
Abstract
Background
Long-term corticosteroid (LTC) use is a known risk factor for adverse outcomes after various surgical procedures. However, the impact of LTC use on surgical complications after TSA remains underexplored. This study aims to assess the influence of LTC use on 90-day and 5-year complications following TSA.
Methods
A retrospective cohort study utilizing the PearlDiver database was conducted. Patients undergoing primary TSA with a minimum 5-year follow-up were included. LTC users were propensity-matched 1:10 with controls based on demographic variables and comorbidities. Postoperative complications within 90 days of surgery and long-term complications within 5 years were compared between groups. Multivariable logistic regressions were used to compare complications controlling for demographic variables and comorbidities.
Results
In a matched cohort of 556 LTC users to 4942 controls, corticosteroid users exhibited a 2.91-fold higher risk of pneumonia (95% CI: 1.69–4.80, p < 0.001) and a 2.19-fold higher risk of venous thromboembolism (VTE) (95% CI: 1.30–3.51, p = 0.001) within 90 days following TSA. No significant differences in 5-year surgical outcomes were observed.
Discussion
LTC users are at a heightened risk for 90-day medical complications, including pneumonia and VTE following TSA. However, their 5-year risk of surgical complications was comparable to patients without LTC use.
Keywords
Introduction
Total shoulder arthroplasty (TSA) is a well-established, effective procedure that improves quality of life and mobility in patients with debilitating shoulder osteoarthritis. 1 The incidence of TSA has been increasing rapidly, with one study projecting a 122% increase in utilization by 2040. 2 With the rising utilization of TSA, comorbidities and long-term medication use in more complex patients may impact medical and surgical outcomes. Long-term corticosteroids (LTC) are an important factor to consider, given their popularity despite negative effects on bone health, wound healing, and immune function.3–5
Corticosteroids disrupt bone health by altering the balance between bone resorption and formation, suppressing osteoblasts and reducing their life span. 6 These effects are time and dose-dependent, with long-term users at a much higher risk of osteoporosis. Prior literature indicates that nearly 90% of patients who have taken corticosteroids for at least 60 days experience some degree of adverse bone effects. 7 These adverse effects on bone quality carry significant implications for patients undergoing orthopedic surgery.
Prior literature has identified several key associations between LTC use and adverse medical or surgical outcomes following total hip arthroplasty (THA) and total knee arthroplasty (TKA). Following these procedures, LTC use has been shown to increase rates of periprosthetic fractures, all-cause revision, and periprosthetic joint infection (PJI) postoperatively.8,9 LTC use in the hip and knee arthroplasty literature has also been shown to increase medical complications, including urinary tract infection (UTI), pneumonia, deep vein thrombosis (DVT), and readmission rates.10,11 Of the few studies that have evaluated LTC use in TSA, these medications have been linked with an increased rate of UTI, readmission, and sepsis within 30 days.12–14 While these findings provide valuable insight into the short-term outcomes associated with LTC use in TSA, little is known about its effects on long-term TSA outcomes. The purpose of this study was to examine how LTC use affects 90-day medical and 5-year surgical complications after TSA. We hypothesized that patients on LTC therapy would experience higher rates of 90-day medical complications as well as higher rates of 5-year surgical complications when compared to controls.
Materials and methods
Data source
Patient data was obtained from the PearlDiver Mariner Database (PearlDiver Inc., Colorado Springs, CO, USA). PearlDiver is a commercially available administrative claims database that contains deidentified patient data from 2010 to 2023. The “M170Ortho” dataset within PearlDiver was used, which contains a sample of 170 million patients. The PearlDiver Mariner database has been used extensively in published peer-reviewed orthopedics outcomes research over the past decade. Diagnostic and procedural codes employed in the present analysis were selected to be consistent with prior studies. As with any administrative claims analysis, the validity of code-defined outcomes is contingent upon the accuracy and consistency of underlying ICD and CPT coding. Data from this dataset is Health Insurance Portability and Accountability Act (HIPAA) compliant, and this study was deemed exempt from review by the institutional review board.
Study design
A propensity-matched retrospective cohort study was performed to evaluate the effect of LTC use on outcomes following TSA. All TSAs were identified using Current Procedural Terminology (CPT) codes and International Classification of Diseases (ICD) 9th and 10th revision codes (Appendix). All patients had at least 5 years of follow-up in the database following TSA. Patients who underwent TSA for fracture, malignancy, or infection were excluded. Additionally, patients who underwent a contralateral TSA within 5 years were excluded to ensure that complications were related to the index TSA.
