
Abstract
Background
Lateral elbow tendinopathy (LET) is the most common musculoskeletal elbow disorder. Evidence suggests that cervicothoracic involvement often contributes to forearm symptoms and that addressing the spine improves clinical outcomes. This review aimed to evaluate screening methods for the cervicothoracic spine in randomized controlled trials (RCTs) that evaluated and treated LET.
Methods
This review included RCTs from PubMed, CINAHL, and CENTRAL (inception to 10 June 2025) that evaluated conservative interventions for adults with a primary diagnosis of LET. Data on cervicothoracic spine screening methods were categorized into three levels: thorough (≥4 screening items), partial (1–3 items), or no screening. Frequencies reported the extent of screening across trials.
Results
A total of 2744 articles were retrieved, and 208 RCTs were included for data extraction. Four (1.9%) RCTs adequately reported a thorough cervicothoracic screening process before diagnosing LET, based on predefined screening criteria. A total of six trials (2.9%) were partially screened, while many (95.2%) reported no screening.
Discussion
Less than 2% of LET RCTs did not perform or explicitly report objective screening of the cervicothoracic region, highlighting a need for standardized screening protocols to better characterize participants in future research and clarify the role of the cervicothoracic spine in LET outcomes.
Keywords
Introduction
Lateral elbow tendinopathy (LET) is the most common elbow musculoskeletal disorder, associated with significant functional decline, increased disability, and overall productivity loss. 1 LET has been estimated to affect up to 3% of the population, 2 with typical signs and symptoms including lateral forearm pain, tenderness over and distal to the lateral epicondyle of the humerus, pain with resisted wrist extension and forearm supination, and difficulties with grip strength and activities of daily living. 2 The clinical examination of LET is relatively straightforward, typically involving palpation, assessing pain with resisted wrist and forearm movements, and performing special tests targeting the lateral epicondyle of the humerus.3–7 The most common musculoskeletal special tests include Mill's, Maudsley's, and Cozen's, with these tests having varying degrees of validity and reliability.3–8 While a recent American Physical Therapy Association (APTA) clinical practice guideline (CPG) provides recommendations for screening procedures and evidence-based interventions for this condition, 8 the discussion of thoroughly screening the cervicothoracic (CT) spine involvement is minimal.
Evidence supports musculoskeletal clinicians providing conservative treatment as best practice for LET.4,8–11 Coombes et al.'s 10 randomized controlled trial (RCT) showed that physical therapy, including mobilization with movement and exercise, was more effective than a monitoring-only approach or corticosteroid injections in the long-term. Treatment of the cervical spine alongside the elbow has also demonstrated superior outcomes, reinforcing the concept of regional interdependence, a clinical model based on the premise that seemingly unrelated impairments in one anatomical region may contribute to or be associated with the patient's primary complaint in a separate region.4,9,12 In the context of LET, this suggests that the function and health of the CT spine directly influence symptoms and recovery at the elbow. Evidence supports the inclusion of treatment focused on the CT spine for the management of LET; however, CT somatic referred pain has been identified as a significant contributor to upper extremity symptoms, 13 accounting for up to 48% of general cases, and as much as 83% in presentations involving the elbow and forearm. 14 This high prevalence of referred pain from the CT spine potentially raises concerns regarding diagnosis based solely on localized elbow testing or pain location. 15 It is important to clarify that while LET is a distinct clinical diagnosis and not one of exclusion, it may frequently present with comorbid neck pathology. Consequently, failure to perform comprehensively screen of the CT spine may result in clinicians overlooking spinal contributors that mimic or coexist with local elbow symptoms. 13 Although there is support regarding regional interdependence for the management of LET, demonstrating that CT spine interventions combined with local elbow treatment yield superior outcomes compared with elbow treatment alone,9,12 it is important to consider whether these improvements truly reflect regional interdependence or instead highlight a subset of patients with LET who present with a CT spine-dominant nociceptive and possible nociplastic pain phenotype that responds preferentially to CT-directed interventions.
