
Abstract
Background
Lower trapezius tendon (LTT) was increasingly used to restore external rotation in massive irreparable posterosuperior rotator cuff tears (PSRCTs), yet its performance remained unclear.
Methods
Following PRISMA 2020, PubMed, EMBASE, and Scopus were searched. Studies reporting ≥12-month outcomes after arthroscopically assisted LTT for irreparable PSRCTs were included; screened 259 records and retained 14 studies (433 shoulders) (PROSPERO CRD420251079171). Quality was assessed with MINORS and certainty with GRADE. Change scores for ER, FE, VAS, ASES, and Constant scores were pooled as standardized mean difference (SMDs); subgroup and leave-one-out analyses assessed heterogeneity, and publication bias was evaluated.
Results
ER improved +27.9° (SMD 1.80, 95% CI 1.35–2.25; I2 = 83.9%), FE +37.0° (SMD 1.10, 95% CI 0.73–1.47; I2 = 82.8%), VAS −4.2 (SMD −2.23, 95% CI −2.57 to −1.89; I2 = 72.7%), ASES +32.5 (SMD 1.95, 95% CI 1.35–2.54; I2 = 84.9%), and Constant +22.7 (SMD 1.63, 95% CI 1.27–1.98; I2 = 17.2%). Graft healing was 89.4% (9 studies; 317 shoulders; 80.6%–100%); complications occurred in 3.70%, reoperation in 3.46%, and conversion to reverse total shoulder arthroplasty in 2.08%.
Discussion
Arthroscopically assisted LTT improved motion, pain, and function with high graft-healing and low complication rates, with outcomes consistent across grafts and ages.
Level of evidence
Level IV; Meta-Analysis
Keywords
Introduction
Massive irreparable posterosuperior rotator cuff tears (PSRCTs) present a difficult clinical challenge, especially in active patients with minimal glenohumeral arthritis. 1 Reverse total shoulder arthroplasty (rTSA) is an effective option for cuff tear arthropathy, but it may not be optimal in younger patients or those without significant arthritis. 2
For patients with preserved joint space and subscapularis function, tendon transfer procedures have emerged as an important joint-preserving alternative.3–7 The latissimus dorsi tendon transfer (LDT), popularized by Gerber, has been used for decades to restore function in irreparable cuff tears, including older patients.8,9 However, LDT primarily augments elevation and is less predictable in restoring active external rotation (ER), particularly if the teres minor is compromised.8–11 The lower trapezius tendon transfer (LTT) is a newer technique that more closely restores external rotation by leveraging a muscle whose force vector is more anatomically aligned with shoulder external rotation.12–19 Originally described for paralytic shoulders (spinal accessory nerve or brachial plexus palsy), the LTT was later adapted to irreparable cuff tears using an Achilles tendon allograft as a bridge to the humerus.20–22
Biomechanical studies have shown that the transferred lower trapezius closely reproduces the line of pull of the infraspinatus and functions “in-phase” with native shoulder external rotators.23,24 Early clinical series by Elhassan et al. reported that LTT can substantially improve shoulder function and reduce pain in massive cuff tears, with particularly notable gains in external rotation.14,17 However, most reports remain small series or cohorts. Earlier systematic reviews underscored the biomechanical rationale and early outcomes of LTT but highlighted the paucity of high-level evidence, 25 and recent qualitative systematic reviews have since summarized post-LTT clinical outcomes for irreparable rotator cuff tears.26,27 None of these reviews, however, performed quantitative pooling with subgroup analyses, publication-bias assessment, or GRADE certainty rating; the present meta-analysis was undertaken to address these gaps.
This systematic review and meta-analysis of arthroscopically assisted LTT quantified pooled clinical outcomes for irreparable PSRCTs, addressing the PICO question: In adults with irreparable PSRCTs (Population), does LTT (Intervention), versus tendon-preserving alternatives or no control (Comparator), improve external rotation, pain, and function (Outcomes)? We hypothesized LTT would yield clinically meaningful improvements with acceptable graft-healing and complication rates, even among older patients with minimal arthritis.
Methods
Literature search
This review adhered to the PRISMA 2020 reporting guideline and was registered a priori with PROSPERO (CRD420251079171). 28 With a medical librarian, we developed database-specific strategies combining MeSH/Emtree headings and free-text terms for LTT transfer and irreparable rotator cuff tears. MEDLINE (via PubMed), Embase (Ovid), and Scopus were searched from inception to 15 April 2025, limited to English-language human studies. A sample PubMed query and full strategies for all databases are provided below (“lower trapezius transfer” [tiab] OR “lower trapezius tendon transfer” [tiab] OR (“lower trapezius” [tiab] AND transfer [tiab])) AND (“rotator cuff tear” [MeSH Terms] OR “rotator cuff tear” [tiab] OR irreparable [tiab] OR massive [tiab]). Equivalent syntax adapted for Embase (“lower trapezius transfer”/exp) and Scopus (TITLE-ABS-KEY) retrieved the same concept set. Reference lists of included articles and relevant reviews were hand-searched, and recent conference abstracts screened to mitigate publication bias. Searches yielded 552 records (PubMed 150, Embase 250, Scopus 152). After removing 293 duplicates in EndNote X9, 259 titles/abstracts were screened independently by two reviewers; 36 full texts were assessed, and 14 studies met criteria for quantitative synthesis (PRISMA flow diagram, Figure 1).