LTC users were identified with the ICD codes ICD-9-CM-V5865 and ICD-10-CM-Z7952 for “long-term (current) use of corticosteroids” at any time prior to the procedure. Additionally, to ensure patients were actively on corticosteroids, we screened for an active insurance claim for an oral corticosteroid prescription within 90-days prior to TSA. An active prescription claim was defined as a filled prescription overlapping the preoperative 90-day window, based on National Drug Code identifiers and fill dates. These criteria for identifying ongoing LTC use have been described previously in the literature. 8 Patients in the propensity-matched control cohort underwent TSA, met inclusion criteria, and did not have any prescriptions for corticosteroids prior to the index TSA.
LTC users were propensity matched 1:10 with controls based on age, gender, Charlson Comorbidity Index (CCI), obesity, tobacco use, and rheumatoid arthritis and osteoporosis, all of which have been shown to increase complications in TSA.15,16
Outcome measures
Short-term complications within 90 days of TSA, including myocardial infarction, pneumonia, venous thromboembolism (VTE), UTI, blood transfusion, wound dehiscence, acute kidney injury (AKI), emergency department (ED) visits, and readmissions, were assessed for each group. Long-term complications within 5-years, including all-cause revision, PJI, dislocation, aseptic loosening, fracture, and stiffness, were assessed for each group. All CPT and ICD codes used to define postoperative complications can be found in Supplemental Information 1.
Statistical analysis
Differences in continuous variables were compared using Welch's t-test, and categorical variables were compared using chi-squared tests. Rates of postoperative complications were compared using multivariable logistic regression controlling for age, gender, CCI, obesity, tobacco use, rheumatoid arthritis, and osteoporosis. All analyses were performed using R (R Foundation for Statistical Computing, Vienna, Austria) embedded within the PearlDiver database. Statistical significance was defined as a p-value <0.05 for all analyses.