To date, existing literature has not established a formal, standardized objective clinical screening process for the CT spine for cases of LET. However, interest in spinal screening is growing, as evidenced by recent work on cervical spine involvement in shoulder pain, as well as sacroiliac joint (SIJ) pain and the thoracolumbar spine.4,5,16–21 Requejo-Salinas et al. 18 conducted a Delphi study developing a standardized cervical screening protocol when evaluating shoulder pain, expanding on earlier findings by Walker et al., 19 who analyzed cervical spine screening procedures in RCTs involving subacromial pain syndrome (SAPS), noting a considerable gap with nearly 75% of trials not screening the cervical spine. Requejo-Salinas et al. 18 emphasized that cervical spine assessment is not intended as universal screening, but rather a clinically guided process, where findings from the subjective examination, such as symptom distribution, aggravating/easing factors, and relevant historical features, are used to determine the need for subsequent objective CT assessment. This highlights that standardized cervical screening should be considered a structured, symptom-informed pathway rather than a blanket approach, with the subjective examination serving as the primary decision-making driver for further testing. Additionally, over 95% of RCTs evaluating treatment effects for SIJ pain did not formally assess the thoracolumbar spine. 21 While the association between screening and patient outcomes is complex and depends on subsequent treatment, the lack of assessment data complicates the interpretation of whether the SIJ was the primary source of symptoms. 21 The absence of a standardized screening process, combined with the prevalence of CT spine pain referring to the forearm and the high success rates of CT-based treatments, supports a need for further investigation into screening methods used for managing LET.
A recent cross-sectional international survey of physiotherapists was conducted by Heale et al. 22 to determine the frequency of examination practices used in the clinical assessment and diagnosis of LET. They highlighted a concerning trend, including the lack of assessment of the CT spine, which was deemed “not routine” during the assessment of LET. 22 This is particularly problematic given observed studies identifying the prevalence of silent CT spinal-mediated referred pain to extremity-only symptoms. 14 By identifying possible inconsistencies in current research screening approaches, this review seeks to provide a foundation for incorporating CT spine evaluation, offering a more complete clinical picture to guide future treatment strategies. Given the limited clarity in both research and clinical practice regarding whether the CT spine is adequately assessed before a diagnosis of LET, the purpose of this systematic review was to investigate how RCTs address CT spine screening in individuals presenting with LET. These findings may help identify inconsistencies in current screening approaches within the literature and inform recommendations for incorporating CT spine screening when evaluating patients with LET, offering a more complete clinical picture that may help guide future treatment strategies.
Methods
This systematic review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 23 (Supplemental Appendix A) and was registered a priori (PROSPERO registration #CRD420251062883).
Data sources and searches
A search strategy of three databases was conducted on 10 June 2025, including PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Central Register of Controlled Trials (CENTRAL), for studies published from inception to 10 June 2025. The search used All Map Terms to Subject Headings, Medical Subject Headings (MeSH) terms, keywords related to LET, conservative therapy interventions (e.g. manual therapy, muscle energy technique, exercise therapy), and the search term including RCTs. The search strategy included electronic searching of databases for RCTs for individuals diagnosed with LET treated with conservative management in at least one of the experimental groups. The first component of the search used MeSH terms and keywords related to LET in PubMed. The second component searched MeSH terms and keywords related to conservative management interventions commonly performed by musculoskeletal clinicians. The third component searched a combination of MeSH terms and keywords for RCTs. The three main search strategies were then combined into one large search with the Boolean operators AND and OR to identify specific studies relevant to the research question, with details provided in Supplemental Appendix B. Each search strategy was modified and adapted based on the requirements of each specific database.
Study selection
LET was required to be the primary diagnosis of the adult patient population within each RCT. Adjunct interventions (e.g. acupuncture, massage, soft tissue mobilization, instrument-assisted soft tissue, and mechanically assisted manipulation), exercise therapy, and other interventions such as modalities, education, or advice were included. This review also included a placebo or true control group as the comparison group of the study. Any study where non-musculoskeletal-related LET was not the primary diagnosis, was not an RCT, and was not published in English was excluded.
Covidence software (Veritas Health Innovation Ltd, Melbourne, Australia) was used for all data management. 24 Titles, abstracts, and full texts were uploaded to Covidence, where duplicates were removed. Two independent reviewers (KR and DE) performed the title and abstract screening in Covidence to determine eligibility for full-text reviews. Following title and abstract screening, the same two reviewers individually screened the full text of the included studies for final eligibility. Any discrepancies were reconciled by a third reviewer (MS).
