
Abstract
Background
This study explores the relationship between thoracic sagittal kyphotic alignment, quantified by the Cobb angle, and postoperative shoulder function, specifically assessing whether the presence and severity of thoracic kyphosis influence clinical outcomes and range of motion (ROM) in patients undergoing reverse shoulder arthroplasty (rTSA).
Methods
A retrospective review was conducted on 110 patients who underwent rTSA from 2020 to 2022 at a single institution. Sagittal kyphosis was quantified on preoperative chest radiographs. Clinical outcomes were measured using the visual analog scale (VAS), constant score (CS), simple shoulder test, Single Assessment Numeric Evaluation (SANE) score, and pre- and postoperative ROM. Patients were separated into three groups based on Cobb angle severity (0–36°, 37–46°, ≥47°) and followed for a minimum follow-up of 2 years. A p-value <0.05 was considered statistically significant.
Results
Patients with a Cobb angle ≥47° exhibited a significant reduction in flexion (132.7° vs 149.4° for Cobb ≤36°; p = 0.031) and abduction (122.9° vs 142.1°; p = 0.035). This group also showed lower mean CSs (75.1 vs 83.3; p = 0.048). No significant differences were observed among groups in SANE or VAS pain scores.
Conclusion
Greater thoracic kyphosis is associated with reduced functional outcomes and diminished flexion and abduction following rTSA. These findings suggest that sagittal spinal alignment may influence postoperative shoulder performance.
Level of evidence
Retrospective Cohort Comparison III.
Introduction
Reverse shoulder arthroplasty (rTSA) is a well-established surgical intervention for managing complex shoulder pathologies, particularly in patients with rotator cuff arthropathy, advanced osteoarthritis, or irreparable rotator cuff tears.1–4 Several biomechanical parameters influence rTSA outcomes, including glenosphere diameter, inferior glenosphere overhang, glenoid lateralization, reduced humeral neck-shaft angle, and humeral lateralization.5–10 However, emerging evidence suggests that spinal alignment, particularly thoracic kyphosis, may significantly impact both the biomechanics and clinical outcomes of this surgical treatment.11,12
A growing body of literature has underscored the intricate relationship between spinal posture and shoulder function. The thoracic spine plays a pivotal role in upper limb mobility, serving as a fundamental component in maintaining scapular position and optimizing shoulder range of motion (ROM).13,14 Conversely, the shoulder complex also contributes to thoracic and cervical spine mobility. Proper thoracic extension is essential for achieving full shoulder elevation, with studies indicating that approximately 9–15° of thoracic extension is required for complete bilateral shoulder flexion in both younger and older populations.15,16 However, interindividual variability and pathological conditions, such as kyphosis, may significantly alter these parameters. 17
The work of Moroder et al. has highlighted the clinical implications of this association, demonstrating that patients with posture type C (characterized by increased scapular internal rotation (IR), anterior tilt, downward rotation, protraction, and drooping, along with thoracic kyphosis and a barrel-shaped chest) experience significant deficits in abduction and flexion following rTSA.18,19 This can be attributed to the increased mechanical challenge of overhead arm elevation in individuals with a more horizontally oriented scapula relative to the vertical body axis, which alters deltoid efficiency and compromises scapulothoracic rhythm. Despite these limitations in elevation, rotational movement outcomes appear to remain consistent across different posture types.
Beyond its impact on postoperative ROM, thoracic kyphosis may also contribute to altered load distribution across the shoulder joint, predisposing patients to an increased risk of complications such as glenoid component loosening, scapular notching, acromial stress fractures, and impaired prosthetic longevity. Furthermore, kyphotic posture may lead to compensatory changes in scapular kinematics, increasing shear forces on the glenoid component and reducing the mechanical advantage of the deltoid muscle, ultimately affecting functional recovery and patient satisfaction.
Given the expanding indications and increasing utilization of rTSA, a substantial proportion of treated patients are older adults in whom thoracic kyphosis is prevalent. 20 Therefore, clarifying the impact of thoracic sagittal alignment on postoperative shoulder function is clinically relevant
The purpose of the study was to assess the impact of the severity of thoracic kyphosis on clinical outcomes and ROM in patients undergoing rTSA.
Materials and methods
From March 2016 to January 2025, prospectively collected data from 110 patients who underwent rTSA by senior surgeons of the group were retrieved from the Fondazione Policlinico Universitario Campus bio-Medico (FP-UCBM) Shoulder Study Group database and included in this retrospective cohort study. Preoperative data were gathered retrospectively, while postoperative data were collected prospectively. Inclusion criteria were as follows: (a) primary rTSA procedure, (b) age >65 years at the time of surgery, (c) patients with preoperative standing chest radiographs in posteroanterior and lateral projections encompassing the cervicothoracic junction and upper lumbar spine. These radiographs were routinely obtained as part of the institutional preoperative anesthesiologic and cardiopulmonary evaluation protocol (d) a minimum of 2 years of clinical and radiographic follow-up. 21 Ethical approval for this study was obtained from the Campus Bio-Medico Ethical Committee (study no. GR7009).