Results
Cohort characteristics
A total of 98,229 primary TSAs within the M170Ortho dataset met the index inclusion criteria of the present analysis. Index criteria included primary TSA performed between 2010 and 2018 (to ensure adequate long-term follow-up), TSA indications other than fracture, malignancy, or infection, and no contralateral TSA within the 5-year follow-up window. Of these, 556 patients met the complete definition for LTC use requiring both an ICD code for LTC use and an active oral corticosteroid prescription within the 90-day preoperative window. All 556 LTC-defined cases were propensity matched, yielding 4942 matched controls. There were no statistically significant differences between cohorts in age, gender, rate of obesity, rate of tobacco use, or rate of rheumatoid arthritis (Table 1). The LTC use group had a significantly lower average CCI and higher rate of osteoporosis than the control group (Table 1, p = 0.001 and p = 0.036, respectively).17,18
Comparison of demographic variables between matched cohorts.
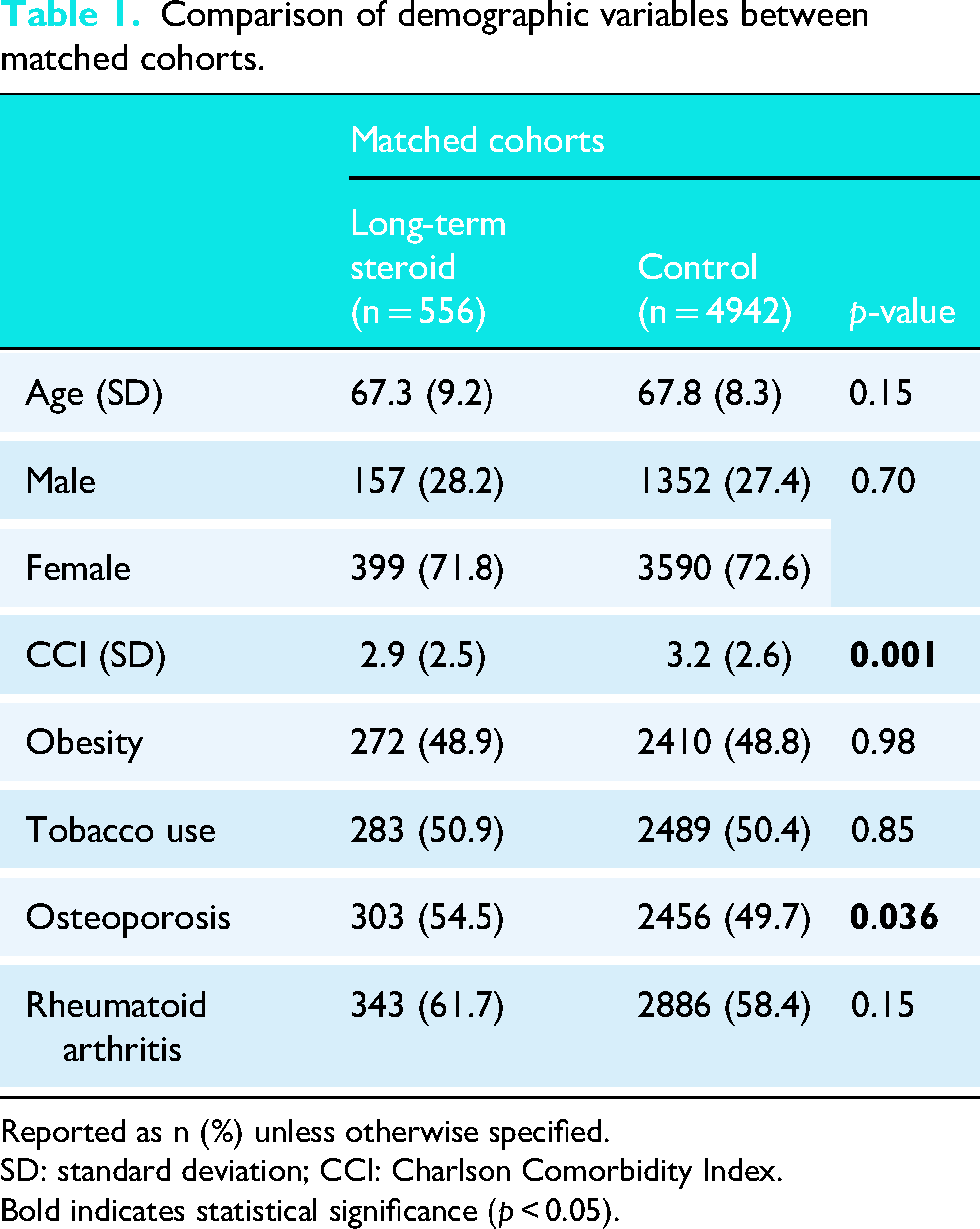
Reported as n (%) unless otherwise specified.
SD: standard deviation; CCI: Charlson Comorbidity Index.
Bold indicates statistical significance (p < 0.05).
90-Day complications
Multivariable logistic regression demonstrated that patients on LTCs experienced higher rates of pneumonia (OR: 2.91; p < 0.001) and VTE (OR: 2.19; p = 0.001) within 90 days relative to controls (Table 2). There were no differences in other 90-day medical complications between groups, including myocardial infarction, UTI, blood transfusion, wound dehiscence, AKI, ED visits, and readmissions.
Comparison of 90-day complications between groups.
