
Abstract
The National Health Service (NHS) faces restricted capacity for first reviews of orthopaedic patients. Advanced Physiotherapy Practitioners (APP) offer an effective alternative to doctor consultations, potentially increasing capacity and promoting efficient use of resources. A new APP-led service for shoulder instability was established on this basis, aiming to promote adherence to recommended care pathways, and increase patient satisfaction. This service evaluation assesses the APP service. Methods included comparing data from the same 6-month period in consecutive years. Wait times from A&E to the first appointment and adherence to care pathways were measured. Process mapping was conducted. Patient satisfaction was measured and thematically analysed qualitatively. Results demonstrated reduction in wait times by 6 days in the APP led service, with 100% patient satisfaction. Adherence to the care pathway improved; all patients under the age of 25 received appointments within 6 weeks, and early imaging referrals increased by 40%. In conclusion, the APP-led service decreased wait time and enhanced adherence to care recommendations, with high patient satisfaction. This supports the use of physiotherapists in delivering care in this cohort of patients. Future service improvements could focus on raising awareness of referral processes to maximise service use.
Keywords
Introduction
The Glenohumeral joint (GHJ) is the most dislocated joint in the body. 1 For the National Health Service (NHS), GHJ dislocation is predominantly seen in men under 20 years and women over 50 years. 2 Traumatic shoulder dislocation can lead to recurrent instability, particularly in patients under 40 due to structural damage such as Bankart and Hill-Sachs lesions, 3 whereas the likelihood of sustaining rotator cuff tear (RC) increases with age. 4 The British Elbow and Shoulder Society (BESS) care pathway provides recommendations for managing these patients, focusing on timely review and appropriate treatment. 5
Historically at the NHS Trust which we evaluated, patients with shoulder dislocations were referred from A & E to the fracture clinic, creating long wait times (median: 19 days) for consultant or registrar reviews. In August 2023, a new APP-led pathway was introduced to increase capacity in the department, with a view to reducing delays and improving adherence to evidence-based care recommendations.
BESS care pathway 5 for patients under 25 years old recommends review within 6 weeks, physiotherapy, and imaging with a view to surgery if appropriate, following clinical reasoning and shared decision making. 5 In the cohort of over 25-year-olds, imaging and surgery are recommended if patients are still getting instability between 4 to 6 months after the injury. 5 Olds et al. 6 developed the ‘Predict Recurrent Instability of the Shoulder’ tool (PRIS tool), a stratification tool using a combination of patient demographics and risk factors to aid clinical decision making on management. The APP pathway aims to utilise this evidence, carefully selecting surgical candidates or referring to physiotherapy.
RC tears, common in patients over 40 years old following dislocation, can be managed either surgically or conservatively with physiotherapy. The fact that not all patients are surgical candidates demonstrates that an APP may be able to offload orthopaedic surgeons, decreasing waitlists and providing rationale for the service. 7 Surgical outcomes are poorer when surgery is delayed. 4 Due to the risk of a poorer surgical outcome with delay to surgery, traumatic acute RC tears should be reviewed in the next available specialist shoulder clinic. 5 The APP service aims to reduce wait time and therefore increase the chances of surgical success if surgery is performed.
Aim
To evaluates the effectiveness of the APP-led service in improving patient outcomes, adherence to care pathways, and patient satisfaction while offloading consultant workloads.
Objectives
The following objectives were identified:
Identify patient pathways through the service to determine if the service was being used as intended. Compare wait times for the APP lead service against wait times within the usual care (UC) service. Compare patient outcomes from both UC and the APP pathway to the BESS care pathway.
5
Monitor patient satisfaction within the APP led patient pathway.
This service evaluation (SE) was conducted to assess the newly implemented APP-led pathway for shoulder instability at a central London secondary care hospital.
The SE did not require NHS ethical approval, the protocol was approved by Brunel University of London (BREO reference: 43682-NER-Jul/2023-46478-1).
The evaluation analysed routinely collected, anonymised patient data. Consent for data use was inherent to clinical care, and no modifications to patient management were introduced.
The study utilised data from August 2023 to January 2024 for the APP pathway and August 2022 to January 2023 for the historical UC pathway. Participants were identified via convenience sampling, all patients attending A and E with a shoulder dislocation between the relevant time frames were identified. Patients attending A and E are routinely coded according to diagnosis via Cerner (Oracle Cerner, London). Shoulder dislocation codes were requested via a Cerner analyst allowing identification of relevant patients.
