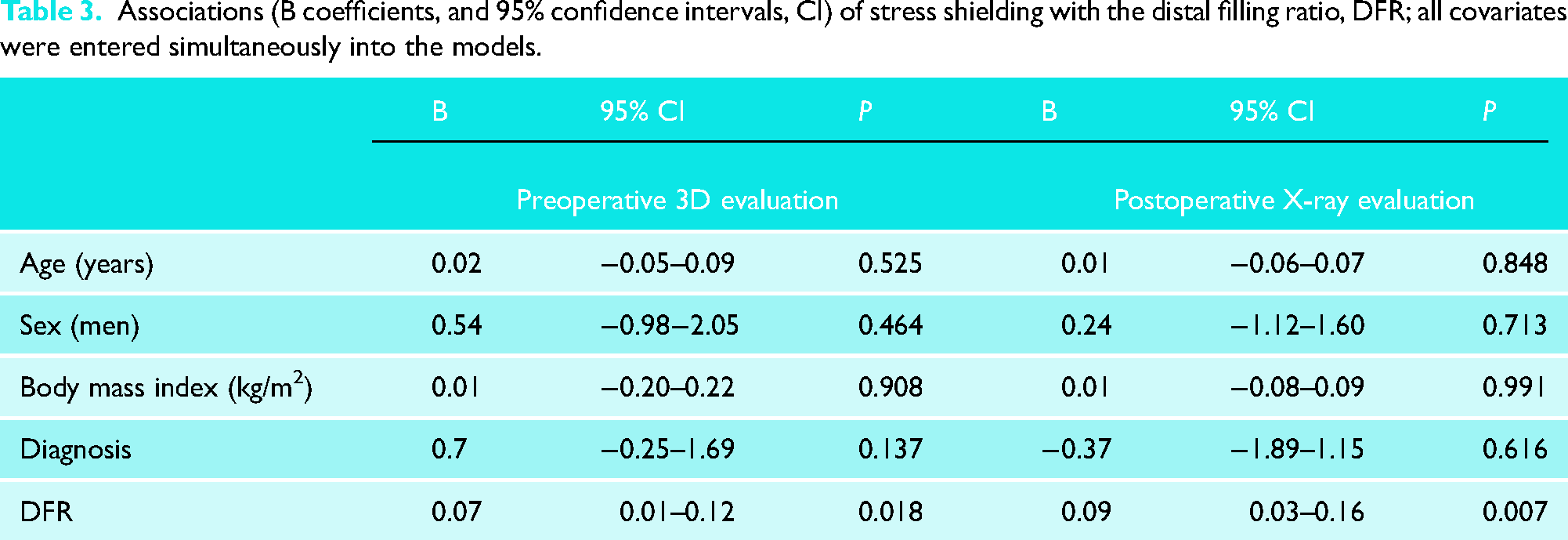
According to multivariable linear regression, there was a significant association between the SS and both the 3D DFR (B 0.07, 95% CI 0.01–.12; P = 0.018) and the X-ray DFR (B 0.09, 95% CI 0.03–.16; P = 0.007; Table 3), after adjusting.
Associations (B coefficients, and 95% confidence intervals, CI) of stress shielding with the distal filling ratio, DFR; all covariates were entered simultaneously into the models.
After stratifying patients for a DFR above or below the 70%, 28 patients were included in group A (3D DFR < 70%) while 22 patients were included in group B (3D DFR > 70%). Results of the distribution of the grade of SS indicated that all patients in group A had a low grade (i.e. 0–1), while 18 (82%) patients in group B had a medium SS (i.e. 2–3) and four (18%) subjects in group B had moderate SS (i.e. 4–6).
Humeral osteolysis was found in 45 patients (90%); radiolucencies condensation lines and spot welds were found in 17 (34%) and 17 (34%) patients, respectively. The resulted distribution of radiographical signs into radiographical zones is reported inFigure 3. Results of the adjusted association between SS and postoperative CMS, expressed as total score and subitems, are shown in Table 4. Specifically, there was a significant association between the SS and the constant score mobility (B −1.00, 95% CI −1.74 to −.26; P = 0.012).
Associations (B coefficients, and 95% confidence intervals, CI) of stress shielding with the constant score, and subitems according to multivariable linear regression models*; all covariates were entered simultaneously into each models.