The exclusion criteria included: revision surgery, infection, fractures, the absence or suboptimal quality of preoperative imaging, and patients under 65 years of age. Surgical indications included eccentric cuff tear arthropathy, eccentric glenohumeral osteoarthritis, and irreparable, nonfunctional rotator cuff tears.
Functional assessment and radiographic analysis
Functional outcomes and shoulder ROM were assessed at the final follow-up using the simple shoulder test (SST), the Constant-Murley Score (CS), the visual analog scale (VAS) for pain, and the Single Assessment Numeric Evaluation (SANE) score.
ROM was evaluated in degrees of flexion, abduction, and external rotation in adduction. The IR was characterized in points based on the functional shoulder-specific CS. A goniometer was used to evaluate the flexion and abduction angles pre-operatively and at the final follow-up. All patients underwent preoperative chest X-ray imaging as part of the pre-hospitalization evaluation, and postoperative clinical assessment was performed at follow-up. Preoperative chest radiographs were independently reviewed by a fellowship-trained shoulder surgeon and two orthopedic residents. Measurements were repeated by the same observers after a 1-week interval. The final Cobb angle was determined by calculating the mean of the three independent measurements. To validate this approach, inter-rater and intra-rater reliability were assessed, yielding intraclass correlation coefficient values of 0.93 and 0.91, respectively, indicating excellent agreement. To minimize measurement bias, the final Cobb angle used for statistical analysis was the mean value of the three independent assessments. Imaging was analyzed in DICOM format or using the Horos software (Pixmeo, Bernex, Switzerland) to calculate the Cobb angle. Patients were stratified into three groups using the Maximally Selected Rank Statistics method. Since universally accepted clinical cut-offs for kyphosis impacting shoulder kinematics are not established, this objective, data-driven approach was used to identify the optimal Cobb angle thresholds that demonstrated the greatest influence on the primary functional outcome (constant score (CS)), thereby minimizing investigator bias in group allocation.
Each patient (n = 110) was then stratified into:
Group A: Cobb angle ≤36°, Group B: 37° < Cobb angle < 46°, Group C: Cobb angle ≥47°.
The Cobb angle was defined as the angle between the superior endplate of the T4 vertebra and the inferior endplate of the T12 vertebra, measured by drawing lines parallel to the respective endplates using anterior and posterior morphometric landmarks 21 (Figure 1).
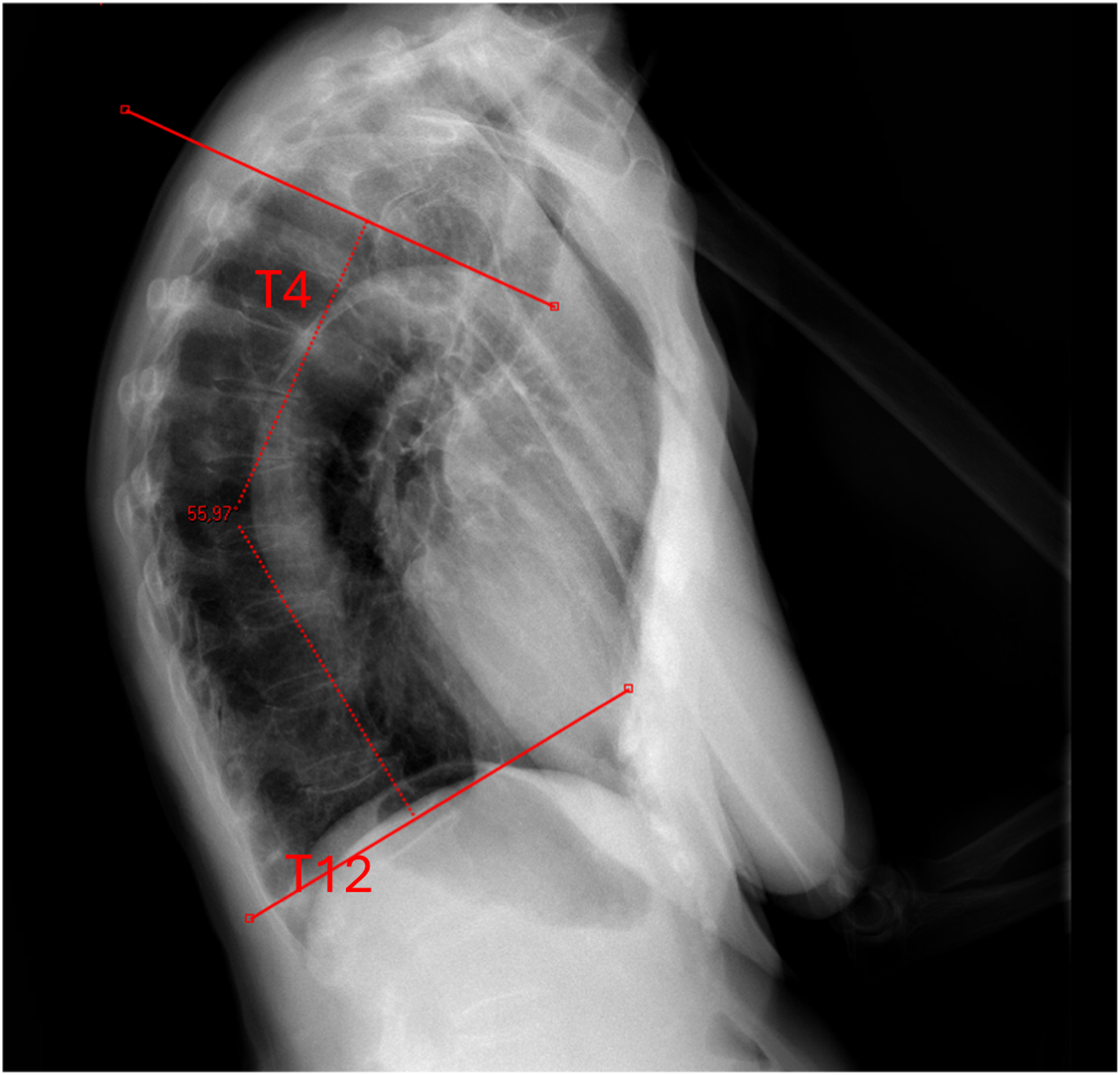
The Cobb angle was defined as the angle between the superior endplate of the T4 vertebra and the inferior endplate of the T12 vertebra, measured by drawing lines parallel to the respective endplates using anterior and posterior morphometric landmarks.