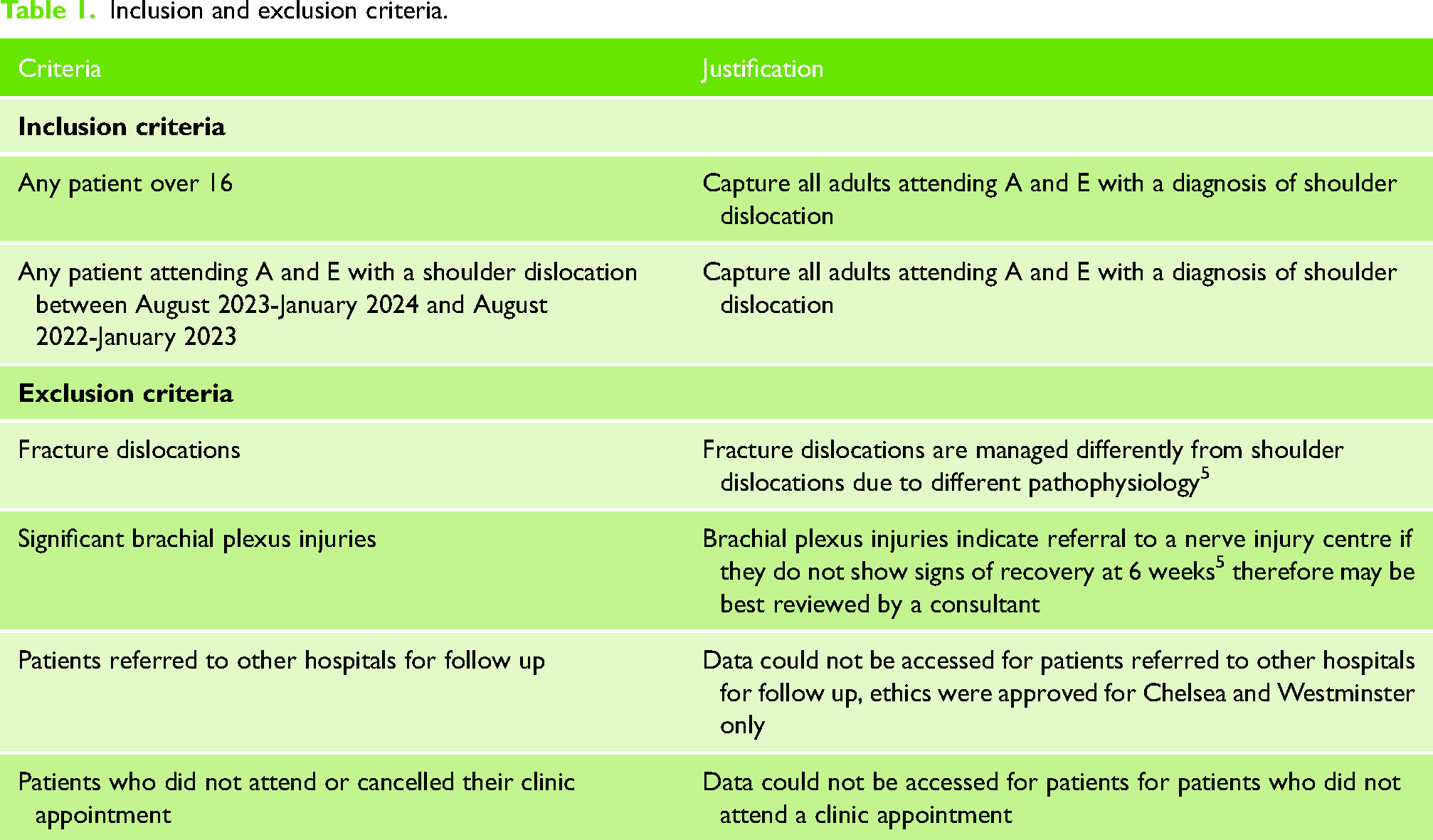
Inclusion/exclusion criteria (Table 1) were applied to the objectives addressing wait times, patient outcomes, and patient satisfaction (objective 2, 3 and 4). To evaluate service utilisation (objective 1), all patient pathways were analysed without criteria application.
Inclusion and exclusion criteria.
Missing data were minimised through requesting missing clinic letters. Data were securely stored on password-protected systems in compliance with the Data Protection Act (2018).
Data collected included wait time from A and E to first appointment, outcome of first appointment, whether this be specialist imaging, referral to physiotherapy or surgery, and patient satisfaction (Friends and Family Test). Process mapping was completed for the new service between August 2023 and January 2024. The data was analysed descriptively. Descriptive theming was performed on the patient satisfaction data – this process is detailed in Supplemental Appendix 1.
Results
In this section the results of the data collection and analysis will be presented, with respect to each objective.
UC includes all patients who attended A and E with a shoulder dislocation between August 2022 and January 2023, with inclusion and exclusion criteria applied.
The APP led service (APPS) includes all patients who attended A and E with a shoulder dislocation between August 2023 and January 2024, with inclusion and exclusion criteria applied. The demographics for the two datasets were recorded in Table 2.
Demographics of UC and APPS.
