
Abstract
Background
Cementless reverse shoulder arthroplasty (RSA) with percutaneous locking screw fixation is an increasingly utilized option for treatment of proximal humerus fractures. The safety of percutaneous screw placement in the humerus has not been well established. This study aims to evaluate the proximity of the axillary and radial nerves to percutaneous screw trajectories in RSA.
Methods
A humeral fracture stem with percutaneous locking screws was implanted into six male cadaveric specimens. Screw holes were over-drilled, and distances from trocars and drill bits to the axillary and radial nerves were measured using precise calipers.
Results
The drill bit was an average of 5.43 mm from the axillary nerve exiting the proximal cross-lock hole, with direct nerve penetration in one specimen. At the distal cross-lock hole, the drill bit was 1.45 mm from the radial nerve and pierced it in two specimens. The middle cross-lock hole showed no proximity to either nerve. Arm rotation did not affect these distances.
Discussion
The axillary and radial nerves are near the proximal and distal locking screws in RSA fracture stems with cross-locking options. Surgeons should exercise caution when placing these screws to reduce nerve injury risk. Further clinical studies are needed to validate these findings.
Keywords
Introduction
Proximal humerus fractures are a common injury, particularly in the elderly population, with the annual incidence increasing as the population ages. 1 Reverse shoulder arthroplasty (RSA) is becoming an important treatment option for these fractures, especially in patients with complex or displaced fractures.2,3 Traditionally, RSA for proximal humerus fractures has involved cemented fixation of the humeral component. However, newer cementless implant designs have emerged, offering potential advantages such as shorter operative times, reduced anesthesia exposure, and elimination of cement-related complications like embolism.4–6
One such option for cementless fixation is the Tornier Perform Humeral System (Tornier, Inc., Bloomington, MN, USA), which provides three options for fixation, including cemented fixation, cementless fixation without screws, and cementless fixation with screws. There are three percutaneous screw options, which are placed through an external jig allowing for minimally invasive fixation. This is currently the only fracture stem that is FDA approved for non-cemented fixation. 7 Despite its increased use, the safety profile regarding the proximity of these percutaneous screws and drill paths to critical neurovascular structures including the axillary and radial nerves, has not been well established. Inadvertent injury to these nerves during screw placement can result in significant morbidity.
The purpose of this study is to evaluate the relationship between the percutaneous screw guide and drill bit trajectories used in the Tornier Perform system and the nearby neurovascular anatomy. Specifically, we aim to quantify the proximity of the drill and trocar trajectories to the axillary and radial nerves to inform surgeons of potential risks and guide safer surgical technique.
Materials and methods
Cadaver specimens
Six cadaver specimens from scapula to fingertip were used in this study. All specimens were male with a mean age of 71 years (SD 6.8; range 64–83 years), mean height of 69.5 inches (SD 1.5; range 68–72 inches), and mean weight of 175.5 lbs (SD 51.9; range 130–240 lbs). Three specimens were left-sided and three were right-sided. The cadavers were stored in a freezer and thawed to room temperature before testing. This study was reviewed by our Institutional Review Board (IRB) and determined to be exempt from review, as cadaveric research does not involve human subjects as defined by federal regulations (45 CFR 46). No personal identifiers were associated with the specimens. All cadaveric specimens were obtained through an accredited anatomical gift program in accordance with applicable state and federal laws governing the use of human tissue for research and education. No additional informed consent was required.