Data analysis
Descriptive statistics were calculated as percentages, means, and standard deviations for all variables. Chi-square test and repeated-measures analysis of variance (ANOVA) were used to compare demographic characteristics across the three Cobb angle groups. ANOVA was then performed to assess differences in CS, its individual components, SST, SANE, VAS, and ROM parameters (flexion and abduction) across the three groups. The significance level was set at p = 0.05. A post hoc power analysis was performed, demonstrating that the study achieved a power greater than 80% to detect the observed differences among the three groups in CS, flexion, and abduction. All data analyses were performed using STATA 18 Software (StataCorp LLC, College Station, USA).
Results
One hundred and thirteen patients met the inclusion criteria. Three patients were excluded because the quality of the chest radiograph did not allow the calculation of the Cobb angle. Of the remaining patients, 110 completed the follow-up and represented our final cohort. There were 72 female (65.5%) and 38 male (34.5%) patients, with a mean age of 72.3 ± 5.1 years and a body mass index of 28.2 ± 3.5 kg/m2, and the mean follow-up was 32 ± 4 month. Group A included 37 patients, group B 31 patients, and Group C 42 patients (Figure 2). Comparative analysis between the groups showed no statistically significant differences in mean age, sex, BMI, functional scores, pain (VAS), or ROM (Flexion and Abduction) (p > 0.05) (Table 1).
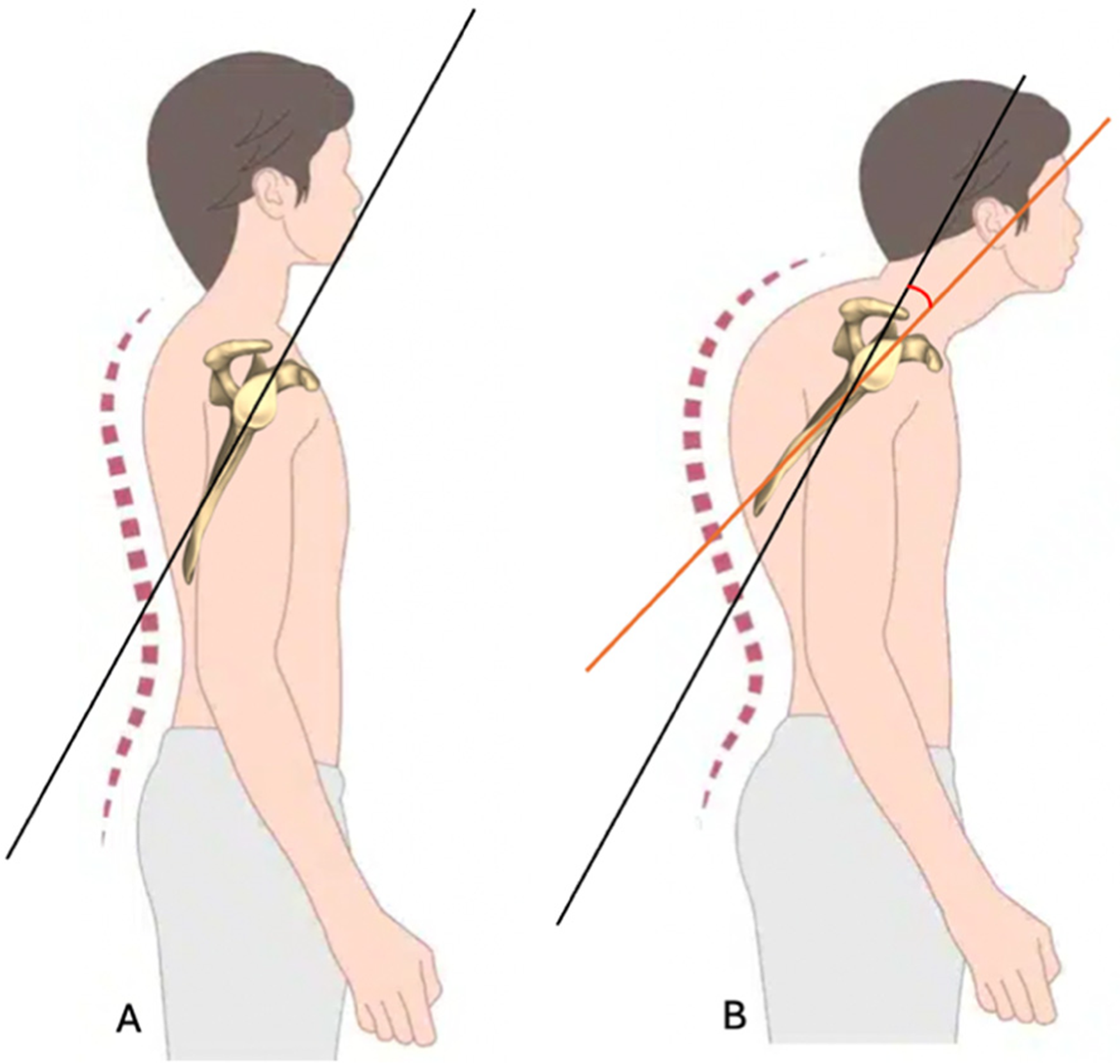
Illustration of different posture types. From A (normal) to B (increased kyphosis) patients show increasing scapular internal rotation, anterior tilt, and protraction.
Demographic characteristics.
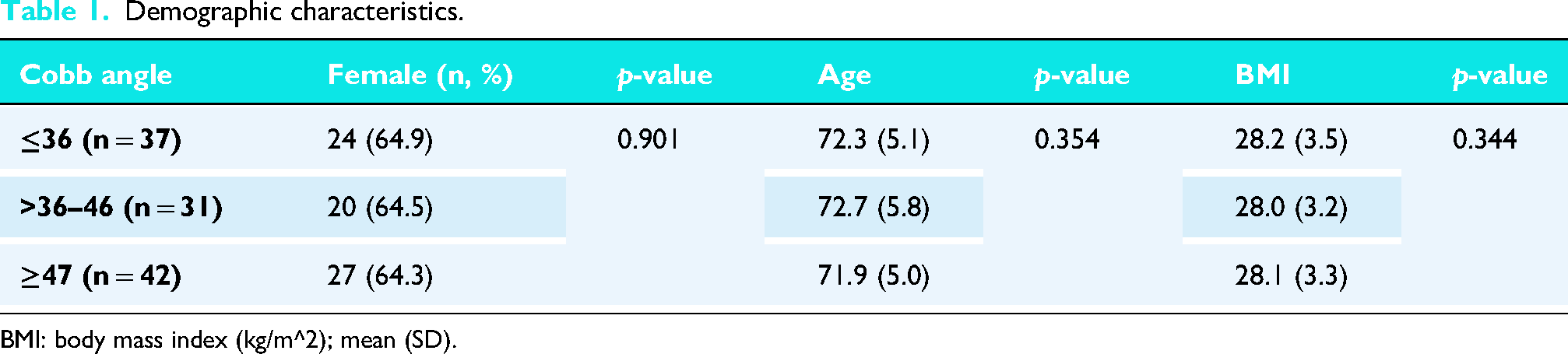
BMI: body mass index (kg/m^2); mean (SD).
There was a significant correlation between the Cobb angle and the CS, with patients presenting a Cobb angle ≤36° showing a mean CS of 83.3, compared to a mean CS of 75.1 in patients with a Cobb angle ≥47° (p = 0.048). A reduction in the SST score was also observed, with a mean value of 9.8 in patients with a Cobb angle ≤36°, compared to a mean value of 9.1 in those with a Cobb angle ≥47° (p = 0.355). No statistically significant differences were found in the SANE score or pain assessment using the VAS among the three patient groups (Table 2-3).
Clinical outcomes.