Data extraction
Details of each RCT, including title, year of publication, country of origin, primary author, total sample size, and patient demographics, were extracted. Each study's specific screening process was extracted into specific CT spine objective screening categories: (1) no screening, (2) partial screening, and (3) thorough screening, guided by previous literature, helping to guide the extraction process. 21 While all authors discussed, collaborated, and agreed upon the development of the screening process into categories guided by previous literature, two authors (KR and DE) carried out each step of the review process. The authors also extracted data pertaining to the Cochrane Collaboration of Risk-of-Bias Tool for Randomized Trials (RoB 2) for each study.
Assessment of the CT screening process
For the purpose of the review, there were three distinct categories of CT screening processes extracted for each trial. This process was reinforced by a similar study that conducted thoracolumbar screening processes for SIJ pain. 21 First, for an RCT to have performed a thorough clinical CT screening examination, it must have had four or more of the following screening items, as defined by the authors through supporting literature (≥4 examination screening items) including: (1) CT active range of motion with overpressure as appropriate, (2) passive accessory intervertebral motion (PAIVM) assessment in the CT spine (C1-T7), (3) passive physiological intervertebral motion (PPIVM) assessment in the CT spine, (4) a neurological examination (e.g. deep tendon reflexes), (5) a neurodynamics examination (e.g. upper limb tension test), (6) palpation of the CT spine, (7) repeated motion testing (Mechanical Diagnosis & Therapy), (8) special tests related to the CT spine (e.g. Spurling's test), and (9) subjective examination/patient history (Table 1). For a study to be categorized as conducting a partial CT screening process, the RCT would have performed between one and three of the aforementioned screening items. This approach was chosen to observe the extent of screening performed across the literature without mandating a specific combination of items, as the determination of an optimal clinical screening cluster remains a subject for future research. Lastly, if a trial mentioned performing a subjective examination/patient history without a detailed list of physical examination items, or other diagnostic measures not related to the CT screening process, it was categorized as having not performed a CT screening process before coming to a LET diagnosis.
Operational definitions for CT screening categories.
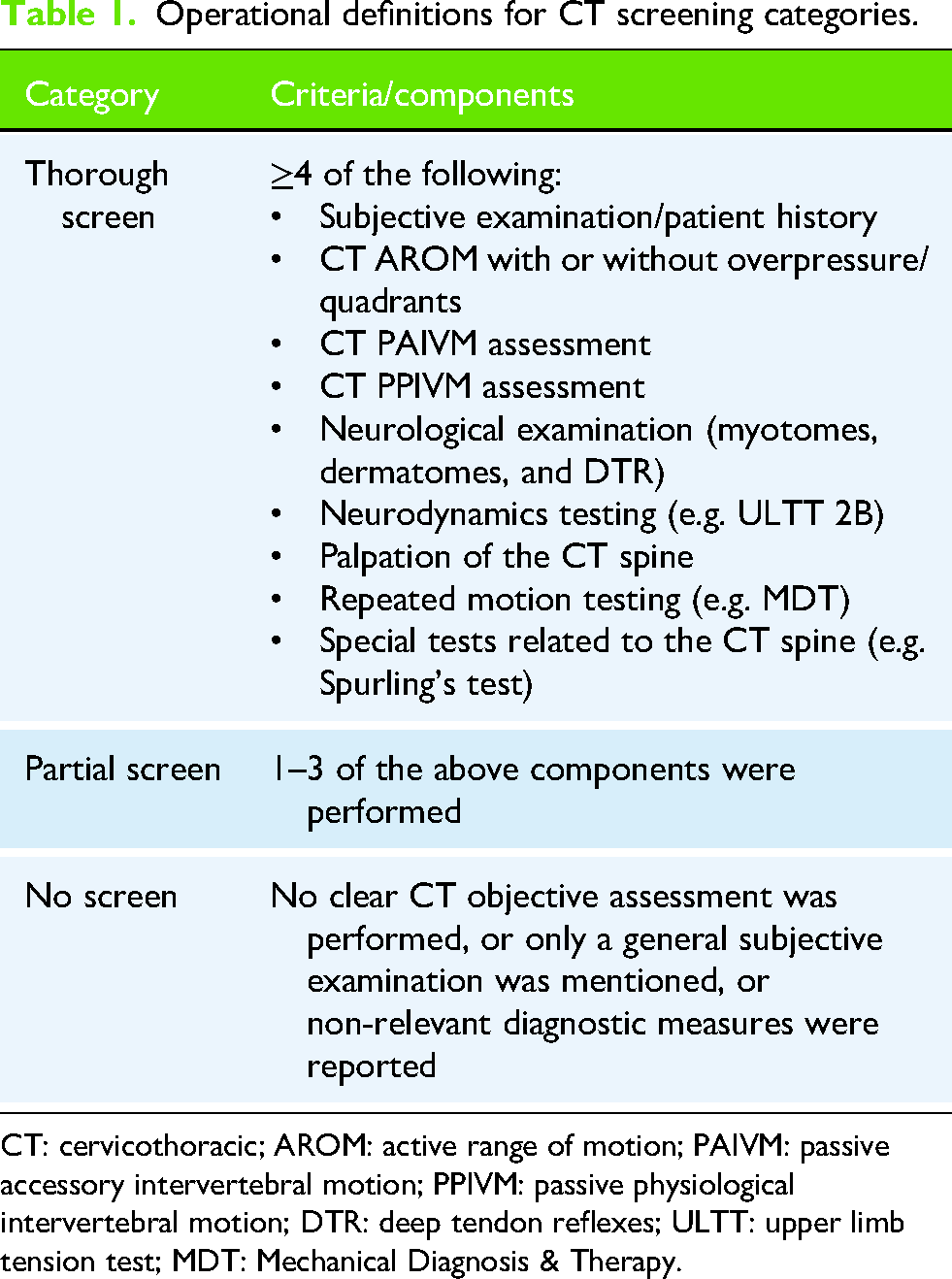
CT: cervicothoracic; AROM: active range of motion; PAIVM: passive accessory intervertebral motion; PPIVM: passive physiological intervertebral motion; DTR: deep tendon reflexes; ULTT: upper limb tension test; MDT: Mechanical Diagnosis & Therapy.