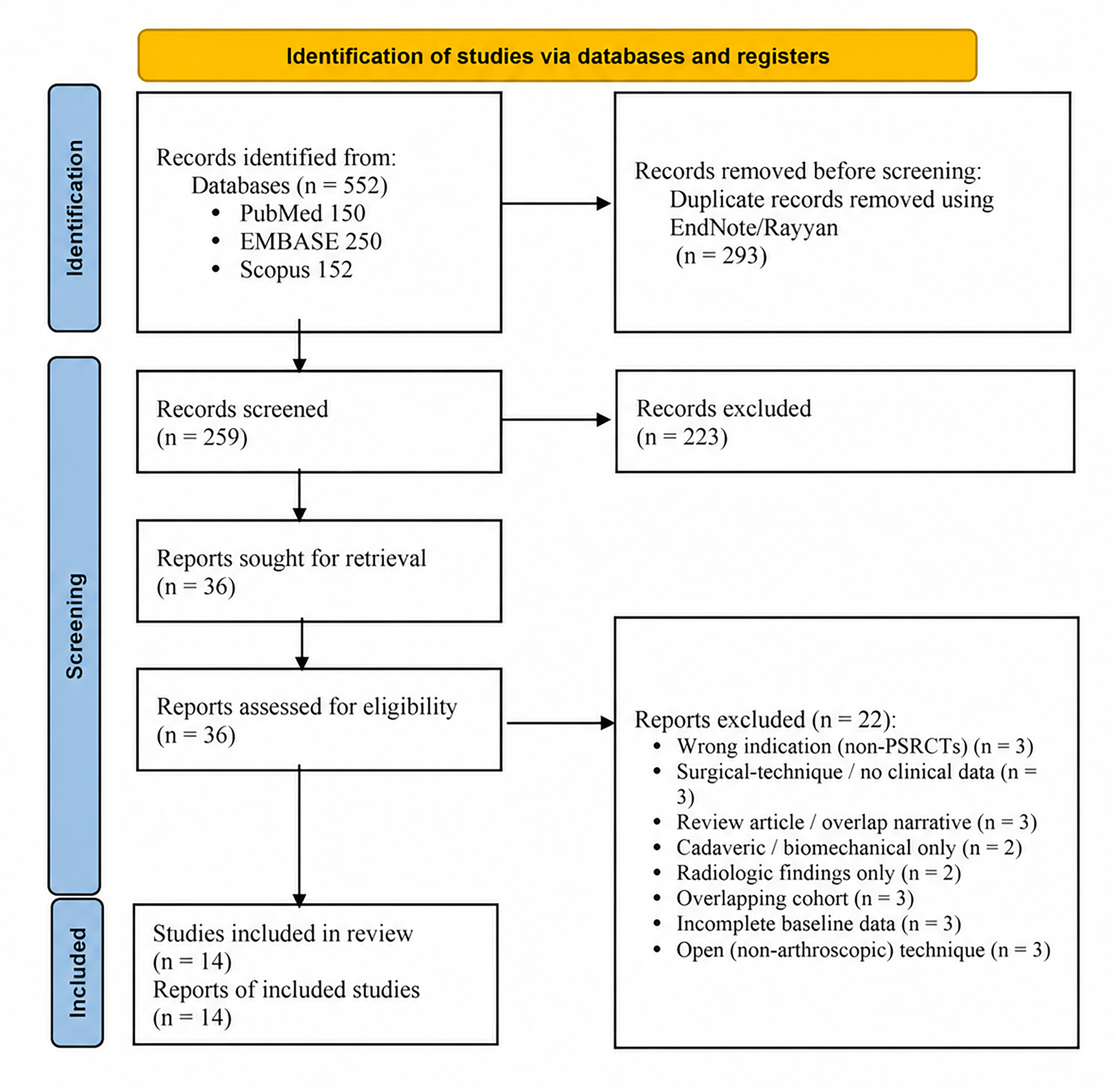
PRISMA 2020 flow diagram summarizing study identification, screening, eligibility assessment, and inclusion for the meta-analysis. Database searches yielded 552 records; after removal of 293 duplicates, 259 titles/abstracts were screened, 36 full-text articles were assessed, and 14 studies were included. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PSRCT, posterosuperior massive rotator cuff tear.
Inclusion and exclusion criteria
Eligible prospective or retrospective reports evaluated arthroscopically assisted LTT for massive, irreparable supraspinatus-infraspinatus tears confirmed intraoperatively or on imaging. Cohorts had intact or reparable subscapularis, minimal glenohumeral arthritis (Hamada ≤ 2), ≥12-month follow-up, and each study provided at least one clinical endpoint (range of motion, pain, or functional score). We excluded LTT for paralysis, open-only LTT series, papers pooling other transfers without discrete LTT data, and technical, cadaveric, or biomechanical articles lacking patient outcomes. Conference abstracts and trial registries were screened to reduce publication bias. For overlapping cohorts, the most recent or comprehensive dataset was retained.
Data extraction
Two reviewers independently extracted data with a piloted form; disagreements were resolved by discussion or, if needed, a third adjudicator. Recorded variables included study design/level, patient demographics, tear pattern, graft type, and stated rehabilitation. Key outcomes included pre- and postoperative shoulder range of motion (external rotation at the side and forward elevation [FE]), pain (visual analog scale [VAS] 0–10), and validated functional scores (ASES, Constant-Murley, Subjective Shoulder Value). Complications, adverse events, and structural results (graft healing on MRI or ultrasound) were also recorded. Complications were classified a priori as minor events (X), reoperations excluding arthroplasty (Y), and conversions to reverse shoulder arthroplasty (Z); categories were not mutually exclusive (see Table 1 footnotes). Where dispersion statistics were missing, a tiered imputation was applied. First, medians ± ranges were converted to means ± SDs using Hozo's method. 29 Second, if a mean difference and p-value (or t/F statistic) were supplied, the corresponding t value was derived to back-calculate the standard error (SE = Δ/t) and SD (SD = SE × √n). 30 Datasets that remained unconvertible were marked “not reported” and excluded from pooled calculations, minimizing bias while preserving maximal analyzable information. All extracted datasets were limited to cohorts undergoing arthroscopically assisted LTT.
Characteristics and clinical outcomes of included lower trapezius tendon transfer studies.