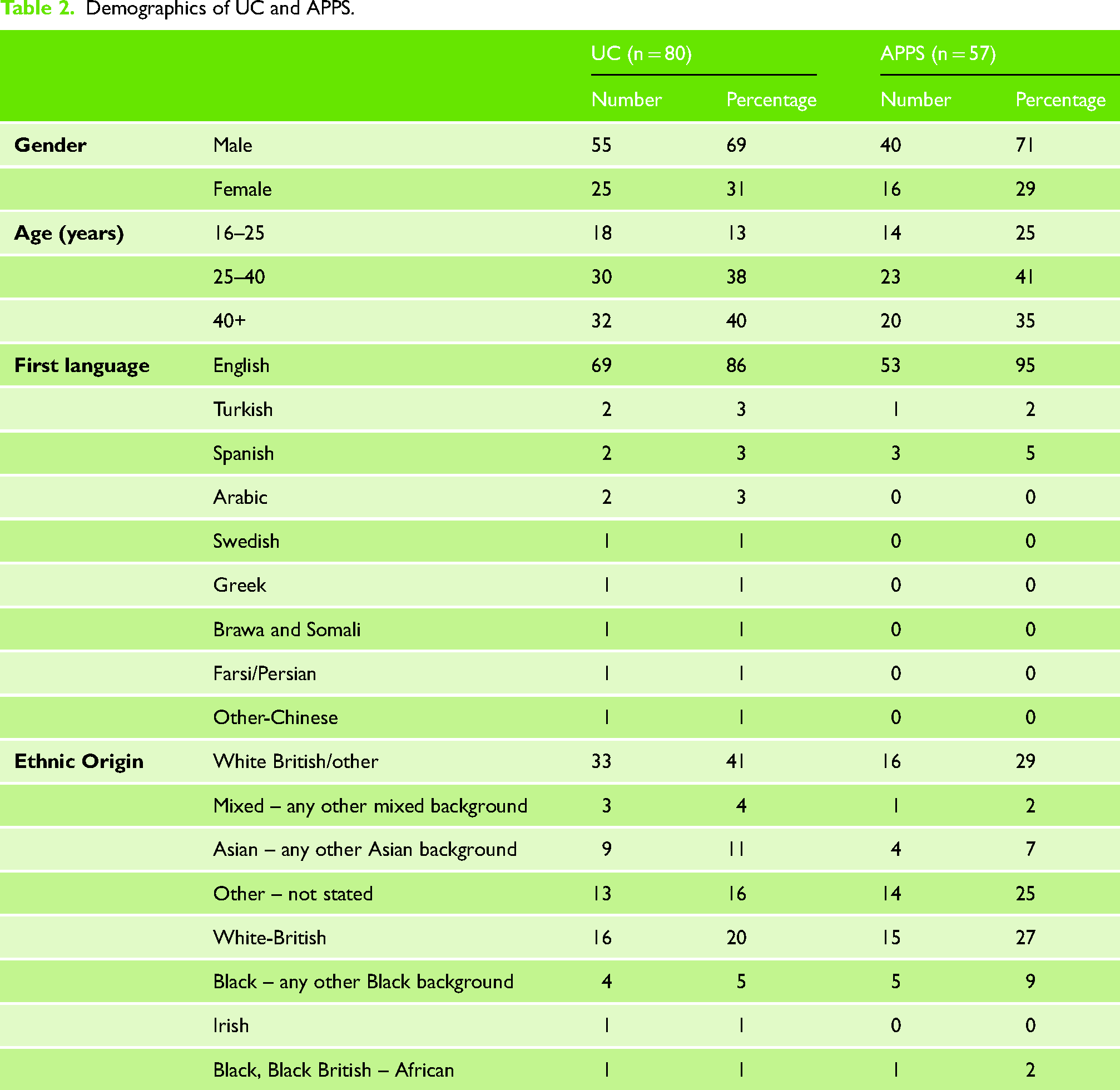
The percentage of patients in each age group varied between UC and APPS, with a higher percentage of patients under 40 years old in the APPS cohort. In both datasets most patients were male, English speakers and identified as white British or white British/other.
Fifty-seven percent of patients followed the planned pathway, through the new APP service. Forty-three percent of patients were reviewed in old, established clinics with an upper limb specialist. Process Map 1 shows the flow of patients through from A and E to first appointment, and outcome of first appointment. It is noted that patients could have had more than one outcome.
