
Abstract
Background
Scapulothoracic abnormal motion (STAM) causes disabling scapular dyskinesis. Alternative, lower-risk strategies are needed. This study evaluates outcomes of scapula-to-scapula tethering (STST).
Methods
This retrospective series included patients undergoing STST between 2016 and 2023. The technique tethers the scapulae in retraction with an Achilles allograft. Inclusion required deltoid strength ≥4/5, intact rotator cuff, failed nonoperative treatment without glenohumeral pathology. Patients were classified as structural or functional STAM, with functional cases subclassified as rigid, dancing, or severe anterior tilt. Outcomes included range of motion (forward elevation (FE), abduction, external and internal rotation), patient-reported outcomes (PROs: visual analog scale [VAS], subjective shoulder value [SSV], American shoulder and elbow surgeons [ASES] score), and complications defined as early (<3 months) or late (>3 months).
Results
Twenty-seven patients (78% female; mean age 29 years; mean follow-up 29 months) were included: 10 structural, 17 functional (rigid = 5, dancing = 5, anterior tilt = 7). VAS, SSV, and ASES improved significantly. FE and abduction increased; rotation was unchanged. Three late graft failures occurred, two requiring reoperations.
Conclusion
STST improved pain, function, and range of motion with low morbidity, suggesting it may be a practical alternative to scapulothoracic fusion. However, findings should be interpreted cautiously given the lack of a comparator group and differing follow-up. Severe anterior tilt may increase graft failure and reoperation risk.
Level of evidence
IV; case series.
Introduction
Scapular stability, powered by coordinated muscle control, is essential for effective shoulder and arm movement. The upper trapezius (UT) and distal serratus anterior (SA) are key in stabilizing the scapula against the chest wall, allowing proper glenohumeral motion. 1 Deficiencies in these muscles lead to abnormal scapular rhythm, also known as scapulothoracic abnormal motion (STAM), 2 which leads to shoulder pain and dysfunction. The prevalence of STAM is likely unknown due to under-recognition of STAM, the mixed etiologies, and definitions ranging such as scapular dyskinesis and winging.
STAM can result from irreversible periscapular muscle injuries due to nerve damage, direct muscle injury, or both neurogenic and non-neurogenic causes. Neurogenic causes include conditions like facioscapulohumeral dystrophy (FSHD), 3 Parsonage–Turner syndrome, 4 and brachial plexus injury. 5 Non-neurogenic causes involve muscle discoordination or dystonias, often leading to abnormal scapular positioning due to muscle imbalances, such as overactive pectoralis minor and UT with underactive SA.6,7 In extreme cases of non-neurogenic STAM secondary to focal dystonias, rigid scapular deformity or involuntary scapular movements may occur. Published accounts of these cases are limited, and treatment options include ineffective medical management or morbid, ablative procedures.8–12
Treatment for STAM varies by etiology. Muscle tendon transfers effectively address paralysis from direct nerve or periscapular muscle injury.13,14 However, in neurogenic or non-neurogenic cases involving multiple muscular abnormalities, scapulopexy or scapulothoracic (ST) fusion is often required. 15 ST fusion, though, carries high complication rates and may not be suitable for pediatric patients with open physes or those with restrictive lung disease. 3 Additionally, no effective surgical options currently exist for non-neurogenic STAM and focal periscapular muscle dystonias. Therefore, exploring innovative procedures to improve outcomes and reduce complications is crucial. This study aims to evaluate a novel scapula-to-scapula tethering (STST) method for treating STAM due to neurogenic and non-neurogenic causes. The hypothesis was that STST leads to significantly improved patient outcomes with minimal complications.
Methods
Institutional review board (IRB) approval was obtained prior to conducting this study (Study Protocol ID: 2021P002572). This study's reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 16
Study design and setting
This was a retrospective chart review of consecutive patients receiving STST for STAM by two high-volume fellowship-trained surgeons specializing in scapula-related procedures between 2016 and 2024. This study was conducted at a referral scapular surgery center at a tertiary academic medical center.
Participants
The inclusion criteria included patients with neurogenic and non-neurogenic STAM who failed extensive conservative management strategies including at least 6 months of physical therapy focusing on scapular stabilization exercises, refused ST fusion, had improved shoulder function with scapular retraction on physical examination, and had a reducible scapular position intraoperatively. Scapular retraction is essential for assessing patient suitability for STST by replicating the post-tethering scapular position. With the examiner behind the patient, the scapulae are retracted towards the midline, and the patient is asked if symptoms improve at rest and during shoulder movements. Symptom relief suggests a favorable outcome with STST. For the intraoperative examination, if the scapula is rigid intraoperatively, ST fusion should be considered instead of STST.