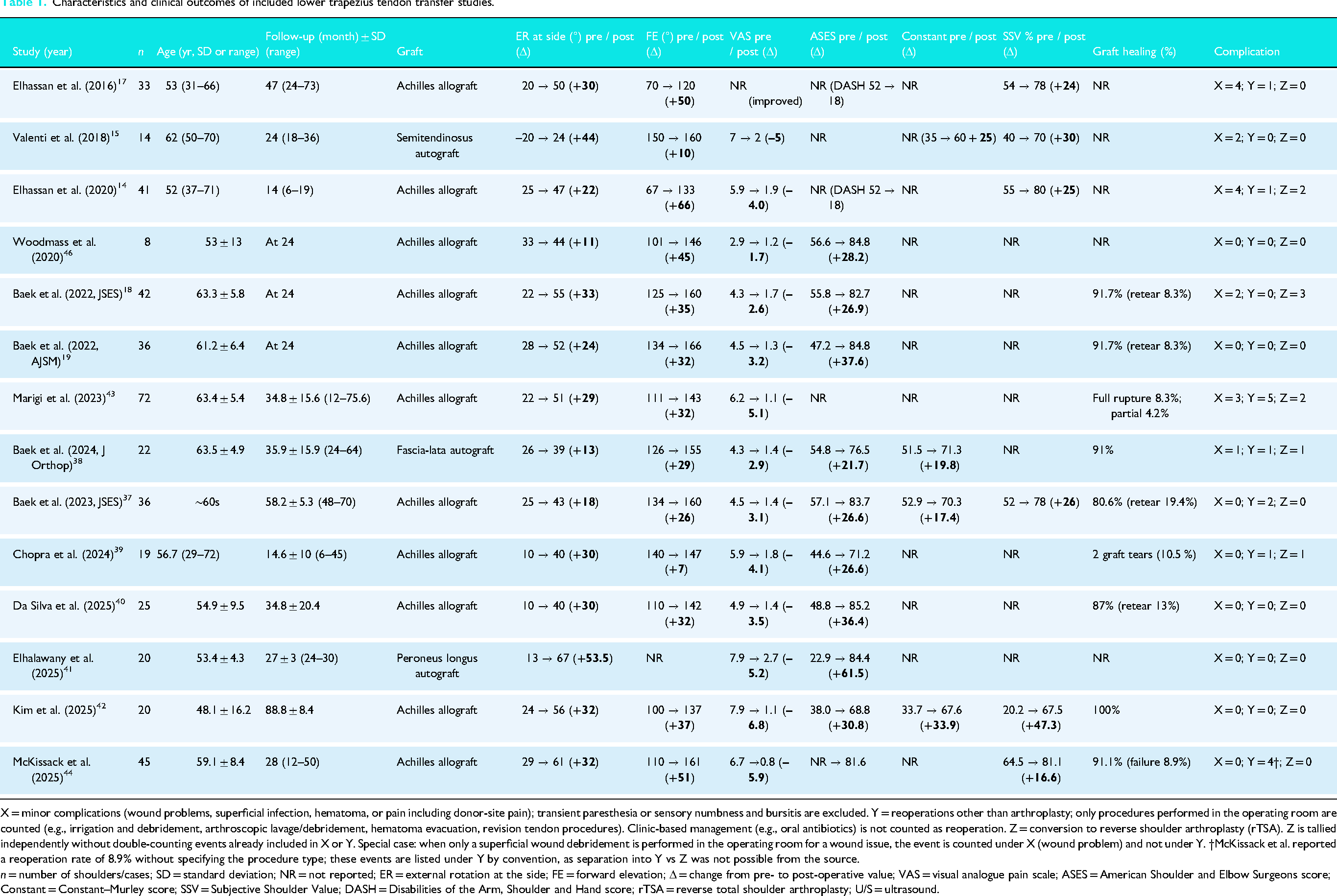
X = minor complications (wound problems, superficial infection, hematoma, or pain including donor-site pain); transient paresthesia or sensory numbness and bursitis are excluded. Y = reoperations other than arthroplasty; only procedures performed in the operating room are counted (e.g., irrigation and debridement, arthroscopic lavage/debridement, hematoma evacuation, revision tendon procedures). Clinic-based management (e.g., oral antibiotics) is not counted as reoperation. Z = conversion to reverse shoulder arthroplasty (rTSA). Z is tallied independently without double-counting events already included in X or Y. Special case: when only a superficial wound debridement is performed in the operating room for a wound issue, the event is counted under X (wound problem) and not under Y. †McKissack et al. reported a reoperation rate of 8.9% without specifying the procedure type; these events are listed under Y by convention, as separation into Y vs Z was not possible from the source.
n = number of shoulders/cases; SD = standard deviation; NR = not reported; ER = external rotation at the side; FE = forward elevation; Δ = change from pre- to post-operative value; VAS = visual analogue pain scale; ASES = American Shoulder and Elbow Surgeons score; Constant = Constant–Murley score; SSV = Subjective Shoulder Value; DASH = Disabilities of the Arm, Shoulder and Hand score; rTSA = reverse total shoulder arthroplasty; U/S = ultrasound.