Surgical dissection and measurements
A 10 cm deltopectoral incision was made starting at the coracoid and extending distally through the interval. Skin flaps were raised and the deltopectoral interval was dissected. The cephalic vein was mobilized laterally. The bicipital groove was opened and a bicep tenotomy was performed. The biceps was then followed up through the rotator interval and the rotator interval was opened. A subscapularis peel was then performed. The humerus was delivered out of the incision, and our humeral neck cut was made by measuring 5.6 cm proximal to the superior aspect of the pectoralis major. The humerus was then broached and prepared according to the Tornier Perform Humeral System (Tornier, Inc., Bloomington, MN, USA) operative technique. 7 A trial stem of 130 mm length was implanted at 20 degrees of retroversion and the trocars for the cross-locking screws were inserted using the percutaneous screw guide. The incisions for the trocars were then extended and the axillary and radial nerves were dissected out. The location of the axillary nerve was confirmed by performing a tug test through the delto-pectoral interval on the anterior aspect of the nerve. Micrometer gauge calipers with measurements to the 0.1 mm were then used to measure the distance from the trocars to the nerve. The screw holes were then drilled and the drill was left in place past the second cortex. The micrometer calipers were used to measure the distance from the drill bit to the axillary and radial nerve. Following measurement in the neutral arm position (0° of rotation), the arm was repositioned at 45° of internal rotation and 45° of external rotation. Each rotational position was confirmed using a standard goniometer. Trocar and drill bit distances to the axillary and radial nerves were re-measured at each position (Figure 1).
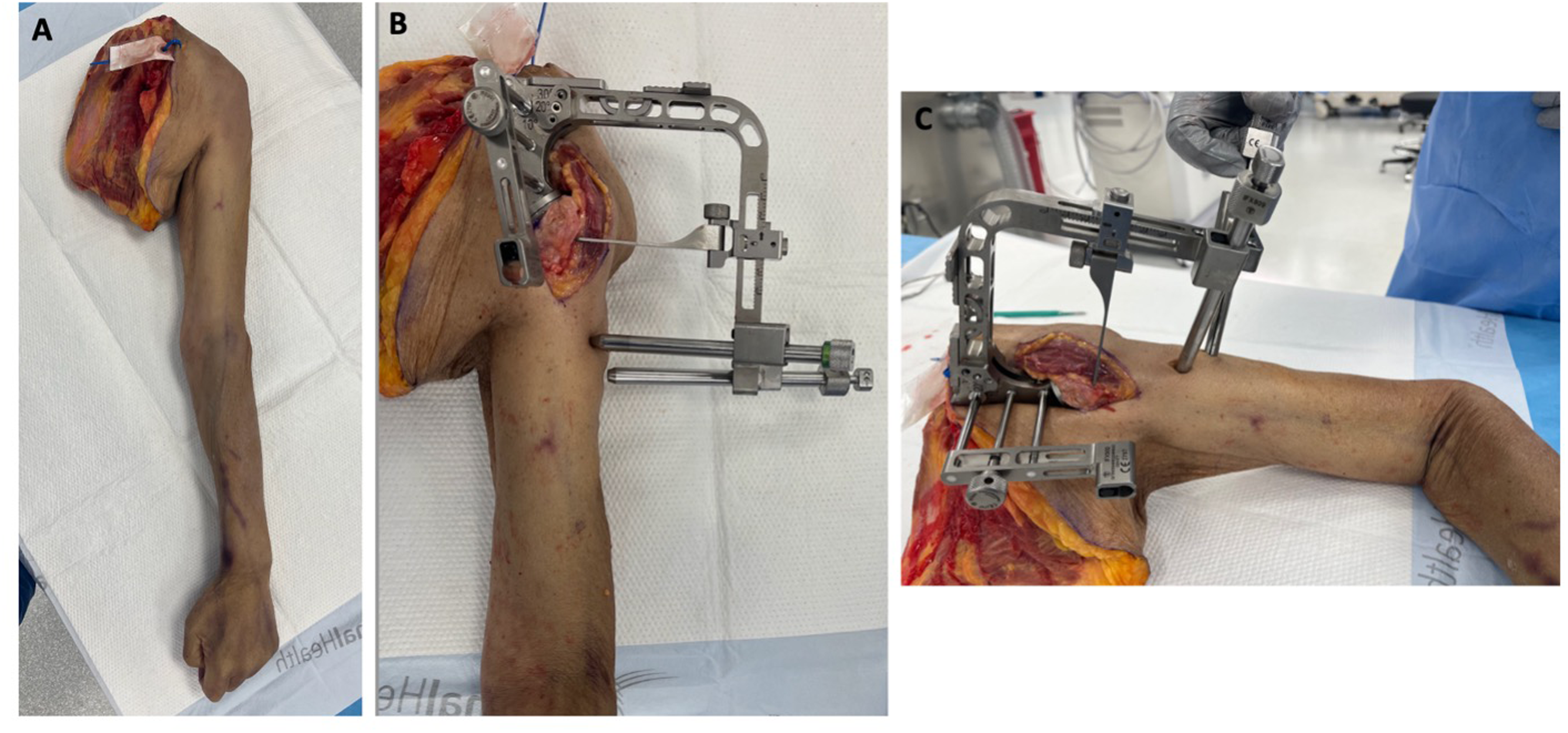
A: Cadaveric specimen prior to dissection. B: Specimen after implantation of fracture stem and application of cross-lock jig. C: Incisions made and trocars placed for percutaneous cross locking screws.
