
Abstract
Objective
To explore potential mediators of treatment effect and moderators of scapular-focused interventions on shoulder disability at 12-week follow-up in patients with chronic shoulder pain.
Design
Secondary analysis of a randomized controlled trial that compared the effects of scapular movement training with standardized exercises.
Methods
Sixty-four participants with chronic shoulder pain were enrolled in the trial, of whom 58 completed the 12-week follow-up and were included in these analyses. Shoulder disability was assessed with Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire. Potential mediators were scapular upward rotation, kinesiophobia, and fear avoidance beliefs. Potential moderators were kinesiophobia, fear avoidance beliefs, and duration of symptoms.
Results
Kinesiophobia, fear avoidance, and scapular upward rotation did not (p >0 .05) mediate the effects of scapular focused interventions on shoulder disability. Our sensitivity analyses indicated that the findings are likely to change because there were some small residual confounding factors between those mediators and the shoulder disability scores at 12 weeks. Kinesiophobia, fear avoidance, and duration of symptoms did not moderate the effects of the intervention on shoulder disability.
Conclusions
Kinesiophobia, fear avoidance, duration of symptoms, and scapular upward rotation did not mediate or moderate the effects of scapular-focused interventions on shoulder disability at 12-week follow-up.
Introduction
Shoulder pain is a common disorder in the general population,1–3 with impact on quality of life, work productivity, daily functional activities, and healthcare expenses over time.4,5 Scapular dyskinesis is frequently observed in individuals with shoulder pain and scapular-focused interventions are commonly recommended and conducted in clinical practice to treat this condition.6,7
Therapeutic exercises, including scapular-focused exercises, are supported and recommended by systematic reviews and clinical practice guidelines,7–10 which often focus on improving scapular movement pattern.11–14 However, it is unclear whether improvements in shoulder disability are mediated or moderated by scapular kinematics, psychological factors, and duration of symptoms. Therapeutic exercises or physical activity may cause changes in pain symptoms or disability indirectly, by changing psychological variables (e.g. kinesiophobia, fear avoidance beliefs).15–17 In addition, previous studies described that patients’ characteristics, such as duration of symptoms and psychological factors, may influence the effects of therapeutic exercises on shoulder disability.18–22 Nevertheless, the role of those potential mediators and moderators of scapular-focused interventions is still unknown.
A recent randomized controlled trial (RCT) investigated whether the scapular movement training is superior to standardized exercises in the treatment of individuals with shoulder pain. 23 The scapular movement training aimed to educate the individuals about the proper scapular position in the rest position and during arm elevation, and the muscle activation during the elevation of the arm, and to improve the pattern of scapular movement during arm elevation and during a relevant functional activity chosen by the patient. The findings suggested that both interventions significantly improved pain intensity, disability, kinesiophobia, and fear avoidance beliefs, but with no clinically important differences between groups. Mediation and moderation analyses can help us to understand whether the intervention failed to cause improvements in potential mediators and whether there is a subgroup of patients who may benefit more from scapular-focused exercises.
Mediation analysis is an approach to study causal mechanisms, which can parse a treatment effect into indirect (effect on an outcome that is carried through a selected mediator) and direct effects (remaining effect not explained by the selected mediator).24–26 Moderators (treatment effect modifiers) are baseline characteristics of individuals that are associated with differential treatment response. Moderators influence the relationship between treatment and outcome (i.e. the effect of treatment on individuals depends on their value of the moderator, which precedes treatment and is not associated with treatment). 27
The aim of this secondary analysis of a RCT was to explore potential mediators and moderators of scapular-focused interventions on shoulder disability at 12-week follow-up in patients with chronic shoulder pain.
Methods
Design
This is a secondary analysis of data from a previous RCT that compared scapular movement training with standardized exercises for patients with chronic shoulder pain (NCT03528499).
Participants
Participants were eligible if they were aged between 18 to 60 years, primary complaint of shoulder pain for at least 3 months with a Numerical Pain Rating Scale score of 3 points23,28 or greater during arm elevation, a positive Scapular Assistance Test (SAT), presence of scapular dyskinesis, and 150° or more of active arm elevation. Scapular dyskinesis was assessed and SAT was performed as previously described.29,30 Individuals were excluded if they presented history of surgery, fracture, instability and/or dislocation of the shoulder, signs of adhesive capsulitis, massive rotator tears (positive drop-arm test), body mass index greater than 28 kg/m2, pregnancy, tingling or numbness in the upper limb reproduced by the upper limb tension test or cervical compression test, self-reported tape allergy, neurologic or systemic illness, and physical therapy and corticosteroid injection in the last 6 and 3 months, respectively.23,28,31
Interventions
The details of the interventions tested within the trial have been described elsewhere.23,28 Both intervention groups involved 16 individual sessions, twice a week, over 8 weeks. Scapular movement training group involved education on scapular position and movements impairments and optimal muscle activation during the first week, which included verbal, tactile, and visual feedback with support of anatomical models, EMG biofeedback of lower trapezius, middle trapezius, and serratus anterior, and mirror for visual feedback. Following the education phase, the treatment included exercises with slow, conscious, and paced movements of arm elevation and a functional activity selected by the patient, which aimed to improve the pattern of scapular movement.