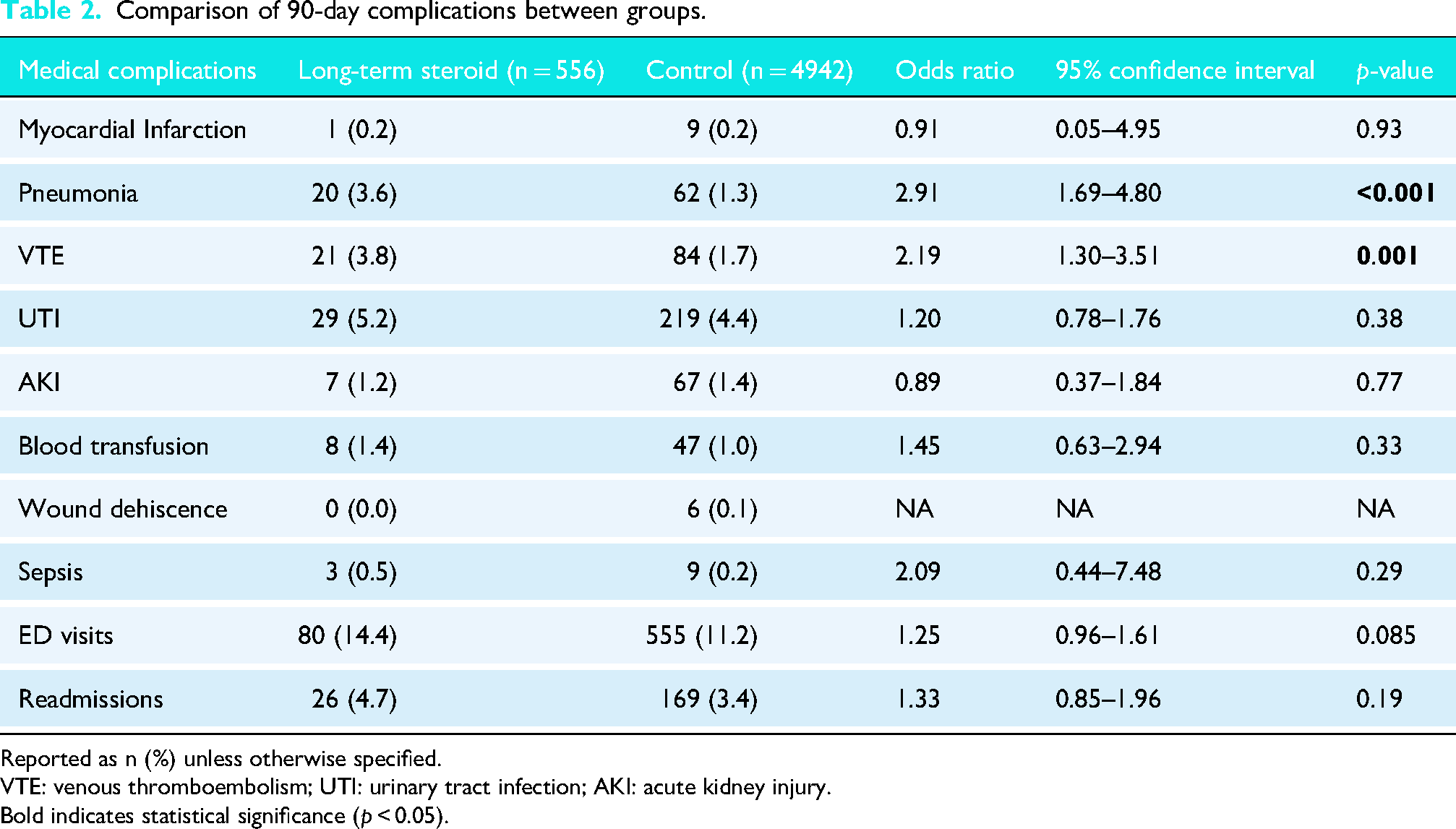
Reported as n (%) unless otherwise specified.
VTE: venous thromboembolism; UTI: urinary tract infection; AKI: acute kidney injury.
Bold indicates statistical significance (p < 0.05).
5-Year complications
Multivariate analysis demonstrated that patients on LTCs did not experience any statistically significant differences in the incidence of any surgical complications relative to matched controls, including all-cause revision, PJI, aseptic loosening, periprosthetic fracture, dislocation, or stiffness within 5 years (Table 3).
Comparison of 5-year complications between groups.