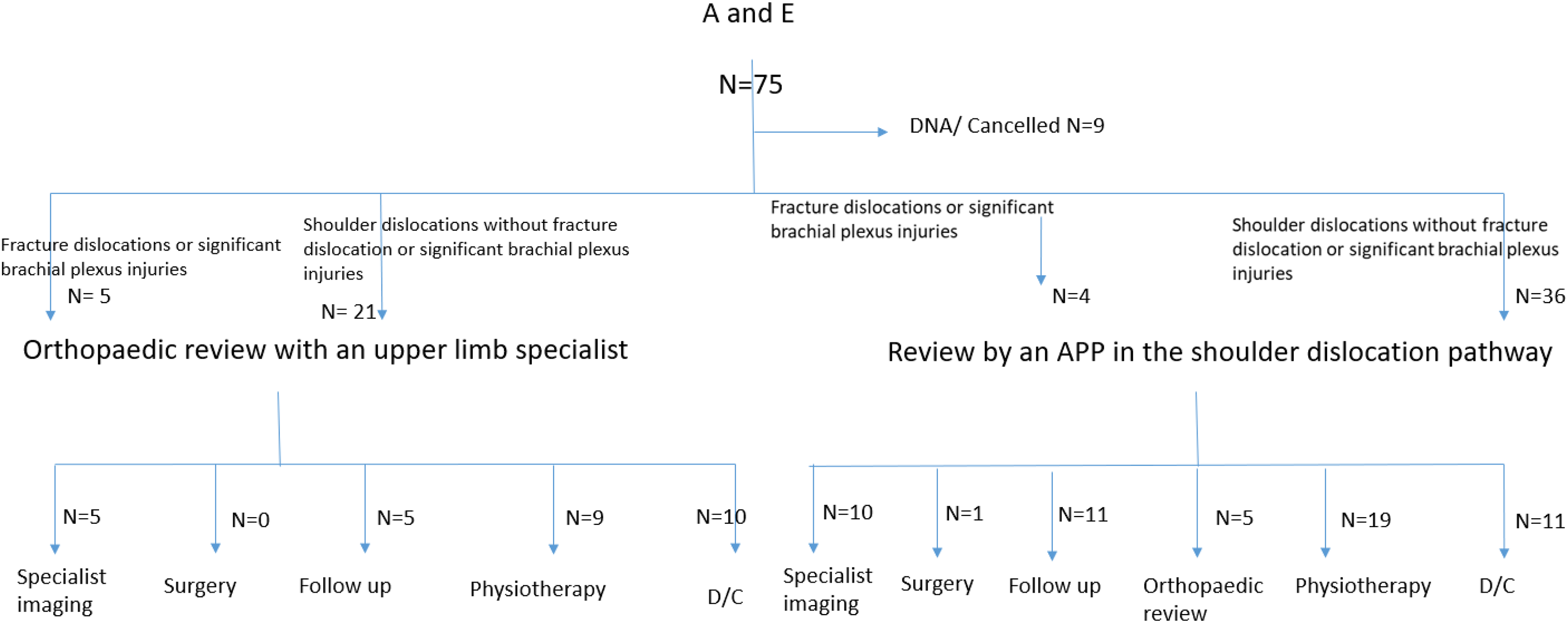
A process map to show patient flow through the whole service in 2023–2024.
The median wait time in days from A & E to first fracture clinic appointment decreased between datasets by 6 days.
In the APPS, all patients under 25 had first time review within 6 weeks, in UC one patient was reviewed outside of this time frame.
The percentage of patients in the different age cohorts with various outcome variables is displayed for APPS and UC.
Chart 1 demonstrates an increase in referral to physiotherapy, and an increase in imaging in the APPS in patients under 25.