While the subjective examination sets the foundation of clinical reasoning and serves as the primary driver for further screening/testing,25–27 it was not included as a standalone criterion, as reported in the reviewer's original protocol. This decision was made not to diminish the importance of gathering patient history or conducting a subjective examination, but to specifically evaluate the extent to which objective screening procedures are used for suspected CT involvement in LET RCTs. The reliance on patient history alone may be a limitation due to “silent” spinal contributors.13,14 Rosedale et al. 14 demonstrated that forearm extremity symptoms often originate from the spine even without reported neck pain. The absence of a patient reporting no neck pain does not necessarily rule out the possibility of the CT spine contributing to the lateral forearm symptoms, highlighting the necessity for objective, multimodal clustering of physical screening items to ensure diagnostic accuracy. While this review prioritizes objective cervical screening, particularly for studies relying on isolated patient history/subjective examination, these criteria should not be viewed as a clinical universal requirement. Rather, they highlight the importance of objective verification when a patient's self-report lacks sufficient depth to definitively exclude a CT driver of symptoms in LET RCTs. The reviewers support that decision-making within the clinical setting should be guided primarily through an entire evaluation, including a thorough subjective examination, with objective CT screening performed when the patient's history and symptom behavior suggest potential spinal involvement. 18 The intent of this review is not to replace clinical reasoning, but to highlight the limited reporting of objective verification methods in LET RCTs.
In addition to these three CT screening categories, the reviewers also collected the following data to determine what each RCT was performing to come to a LET diagnosis. This included: (1) pain location, (2) palpation of the lateral epicondyle, (3) wrist/forearm range of motion and/or manual muscle testing, (4) special tests of the elbow/forearm (e.g. Cozen's test), (5) grip strength, and (6) any functional non-traditional provocative manuevers/other items (e.g. Chair test).
Risk of bias
Risk of bias for each trial was analyzed by two reviewers (KR and DE) using the Cochrane Collaboration of Risk-of-Bias Tool for Randomized Trials (RoB 2). 28 The RoB 2 tool assesses bias in five domains, including randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. 28 A score of low, high, or some concerns was assigned for each domain, with an overall risk of bias judgment for each trial. 29 A judgment of low risk of bias was assigned if the trial was judged to be at low risk of bias across all five domains. A judgment of some concerns was assigned if at least one domain was judged to raise some concerns, but the trial was not at high risk of bias for any single domain. Finally, a judgment of high risk of bias was assigned if the trial was judged to be at high risk of bias in at least one domain, or if it raised some concerns across multiple domains in a manner that substantially lowered confidence in the result as a matter of expert judgment.