Contraindication were (1) Identifiable single periscapular muscle deficiency that is amenable to treatment with tendon transfers, (2) deltoid weakness of <4/5 using the Medical Research Council grading scale which is concerning for limb girdle dystrophy or (3) those with discernible local shoulder pathology such as rotator cuff or shoulder instability amenable to conventional treatment.
The definition of STAM was any visually observable abnormal scapular rhythm or winging in one of three scapular planes including protraction-retraction, anterior-posterior tilt and upward-downward rotation during active shoulder range of motion (ROM) examination.1,13 STAM further was divided into neurogenic and non-neurogenic STAM. Neurogenic STAM included patients with a diagnosis of FSHD with shoulder pain and STAM resulting in limited ROM that improved with the scapular repositioning test (SRPT). 17 The diagnosis of FSHD was further consolidated with electromyography (EMG) and multidisciplinary evaluation including geneticists. Non-neurogenic STAM was observed in patients without muscular deficiency on physical examination which includes observable muscle atrophy, and periscapular muscle testing using the Medical Research Council scale (scored on a 0 to 5 scale). The UT was evaluated with a shoulder shrug, and if absent, the levator scapulae (LS) was assessed by placing the patient's arm behind the back while elevating the elbow. An intact LS would be visible and palpable during this maneuver. The middle and lower trapezius (MT, LT) were evaluated during resisted scapular retraction, and if absent, the rhomboids were checked by visualizing their contraction with resisted scapular retraction; rhomboid absence was indicated by palpable ribs. The SA is best evaluated using resisted protraction, or the shoulder flexion resistance test, raising the arm in forward elevation (FE) while the examiner exerts a downward force on the forearm as a break test. The LD was evaluated through resisted arm extension and internal rotation (IR) from 90˚ elevation position and palpation of the posterior axillary fold. The PM was examined by observing the bulk and contraction of its sternal and clavicular heads, and its strength was tested through resisted arm adduction.
All non-neurogenic STAM patients had undergone a multidisciplinary evaluation which entails the discussion among orthopedic surgeons, radiologists and geneticists to exclude any potential structural pathologies that would explain the cause of the STAM from a structural rather than functional non-neurogenic origin. This included scapula computed tomography imaging to evaluate for osseous periscapular lesions such as chondrosarcomas or scapular congenital osseous deformities. Scapula and shoulder magnetic resonance imaging was utilized to exclude structural soft-tissue injuries such as periscapular muscle tears or rotator cuff tears. Patients with non-neurogenic STAM were determined to have three patterns of motion attributed to focal periscapular muscle dystonias. These dystonias were refractory to multiple conservative management strategies including medications, injections, and physical therapy. Patients with these conditions demonstrated reduced FE and abduction.
Rigid scapula: Scapula fixed in severe anterior tilt, protracted, and elevated, irreducible on examination compared to the contralateral scapula, but reducible intraoperatively under anesthesia. Severely anteriorly tilted scapula: Reducible on examination with SRPT, with hyperactivity of the pectoralis minor and UT and hypoactive distal SA. Dancing scapula: Involuntary choreiform periscapular muscle contractions occurring at rest or triggered by light stimulation or strength testing. Video 1 displays the choreiform contractions which occur with light stimulation and are resolved with forced scapular retraction.
Surgical technique
The primary rationale behind this surgical technique is to offer a minimally invasive option for patients with neurogenic and non-neurogenic STAM, avoiding the need for ST fusion. The technique is designed to maintain both scapulae in a retracted position, effectively counteracting the deforming forces associated with neurologic and non-neurologic STAM.