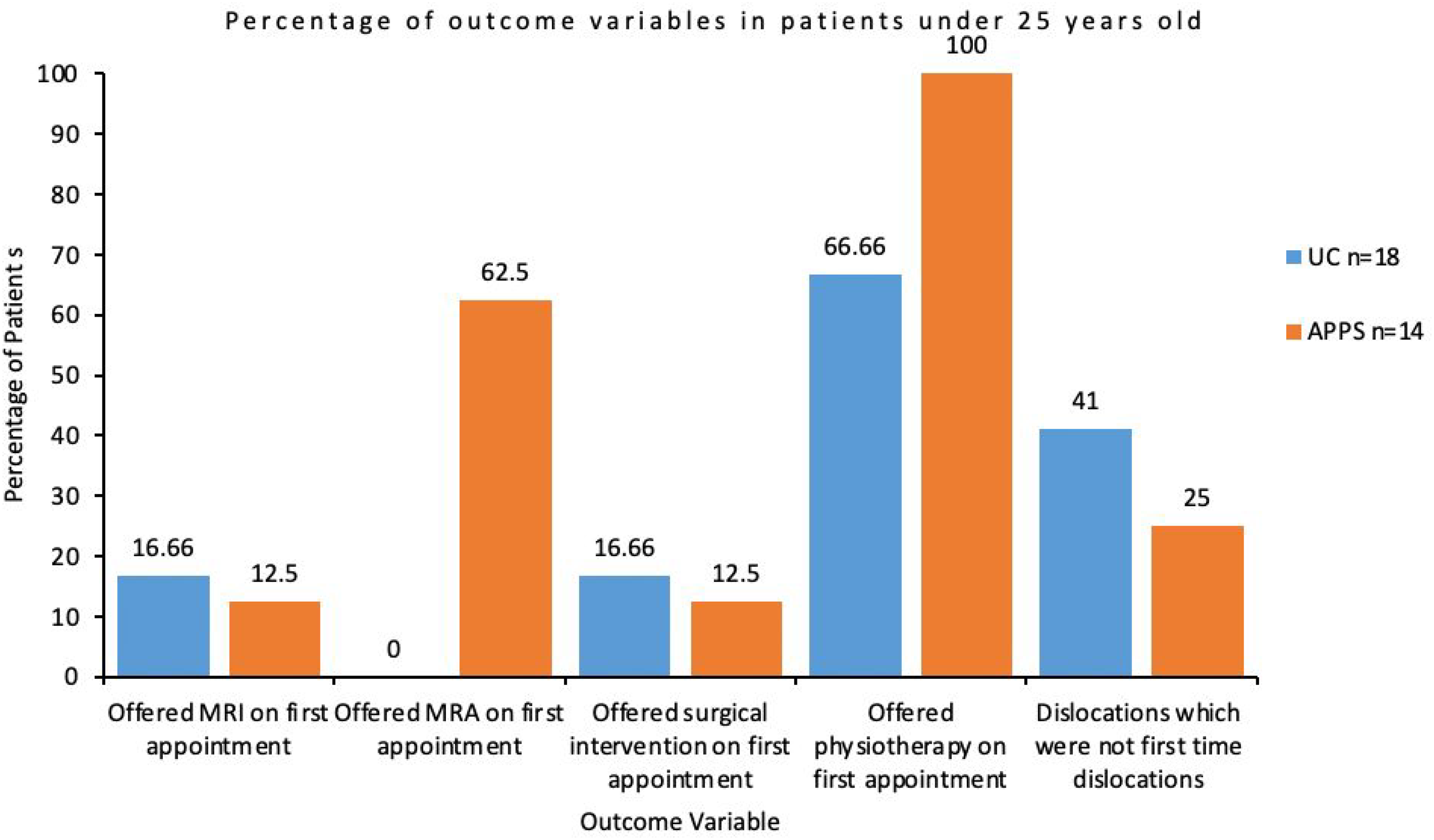
Percentage of appointment outcomes in patients under 25 years old.
Chart 2 shows an increase in patients assessed for ongoing instability, and for those offered specialist imaging in the APP cohort compared to the UC cohort, whereas referrals for surgical intervention and physiotherapy reduced in patients between 25 and 40 years old.
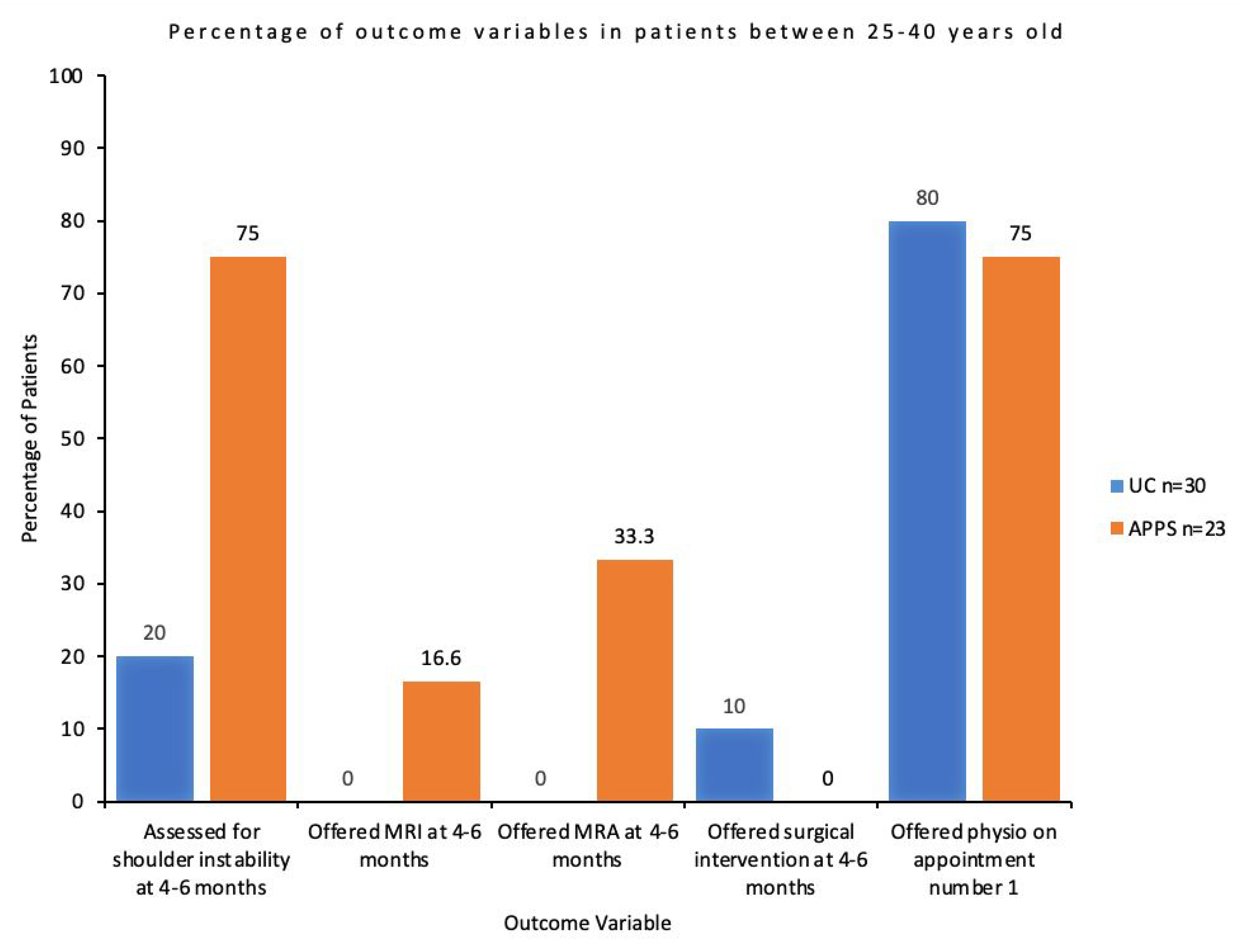
Percentage of appointment outcomes in patients between 25 and 40 years old.