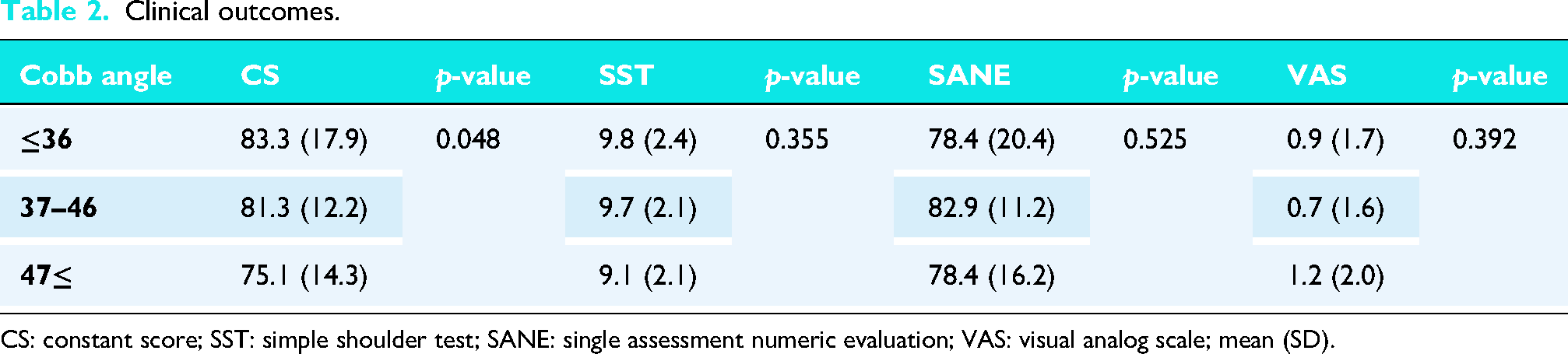
CS: constant score; SST: simple shoulder test; SANE: single assessment numeric evaluation; VAS: visual analog scale; mean (SD).
Constant score.
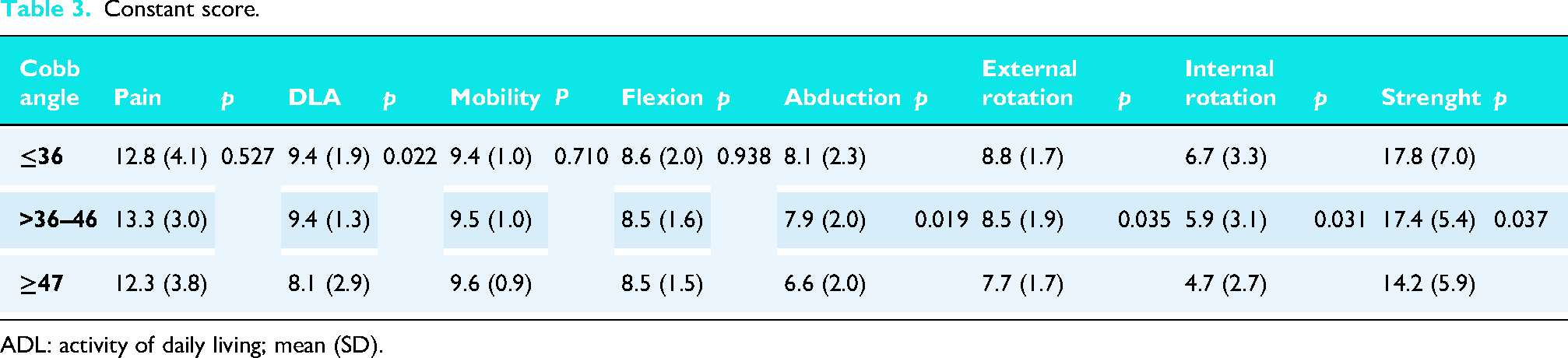
ADL: activity of daily living; mean (SD).
Furthermore, patients with a Cobb angle ≥47° showed a significant reduction in shoulder flexion (132.7° vs. 149.4° in patients with Cobb angle ≤36°; p = 0.031) and abduction (122.9° vs. 142.1°, respectively; p = 0.035) (Table 4, Figure 3).
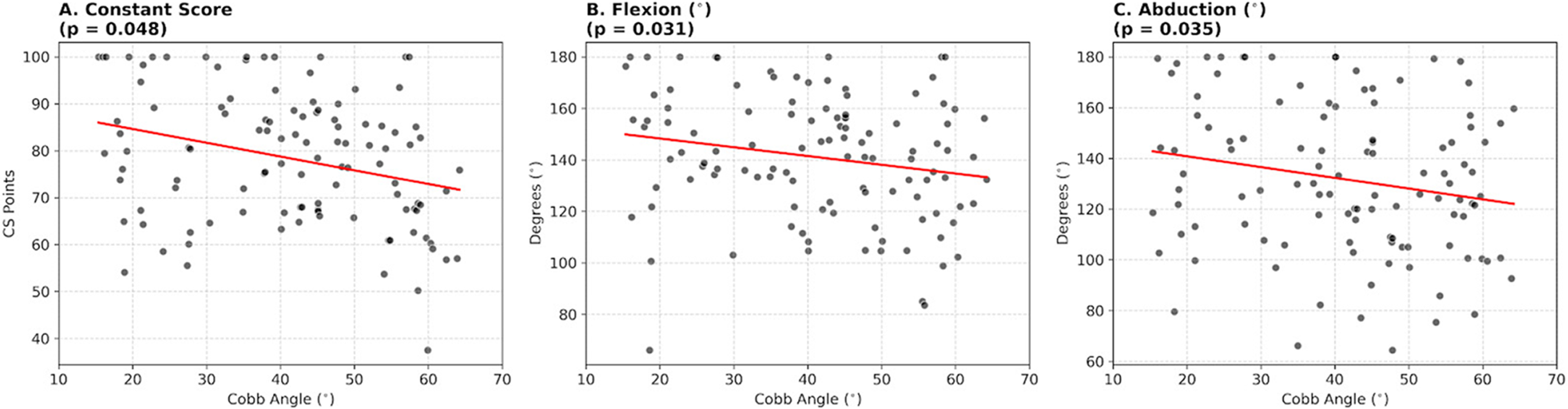
Scatter plots illustrating the relationship between the Cobb angle and (A) constant score, (B) Flexion, and (C) Abduction.