Patients were positioned prone on a standard operating room table. Under general anesthesia, the scapula and glenohumeral joints were examined for ROM. For patients initially presenting with a rigid scapular position, we first confirmed that the scapula can be reduced intraoperatively by performing scapular retraction which is essential to proceed with the STST procedure. The neck, bilateral scapula and shoulders were prepped and draped to allow for retraction of the scapula. Incisions are produced over the medial scapular spine and curving distally along the medial scapular border (Figure 1). Dissection was carried down to the lower trapezius musculature, and this is partially elevated to allow access to the medial scapular spine. The infraspinatus fascia was incised, and the upper border of the infraspinatus was elevated off the bone using electrocautery to provide an approximate 3 cmx3 cm area for allograft fixation. A subcutaneous tunnel was created between both incision sites using blunt dissection (Figure 2). A looped, non-absorbable suture was passed through the medial spine of both scapula and tied together to act as an internal splint/brace, holding the scapula in a retracted position while the allograft is prepared. The scapulae are placed and held in the maximally retracted position.

Intraoperative photograph depicting the two incisions at the medial borders of the scapula. The Achilles tendon allograft for the scapula-to-scapula tethering is also displayed.

A subcutaneous tunnel is created between both incision sites using blunt dissection and a clamp to shuttle the Achilles tendon allograft subcutaneously from one scapula to the other is depicted.
An achilles tendon allograft was prepared using non-absorbable suture in a running Krakow fashion on the thick, calcaneal end. Two suture buttons were placed through the medial scapular spine, and the achilles tendon was secured. A grasping instrument was then used to pass the allograft through the subcutaneous tunnel and was likewise secured on the contralateral scapula again using two buttons. Excess achilles tendon allograft is removed. The sutures from the suture buttons were used to reapproximate the reflected infraspinatus and associated fascia to the lower trapezius tendon and muscle and to cover the insertions of the achilles allograft.
Postoperative protocol
Patients were placed in a shoulder immobilizer for comfort unilaterally beginning with the most symptomatic shoulder and allowed to alternate immobilization. Patients are encouraging to refrain from motion for the first week to promote wound healing. Passive ROM was allowed after 1 week; however, reaching and weight bearing are prohibited for the first 6–8 weeks. After the first 6–8 weeks, patients were progressed to active-assist and active ROM as tolerated under the guidance of a physical therapist with no