Data synthesis and analysis
To ensure consistency, two independent reviewers (KR and DE) extracted data independently from the initial 10 studies to assess overall agreement before separately extracting data, alphabetized by the first author's last name. The level of agreement for data items extracted for the first 10 studies was above 95%. Data included general study characteristics, RoB 2, categorization of CT screening processes, and categorization of the elbow examination techniques performed. Given the accepted level of agreement, the remaining studies were then divided, and data were extracted independently by the same two reviewers. After the data regarding the screening processes were extracted, results were reported descriptively, including count and percentage data for RoB 2, and each study was calculated based on the number of trials having low, high, or some concerns for risk of bias.
To formally assess inter-rater reliability for title, abstract, and full-text screening, Cohen's kappa (κ) statistics were calculated. Statistical analysis included descriptive statistics, identifying frequency counts and percentages to summarize the characteristics of the included studies and the extracted variables, including screening methods, special testing of the elbow, and risk of bias judgments. All analyses were performed using IBM SPSS Statistics (Version 29.0; Chicago, IL, USA). 30
Results
The combined search of the three databases identified 2744 studies performed on 10 June 2025. A total of 450 duplicates were removed, resulting in 2294 studies for screening of the title and abstract. After title and abstract screening, 1916 studies were excluded, followed by another 170 after full-text review, resulting in a final total of 208 trials (n = 14,186 participants) (Figure 1). There was substantial agreement between reviewers for title and abstract screening (k = 0.65) and almost perfect agreement for full-text review (k = 0.91). 