Statistical analysis
Cadaveric measurement data were analyzed using descriptive statistics. The mean, standard deviation (SD), and 95% confidence intervals (95% CI) for all measurements were calculated using R (version 4.5.2). All measurements from six specimens were included in the analysis. All measurements were performed by a single trained observer using micrometer gauge calipers precise to 0.1 mm. Repeated measurements were taken at each site, with the averages used for analysis to minimize intraobserver variability. Although interobserver reliability could not be assessed due to a single observer, meticulous dissection and measurement techniques were employed to avoid nerve distortion and optimize measurement accuracy.
Results
Six male cadaveric specimens with an average age of 71 years (range 64–83 years) were included in this study and analyzed using descriptive statistics (Table 1). Data points from all six specimens were analyzed to assess the proximity of trocars and drill bits to the axillary and radial nerves (Table 2).
Specimen information.
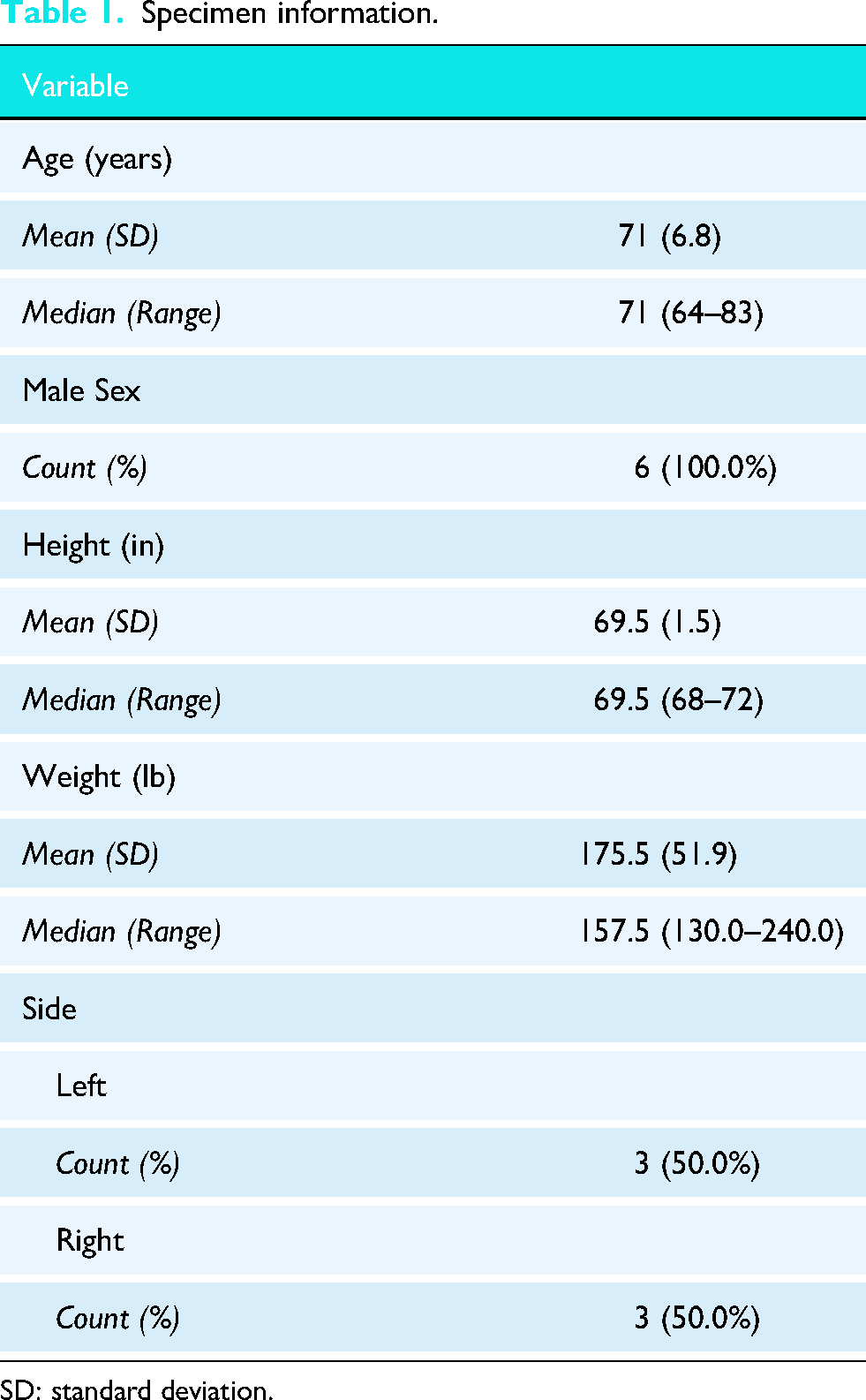
SD: standard deviation.
Distance of cross-lock trocar and drill bits from the axillary and radial nerves.
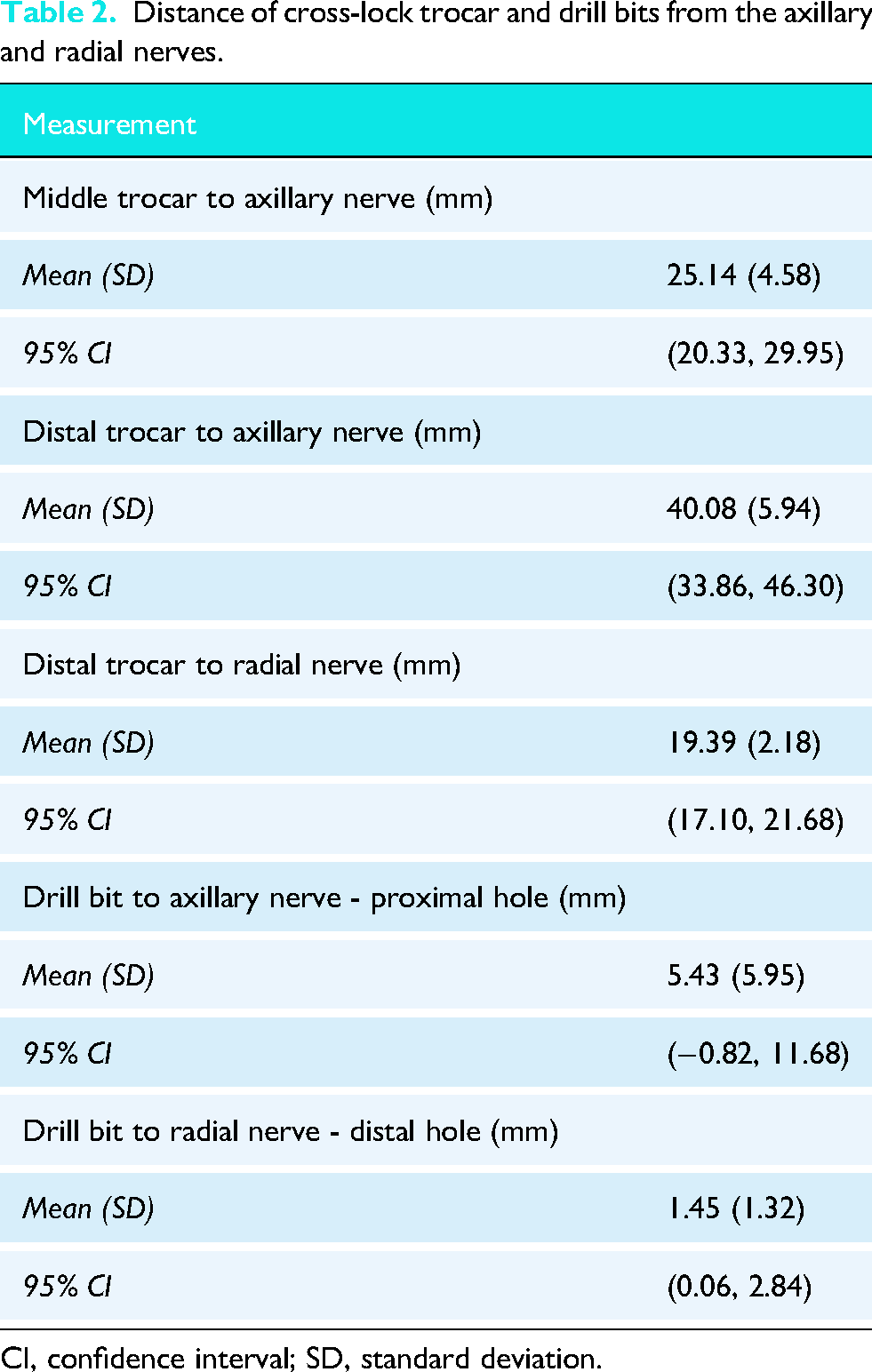
CI, confidence interval; SD, standard deviation.
The most proximal trocar was not in close proximity to any neurovascular structures in any specimen. The middle trocar was found to be on average 25.14 mm away from the axillary nerve and was not in close proximity to the radial nerve in any specimen. The distal trocar was an average of 40.08 mm from the axillary nerve and 19.39 mm from the radial nerve.