Chart 3 shows an increase in patients offered imaging, referred to physiotherapy, and patients tested for rotator cuff weakness in the APP led clinic, with fewer patients referred for surgery in patients over 40 years old.
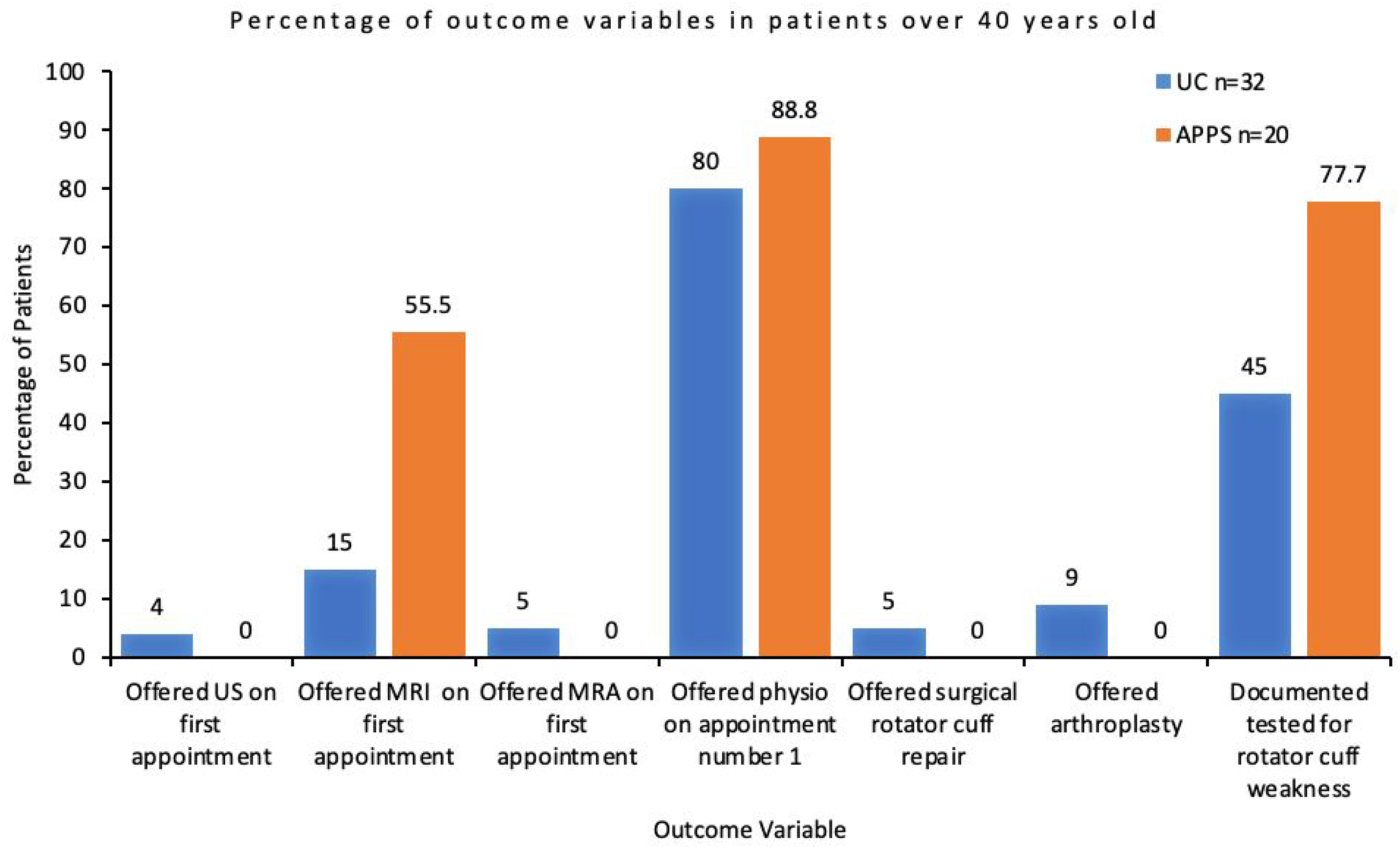
Percentage of appointment outcomes in patients over 40 years old.