31 The countries with the greatest number of publications included Turkey (n = 50), India (n = 27), the United Kingdom (n = 12), and Spain, Australia, and the United States, each with 10. The first RCT was published in 1985.
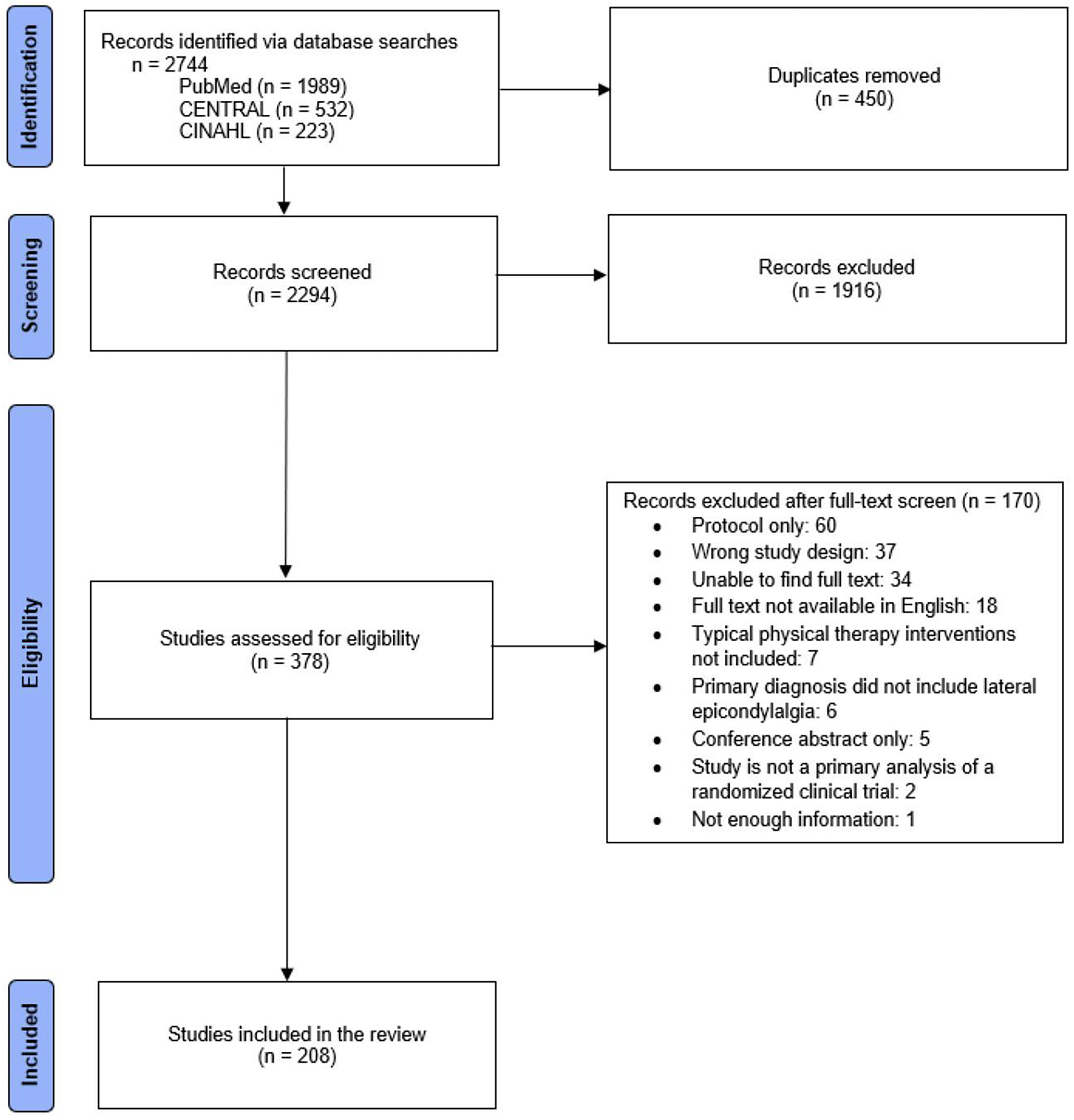
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
CT screening
Based on the predefined screening criteria outlined in the methods section of this review, four (1.9%) studies implemented a CT screening process by performing and reporting on four or more of the CT screening items. For example, Cleland et al. 32 reported on four of the nine possible items defined in the predefined criteria, including a neurodynamic examination, CT range of motion, CT PAIVM assessment, and CT PPIVM assessment. Additionally, using these same criteria, a total of six trials (2.9%) incorporated partial screening (between one and three items, excluding studies that perform a subjective examination only) before a LET diagnosis was made, and the vast majority (n = 198, 95.2%) performed no CT spine screening process or failed to properly report such in their methodology.
Each of the 208 articles reported the process they used to screen the CT spine. Eight (3.8%) reported a neurodynamics examination (e.g. upper limb tension test 2b for the radial nerve), seven (3.4%) reported a neurological examination (e.g. myotome testing), and three (1.4%) reported completing a PAIVM assessment of the CT spine. See Table 2 for more details on each study with a partial or thorough CT screening process and what was reported.
Summary of CT screening procedures across partial and thorough screening RCTs.