The standardized exercise group involved stretching exercises targeting the UT, 31 posterior region of shoulder, and pectoralis minor, 32 and the following strengthening exercises using elastic resistance bands (Theraband®): prone extension, 33 prone horizontal abduction with external rotation, 33 serratus punch, 34 and side-lying external rotation. 33
Outcome measure
Shoulder disability was assessed with the Brazilian version of Disabilities of the Arm, Shoulder and Hand (DASH). The DASH is composed of 30 items that assess the ability to perform activities using the upper limb, and the final score ranges from 0 to 100, with lower scores indicating lower disability. The minimal clinically important difference in the DASH score is 10.8 points and the inter-rater and intra-rater reliability are 0,93 and 0,99, respectively.35,36
Potential mediators
The selection of mediators was based on the theoretical rationale that both scapular upward rotation and psychological factors may cause improvement role in shoulder disability outcomes.37,38 Previous observational studies found that changes in scapular upward rotation have been associated with shoulder pain and disability.37,38 Scapular movement training focused on improving scapular movement patterns which would cause improvements in shoulder disability outcomes. 23 Psychological factors such as kinesiophobia and fear-avoidance beliefs were considered as putative mediators due to their association with higher pain intensity and greater disability in individuals with chronic shoulder pain.39–42 These factors have been suggested to mediate the effects of therapeutic exercises on clinical outcomes (Figure 1).43–46
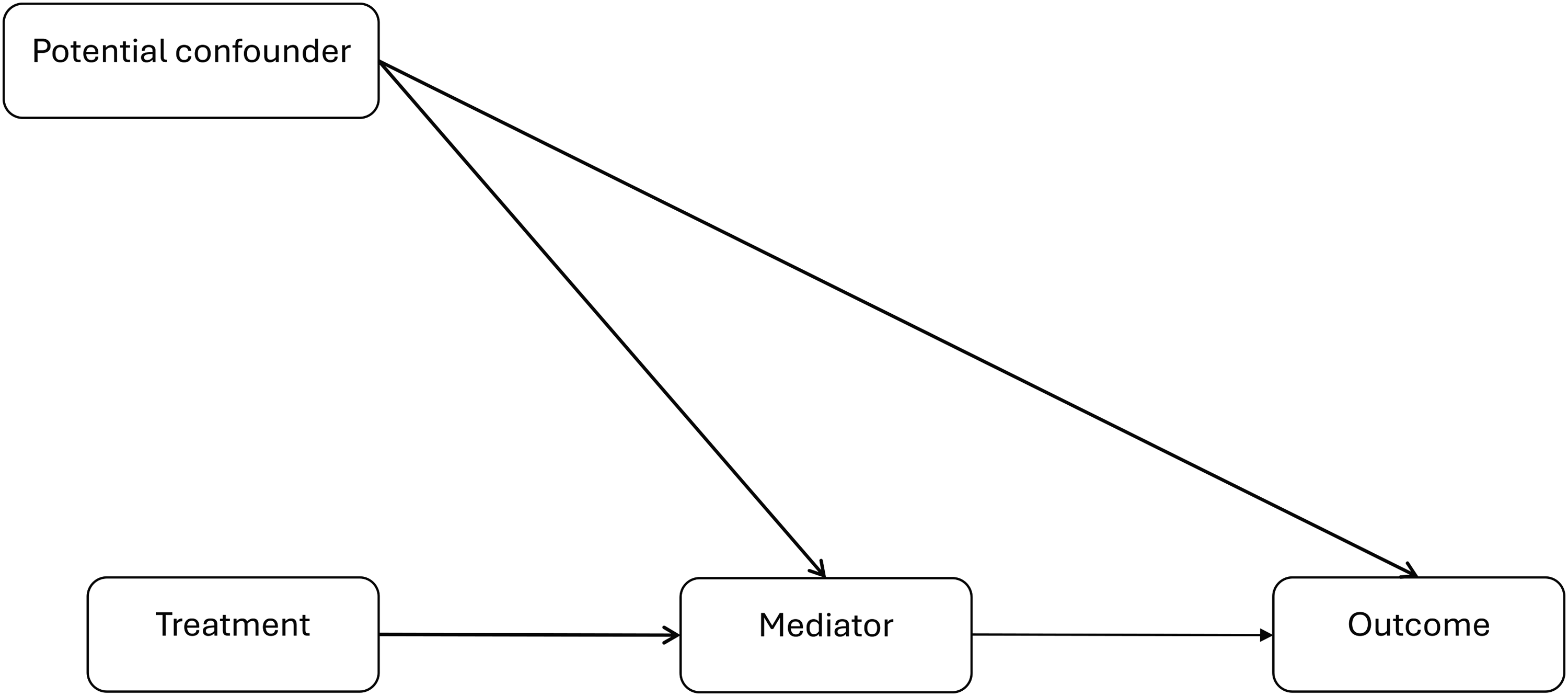
Directed acyclic graph representing the causal model with mediator of treatment effect on clinical outcomes (shoulder disability). *Mediators tested included: kinesiophobia, fear-avoidance beliefs, and scapular upward rotation.