stretching or strengthening. During this phase, special focus on UT activation. Aquatic therapy was encouraged during this period. At 12–14 weeks from surgery, progressive shoulder stretching and strengthening were started. At 18–20 weeks from surgery, the patient was allowed activity as tolerated without restriction. Figure 3 shows a patient who completed postoperative rehabilitation following the STST procedure, successfully achieving full shoulder FE. In Figure 4, one can see the Achilles allograft tether visible and can be palpable throughout shoulder ROM.
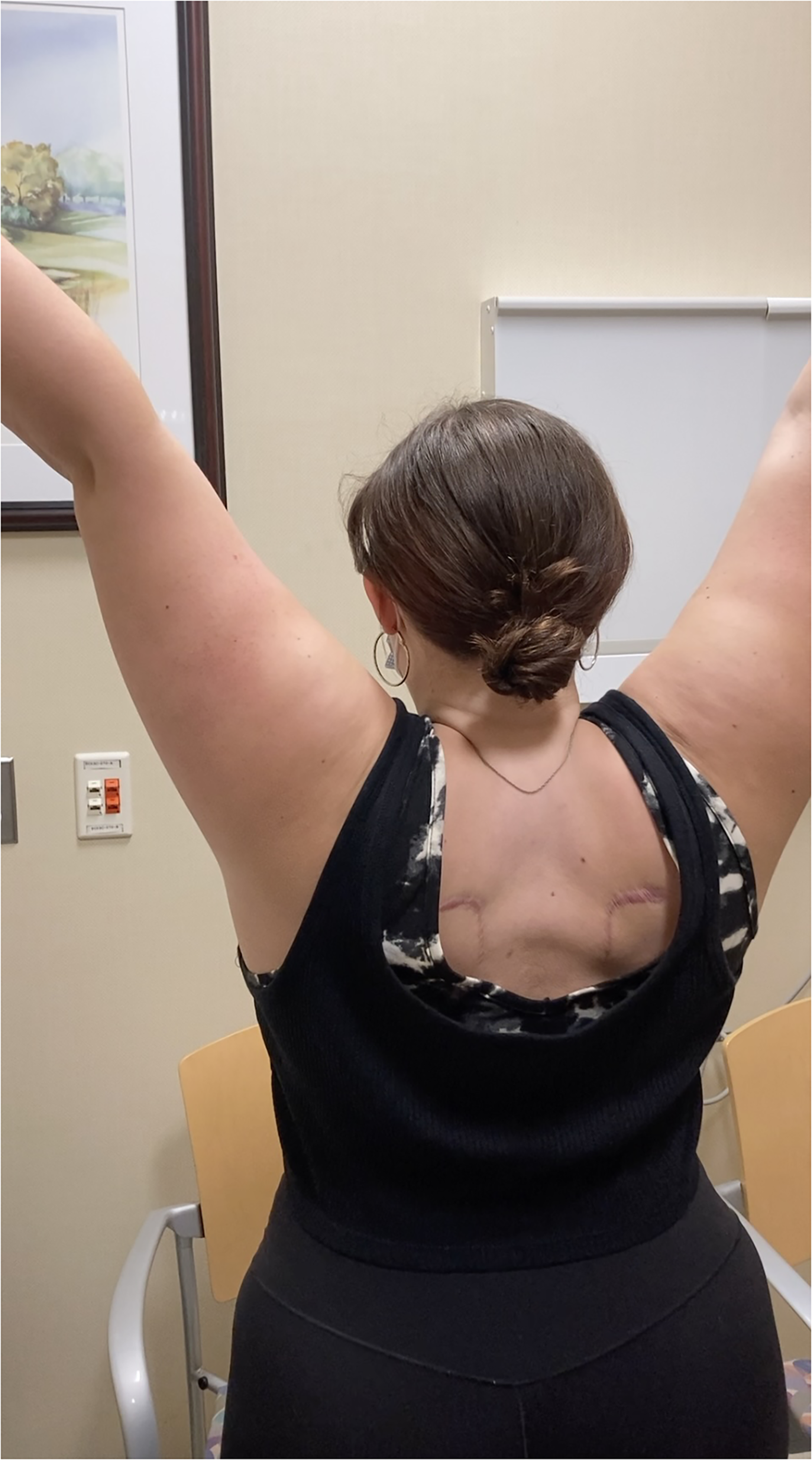
A clinical photograph demonstrating a patient achieving full shoulder forward elevation after complete rehabilitation following the scapula-to-scapula tethering procedure.

In this clinical photograph one can see the Achilles allograft tether visible, this is palpable throughout shoulder range of motion as well confirming the integrity of the scapula-to-scapula tethering.
Variables
Preoperative and postoperative ROM in domains of FE, abduction, external rotation (ER) at the side, and IR up the back were collected by the senior authors by using a goniometer. IR was graded based on a previously published scale, 18 ranging from a value of 1 (abdomen) to 14 (T7). Patient-reported outcome (PRO) measures including visual analog scale (VAS) pain, shoulder subjective value (SSV), and American shoulder and elbow surgeons (ASES) score were collected pre- and postoperatively. Complications were defined as early when occurring less than 3 months from surgery, and late when occurring greater than 3 months from surgery. Further, they were defined as major when requiring reoperation or intervention or minor when observation and spontaneous recovery occurred.
Statistical analysis
Descriptive statistics were conducted to report the patients’ characteristics. Continuous variables were reported as means and standard deviations or ranges when appropriate, whereas categorical variables were expressed as percentages. The two-group t-test was used for comparing pre- and postoperative ROM and patient-reported outcome measures (PROMs). All statistical analyses were performed using R statistical software (Version 1.2.1335; R, Vienna, Austria).
Results
Patients’ demographics
Twenty-seven patients met the inclusion criteria receiving STST. Patients were predominantly female (n = 21; 78%) with an average age of 29 ± 16 years (range 12–57). The average body mass index (BMI) was 28.8 ± 5.8 kg/m2. All patients were right-hand dominant. Twenty-five patients were non-smokers, and two were former smokers. The average follow-up period was 29.3 ± 15.9 months (range 3–72 months). Please see Table 1.
Demographic and preoperative values for combined and neurogenic and non-neurogenic scapulothoracic abnormal motion (STAM) groups, with comparison presented between STAM groups.