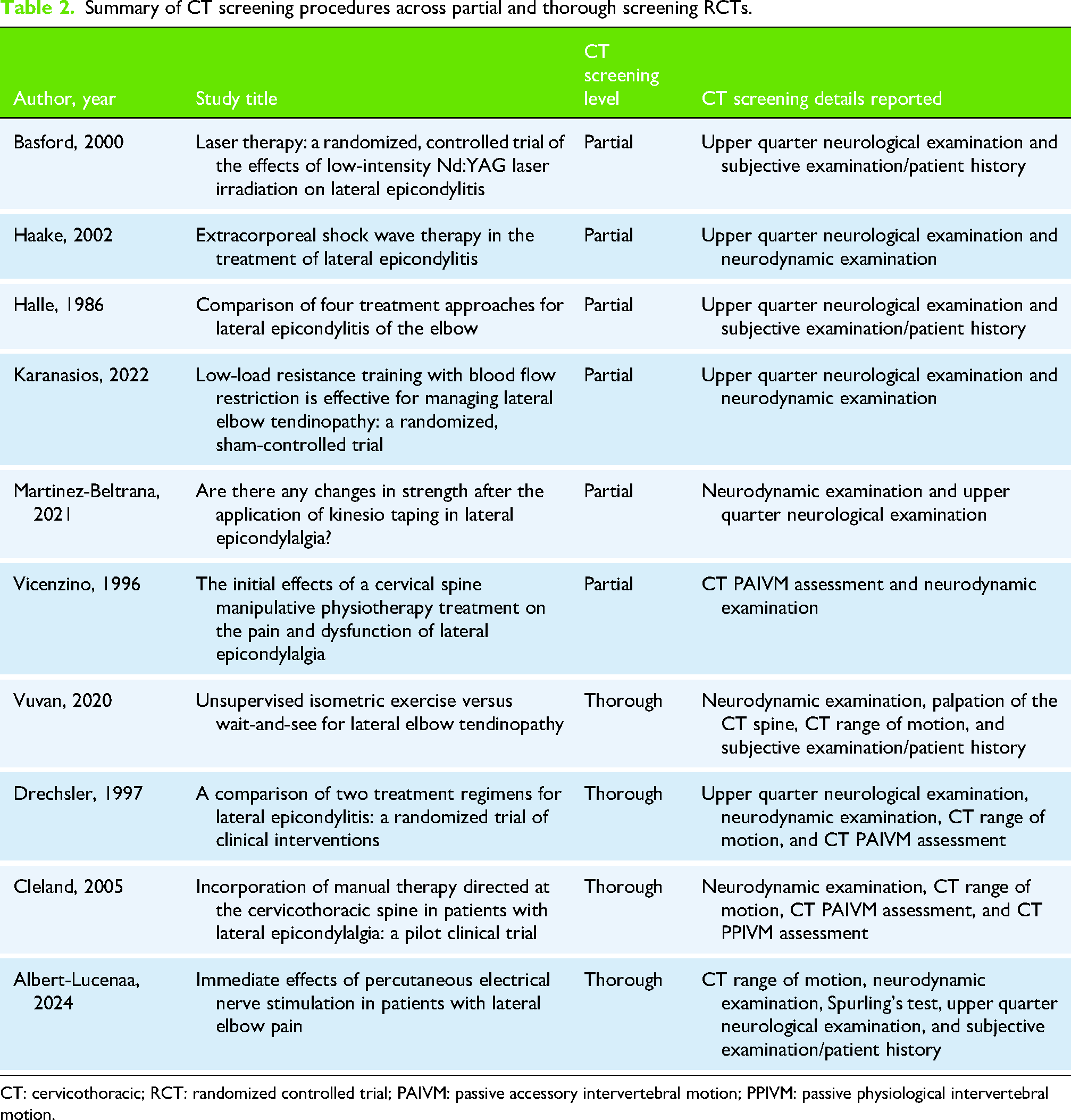
CT: cervicothoracic; RCT: randomized controlled trial; PAIVM: passive accessory intervertebral motion; PPIVM: passive physiological intervertebral motion.
Local elbow examination
This review reported on the elbow examination items specifically used before coming to a diagnosis of LET. A total of 148 (71.2%) reported performing special tests of the forearm/elbow (e.g. Cozen's test), while 128 (61.5%) trials made a diagnosis through palpation of the lateral epicondyle. Seventy-eight trials (37.5%) used pain location in the lateral elbow as a diagnostic criterion. Only 17 trials (8.2%) used hand-held grip strength in their objective assessment, while six (12.9%) looked at wrist/forearm range of motion. Eighty-five trials (40.9%) reported “other” objective examination/functional screening items, which included examples such as a “chair test.”
Risk of bias (RoB 2) quality assessment
The majority of trials had a high risk of bias (Figure 2). A total of 13 (6.3%) trials were judged as having a low risk of bias, 68 (32.7%) having some concerns of bias, and 127 (61.1%) having an overall high risk of bias. The most common reasons were concerns identified with the patient using patient-reported outcomes, the randomization process, and not registering the trial a priori. It is important to consider that a priori trial registration did not become a standard requirement until relatively recently, around 2005, by the International Committee of Medical Journal Editors, 33 resulting in 35 RCTs published beforehand. Consequently, the high prevalence of non-registration in this review may reflect the inclusion of older, dated trials that were conducted before these registration mandates were widely implemented.