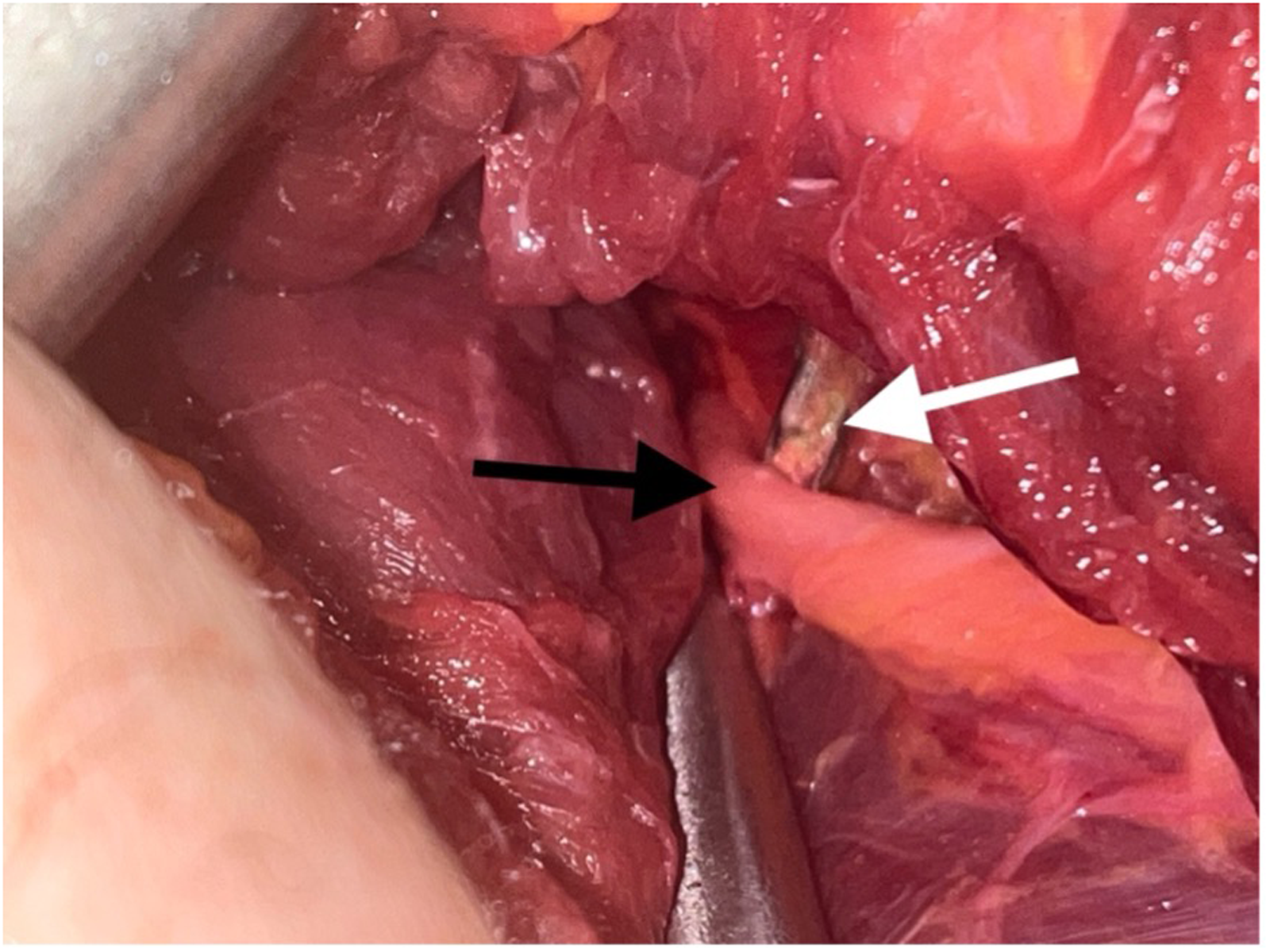
The drill bit exiting the proximal cross-lock hole was an average of 5.43 mm from the axillary nerve; however, in one specimen, the drill bit pierced the axillary nerve (Figure 2). The drill bit exiting the middle cross-lock hole was not found near the axillary or radial nerves. The drill bit exiting the distal cross-lock hole was an average of 1.45 mm from the radial nerve and pierced the radial nerve in two specimens (Figure 3).
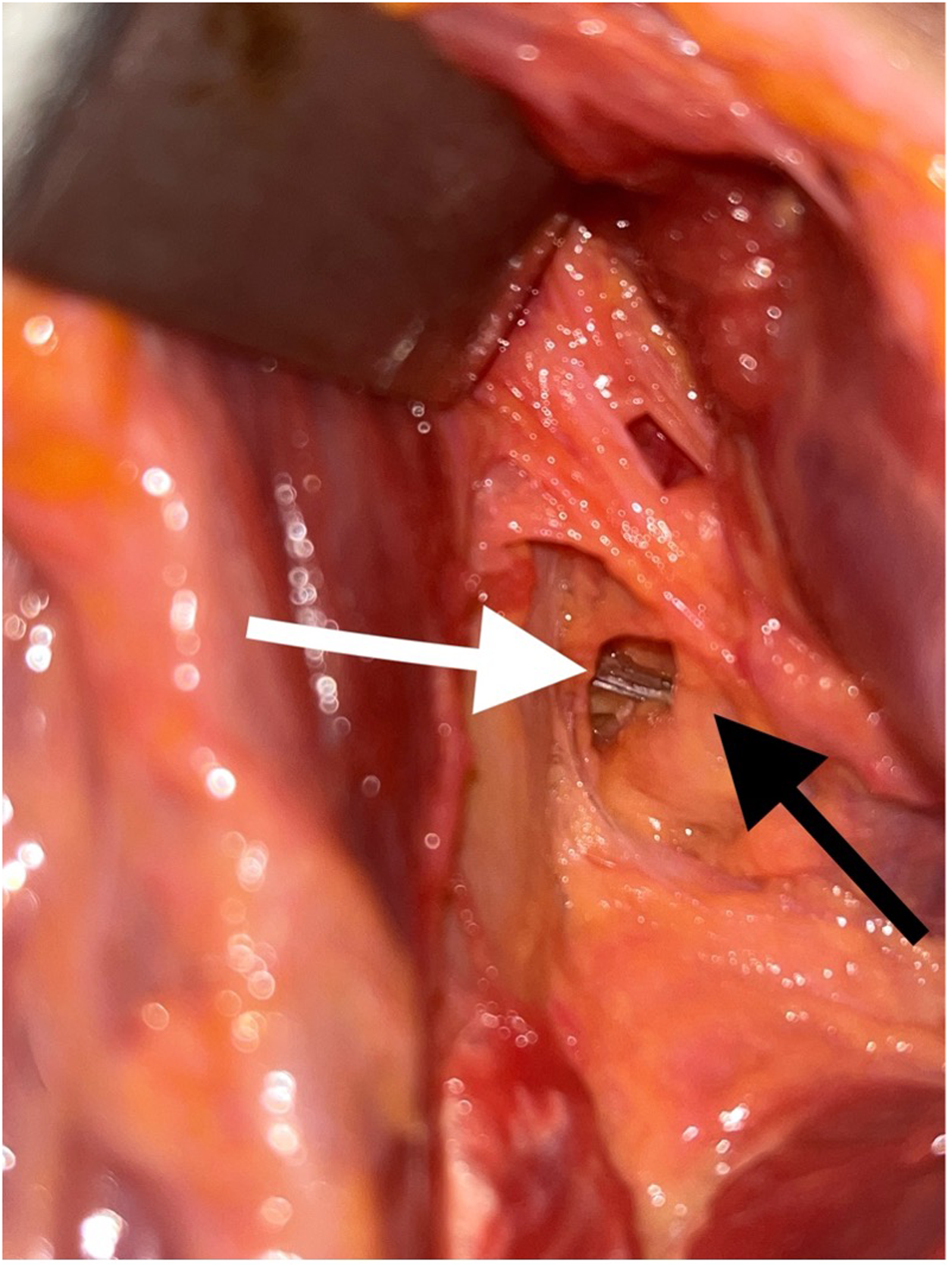
Drill bit exiting the proximal cross-lock screw hole, abutting a branch of the axillary nerve. Black arrow: Axillary nerve; White arrow: Drill bit.