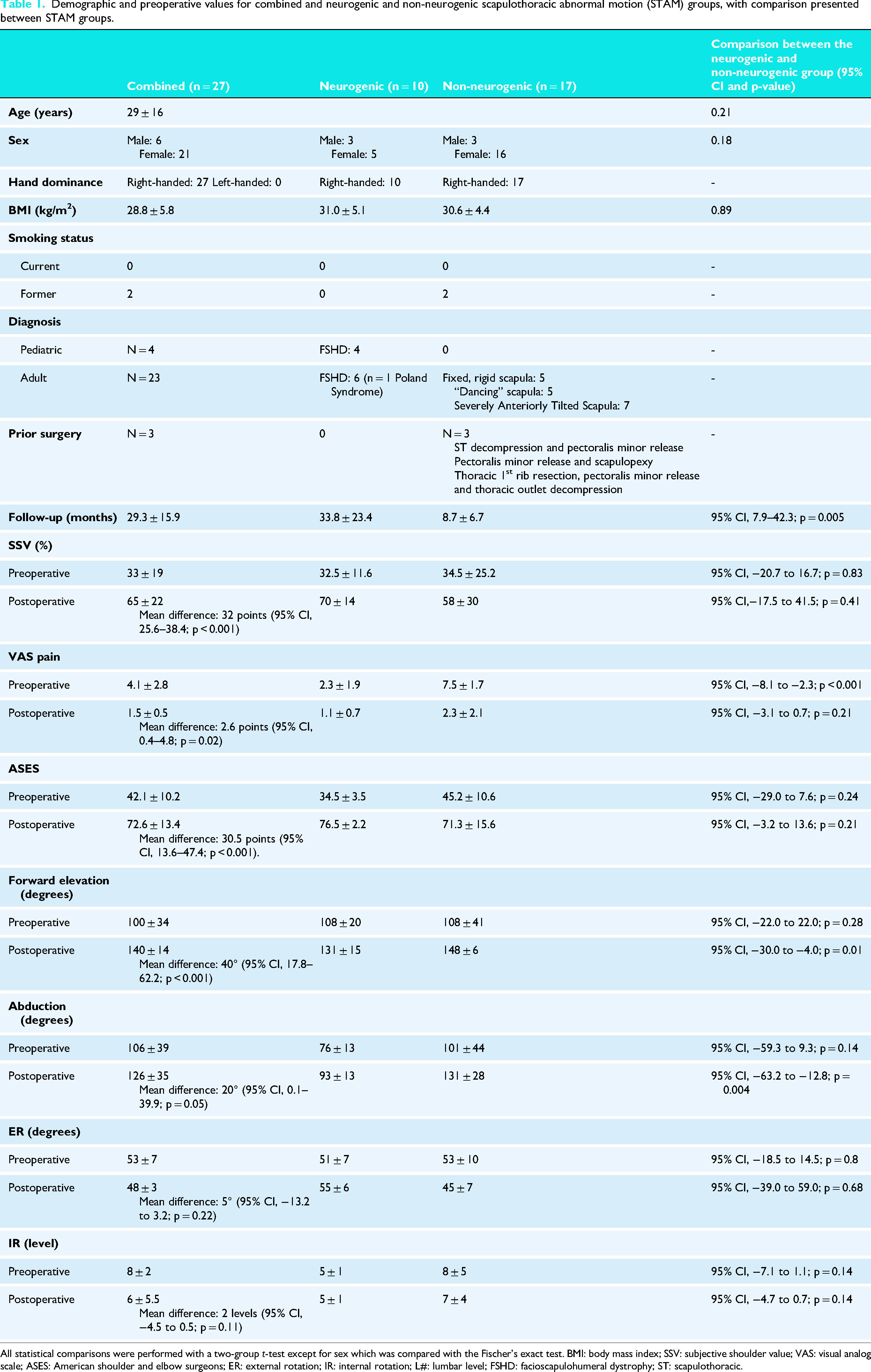
All statistical comparisons were performed with a two-group t-test except for sex which was compared with the Fischer's exact test. BMI: body mass index; SSV: subjective shoulder value; VAS: visual analog scale; ASES: American shoulder and elbow surgeons; ER: external rotation; IR: internal rotation; L#: lumbar level; FSHD: facioscapulohumeral dystrophy; ST: scapulothoracic.
Ten patients out of all 27 patients (37%) had a diagnosis of FSHD with combined deficiency of the trapezius and SA musculature producing STAM. Four patients having FSHD (40%) were pediatric (age 12–16), while the remaining were adult patients with bilateral pathology. Seventeen patients out of all 27 patients (63%) had diagnoses of non-neurogenic STAM which were further differentiated based on aforementioned clinical exam features. Five patients (29.4%; 5 out of 17) presented with rigid scapulae irreducible on examination but reducible intraoperatively. Seven (41.2%; 7 out of 17) patients had severe, bilateral anteriorly tilted scapula reducible to neutral non-tilted position on examination. Five patients (29.4%; 5 out of 17) presented with a dancing scapula. Three patients (30%) had prior ipsilateral shoulder surgeries including n = 1 scapulothoracic arthroscopic decompression with arthroscopic pectoralis minor release, n = 1 arthroscopic pectoralis minor release and scapulopexy, and n = 1 remote thoracic first rib resection, pectoralis minor origin release and thoracic outlet decompression.