Eighty-six percent of patients were treated conservatively in UC, and 98% in APPS.
Hundred percent of patients who responded were satisfied with the service. No patients were unsatisfied or ‘didn’t know’. Themes highlighted are visualised on thematic analysis map 1. And 30% of patients did not fill in the form and were not contactable after clinic.
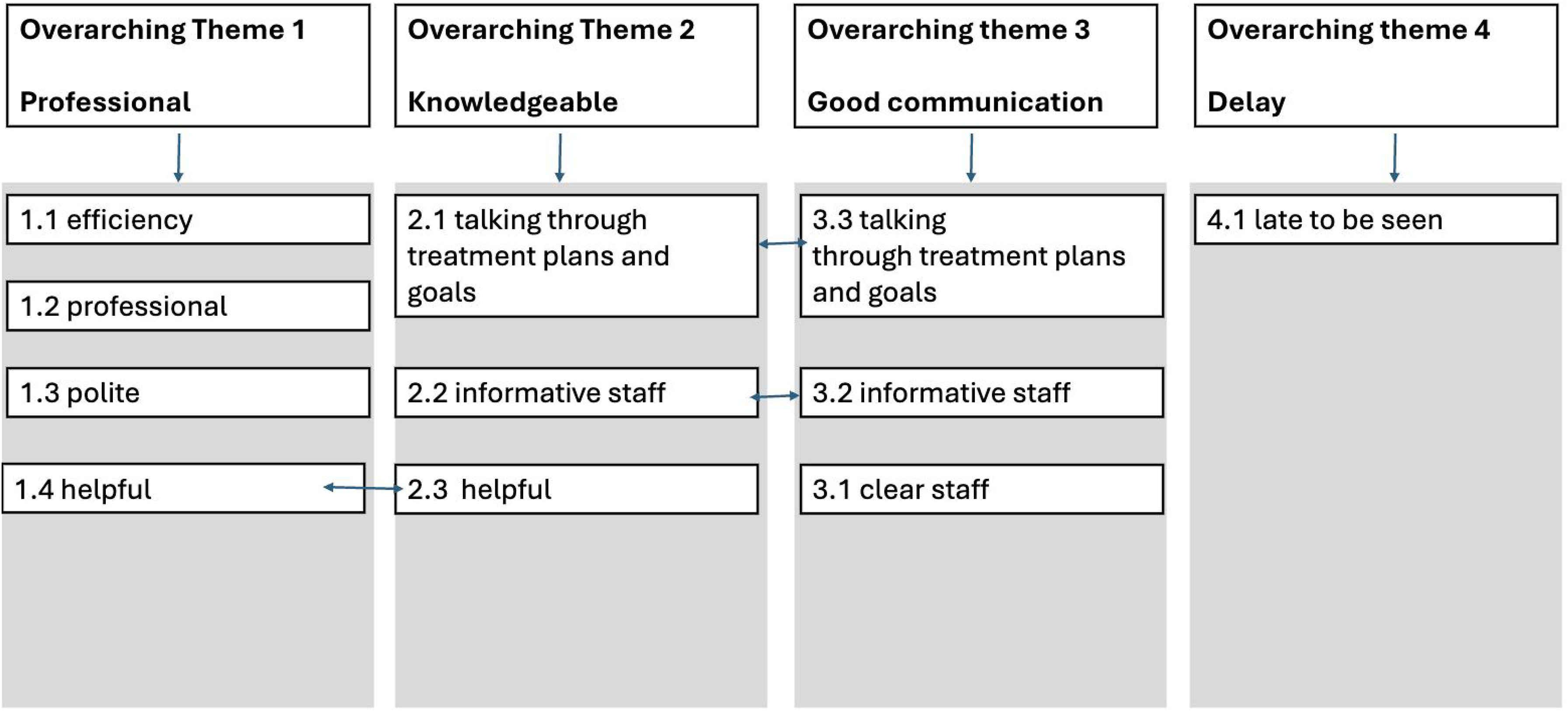
A thematic analysis map to visualise patient feedback.
Descriptive theme map 1: A descriptive theme map to visualise patient feedback
Key positive themes included knowledgeable, professional and communication. Time delay was highlighted as an area for improvement. Themes overlapped, for example helpful, informative staff and talking through treatment plans and goals.
Discussion
This service evaluation (SE) aimed to assess whether the APP-led clinic was being utilised as intended, while monitoring wait times, patient satisfaction and adherence to the BESS care pathway. The findings showed reduced wait times, high patient satisfaction and improved adherence to the care pathway. However, inconsistent utilisation of the clinic was noted, with patients referred to UC despite available capacity. Key findings and their relevance to clinical practice are discussed below.
With respect to objective 1, process map 1 highlights inconsistent pathway utilisation. Many eligible patients were referred to old, established clinics instead of the APP service, despite capacity, while some ineligible patients were referred to the APP service. Improving referral awareness or expanding criteria could better utilise capacity and increase uptake.