Mediation analysis was conducted to identify the causal mechanisms through which ascapular-focused interventions affects shoulder disability. Such analyses allow researchers to estimate the direct and indirect effects of scapular-focused interventions.24–26 The effect of a treatment analyzed through a selected mediator is considered the indirect effect, while the effect not determined by the selected mediator is the direct effect. 47
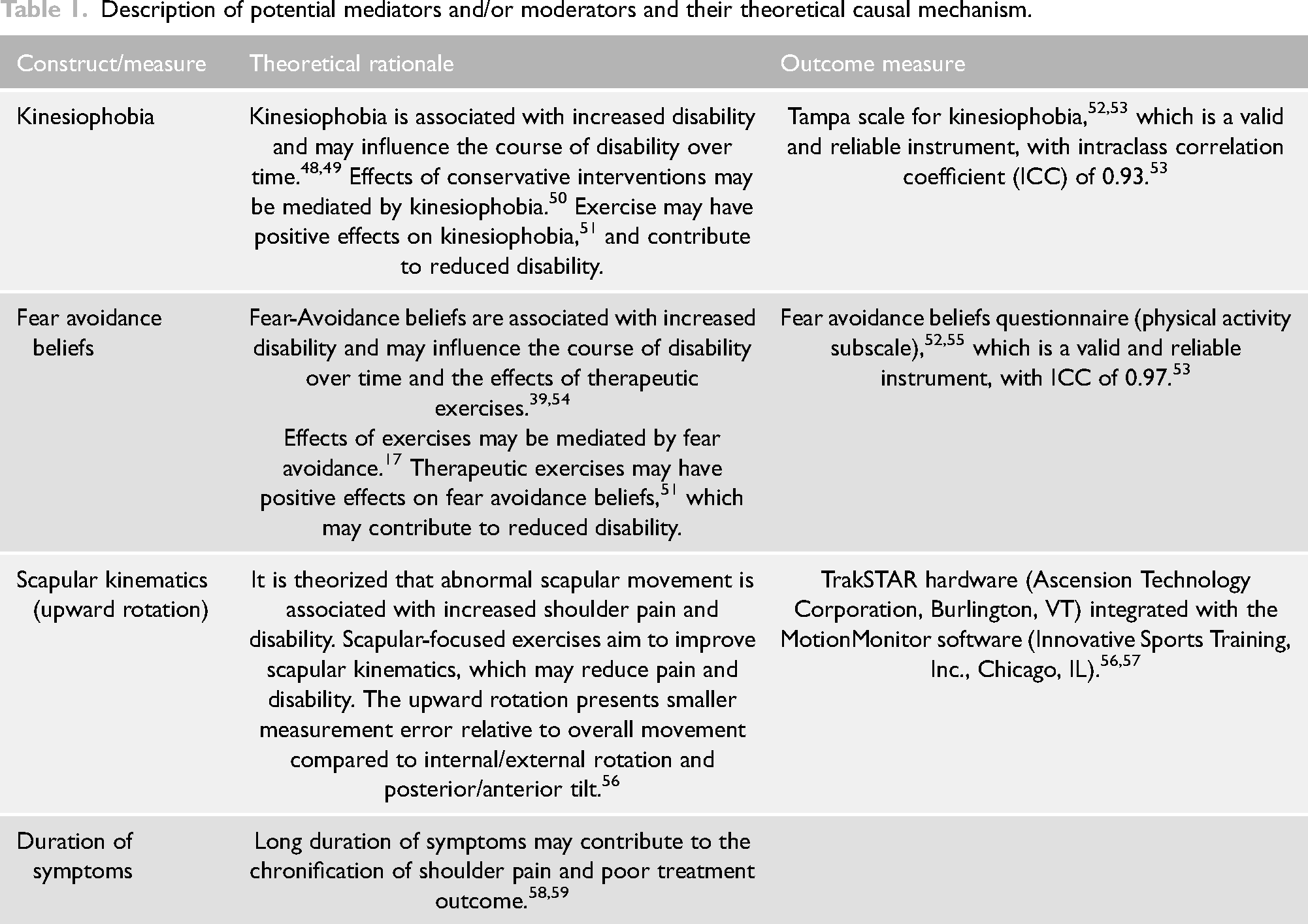
The selected mediators and theoretical rationale for the potentially important mediators are described in Table 1. The mediators were selected prior to the analysis. The scapular upward rotation was not considered in the moderation analysis because all individuals presented scapular dyskinesis and positive SAT. All mediators were measured at baseline and at the 12th week, except for scapular kinematics, which was measured in the 8th week.
Description of potential mediators and/or moderators and their theoretical causal mechanism.
Potential moderators
Through moderation analyses, researchers can estimate the interaction between baseline characteristics of patients with chronic shoulder pain, such as duration of symptoms, kinesiophobia, and fear avoidance beliefs, and clinical outcomes, following scapular-focused interventions. Such analyses assist in identifying which group of patients may respond better to a given treatment. 24
The following variables were assessed as potential moderators of the treatment effect: kinesiophobia, fear avoidance beliefs, and duration of symptoms. The work subscale of Fear Avoidance Beliefs Questionnaire was not considered due to possible floor effect in individuals with shoulder pain (Figure 2), 52 and only the physical activity subscale was used in this mediation and moderation analysis.