Patients with non-neurogenic STAM were compared to those presenting with neurogenic STAM (FSHD). Patients with non-neurogenic STAM had significantly greater preoperative VAS pain scores (7.5 ± 1.7 vs 2.3 ± 1.9; p < 0.001). There were no significant differences between groups for other demographic variables of age, sex or BMI. Follow-up was significantly shorter for patients with non-neurogenic STAM (8.7 ± 6.7 months vs 33.8 ± 23.4 months; p = 0.005). There were no significant differences between groups for preoperative ROM in flexion, abduction, ER, and IR.
Postoperative outcomes
The average VAS pain score improved postoperatively (4.1 ± 2.8 vs 1.5 ± 0.5; p = 0.02). SSV scores improved from 33% ± 19% to 65 ± 22% postoperatively (p < 0.001). The ASES score improved from 42.1 ± 10.2 to 72.6 ± 13.4 postoperatively (p < 0.001).
Postoperative ROM improved for measured parameters across all patients. FE improved from 100˚ ± 34˚ preoperatively to 140˚ ± 14˚ postoperatively (<0.001)) and abduction improved from 106˚ ± 39˚ preoperatively to 126˚ ± 35˚ postoperatively (p = 0.05). Both IR and ER remained unchanged, (8.0 ± 2 (L2) preoperatively vs 6.0 ± 5.5 (L3) postoperatively; p = 0.11) and (53˚ ± 7˚ preoperatively vs 48˚ ± 3˚ postoperatively; p = 0.22), respectively. A greater improvement was seen in patients with non-neurogenic STAM when compared to neurogenic STAM in both FE (148˚ ± 6˚ vs 131˚ ± 15˚; p = 0.01) and abduction (131˚ ± 28˚ vs 93˚ ± 13˚; p = 0.004) (Table 1).
There were no early complications in this series such as infection, neurovascular injury, or graft failure. The overall late complication rate was 11.1% (3 out of 27) which involved graft failure in one patient with FSHD (neurogenic STAM), and two patients with non-neurogenic STAM in the severe anterior tilt scapula subgroup. The two patients with severely anteriorly tilted scapulae developed recurrent STAM and ultimately received additional procedures at 10 and 18 months after their STST in the form of a distal SA advancement. Notably, both patients had prior ipsilateral procedures for STAM including pectoralis minor release and ST decompression, and first rib resection with pectoralis minor origin release and thoracic outlet decompression. One patient with FSHD had rupture of their graft occur 36 months postoperative though did not receive further revision. The overall binary patient satisfaction at final follow-up was 89%.
Discussion
The purpose of this study was to report the outcomes of a novel procedure of STST in patients with varying etiologies of STAM. Further, this study characterized different, non-classic, neurogenic forms of STAM that have very limited clinical reporting. This case series provides to the best of our knowledge, the first reported technique of STST, as well as indications for the use of this procedure. These findings suggest that appropriate surgical indication may provide patients with improved motion, reduced pain, and overall higher levels of patient satisfaction following STST. These indications include neurogenic (including FSHD) and non-neurogenic STAM.
Treatment for FSHD has traditionally included scapulopexy or ST fusion. Giannini et al. reported on nine patients (18 procedures) with a 9.9-year follow-up, where scapula fixation to the ribs without fusion using metallic wires resolved abnormal motion and winging, with increased ROM. 4 A similar study with 13 patients (26 procedures) showed comparable results. 5 Non-arthrodesis fixation techniques, such as fascia lata, mersilene tape, or Dacron strips, have also been used.6,19 Treatment for FHSD has most consistently relied on arthrodesis of the scapula to the chest wall, termed ST fusion. Various techniques have been employed with ST fusion, with reported complication rates up to 41%, including hardware failure, nonunion, and pneumothorax. 7 Contraindications to ST fusion include weak deltoid muscles, inability to comply with postoperative immobilization, general anesthesia risks, restrictive lung pathology, and potential for muscle transfers.3,20,21 Patient expectations and desire to avoid fusion are also important considerations. This novel approach of STST offers an alternative, providing scapular retraction, stability, and sufficient subacromial space for arm elevation or abduction in patients with intact deltoid and rotator cuff muscles. This dynamic stability is achieved through contralateral lower trapezius contraction. 22 STST is a viable option for FSHD patients, particularly those wishing to avoid fusion, those with respiratory conditions, pediatric patients, or those with other limb girdle dystrophies. The limited case series showed no early complications, avoiding pleural injuries and nonunion.