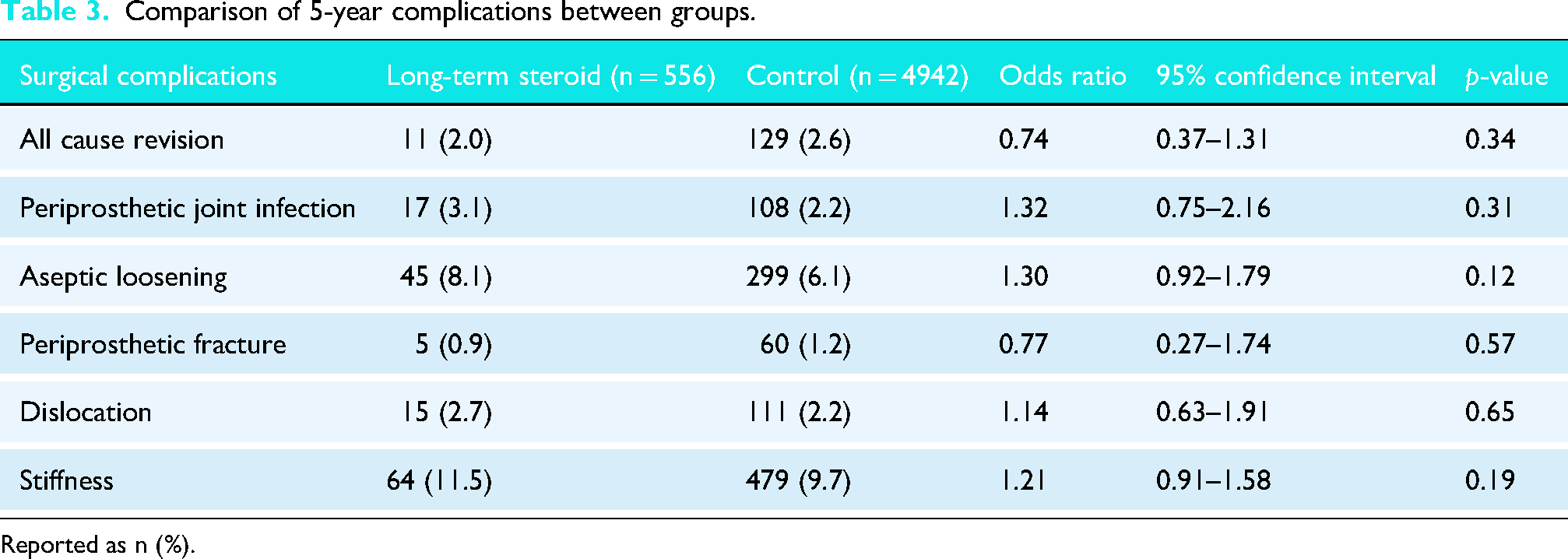
Reported as n (%).
Discussion
The main finding of this study was that patients on LTC therapy had higher rates of VTE and pneumonia within 90 days of TSA compared to controls, but there were no differences in 5-year complications between the groups. While the adverse short-term outcomes of this study are substantiated by prior literature, the long-term findings of this study are unique, as LTC use has been consistently identified as a risk factor for long-term complications following other types of joint arthroplasty.8,11
The increase in short-term complications observed in this study is supported by prior literature. Multivariable regression analysis revealed that LTC use was associated with 90-day medical complications following TSA, including a 2.91- and 2.19-times increased risk for pneumonia and VTE, respectively. These findings align with previous studies which have reported increased postoperative pneumonia rates among LTC patients who underwent lower extremity TJA, as well as in patients who underwent lower extremity revascularization procedures.11,19 The immunosuppressive effects of corticosteroids are well-documented, with their use being associated with an increased risk of infectious complications, such as pneumonia.20,21 Therefore, the higher incidence of pneumonia observed among TSA patients on LTC therapy is likely attributable to the immunosuppressive properties of these drugs.
In addition to the increased risk of pneumonia, LTC use was associated with an increased risk of VTE following TSA. These results are consistent with the results of studies by Chamseddine et al. and White et al., which found higher short-term DVT risk among LTC patients after lower extremity bypass surgery and adult spinal deformity surgery, respectively.19,22 Mechanistically, glucocorticoid therapy has been associated with a marked increase in clotting factors VII, VIII, and XI, which have been suggested as contributory to thromboembolic events experienced by patients on these medications. 23 Further research is warranted to explore the mechanism by which corticosteroid use may be associated with increased risk for VTE, both post-operatively and generally. Collectively, these findings demonstrate that LTC users may face a heightened risk of short-term medical complications after TSA and may benefit from more intensive postoperative monitoring or preoperative adjustments in thromboembolic prophylaxis and antibiotic regimens.