Flexion and abduction.
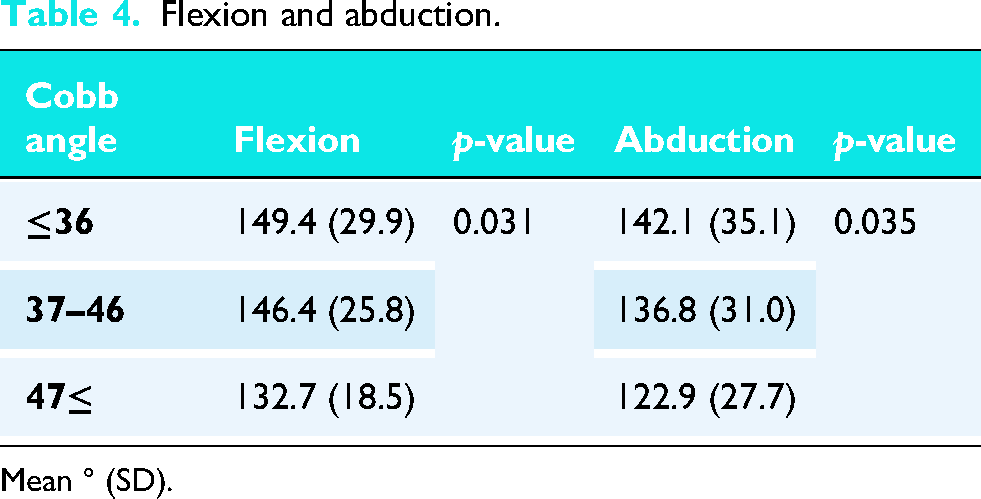
Mean ° (SD).
Discussion
In surgical practice and preoperative planning for rTSA, multiple biomechanical and anatomical factors are considered to optimize implant selection and improve patient outcomes.22–25 However, the influence of thoracic kyphosis on postoperative shoulder function has not been thoroughly integrated into standard preoperative assessment protocols. The present study highlights the impact of kyphosis severity on both postoperative ROM and overall clinical outcomes, reinforcing the importance of spinal alignment in the management of patients undergoing rTSA.
Impact of kyphosis on shoulder function
Our findings corroborate previous hypotheses proposed by Moroder et al., demonstrating that patients with increased thoracic kyphosis exhibit significant deficits in abduction and flexion.18,19
Notably, our study revealed a more pronounced reduction in abduction compared to flexion.
One possible explanation for this finding is that increased thoracic kyphosis alters scapulothoracic orientation, leading to increased scapular anterior tilt and IR, which may reduce the mechanical efficiency of shoulder elevation after rTSA. Patients with a Cobb angle ≥47° exhibited a mean flexion of 132.7°, compared to 149.4° in those with a Cobb angle ≤36°. Similarly, the mean abduction was 122.9° in patients with a Cobb angle ≥47°, whereas it reached 142.1° in those with a Cobb angle ≤36°. This observation may suggest that kyphotic posture influences scapulohumeral mechanics during shoulder elevation, potentially affecting movements requiring coordinated scapular upward rotation and glenohumeral motion.
Biomechanical mechanisms underlying the correlation between kyphosis and shoulder ROM
The relationship between thoracic kyphosis and shoulder ROM can be explained by several biomechanical mechanisms. Firstly, excessive kyphosis is associated with increased scapular protraction and downward rotation , which in turn contributes to subacromial tissue compression beneath the acromion. This positional alteration predisposes patients to mechanical impingement and may exacerbate degenerative changes surrounding soft tissues.