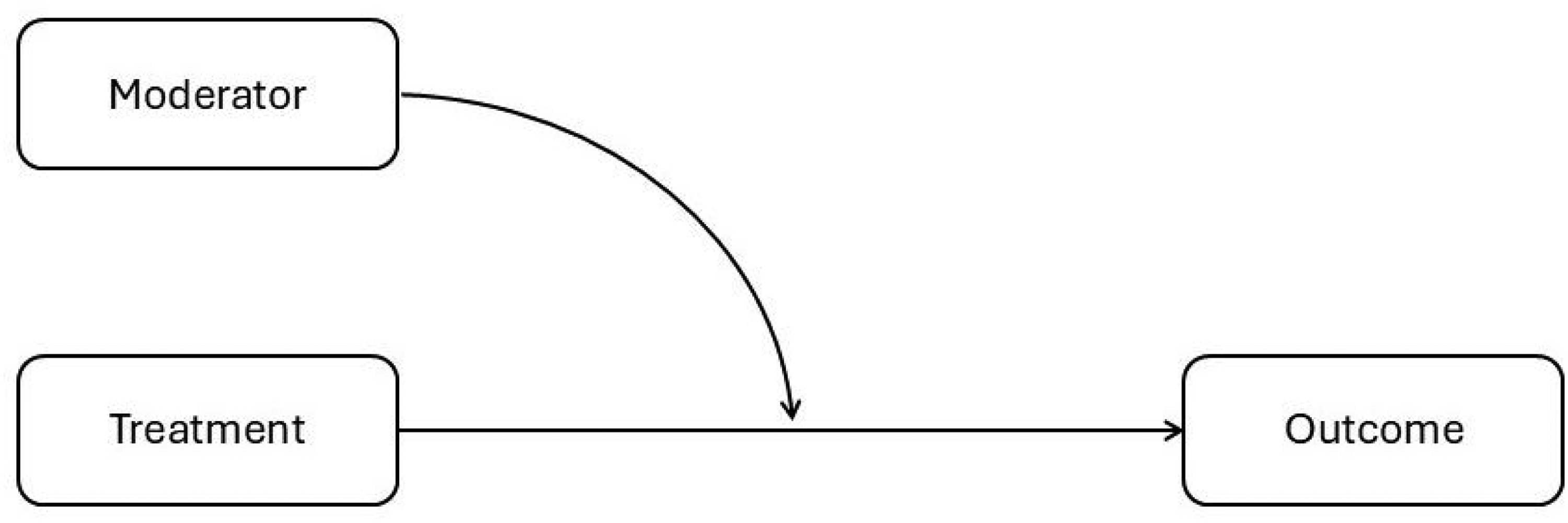
Directed acyclic graph representing the causal model with moderator of treatment effect on clinical outcomes (shoulder disability). *Moderators tested included: kinesiophobia, fear-avoidance beliefs, and scapular upward rotation.
Missing data
Sixty-four participants with chronic shoulder pain were included in the original trial, 59 (92.1%) completed the 8-week follow-up, and 58 (90.6%) completed 12-week follow-up, which resulted in missing data of 6 participants. In addition, the scapular kinematics data of 2 individuals were excluded from analysis due to noise in the electromagnetic signal, which also resulted in missing data in the analysis of scapular kinematics. We assumed missing data was missing at random (MAR) and implemented conditional multiple imputation by using the package mice 60 (R software), 61 allowing for a maximum interaction of 50.
Statistical analysis
Sample size estimation
This is a post-hoc, secondary analysis of a previous trial, 23 which had an appropriate sample size to identify a minimum difference of 5.5o in the scapular posterior tilt between the two groups. Despite this being a post-hoc and exploratory study, we estimated the required sample size for a mediation analysis under two different scenarios. In the first scenario, we assumed a large treatment-mediator and mediator-outcome effect (r = 0.6) in the second scenario, we assumed a moderate treatment-mediator and mediator-outcome effect (i.e. r = 0.3). We also assumed there was: (a) no exposure-mediator confounding, given this is a randomized trial; (b) a moderate confounding for the mediator-outcome (r = 0.3). 62 We set power at 0.8.
The results of our sample size estimation suggested that: a minimum of 80 participants (40 per group) were required if there were large treatment-mediator and mediator-outcome effects. In case of moderate treatment-mediator and mediator-outcome effects, a minimum of 342 participants would be required. Those analyses suggest our present study was powered for detecting a large mediating effect but lacked power for detecting a moderate mediating effect.
Mediation
Mediation analyses was performed using the counterfactual framework,63,64 assuming that there were: (1) no unmeasured confounding between the intervention-mediator relationship; (2) no unmeasured confounding between intervention-outcome relationship; (3) no unmeasured confounding between mediator and outcome; (4) no mediator-outcome confounder that is affected by the intervention; and (5) presence of temporal sequence from exposure (i.e. intervention), to the mediator to the outcome.
Assumptions #1 and #2 are satisfied because the participants were randomly allocated to interventions tested within the trial. Mediators were not randomized, so this path was potentially confounded. Hence, duration of symptoms was considered as confounder, and it was included as covariates in the outcome regression models. The baseline measures of potential mediators and baseline measures of the outcome measure were also included in the regression models (i.e. DASH score at the baseline) and included those as covariates in the outcome regression models.