This study defines a previously unclear patient category within the literature: non-neurogenic STAM caused by local dystonia. This category includes three deformities: rigid scapula, anteriorly tilted scapula reducible on examination, and dancing scapula. Patients with dancing scapula showed features of peripherally induced movement disorders, often with continuous, non-stimulus-based movement and overflow to all periscapular muscles. These disorders, described in various terms like “scar dancing syndrome,” “dancing quadrilaterals,” and “focal shoulder elevation dystonia” have been poorly characterized in the literature, with case reports and small series noting inconsistent outcomes from botulinum toxin injections.9–12 Lizzaraga et al. evaluated four patients with a “dancing quadrilateral” syndrome after spinal instrumentation without effective treatment. 10 They hypothesized that these patients show the effects of damaged spinal inhibitory neurons, and that there may be abnormal proprioceptive information conveyed to the segmental spinal reflex networks producing this motion. Our series is the only published account of patients with conservatively managed, refractory dancing scapula effectively treated by surgical means without nerve ablative or destructive procedures. Though rare, it is essential that surgeons and clinicians understand that these conditions exist, and that there are alternative, effective treatment options. Our limited series describing five of these patients with dancing scapula showed improvements in VAS for pain, ROM, and PROMs in this subgroup and subjective satisfaction. It may be that the altered scapular skin and muscle position provided through STST is enough to overcome the abnormal inhibitory local reflex arc hypothesized to cause this condition. In this patient subset, STST maybe an alternative first-line treatment due low complication profile treatment in this limited series compared to previously described scapular methods of stabilization including scapulopexy or ST fusion. In patients with STAM secondary to severely anteriorly tilted scapulae due to pectoralis minor and UT hyperactivity and distal SA hypoactivity as described by Elhassan et al., 23 STST may be a second-line procedure as failures and dissatisfaction were the highest in this subgroup. It is important to council patients receiving STST, that this is a rarely performed procedure, and that it may be less effective in patients with more severe forms of non-neurogenic STAM, such as those with constant motion without discernible stimulus-induced movement.
Limitations of the study include the small patient population and heterogeneous cohorts. Between group analysis could not be reliably performed because of the limited sample size. Further exploratory data analysis could not be performed such as risk factors for failure or poor outcome due to small sample sizes. The study is retrospective in nature and therefore limits the level of evidence. Follow-up is also limited, and patients may require additional procedures or eventually fail their scapula-to-scapula tether, and our follow-up duration may not capture this. It is unknown currently how many of these patients go on to require additional procedures or salvage operations such as ST fusion. Though collected PROMs included SSV and ASES values, these scores may not be reliable in periscapular pathology, as SSV and ASES are validated outcome measures primarily designed to assess glenohumeral pain and function rather than ST mechanics. Consequently, improvements or persistent deficits in ST motion and biomechanics may be underrecognized when relying solely on these outcome measures. Another important limitation is that the proposed biomechanical rationale of STST as a stabilizing construct by tethering the two scapulae remains theoretical, as this study did not directly evaluate scapular kinematics. Further studies are required to characterize and classify patients with non-neurogenic STAM based on clinical examination, EMG features, and treatment modalities to provide a robust framework of evaluation and treatment. We feel that our study provides additional insight into patients with STAM and adds intuitive terminology that does not classically fall into categories of winging.
Conclusion
STST resulted in significant improvement in PROMs and ROM in the short follow-up. STST may be an alternative treatment for patients to avoid fusion, or in those with specific types of non-neurogenic STAM. However, findings should be interpreted cautiously given the lack of a comparator group and differing follow-up. Further studies are required to determine the long-term outcomes of this procedure and define additional indications and contraindications.
Supplemental Material
Footnotes
Ethical approval
Mass General Brigham IRB (IRB approval number 2021P002544).
Informed consent
Exempt as this was a retrospective study.
Contributorship
AFA and RL contributed to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Bassem Elhassan
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.