To the authors’ knowledge, this is the first study to evaluate long-term complications for LTC patients undergoing TSA, but several studies have identified an increased risk of surgical complications for patients on LTC therapy undergoing THA and TKA. Kittle et al. identified an increase in 30-day postoperative infection rates in a large database study of patients with LTC use who underwent THA or TKA. 11 Haft et al. also evaluated 10-year surgical outcomes for LTC patients who underwent TKA and found that they were more likely to experience fragility fracture, all-cause revision, and PJI. 8 In contrast, our analysis of TSA patients on LTC therapy did not find an increased risk of complications over a 5-year postoperative timeframe. Previous studies have evaluated overall complication rates for TSA patients compared to patients who underwent THA or TKA and found that TSA patients have lower rates of short-term adverse postoperative outcomes.24–26 These studies were performed without specifying for corticosteroid use and suggest that TSA patients may be at a lower baseline risk for surgical complications than THA or TKA patients. However, there is a paucity of literature regarding the potential causes for this association, and future research should assess the possibility of this difference between TSA and THA or TKA patients. Future studies should also consider a time-to-event analytic framework such as Cox proportional hazards regression with a formally defined time-at-risk, which would allow inclusion of LTC-exposed patients across a broader range of follow-up durations and could detect time-to-event differences between cohorts that this study is not specifically designed to identify. Further investigation is necessary to understand the impact of LTC use on TSA patients, and whether an intervention such as a preoperative steroid taper or time-dependent cessation would influence complications following TSA.
The cumulative incidence of specific 5-year surgical complications exceeds the all-cause revision rate (Table 3). This reflects the methodology of this analysis. Specific complications were captured by ICD-10 codes in any postoperative encounter, whereas all-cause revision was captured independently by separate CPT and ICD codes (Supplemental Information 1). Many shoulder arthroplasty complications are managed non-operatively or by procedures other than formal component revision. PJI is frequently managed with intravenous antibiotics, chronic suppressive antibiotic therapy, or debridement with implant retention. Aseptic loosening may be diagnosed radiographically and managed expectantly, particularly in asymptomatic or low-demand patients. Dislocation is commonly addressed initially via closed reduction. Thus, this discrepancy may be explained by the study design and CPT/ ICD coding practice.
There are several limitations to this study. First, causation between LTC use and either short or long-term complications was unable to be established due to the inherent nature of a retrospective cohort study as well as the granularity of clinical information able to be obtained from a large database, which is limited to data available from CPT and ICD codes. Second, LTC use was defined using ICD codes and confirmed with an active oral corticosteroid prescription, but it is possible that this study included patients who may have been LTC users at an earlier time point, stopped LTC use, and were again actively on short-term oral corticosteroids prior to surgery. Our database did not allow us to exclude these patients, and we were unable to determine the dose, type, and lifetime duration of the corticosteroids given to patients. Similarly, given the nature of the data, it was not possible to account for if the patients tapered or stopped usage perioperatively. Third, we were unable to account for variation that may have occurred during surgery, including possible intraoperative complications, type of hardware used, and surgical technique. Fourth, despite propensity score matching for osteoporosis, the LTC cohort had significantly higher rates of osteoporosis and a lower CCI. We attempted to correct for these differences in the multivariable regression to control for each of these variables, but it is also worth noting that a lower CCI in the LTC cohort suggests that patients in our study on LTC use were not necessarily sicker and at higher risk of complications to begin with. While matching for osteoporosis helped to isolate the effects of LTC use, it is possible that this methodology may have minimized any possible contributions of corticosteroid-induced osteoporosis on the negative outcomes discussed in this paper. 27 Lastly, the CPT codes do not distinguish between reverse and anatomic TSA. LTC use is known to have detrimental effects on tendon strength. 28 Therefore, the effect size of LTC use may vary between a soft tissue independent reverse TSA and a soft tissue dependent anatomic TSA. Despite these limitations, this study provides valuable insight into the effect of LTC use on outcomes following TSA.
Conclusion
This large database, propensity-matched retrospective cohort study provides valuable insight into how LTC use may be associated with long-term outcomes following TSA. LTC patients who underwent TSA were more likely to experience pneumonia and VTE within 90 days compared to controls. However, there were no significant differences in 5-year outcomes following TSA between LTC users and controls. While patients on LTCs may require closer monitoring in the short-term, their long-term outcomes remain largely like patients without LTC use.
Supplemental Material
sj-docx-1-sel-10.1177_17585732261460807 - Supplemental material for Long-term corticosteroid use elevates 90-day medical complications but not 5-year surgical complications after shoulder arthroplasty
Supplemental material, sj-docx-1-sel-10.1177_17585732261460807 for Long-term corticosteroid use elevates 90-day medical complications but not 5-year surgical complications after shoulder arthroplasty by Joshua A Holmstrom, Annika N Hiredesai, Alejandro M Holle, Collin L Braithwaite and Jeffrey D Hassebrock in Shoulder & Elbow
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Previous communication
This article is not based on a previous communication to a society or meeting.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.