Mediation analysis was performed using structural equation modeling to estimate the average causal mediation effect, average direct effect, average total effect, and proportion mediated. 64 Two linear models were fitted: the mediator model and the outcome model. The mediator model considered the potential mediator the dependent variable and treatment allocation the independent variable. The outcome model considered DASH scores at 12-week follow-up as the dependent variable and treatment allocation as the independent variable. The mediate disability (mediation package) 65 was used to compute the average causal mediation effect, average direct effect, average total effect, and proportion mediated, with bootstrap simulations (n = 1000) to compute 95% confidence intervals. 65
The first regression model included the mediator as the dependent variable; treatment as the independent variable, and duration of symptom as covariate. The second regression model included the DASH score at 12-week follow-up as dependent variable, and treatment as the independent variable and duration of symptoms as covariate.
Indirect and direct effects may be dependent on treatment allocation. Therefore, an interaction term (treatment×mediator) was included in the outcome model. The average causal mediation effects was calculated for each conditional on treatment exposure (x = 1 and x = 0) and their respective marginal effects because interaction effects can lead to significant bias on indirect and direct estimates of treatment effect.66,67 The function “mediate” was used in R software to assess the total, direct, indirect effects and the proportion mediated. 68
To assess the robustness of our mediation analyses, sensitivity analyses was conducted to the no unmeasured confounding assumption 69 because we cannot rule out the possibility of confounding for the mediator-outcome relationship.66,70 Sensitivity analyses was conducted using the medsens function (mediation package). 69
Moderation
Linear regression models were used to assess whether selected characteristics of participants at baseline moderated the effect of randomized interventions on pain and disability. Linear regressions were performed using the DASH score at 12 weeks follow-up as the dependent variable. Treatment allocation was included as the independent variable, while the duration of symptoms, fear avoidance, kinesiophobia, and DASH score at baseline as covariates.
For assessing whether treatment effects were moderated by one of the chose moderators, we included a standard interaction term between the selected moderator and group intervention. Standard diagnostic plots were used to assess regression assumptions of linearity and homoscedasticity. Interaction between exposure (i.e. treatment) and the potential moderator through plots of DASH score at 12 weeks versus the potential moderator were also visually assessed.
Descriptive statistics were conducted to summarize participants’ characteristics (i.e. number and percentage for describing categorical variables, mean and standard deviations for describing continuous variables). The R Software 61 was used for conducting all analyses and set alpha at 0.05.
Results
The baseline characteristics of the participants are described in Table 2.
Baseline characteristics of participants.
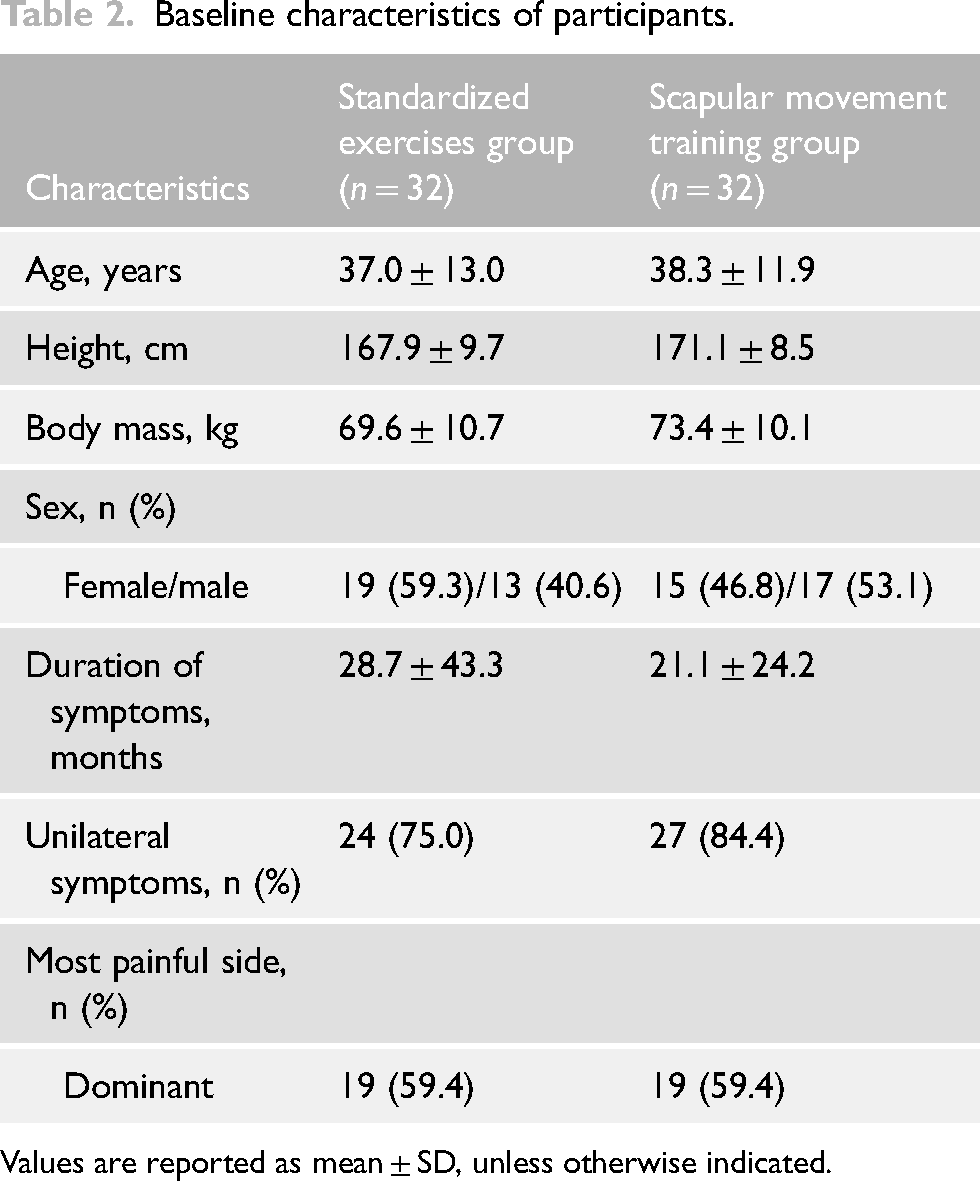
Values are reported as mean ± SD, unless otherwise indicated.