Quality assessment
Methodological quality was appraised with the single-arm MINORS tool (max = 16) because all 14 eligible studies were non-randomized Level III–IV series. 31 Two reviewers independently scored each article and reconciled discrepancies by consensus; summary scores and inter-rater reliability appear in Results. Publication bias was assessed for outcomes with ≥ 10 studies by funnel-plot inspection, Egger's regression (intercept tested with a t distribution; df = k–2), and Duval–Tweedie trim-and-fill. For outcomes with fewer studies, Egger's regression was considered exploratory and reported only in the Supplement, without formal inference. 32
Statistical analysis
For each continuous endpoint, pre-to-post change scores were pooled as Hedges g standardized mean differences (SMDs). Mean changes in external rotation, FE, VAS pain, ASES, and Constant scores were extracted directly or, when missing, SDs were reconstructed from 95% CIs or p-values; if only medians ± ranges were provided, Hozo's method supplied estimates. 29 No dataset required Wan/Luo conversions. 33 When change-score SDs were absent and could not be reconstructed from other reported statistics, they were imputed with √(SDpre2 + SDpost2 – 2 r SDpre SDpost) assuming r = 0.50; sensitivity tests varying r from 0.25 to 0.75 shifted pooled effects by <3%, but we acknowledge that this correlation-based imputation remains an approximation. Random-effects models (DerSimonian–Laird) generated pooled SMDs with 95% CIs. 34 Heterogeneity was quantified with Cochran's Q and Higgins’ I2 statistics; consistent with the tentative adjectives proposed by Higgins et al., I2 values were classified as low (<25%), moderate (25–75%), or high (>75%), 35 acknowledging that the current Cochrane Handbook (Section 10.10.2) instead recommends overlapping interpretive bands (0–40%, might not be important; 30–60%, moderate; 50–90%, substantial; 75–100%, considerable) and that the importance of I2 ultimately depends on the direction and magnitude of effects. Prespecified robustness checks comprised graft-source and age subgroups plus leave-one-out influence analysis; results appear in Results. Publication bias was probed with funnel plots, Egger regression, and trim-and-fill. Evidence certainty followed the GRADE framework. All analyses were performed in RevMan 5.4; figures were redrawn in R 4.3.1 (metafor) and Python 3.10 (matplotlib) for high-resolution publication output. 36
Results
Search yield
The literature search and study selection process are summarized in the PRISMA flow diagram (Figure 1). In total, 14 studies met all eligibility criteria and were included in the quantitative synthesis (Table 1).14,17–19,37–46
Study characteristics and quality
The 14 included studies, comprising uncontrolled case series and comparative cohort studies, encompassed 433 shoulders and were published between 2016 and 2025. Sample size ranged from 8 to 72 (median 29). Weighted mean age was 58.3 years (study means 48.1–63.5 years) and overall cohorts spanned the mid-20s to late-70s; approximately 68% of participants were male. The patient-weighted mean follow-up was 33.4 months (range 12–89). All series enrolled massive, irreparable posterosuperior cuff tears (Goutallier ≥ 3) with an intact or reparable subscapularis and minimal glenohumeral arthritis (Hamada ≤ 2); 27–66% of shoulders had a prior failed repair, and several cohorts included pseudoparalytic patients. Table 1 summarizes cohort demographics, tear characteristics, and baseline outcomes. The median MINORS score was 12/16 (IQR 10–12), reflecting moderate methodological quality but inevitable limitations from the absence of randomization and control groups (Table S1). Δ values are reported for clinical interpretability, whereas SMDs are provided for pooled meta-analytic effect sizes; overlapping outcomes across supplementary tables reflect different analytical purposes.
Surgical technique