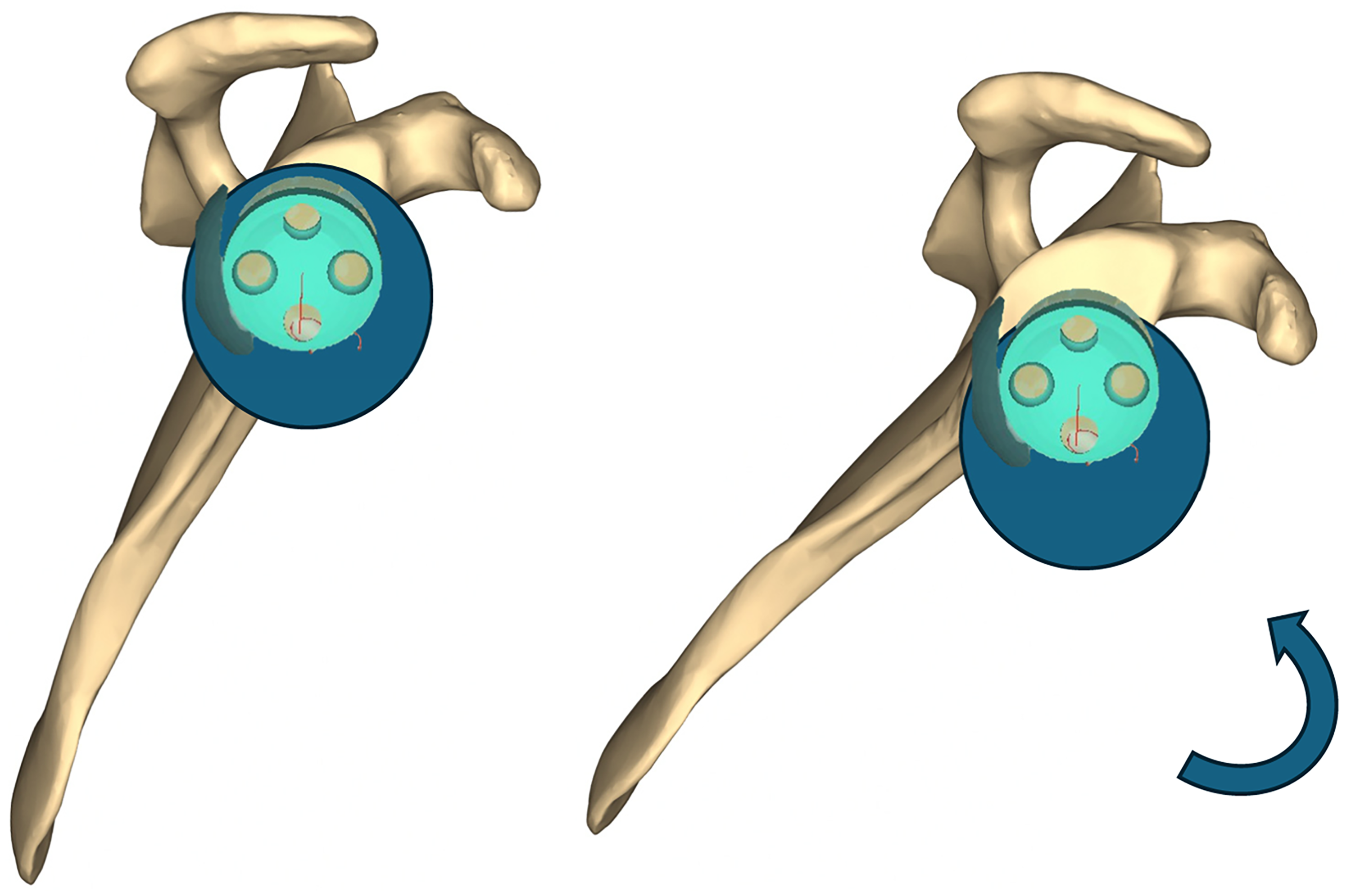
In patients exhibiting kyphosis with increased forward tilt of the scapula, it is advisable to position the glenosphere's eccentricity not directly at the inferior (“South”) glenoid point, but rather toward the antero-inferior zone of the glenoid, which generally aligns between the 4 and 5 o’clock position. This strategy could adapt to the altered scapular alignment and helps minimize impingement and notching.
Secondly, thoracic spine extension plays a crucial role in facilitating full shoulder elevation; therefore, restricted thoracic mobility due to kyphosis compromises overall scapulohumeral rhythm and limits functional overhead motion.26–29
Furthermore, anteriorly tilted scapular position associated with kyphosis disrupts scapulothoracic muscle dynamics, particularly affecting the force couples between the serratus anterior, lower trapezius, and upper trapezius. This imbalance in patients without rTSA has been associated with an increased risk of shoulder impingement syndrome and rotator cuff pathology.30–32 Therefore, understanding this relationship in patients who have undergone rTSA is of particular interest.33,34 Finally, muscle strength and flexibility are key determinants of scapular kinematics and shoulder ROM. In particular, serratus anterior weakness and pectoralis major tightness contribute to increased anterior scapular tilt and protraction, further exacerbating the biomechanical disadvantages associated with kyphosis. 35
Implant positioning implications
As suggested by Moroder et al., 19 scapular orientation and overall posture should be key considerations when determining the appropriate retrotorsion of the humeral component in rTSA. Theoretically, increasing humeral component retrotorsion can enhance neutral alignment between rTSA components in patients with pronounced scapular IR. Based on the variability in scapular positioning, they proposed categorizing patients into three distinct postural types (A–C) to better assess and account for scapulothoracic orientation during surgical planning. Moreover, since one of the primary goals in rTSA is to prevent scapular notching, which has been associated with decreased implant longevity and poorer functional outcomes, special attention must be given to glenosphere positioning. In patients with kyphosis and consequently increased anterior tilt of the scapula, we recommend that the glenosphere be positioned as low as possible, not strictly to the inferior 6 o’clock position of the glenoid but rather toward the antero-inferior zone, which is typically oriented around 4 to 5 o’clock position. This adjustment could better accommodate altered scapular anatomy and reduce the risk of impingement and notching. We suggest that this finding may have potential clinical implications; however, this remains a conceptual and hypothesis-generating consideration that is not directly supported by the present data and requires further investigation (Figure 4). In patients with severe thoracic kyphosis undergoing rTSA, a potential approach could involve attempting to improve spinal alignment through postural exercises and bracing. Optimizing thoracic posture may positively influence scapular orientation and, consequently, shoulder function. However, given the advanced age of most patients indicated for this procedure, spinal deformities are often fixed or would require prolonged treatment and a level of patient compliance that is rarely achievable in routine clinical practice. Therefore, while postural correction remains a theoretically valuable adjunct, its practical application in this patient population is limited. A more feasible and potentially impactful strategy may be to focus on postural rehabilitation in the postoperative phase, with the goal of enhancing shoulder biomechanics and promoting the long-term durability of the prosthetic implant.