Mediators
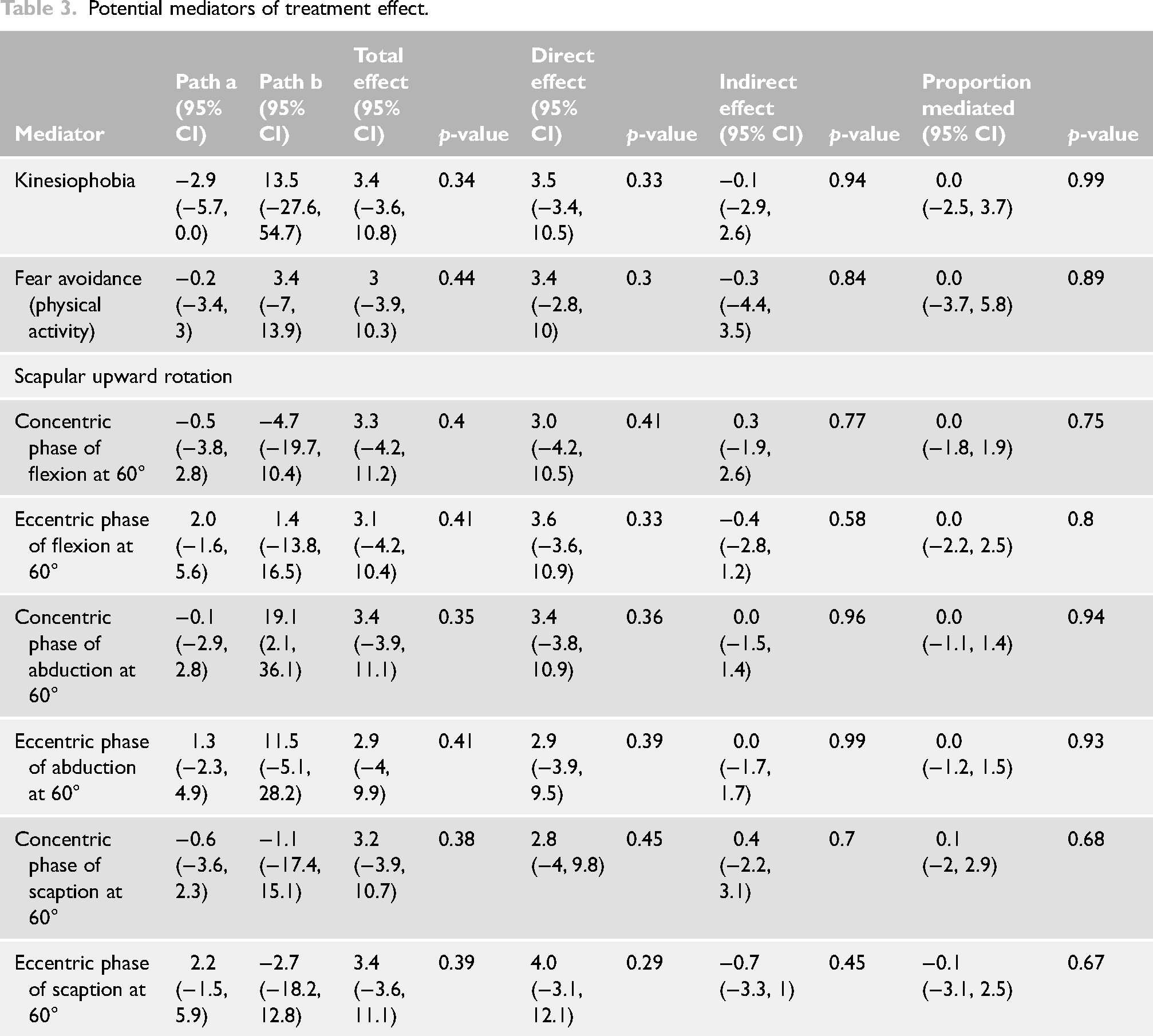
The findings of the mediation analyses are presented in Table 3. Changes in kinesiophobia, fear avoidance, and scapular upward rotation during arm elevation and lowering at scapular plane did not present direct or indirect mediator effect on shoulder disability in individuals with chronic shoulder pain. Sensitivity analyses suggest small violations of the no unmeasured confounding assumption (e.g. r ≥ 0.1) may change our estimate of mediation effect (Supplemental material).