All 14 cohorts reported an arthroscopically assisted lower trapezius transfer. Among these, Valenti et al. (2018) and Elhalawany et al. (2025) both used a 4- to 6-cm posterior mini-open window to harvest the muscle. Maneuvers included glenohumeral/subacromial debridement, arthroscopic preparation of the greater-tuberosity footprint, open detachment of the lower trapezius from the scapular spine, and subdeltoid tunneling of a bridging graft to the tuberosity. A single-strand Achilles-tendon allograft bridged 377 of 433 shoulders (87.1%). The remaining 56 reconstructions relied on autografts: semitendinosus (n = 14), peroneus longus (n = 20), and fascia lata strips (n = 22). Greater-tuberosity fixation most often used a double-row suture-anchor construct (8 studies); the remaining studies either employed single-row techniques or did not report the specific configuration. Several series documented a concomitant subscapularis repair when torn, while most other cohorts either had intact subscapularis tendons by inclusion criteria or did not report specific management. Postoperative care was similar: 6 to 8 weeks of immobilization at 30° to 45° abduction and 10° to 30° external rotation, passive motion from week 6, graded active motion by weeks 8–10, and deltoid–trapezius strengthening after month 3.
Clinical outcomes
Range of motion
Thirteen of the 14 studies reported postoperative ranges, and 12 provided extractable change data for external rotation (ER). The patient-weighted mean increase in ER was 27.9° (standardized mean difference [SMD] 1.80, 95% CI 1.35–2.25; I2 = 83.9%; Q = 68; p < 0.001). Forward elevation improved by 37.0° (SMD 1.10, 95% CI 0.73–1.47; I2 = 82.8%; Q = 70; p < 0.001). Forest plots of ER and FE improvement are shown in Figure 2. Absolute postoperative ER ranged from 24° to 67°. Heterogeneity in FE gains arose chiefly from baseline disparities: cohorts starting below 90° gained >45°, whereas those beginning near 150° showed only maintenance (+10°). No study documented loss of elevation.
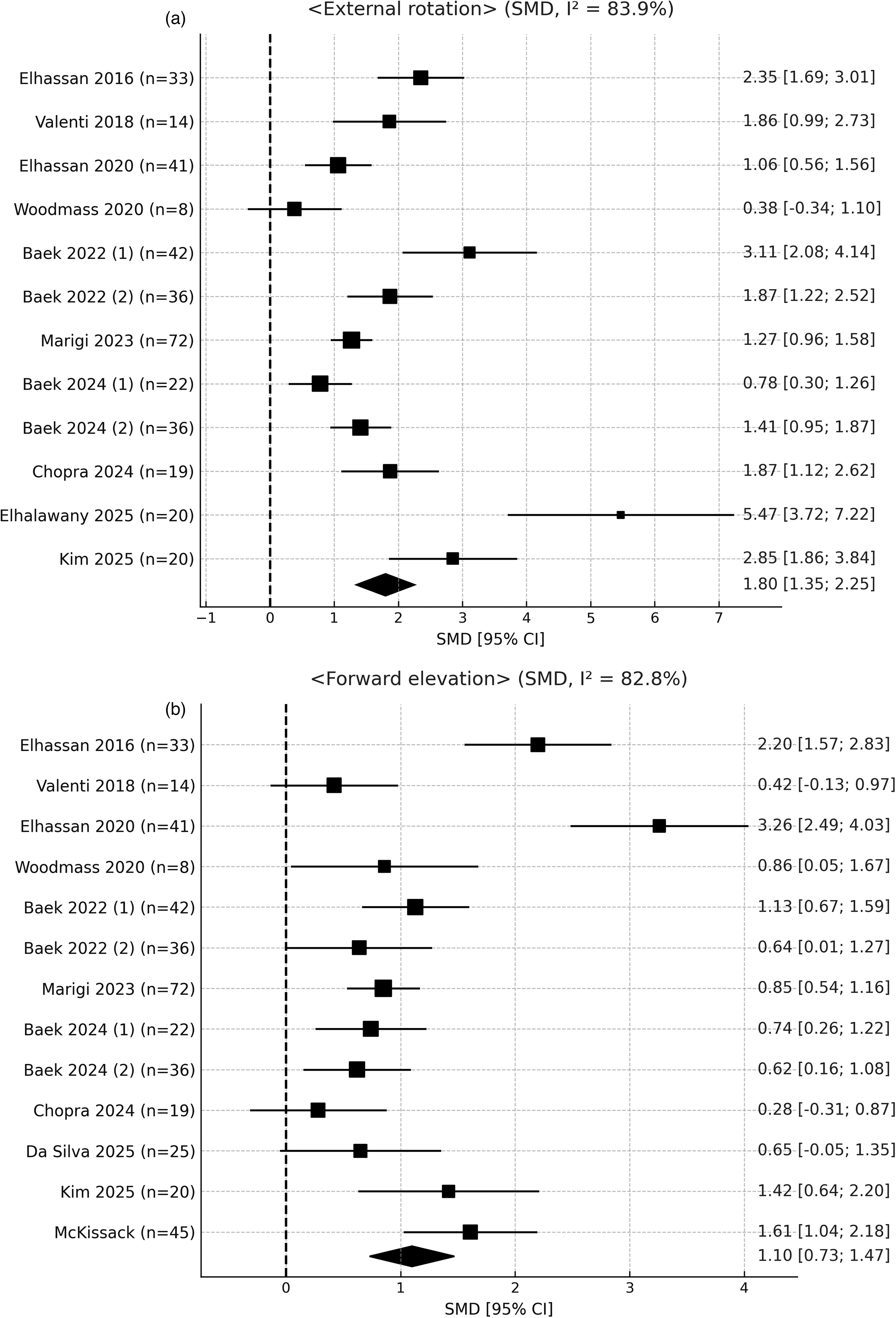
Forest plots of standardized mean differences (SMDs) after arthroscopic lower trapezius transfer (LTT). (a) External rotation (ER): study-specific SMDs are displayed as squares scaled to inverse-variance weight; horizontal bars denote 95% confidence intervals (CIs); the diamond represents the pooled random-effects estimate (SMD = 1.80, 95% CI 1.35–2.25). Heterogeneity: I2 = 83.9%. (b) Forward elevation (FE): pooled random-effects estimate SMD = 1.10 (95% CI 0.73–1.47) with I2 = 82.8%. SMD: standardized mean difference; CI: confidence interval; I2: Higgins heterogeneity statistic.
Pain and function
Pain scores were pooled from 13 cohorts. Baseline VAS averaged 2.9–7.9/10 and declined to 0.8 to 2.7, yielding a weighted Δ = –4.2 points (SMD −2.23, 95% CI −2.57 to −1.89; I2 = 72.7%; Q = 44; p < 0.001), as shown in Figure 3(a). Functional metrics improved substantially: ASES improved 32.5 points (SMD 1.95, 95% CI 1.35–2.54; I2 = 84.9%; Q = 53, p < 0.001), while the Constant–Murley score rose 22.7 points (SMD 1.63, 95% CI 1.27–1.98; I2 = 17.2%; Q = 4; p = 0.31), depicted in Figure 3(b) and (c). Subjective Shoulder Value increased by approximately 17 to 47 percentage points (e.g., from 30–40% to 60–80%). Two included cohorts explicitly reported postoperative external-rotation lag-sign resolution or reversal (Valenti, 2018; Chopra, 2024): Valenti 2018 reported postoperative negativity of the lag/drop signs in all 14 patients with positive preoperative lag signs, and Chopra 2024 reported reversal in all 15 patients with a preoperative external-rotation lag sign (out of a total cohort of 19); the remaining cohorts either reported active external rotation in degrees or recorded the lag sign only as a preoperative characteristic or selection variable, precluding a pooled estimate across all included studies.
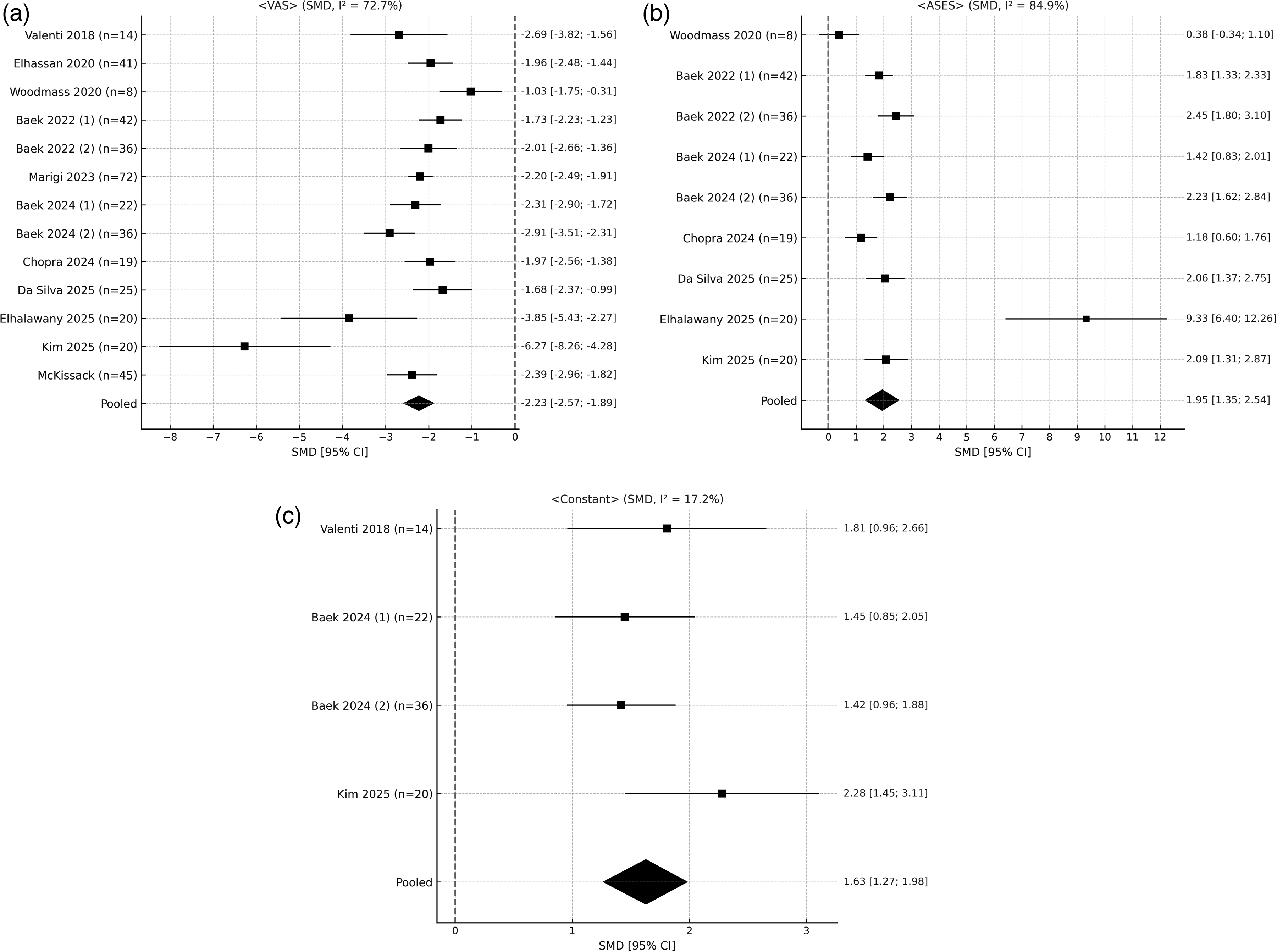