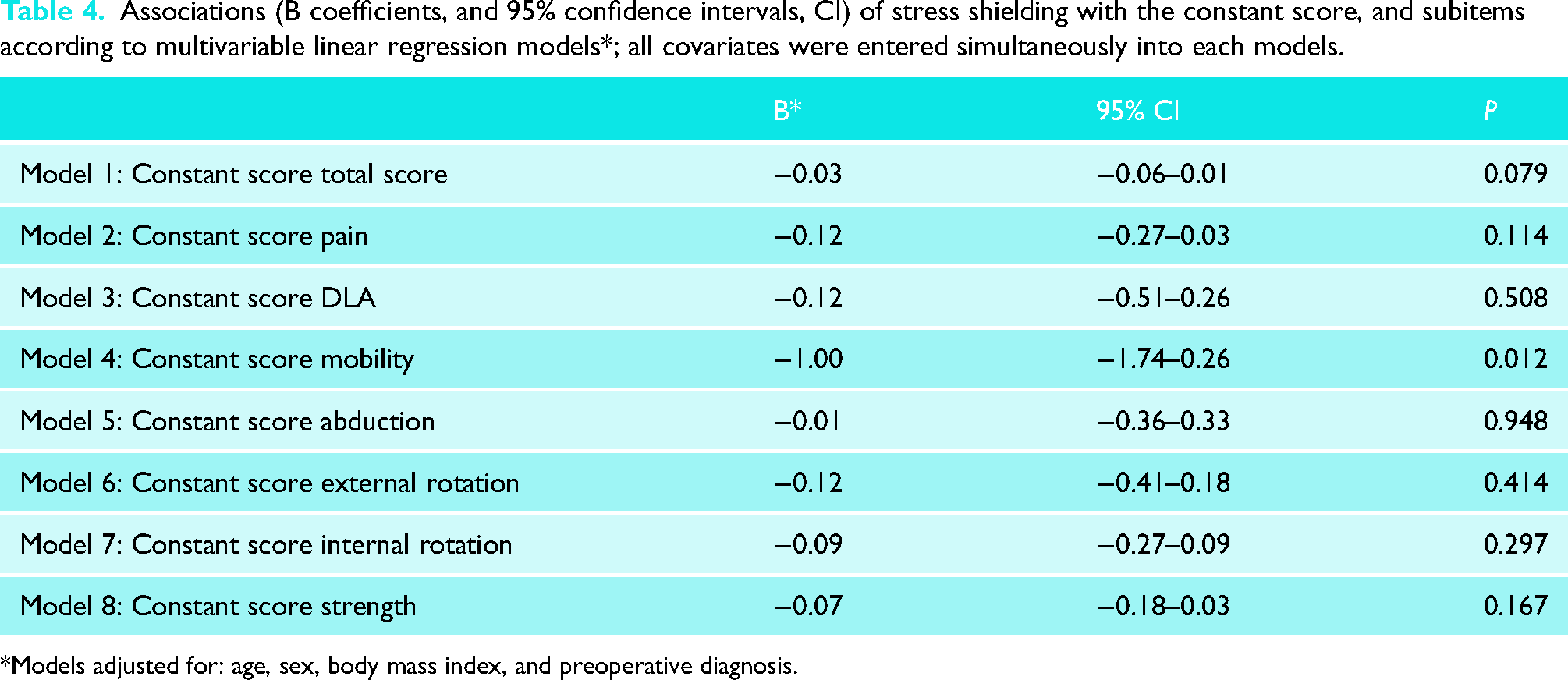
Models adjusted for: age, sex, body mass index, and preoperative diagnosis.