Clinical implications for rTSA patients
Our study extends the existing literature by demonstrating a direct association between kyphosis severity and functional outcomes following rTSA. The observed reduction in postoperative ROM among kyphotic patients has meaningful implications for daily function. Notably, we found a statistically significant decrease in the ADL scores in patients with a Cobb angle ≥47°, highlighting the functional limitations imposed by reduced ROM in performing overhead and reaching tasks.
Interestingly, despite these biomechanical and functional differences, our analysis did not reveal a significant variation in postoperative pain levels among kyphotic and non-kyphotic patients. Similarly, no significant differences were observed in the SANE score between groups, despite the differences in ROM and CS. Given that the SANE score has been proposed as a reliable indicator of overall shoulder function, 36 this finding may suggest that increased thoracic kyphosis primarily affects specific biomechanical aspects of shoulder performance rather than the patient's perceived global shoulder function.
These findings underscore the complex relationship between mechanical dysfunction and patient-reported outcomes, suggesting that while spinal curvature may influence mechanical efficiency, it does not necessarily correlate with increased postoperative discomfort or perceived functional limitation. Importantly, postoperative pain was generally well controlled across all patients, further supporting the efficacy of modern rTSA techniques in providing reliable pain relief.37,38
Limitations and future directions
While our study provides valuable insights into the role of kyphosis in rTSA outcomes, it has several limitations. First, our follow-up period was relatively short, limiting our ability to assess long-term functional adaptations. Future research should aim to extend follow-up to 5 and 10 years postoperatively to better understand the long-term influence of thoracic kyphosis on functional outcomes after rTSA.
Second, kyphosis measurements were based on preoperative chest radiographs, which may provide less precise Cobb angle estimations than computed tomography (CT)-based assessments. Incorporating CT imaging could enhance accuracy and allow for a more detailed three-dimensional analysis of spinal alignment and its impact on shoulder mechanics. However, this would expose patients to a higher amount of radiation. Although we did not assess bone mineral density (BMD) in our patient population, it is well-established that thoracic kyphosis is strongly influenced by the presence of osteoporosis. The potential relationship between reduced BMD and greater degrees of kyphosis represents an important area for future investigation. Evaluating BMD in similar cohorts could help clarify the role of osteoporosis in the progression of spinal curvature and further highlight the need for early diagnosis and treatment of bone fragility. Another potential limitation is that patients with lower Cobb angles may present less overall spinal degeneration and therefore better global functional status, which could partially influence CS values despite it being a shoulder-specific outcome measure.
Additionally, patients with different underlying pathologies leading to rTSA were included in the present cohort. As preoperative diagnosis and surgical indication may influence postoperative ROM and clinical outcomes, the lack of stratification according to underlying pathology represents a potential confounding factor and should be considered when interpreting the results.
The representativeness of the underlying cohort is limited, as the data were derived from patients treated by only two surgeons. This may introduce bias due to the low variability in surgical techniques. Longer follow-up studies are warranted to determine the progression of clinical outcomes over time and to better understand their correlation with thoracic alignment. Lastly, a single implant was used underling a possible lack of reproducibility of these results for patients with different prosthesis configuration.
Additionally, patient stratification was performed using data-driven cut-offs derived from Maximally Selected Rank Statistics. While these thresholds are consistent with recognized clinical ranges for kyphosis, we acknowledge that they were optimized based on the current cohort's functional outcomes. Future prospective studies are needed to validate these specific cut-offs as independent clinical predictors.
Finally, a crucial next step will be to anatomically investigate the correlation between the Cobb angle, anterior scapular tilt, and scapular IR. Understanding these interrelationships would enhance our ability to refine preoperative planning strategies and optimize implant positioning in kyphotic patients undergoing rTSA.
Conclusion
Thoracic kyphosis significantly impacts postoperative function after rTSA, with greater kyphotic deformity correlating with reduced ROM and lower functional performance, particularly in abduction and flexion. Further studies are needed to clarify the clinical relevance of thoracic alignment in patients undergoing rTSA.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.