Forest plots of standardized mean differences (SMDs) in patient-reported outcome measures after arthroscopic lower trapezius transfer (LTT). (a) Pain on the 0–10 visual analog scale (VAS): study-specific SMDs are displayed as squares scaled to inverse-variance weight; horizontal bars denote 95% CIs; the diamond represents the pooled random-effects estimate (SMD = −2.23, 95% CI −2.57 to −1.89). Heterogeneity: I2 = 72.7%; negative values indicate pain reduction. (b) American Shoulder and Elbow Surgeons (ASES) score: pooled random-effects SMD = 1.95 (95% CI 1.35–2.54) with I2 = 84.9%. (c) Constant–Murley score: pooled random-effects SMD = 1.63 (95% CI 1.27–1.98) with low heterogeneity (I2 = 17.2%). SMD: standardized mean difference; CI: confidence interval; I2: Higgins heterogeneity statistic; VAS: visual analog scale; ASES: American Shoulder and Elbow Surgeons score.
Structural healing and complications
Routine postoperative imaging was reported in 9 of the 14 studies (317 shoulders). The weighted graft-healing rate was 89.4% (study range 80.6%–100%). All documented failures occurred at the greater tuberosity fixation site; no report described detachment from the scapular origin. Three cohorts quantified acromiohumeral distance: two demonstrated a mean increase of +1.2 mm, whereas Baek et al. 38 (2024, J Orthop) noted a minor decrease (–0.4 mm). Across individual series, superficial wound complications were reported in 0% to 13% of cases and infections in 0% to 6%; the pooled minor-complication rate was 3.70%. Donor-site hematomas were confined to hamstring- or fascia lata-harvesting autografts. No spinal-accessory nerve palsies or deltoid detachments were reported. Reoperation was required in 3.46% of cases—predominantly infection irrigation and debridement or revision tendon procedures—and conversion to rTSA in 2.08%.
Sensitivity and sub-group analyses
Removing the comparative cohorts left 11 single-arm series; the patient-weighted gains remained nearly identical to the primary analysis (ER +27.9°, ASES +32.5 points). Subgroup pooling showed that graft source did not influence motion: Achilles allograft yielded a mean ER gain of +27.0° versus +32.0° with autograft (p = 0.46). Age stratification (≤ 60 vs > 60 years) likewise revealed no meaningful differences in ER, FE, VAS, or ASES (p ₍interaction₎ = 0.64 for ER, 0.08 for FE, 0.30 for VAS, and 0.25 for ASES; Table S2). Leave-one-out testing confirmed robustness: removing any single study shifted the pooled estimate between 1.62 and 1.92 for ER, 1.71 and 2.11 for ASES, −2.12 to −2.31 for VAS, 1.49 to 1.78 for Constant, and 0.94 to 1.17 for FE (Table S3).
Risk-of-bias, publication bias, and evidence certainty
The weighted MINORS score was 12 / 16 (interquartile range 10–12), reflecting moderate methodological quality. Limitations stemmed from retrospective data collection, variable follow-up, and the absence of randomized controls, whereas strengths included clearly defined eligibility criteria and validated outcome measures in nearly every cohort. Frequent shortcomings reflected typical surgical case series: lack of control cohorts, retrospective data capture, limited follow-up, and variability in graft type and rehabilitation. No study incorporated randomization or blinding, so selection, performance, and detection bias cannot be excluded despite moderate MINORS scores. Publication bias was examined visually. Despite substantial heterogeneity (I2 = 83.9%), Egger's test for ER revealed small-study effects (intercept = 4.235, p = 0.012; see Table S4). FE (p = 0.225) and VAS (p = 0.177) showed no asymmetry, and ASES (p = 0.076) and Constant (p = 0.145) likewise did not demonstrate significant asymmetry. Duval and Tweedie's trim-and-fill procedure (random-effects, DerSimonian–Laird) imputed 2–8 potentially missing studies (Table S4), and the adjusted pooled effect sizes changed by ≤ 0.26 compared with the observed estimates. These minimal differences indicate that potential publication bias is unlikely to have meaningfully affected the meta-analytic conclusions. Although selective reporting bias cannot be excluded, the directionally consistent and clinically important improvements observed across all cohorts bolster the robustness of the findings. According to GRADE, evidence certainty was very low for ER (12 studies), FE (13 studies), VAS (13 studies), and ASES (9 studies), and low for the Constant–Murley score (4 studies) (Table S5).