Potential mediators of treatment effect.
Moderator
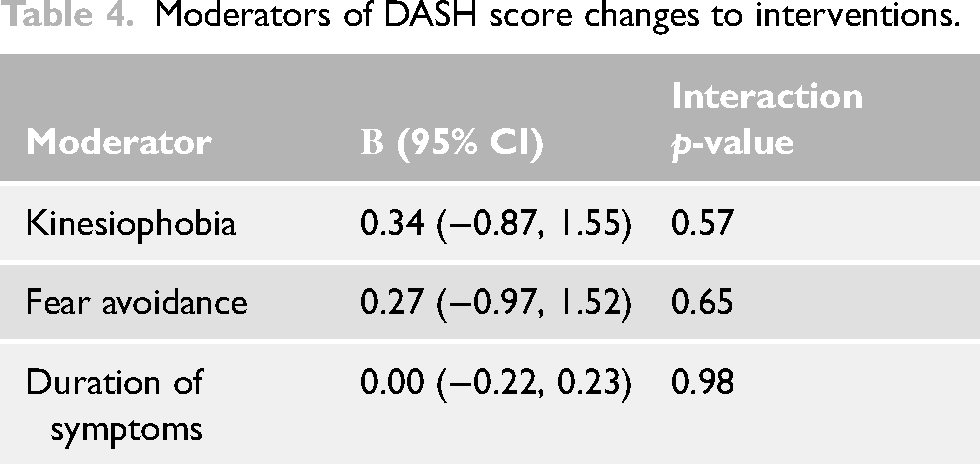
The findings of the moderation analyses are presented in Table 4. Kinesiophobia (effect = 0.34, 95% CI: −0.87 to 1.55), fear avoidance (effect = 0.27, 95% CI: −0.97 to 1.52), and duration of symptoms (effect = 0.00, 95% CI: −0.22 to 0.23) did not moderate the treatment effect of interventions.
Moderators of DASH score changes to interventions.
Discussion
We conducted this exploratory secondary analysis a recently published trial, (NCT03528499), to explore whether kinesiophobia, fear-avoidance beliefs, and scapular upward rotation during arm elevation and lowering at scapular plane mediated treatment effects, or whether kinesiophobia, fear avoidance, and duration of symptoms moderated treatment effects. Our results showed no mediation effect on shoulder disability, and that kinesiophobia, fear avoidance, and duration of symptoms did not moderate treatment effects in patients with chronic shoulder pain being treated with scapular movement training or standardized exercises.
The results of this study did not find any mediating effect of scapular upward rotation on shoulder disability. Our results suggest scapular-focused interventions did not cause changes in scapular upward rotation (i.e. path a). The findings of this study are in accordance with a previous study, 71 which suggests that scapular kinematics do not mediate the effects of scapular exercises on shoulder pain or disability in individuals with shoulder pain. The role of scapular dyskinesis has been questioned72–74 as the pattern of altered scapular kinematics is not consistent among patients with shoulder pain, scapular dyskinesis may be present in asymptomatic individuals, the changes in muscle activity or scapular movements may be a consequence of painful symptoms in shoulder region.72,73,75–77 In addition, no association has been found between changes in pain or function scores and changes in scapular upward/downward rotations or scapular anterior/posterior tilt. 78 On the other hand, a previous study found that changes in scapular movement patterns were fairly correlated with disability scores in patients with shoulder subacromial pain, but those correlations may be confounded. 79
Systematic reviews have indicated that scapular-focused exercises may present small and not clinically important benefits on pain intensity and disability compared to the general approach,7,80,81 and that there are conflicting findings or no changes on scapular movement or position. 81 However, clinicians still recommend scapulothoracic muscle strengthening exercises or scapular movement training based on the rationale that patients with shoulder pain frequently present weak or altered muscle activity of scapulothoracic muscles or impaired scapular movement.82–86 Nevertheless, the improvements in disability of the patients of this study were not explained by changes in scapular upward rotation, which suggests that clinicians should not focus on changing scapular upward rotation during the treatment of patients with shoulder pain. Therefore, further studies should consider the analysis of additional outcomes, such as pain intensity and self-perception of change in health condition, and additional mediators or moderators, including pain catastrophizing, self-efficacy, anxiety, depression, patient's expectations, scapulothoracic muscle activity or muscle strength, and tendon structural changes, all of which may play an important role in shoulder rehabilitation.