Discussion
The study aimed to evaluate the accuracy of the 3D CT-scan DFR measurements in relation to the postoperative X-ray 2D measurements. A second aim was to investigate an eventual association between SS and clinical outcomes at minimum 24 months follow-up after RSA with short press-fit stem. Our results support the first hypothesis, finding a significant association between 3D CT-scan and 2D DFR measurements. However, the second hypothesis was not confirmed since a significant association between SS and clinical outcomes at 24 months follow-up was found. No significant correlation was found between DFR and SS according to preoperative diagnosis. In the history of RSA, humeral stems have traditionally been cemented; however, one of the most common long-term complications observed is humeral loosening. 3 Bacle et al. 16 reported a 93% survival rate at 10 years follow-up in 86 RSAs with cemented humeral stem, but also found a significant decrease of Constant score between 5 and 10 years follow-up. These facts highlight that the bone preservation should be considered in order to reduce humeral loosening and increase clinical outcomes in the long term. The main finding of the present investigation is the resulted significant negative correlation between the SS and the Constant score mobility according to multivariable linear regression (B −1.00, 95% CI −1.74 to −.26; P = 0.012). This result defines SS not only as a radiological complication but also as a predisposing factor for inferior outcomes in the short term. Mazaleyrat et al. 9 compared two matched cohorts of 56 RSAs with cemented stems and 56 RSAs with press-fit stems with a mean follow-up 9.5 years finding no differences in the CMS between shoulders that underwent RSA with a cemented stem or a press-fit stem, although active ROM was significantly worse in the press-fit group than in the cemented group. They ascribe such results to the tuberosity resorption and signs of SS, more often present in the shoulders with press-fit stems. Even though their study did not include short metaphyseal press-fit stems, the discrepancy between clinical results could be due to the observed radiological complications, which focuses the discussion on preventing their onset in all the different type of stems.
On the contrary, King et al. 17 found no difference in term of outcomes or stem loosening between RSA with cemented humeral fixation and RSA with press-fit humeral fixation in a 2-year follow-up analysis. However, they used a different type of stem (long) and did not stratify their results for every point of the Constant score, where we found significant negative correlation with SS. Another limitation is the lack of randomization between cementation and press-fitting of the humeral stems, as their senior surgeon initially cemented all implants early in the series and subsequently cemented almost none of the stems in the later stages, potentially introducing a selection bias.
Wiater et al. 18 also investigated the two types of fixations, finding no differences. Unlike our study, they used two types of implants for the different techniques finding 48 min longer operative time for the cement group. These results focus the attention of the mean reported lower operative time as another advantage of the press-fit humeral fixation.
Yet, none of the above studies stratified their results in relation to the presence of SS.
Patterns of SS might be different between humeral designs. We found humeral osteolysis in 45 patients (90%), and radiolucencies condensation lines and spot welds in 17 (34%) and 17 (34%) patients, respectively. In the present study, the threshold for DFR was set at 70% since Raiss et al. 11 mentioned it as a risk factor for the occurrence of SS for some uncemented convertible short stems. Indeed, they evaluated radiological complications of short press-fit stems at 2 years finding 35% of SS; the most common findings were cortical thinning and spot welds in the lateral diaphysis (22%) or osteopenia in the medial metaphysis (33%). These results are in line with the present study where a similar association was found for a DFR greater than 70%. Only one study aimed to validate the manually measured DFR on 2D radiographs with an automated measurement based on CT scans. 7 Manual measurement of the DFR was found to underestimate on conventional radiographs compared to automated calculation on CT scans by a mean of 3%. Even though this slight significant difference between methods exists, manual technique provides a reasonable compromise for calculating the DFR in cases with no available CT scans. The debate regarding the optimum value of DFR to implant uncemented short stem remains open. However, this study supports the concept that SS should be avoided and evaluating DFR in the preoperative setting could be the key to prevent it. The findings of this study shed light on the critical importance of preoperative assessment when determining the appropriate stem size. Specifically, relying solely on the intra-operative Twist test may result in the placement of an oversized stem, leading to subsequent SS and deterioration of clinical outcomes. Therefore, having prior knowledge of the maximum stem size deemed suitable can guide the surgeon in utilizing the Twist test up to that limit. Should the Twist test at that size prove unsatisfactory, alternative solutions such as cementation or impaction grafting should be considered. This proactive approach ensures a more informed decision-making process and potentially improves patient outcomes.
The present study had several limits. First, this was an analysis of radiological exams collected in the past, a prospective analysis of randomized patients would be more significant. Second, the representativeness of the underlying cohort is limited and since results came from a two-surgeons patients’ cohort, the small heterogeneity of surgical techniques could bias the results. Longer follow-up studies are required to assess whether the progression of SS occurs and to analyze its relationship with long-term survivorship in uncemented stems with DFR > 70%.
Finally, a single implant was used underling a possible lack of reproducibility of these results for patients with different humeral stems configuration.
Conclusion
3D CT-based measurements are accurate for prediction of postoperative DFR in short-stem press-fit RSA. Postoperative DFR higher than 70% was found to be significantly associated with an increase of SS. In this study, at minimum 2-year follow-up, the presence of SS was significantly associated with a decrease of anterior elevation after RSA. Further studies are needed to investigate the validity of these results at mid-term and long-term follow-ups.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.