Discussion
This meta-analysis, devoted exclusively to LTT for irreparable PSRCT, demonstrates substantial functional benefits. Pooled data indicate mean gains of 27.9° in external rotation, 37.0° in FE, an increase of 32.5 points in ASES, and 22.7 points in Constant–Murley, all exceeding accepted MCIDs.47,48
The biomechanical effectiveness of LTT primarily results from its anatomical suitability for restoring function in massive cuff tears.23,24 The lower trapezius closely mirrors the native infraspinatus in both vector alignment and excursion, effectively reestablishing the posterior force couple and stabilizing the humeral head within the glenoid. Biomechanical studies have confirmed that inserting the LTT at the infraspinatus footprint on the greater tuberosity generates substantial ER and abduction moment arms, more closely replicating natural cuff function when compared to traditional LDT. 24
In contrast, LDT transfers a muscle–tendon unit that is not synergistic with the native external rotators and therefore typically requires postoperative cortical retraining to achieve effective external rotation function. 49 Consequently, external rotation improvements after LDT are inconsistent, with many patients exhibiting persistent ER lag, especially if the teres minor is compromised. 10
An increasing number of clinical series from high-volume, fellowship-trained shoulder surgeons suggest that LTT is a reproducible surgical technique that yields more predictable outcomes and consistent functional improvements. 50 However, arthroscopically assisted LTT is technically demanding, and reproducibility is likely to depend on the learning curve, institutional volume, and surgeon background in arthroscopic and open shoulder reconstruction; these factors should be acknowledged when extrapolating our findings to lower-volume settings. Baek et al. reported that LTT increased external rotation by approximately 28 degrees, exceeding the 10 to 15 degree improvement seen after LDT. 18 Recent comparative studies and systematic reviews have demonstrated superior pain relief and functional outcomes with LTT compared with LDT. 51 Furthermore, biomechanical studies show that LTT contracts in phase with native cuff muscles, whereas the transferred latissimus dorsi is activated out of phase during elevation, limiting its mechanical efficiency.52,53
Superior capsular reconstruction (SCR) is another joint-preserving approach for irreparable cuff tears.54,55 SCR stabilizes the glenohumeral joint by preventing superior migration but does not actively restore muscular function.19,56,57 A meta-analysis of 18 SCR cohorts (637 shoulders) found forward elevation to improve by 40 degrees (from 113° to 153°) and the ASES score by 33 points (from 48 to 81). 58 External rotation increased only 8 degrees, from 35 to 43, reflecting the uncorrected external rotation deficit. 58 Consequently, LTT is favored for younger active patients with external-rotation loss, whereas the less invasive SCR suits older patients with limited functional demands.50,59 Within this treatment spectrum, current algorithms typically reserve LTT for patients with massive irreparable posterosuperior tears, preserved glenohumeral cartilage (Hamada ≤ 2), an intact or reparable subscapularis, and a clinically meaningful ER lag. By contrast, patients with advanced arthritis or poor deltoid function are generally directed toward reverse shoulder arthroplasty, whereas those with pain but preserved active motion may be candidates for debridement or SCR. These principles align with the inclusion criteria of the cohorts synthesized in our meta-analysis and provide a practical framework for case selection. In addition, similar to rotator cuff repair, physiologic and nutritional optimization (e.g. smoking cessation, glycemic control, and attention to overall musculoskeletal health) should be considered when planning tendon transfer, although these patient-level factors could not be evaluated in our pooled analysis because they were rarely reported in the primary studies. Emerging reports describe combined or staged strategies, such as performing SCR first and subsequently adding a tendon transfer; however, rigorous comparative studies are still required to define the optimal indications and sequencing for these approaches.60,61
Successful tendon transfer depends on both clinical outcomes and biological healing of the transferred tendon. 17 The studies in this review showed high graft integrity on postoperative imaging. In cohorts that used routine MRI or ultrasound, graft continuity was maintained in 89.4% of shoulders (9 studies; 317 shoulders), with individual study rates ranging from 80.6% to 100% (Table 1). Baek et al. 37 recorded 80.6% healing with an Achilles tendon allograft, and Chopra et al. 39 confirmed 90% continuity at 12 months. Kim et al. 42 notably reported a 100% graft healing rate in younger patients (mean age 48 years) at a mean follow-up of 7.4 years. These rates equal or surpass those of SCR, which preserves graft integrity in 80% to 85% of shoulders at 2 years, and are comparable to those of LDT, although direct comparison is hampered by inconsistent imaging protocols in LDT studies.9,58,62 Notably, most observed graft failures occurred within the first postoperative year and were usually linked to discrete trauma or premature return to overhead activity.
Regarding complications, LTT showed an overall minor-complication rate of 3.70% (Table 1, 433 shoulders). Most events were superficial wound issues or minor infections and resolved with local care; one deep infection led to arthrodesis. 17 Other postoperative infections occurred in 2% to 3%, matching rates for comparable graft procedures. Nerve injury was very rare; unlike latissimus dorsi transfer, LTT spares the thoracodorsal nerve and protects the spinal accessory nerve during distal dissection.7,12 Donor-site morbidity was minimal, and no scapular dyskinesis, spinal accessory palsy, neurologic injury, deltoid detachment, or acromial fracture were observed. 12 Reoperation, usually revision transfer, was needed in 3.46%, and conversion to reverse shoulder arthroplasty in 2.08%, figures broadly comparable to those for SCR and latissimus dorsi transfer.