Previous studies demonstrated that psychological factors play an important role in the development and prognosis of shoulder pain,22,39 and kinesiophobia and fear-avoidance beliefs were associated with high intensity of shoulder pain and disability.22,39,40,87 Therapeutic exercises may reduce pain-related fear in individuals with chronic musculoskeletal disorders.51,88 Our findings showed that patients’ kinesiophobia and fear-avoidance beliefs did not mediate nor moderated the effects of scapular-focused interventions. The lack of mediation may be explained by the small changes observed in kinesiophobia and fear-avoidance outcomes at 12-week follow-up. In addition, the changes in those variables did not exceed the minimal detectable change of those outcome measures.52,89–91 Another possible explanation is that the Tampa Scale for Kinesiophobia and the Fear-Avoidance Beliefs Questionnaire were originally developed for individuals with chronic low back pain and may exhibit floor effects when used in populations with shoulder pain. 52
Riley et al. (2020) conducted mediation analyses that suggested that improvement in positive psychological factors (i.e. self-efficacy) may be more meaningful for functional outcome than improvements in negative psychological factors (e.g. fear avoidance beliefs) in individuals with low back pain. Unfortunately, in the original trial, other psychological factors were not measured, including pain catastrophizing, anxiety, depression, self-efficacy, and patients’ expectations, which might have provided valuable information on mechanisms of therapeutic exercises on shoulder rehabilitation. Therefore, future studies should also measure psychological variables (e.g. self-efficacy, anxiety, depression, pain catastrophizing) at different time points to estimate whether they mediate treatment effects of scapular-focused interventions.
Previous studies indicated that the duration of symptoms predicts poorer outcomes after treatment.58,92–94 Interestingly, the duration of symptoms did not moderate the effects of scapular-focused interventions on shoulder disability. Only individuals with chronic symptoms were included in the original study, potentially accounting for the lack of moderation effects by the duration of symptoms on shoulder disability.
This study provides important insights, describing that treatment effects were not mediated by kinesiophobia, fear-avoidance beliefs, or scapular upward rotation. Furthermore, it describes whether treatment effects were not moderated by kinesiophobia, fear avoidance, or duration of symptoms. The information on how interventions work may assist the delivering effective treatments and reaching better outcomes.
There are limitations to our study. The sample size was calculated for comparison of the effects between scapular movement training and standardized exercises. The secondary analyses reported in this study were not planned a priori and were only powered to detect large mediating effects. Therefore, the sample size was insufficient to detect small or moderate effects. There are different methods for estimating sample size for mediation studies, with different trade-offs between those methods. 95 Given the little literature in this area and despite the limitations of our study, our findings are informative for researchers planning future projects in this area. Multiple analyses were conducted which increased the risk of type I error. However, our goal was to explore potential mechanisms of action of the interventions tested within the original trial, and confirmation analyses on larger data sets should be conducted before the results of this study are interpreted with certainty. Nevertheless, these are valuable for improving the design of future trials. The analyses considered only the changes in shoulder disability as the outcome with a limited number of mediators (scapular upward rotation, kinesiophobia, and fear avoidance beliefs) and moderators (kinesiophobia, fear avoidance beliefs, and duration of symptoms) that were collected in the original trial and due to limited sample size. 96 In addition, there are other factors that were not measured in this study (e.g. self-efficacy, anxiety, depression, pain catastrophizing) that might interact with the factors measured in this study. These unmeasured factors should be investigated in future studies.
In conclusion, the effects of scapular-focused interventions on shoulder disability were not mediated by changes in scapular kinematics, kinesiophobia, and fear avoidance beliefs. In addition, those effects were not moderated by the duration of symptoms, kinesiophobia and fear avoidance beliefs as measured at baseline.
Supplemental Material
sj-docx-1-sel-10.1177_17585732251354920 - Supplemental material for Mediators and moderators of scapular focused interventions on shoulder disability in individuals with chronic shoulder pain: Secondary analysis of a randomized controlled trial
Supplemental material, sj-docx-1-sel-10.1177_17585732251354920 for Mediators and moderators of scapular focused interventions on shoulder disability in individuals with chronic shoulder pain: Secondary analysis of a randomized controlled trial by Danilo Harudy Kamonseki, Daniel Cury Ribeiro, Melina Nevoeiro Haik, Larissa Pechincha Ribeiro, Rafaela Firmino Almeida and Paula Rezende Camargo in Shoulder & Elbow
Footnotes
Author contributions
Each of the authors has contributed substantially and concurs with the content in the manuscript. Conceptualization: DHK, DCR, MNH, LPR, PRC. Data curation: DHK, DCR, MNH, PRC. Formal analysis: DCR. Funding acquisition: DHK, DCR, PRC. Investigation: DHK, LPR, RFA. Methodology: DHK, MNH, LPR, RFA, PRC. Project administration: DHK, MNH, RFA, PRC. Resources: DHK, PRC. Supervision: MNH, PRC. Validation: DCR, MNH, PRC. Visualization: DCR, MNH, LPR, PRC. Roles/Writing—original draft: DHK, DCR, MNH, RFA, PRC. Writing—review & editing: DHK, DCR, MNH, LPR, PRC.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This is a secondary analysis of a randomized controlled trial (NCT03528499), which was approved by the Human Research Ethics Committee of the Federal University of São Carlos (reference number: 86974318.7.0000.5504).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo—FAPESP (2018/04911-1; 2020/00771-0), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES), and Conselho Nacional de Desenvolvimento Científico e Tecnológico—CNPq (142373/2018-4). The research was conducted during tenure of The Sir Charles Hercus Health Research Fellowship of the Health Research Council of New Zealand [Grant number: 18/111] awarded to DCR.
Informed consent
All individuals signed a written consent before study enrollment and were aware of the main purpose of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.