Drill bit exiting the distal cross-lock screw hole and touching the radial nerve. Black arrow: Radial nerve; White arrow: Drill bit.
Internal and external rotation of the arm did not significantly affect the distances measured between the trocars or drill bits and the nerves.
Discussion
This cadaveric study demonstrates that, in a commercially available RSA humeral fracture stem with cross-locking screw options, the exiting drill bit trajectory through the proximal and distal cross-lock holes lies in close proximity to the axillary and radial nerves, respectively. Notably, direct nerve contact occurred in one specimen with the axillary nerve and two specimens with the radial nerve, emphasizing the potential risk of iatrogenic neurovascular injury. Conversely, the middle cross-lock hole did not pose a similar risk. Internal and external rotation of the arm did not significantly change the distance from the drill bit to these nerves.
The clinical relevance of these findings lies in the growing utilization of cementless humeral stems with percutaneous cross-locking screw fixation as an alternative to cemented RSA fixation in proximal humerus fractures.2,3,6 Cementless stems, such as the Tornier Perform Humeral System (Tornier, Inc., Bloomington, MN, USA) evaluated here, aim to reduce operative times and complications associated with cement while providing biologic fixation and enhanced stability through screw augmentation. 8 However, the percutaneous placement of locking screws introduces neurovascular risks that have not been previously characterized in RSA fracture stems.