Our exploratory analysis suggests that patient age may modulate clinical outcomes after LTT, although the available evidence is limited and hypothesis-generating. Age-stratified subgroup analyses (≤ 60 y vs > 60 y; 7 studies for ER, 8 for FE, 7 for VAS, and 5 for ASES) showed no statistically significant interactions (p_interaction = 0.64 for ER, 0.08 for FE, 0.30 for VAS, and 0.25 for ASES); we therefore did not detect a quantitative age × treatment effect at the study level. Biological age and activity level plausibly influence tendon healing and functional recovery, and prior work on LDT indicates that preoperative teres minor integrity and subscapularis function are also critical determinants of postoperative external rotation. Although most included LTT cohorts required an intact or reparable subscapularis, teres minor status and detailed baseline strength were incompletely reported across studies, and we could not quantify their independent impact on outcomes. Given the absence of a statistically significant age × treatment interaction in our subgroup analysis, an age-based recommendation cannot be supported by our pooled data alone; however, in selected older individuals with advanced cuff arthropathy (Hamada ≥ 3) or limited functional demand, reverse shoulder arthroplasty may be preferable, with the decision driven by cuff and joint status rather than by chronological age. This should not be generalized to all older patients, since posterior cuff and subscapularis status, rather than chronological age, are likely the dominant determinants of outcome. In younger and active patients with confirmed irreparability of the posterosuperior cuff but preserved glenohumeral cartilage (Hamada ≤ 2) and intact or reparable subscapularis—and for whom primary cuff repair is not achievable—LTT may be considered as a joint-preserving option that may delay or avoid the need for arthroplasty.7,50
Graft type showed minimal influence on postoperative recovery. Allografts—primarily Achilles tendon in 377 shoulders—accounted for 87.1% of the 433 reconstructions. The remaining 56 used autografts: semitendinosus (n = 14), peroneus longus (n = 20), and fascia lata strips (n = 22). Subgroup pooling showed no meaningful difference: external-rotation gain averaged 27.0° with allograft versus 32.0° with autograft (interaction p = 0.46), while ASES score improved 32 versus 37 points, respectively. Complication rates were comparable (3.83% [95% CI 2.3–6.2%] vs 5.36% [95% CI 1.8–14.6%]; Fisher's exact p = 0.48). Given the observational design and marked size imbalance, evidence certainty is low; graft selection should be guided by surgeon preference, availability, and cost rather than the expectation of superior outcomes. 25 Baseline forward elevation appeared to influence postoperative gains; based on descriptive data extracted from Table 1, shoulders with preoperative FE < 90° improved by approximately 46°, whereas those starting near 150° improved by about 10°.
Limitations
This review has limitations. Most included studies were small, uncontrolled Level III–IV cohorts, predominantly retrospective case series, with short- to mid-term follow-up and heterogeneous outcome sets. No Level I or II trials have directly compared lower trapezius transfer with alternative procedures. The median sample size per study was 29 shoulders (range 8–72), so our pooled estimates are driven by multiple underpowered cohorts rather than large prospective registries. In the absence of true controls, placebo effects or structured rehabilitation may have contributed to improvements, although the magnitude and consistency of benefit suggest nonoperative care alone is unlikely to achieve similar results. Statistical heterogeneity was substantial (I2: ER 83.9%, FE 82.8%, VAS 72.7%, ASES 84.9%, Constant 17.2%). Leave-one-out analyses indicated that no single study disproportionately influenced the pooled estimates, implying variation in effect size rather than direction. Despite the use of random-effects modeling and prespecified subgroup analyses, residual heterogeneity likely reflects differences in surgical technique, rehabilitation protocols, baseline function, prior surgery, and the status of the teres minor and subscapularis. Because these variables were inconsistently reported, detailed stratified analyses could not be performed, and the pooled values should be interpreted as average effects that may not predict outcomes in any individual patient. Outcome reporting was inconsistent: only four studies reported Constant scores, three assessed strength, and nine evaluated graft healing with imaging, limiting secondary analyses and precluding robust meta-regression of clinical outcomes according to follow-up duration or imaging-confirmed graft healing. Publication bias is possible, as suggested by an Egger intercept of 4.235 for ER (p = 0.012). Future research should adopt prospective comparative designs, longer follow-up, standardized imaging protocols, and detailed baseline stratification. Although overall certainty is low, the consistent and clinically meaningful improvements observed support consideration of lower trapezius transfer for appropriately selected patients.
Conclusion
Arthroscopically assisted LTT transfer appears to preserve shoulder function in selected patients with massive irreparable posterosuperior cuff tears, providing clinically meaningful improvements in motion, pain, and patient-reported function with high graft integrity and a low complication burden. These findings support LTT as a viable joint-preserving option in patients in whom primary cuff repair is not achievable and reverse shoulder arthroplasty is not yet indicated. Long-term comparative trials, uniform imaging protocols, and refined graft and patient selection will be required to optimize indications and refine technique.
Supplemental Material
sj-docx-1-sel-10.1177_17585732261455827 - Supplemental material for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears
Supplemental material, sj-docx-1-sel-10.1177_17585732261455827 for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears by Chang Hee Baek, Jung Gon Kim, Bo Taek Kim and Chaemoon Lim in Shoulder & Elbow
Supplemental Material
sj-docx-2-sel-10.1177_17585732261455827 - Supplemental material for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears
Supplemental material, sj-docx-2-sel-10.1177_17585732261455827 for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears by Chang Hee Baek, Jung Gon Kim, Bo Taek Kim and Chaemoon Lim in Shoulder & Elbow
Supplemental Material
sj-docx-3-sel-10.1177_17585732261455827 - Supplemental material for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears
Supplemental material, sj-docx-3-sel-10.1177_17585732261455827 for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears by Chang Hee Baek, Jung Gon Kim, Bo Taek Kim and Chaemoon Lim in Shoulder & Elbow
Supplemental Material
sj-docx-4-sel-10.1177_17585732261455827 - Supplemental material for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears
Supplemental material, sj-docx-4-sel-10.1177_17585732261455827 for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears by Chang Hee Baek, Jung Gon Kim, Bo Taek Kim and Chaemoon Lim in Shoulder & Elbow
Supplemental Material
sj-docx-5-sel-10.1177_17585732261455827 - Supplemental material for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears
Supplemental material, sj-docx-5-sel-10.1177_17585732261455827 for The meta-analysis and systematic review of arthroscopic lower trapezius tendon transfer for massive irreparable rotator cuff tears by Chang Hee Baek, Jung Gon Kim, Bo Taek Kim and Chaemoon Lim in Shoulder & Elbow
Footnotes
Acknowledgments
The authors extend their gratitude to Seung Jin Kim, Sung Hak Choi, and Seung Hwan Oh, who served as research coordinators and provided valuable assistance in collecting clinical and statistical data.
Acknowledgments
The authors extend their gratitude to Seung Jin Kim, Sung Hak Choi, and Seung Hwan Oh, who served as research coordinators and provided valuable assistance in collecting clinical and statistical data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study is a meta-analysis based solely on previously published data and does not involve new human or animal subjects
Trial Registration
PROSPERO (CRD420251079171).
Guarantor
Chang Hee Baek, MD (corresponding author).
Contributorship
Chang Hee Baek and Jung Gon Kim contributed equally to this work. All authors contributed to study conception/design, study selection and data extraction, and manuscript drafting and critical revision. All authors approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.