With respect to objective 2, for under-25 s, all patients in APPS were reviewed within 6 weeks, compared to all but one in UC. Patients under-25 have a significantly higher dislocation recurrence rate compared to older individuals and are more likely to develop chronic instability. 8 Early identification of instability can allow for timely imaging, and appropriate management. 5 In some cases, surgical stabilisation is indicated. 8 Timely review ensures relevant surgical candidates are identified early. This has been linked with improved surgical outcomes by minimising pre-operative recurrent instability.9,10 The pathway therefore met the 6 week review recommendation for patients under-25, 5 further data collection is indicated to identify whether this impacts post-operative outcomes.
Median wait time from A&E to the first appointment reduced from 19 (UC) to 13 days (APPS), aligning with the wider evidence base.11–14 While the clinical significance of a 6-day reduction is unclear, 4 minimising delays should remain a priority to facilitate timely surgical interventions. This is especially relevant when considering the evidence discussed on improved functional recovery and decreased re-tear rate following early rotator cuff repair. 15
With respect to objective 3, referral to physiotherapy increased in APPS in under-25s, reflecting improved pathway adherence. Early physiotherapy has been shown to reduce risk of recurrent instability, 8 thereby promoting quicker return to daily activities, work and sport 9 as well as decreasing the likelihood of post-traumatic osteoarthritis. 10 Increased referral to physiotherapy following the introduction of the APP led clinic, therefore may positively impact patient outcomes – further research would help clarify this.
For 25- to 40-year-olds, APPS showed increased imaging and assessment for instability symptoms, indicating improved pathway adherence. Appropriate imaging and assessment may allow for the identification of structural damage sustained during shoulder dislocation, 5 which can lead to repeat dislocations and functional impairment. 10 Identification of these risks therefore can improve patient outcomes by allowing suitable management plans to be formed.
In the over-40 cohort, early imaging increased from 15% to 55% in the APPS, though no patients were offered surgery. Early imaging may reduce delays to surgery by identifying repairable rotator cuff (RC) tears earlier. 5 Early repair of traumatic rotator cuff injuries can lead to better functional recovery, including improved range of motion and strength when compared to delayed repair. 16 Delayed surgery can also increase the risk of re-tear. 17
Surgical management remained low, supporting previous evaluations11–14 and justifying the APP's role in managing nonsurgical cases, potentially increasing capacity in the orthopaedic setting. 7
With respect to objective 4, patient satisfaction was high, consistent with previous findings 11 in APP specific studies. High patient satisfaction often correlates with improved pain relief and restored function in shoulder instabilty, 18 furthermore patient satisfaction is closely linked with psychological wellbeing, affecting factors such as anxiety and confidence in shoulder function. 19 Improving patient satisfaction throughout the entire patient pathway is therefore essential for optimum patient care.
Service limitations
The APP clinic faced disruptions from external factors such as doctor strikes and annual leave, potentially underrepresenting its effectiveness. Some referrals were misdirected to UC despite APP availability, while others outside inclusion criteria were referred to the APP clinic. Improving referral awareness or expanding criteria could better utilise capacity.
Methodological limitations
The SE's small sample size limited statistical analysis and broader applicability, with percentages used to describe data unlikely to reflect wider populations. Conducted at a single hospital with one APP, external validity is constrained, though findings align with existing evidence on APP services.7,11–14
Missing satisfaction questionnaires for 30% of APP pathway patients, despite follow-up efforts, means patient satisfaction data is incomplete and not fully representative. A more comprehensive understanding of patient feedback could have been achieved through semi-structured interviews, complimented by a rigorous analytical approach such as thematic analysis. 20
Other confounding factors include the SE measuring 6 months of data. This does not account for possible seasonal variation.
Data on whether the service decreased the time to surgery or impacted the number of orthopaedic and physiotherapy appointments offered would have been useful in measuring the impact of the service.
Conclusion
This service evaluation demonstrates that an APP-led clinic reduced waiting times, had high patient satisfaction, and enhanced adherence to the BESS care pathway in the management of shoulder instability, establishing that this pathway of care can be delivered by an APP. Key findings include improved early review of patients under-25, increased physiotherapy referrals, and improved appropriate early imaging across age groups, all of which likely contribute to better patient outcomes and more efficient care.
Challenges included inconsistent clinic utilisation highlighting an area for further improvement. Expanding awareness of referral criteria could enhance clinic effectiveness and optimise patient care. Future research with larger sample sizes and extended evaluation periods is recommended to validate these findings and explore the clinic's broader impact on shoulder instability management.
Supplemental Material
sj-pdf-1-sel-10.1177_17585732251377775 - Supplemental material for A service evaluation of a newly implemented Advanced Physiotherapy Practitioner led shoulder instability service
Supplemental material, sj-pdf-1-sel-10.1177_17585732251377775 for A service evaluation of a newly implemented Advanced Physiotherapy Practitioner led shoulder instability service by Amy Banning, Catharine Sian Macrae, Elizabeth Ratcliffe and Dana Maki in Shoulder & Elbow
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.