Although cemented stems have the advantage of immediate fixation without percutaneous screw placement, cementless stems with screw augmentation aim to improve rotational stability and long-term implant survivorship.2,5 Literature on cementless versus cemented fixation in RSA for fractures remains equivocal, with some systematic reviews suggesting comparable clinical outcomes but differing complication profiles. 6 Our study contributes by highlighting an important consideration unique to cementless designs with cross-lock screws, which is the risk posed to neurovascular structures during screw insertion.
Beyond the neurovascular risks described in this study, surgeons should consider implant-related biomechanical complications associated with cross-locking screw fixation. The percutaneous cross-locking screws are not required in all cases but are recommended when intraoperative press-fit stability is suboptimal, particularly in the setting of poor bone quality or significant comminution. 9 The screw-stem interface creates a stress riser effect that may increase the risk of periprosthetic fracture at the cross-link site, especially in osteoporotic bone. 10 Additionally, early prosthetic loosening remains a concern with cementless designs, and cross-locking screws serve a critical stabilizing role during the osseointegration period. 11 Surgeons must weigh these biomechanical considerations alongside the neurovascular risks described herein when deciding whether to utilize percutaneous cross-locking screw fixation.
It is important to note that stem height, retroversion, and implant-specific design features, such as screw hole location and angulation, can influence the relationship between locking screws and surrounding anatomy.12–14 For example, variations in stem positioning may alter the proximity of cross-lock screws to the axillary and radial nerves, potentially increasing or decreasing risk. While this study maintained standard implantation techniques consistent with the Tornier Perform Humeral System (Tornier, Inc., Bloomington, MN, USA) surgical protocol, further research is needed to evaluate how these variables affect nerve safety.
Limitations of our study must be acknowledged. A significant limitation is the exclusive use of male cadaveric specimens (mean height 69.5 inches, range 68–72 inches; mean weight 175.5 lbs, range 130–240 lbs). Proximal humerus fractures disproportionately affect elderly females, who typically have smaller anatomical frames, narrower humeral diameters, and potentially shorter distances between implant trajectories and neurovascular structures. As a result, our findings may underestimate the nerve injury risk in the female population most commonly treated with this implant.15,16 Future studies using female cadaveric specimens are strongly encouranced. Additionally, anthropometric data, including segmental arm length and olecranon-to-fingertip distance, were not systematically collected. These measurements would have allowed correlation between limb dimensions and neurovascular proximity. Future cadaveric studies should incorporate standardized anthropometric measurements. The small sample size also limits generalizability and statistical power. Our intent to drill past the far cortex (“plunging”) represents a worst-case scenario and may overestimate risk during meticulous surgery. This study did not vary stem height or retroversion, nor did it evaluate dynamic movements beyond the rotational positions assessed (0°, 45°, 45°), which might influence nerve safety profiles.
Conclusion
This cadaveric study demonstrates that the axillary and radial nerves lie in close proximity to the proximal and distal cross-locking screw holes in the Tornier Perform Humeral System (Tornier, Inc., Bloomington, MN, USA) fracture stem. Notably, the drill bit contacted the axillary nerve in one specimen and the radial nerve in two specimens, highlighting potential risks during percutaneous screw placement. The middle cross-locking screw hole appeared to pose less risk to neurovascular structures in our sample.
Given the limited sample size and inherent constraints of cadaveric models, these findings should be interpreted with caution. Precise surgical technique and thorough anatomical knowledge are critical when placing proximal and distal cross-locking screws to minimize the risk of iatrogenic nerve injury. Further clinical studies are warranted to validate these findings and to develop surgical guidelines for safe percutaneous screw placement in RSA fracture stems.
Footnotes
Acknowledgements
None
Contributorship
SR
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Allegheny Health Network Orthopedic Institute Research Committee.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
SR (PI), RT (CI), AD (CI).