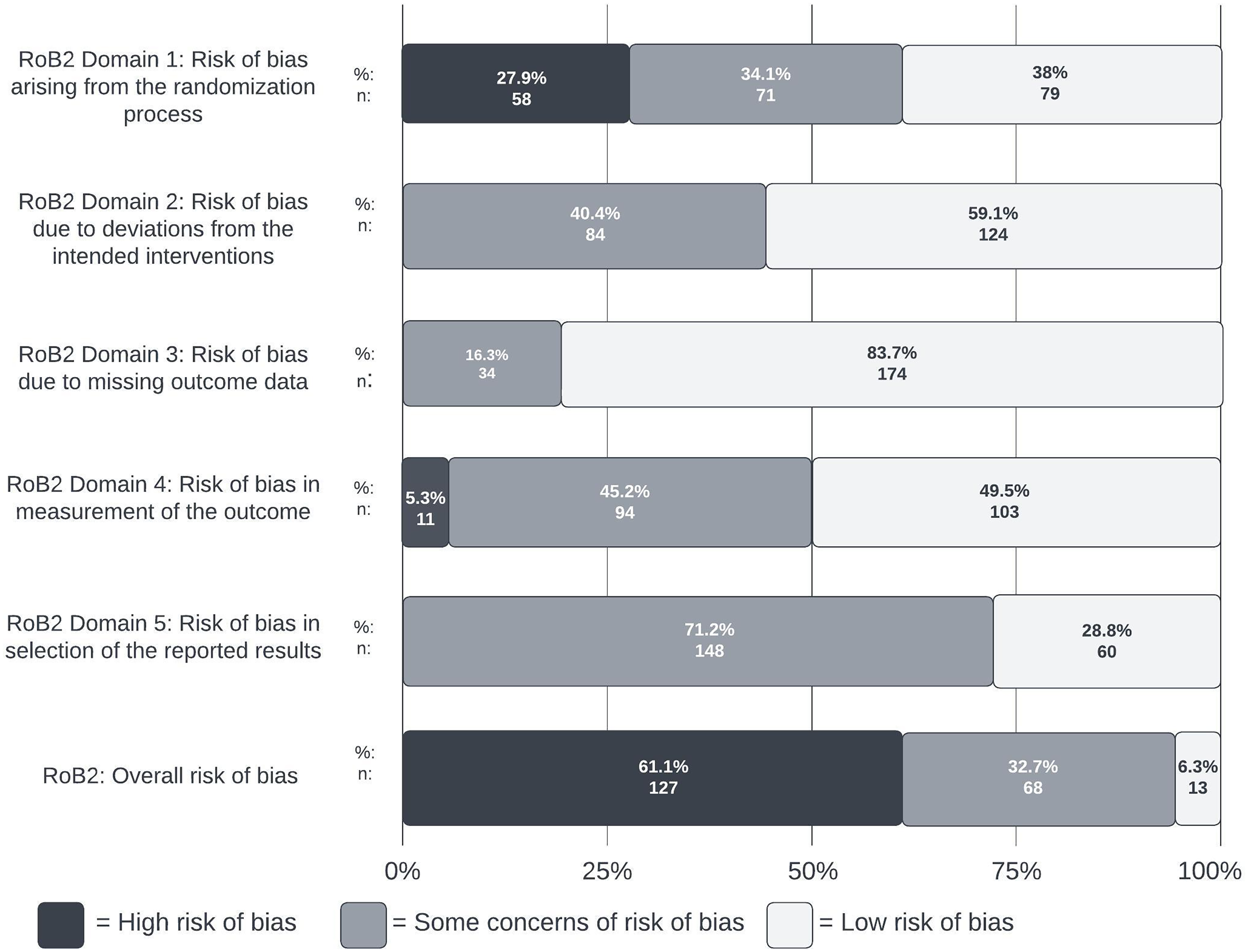
Aggregate risk of bias summary across all studies included in this review.
Discussion
The purpose of this systematic review was to evaluate CT spine screening methods in RCTs focused on conservative management for LET. The findings of this study, based on the predefined criteria established for this review, emphasize the scarcity of screening the CT spine before coming to a diagnosis of LET. Four of the 208 trials conducted a thorough objective CT screening process, 2.9% performed a partial CT screening process, and over 95% either did not perform or adequately report a CT screening process before diagnosing LET in their trial. The nearly universal lack of CT screening in the reviewed trials introduces significant diagnostic uncertainty, as it remains unclear whether these study populations represent “pure” LET or include undetected spinal contributors, or both. While it is established that adding CT interventions can improve LET outcomes, 9 the primary finding of this review is the systemic failure to verify the diagnostic source objectively. The lack of comprehensive screening practices raises concerns regarding the diagnostic homogeneity of participants in these trials. This diagnostic uncertainty may impact the clinical generalizability of the evidence for conservative LET management and highlights the need for future research to implement standardized, multimodal, thoroughly documented screening processes to ensure that participants are accurately categorized at the time of inclusion. It is also important to consider that patients may have more than one diagnosis occurring (e.g. LET with concomitant cervical spine contributions).
A growing body of research reveals that inadequate screening of adjacent regions presents a critical gap in orthopedic diagnostic clinical practice.19,21,34 Walker et al. 19 reported that nearly 75% of trials omitted CT screening before diagnosing SAPS. Likewise, another similar study found that fewer than 5% of trials conducted a thorough thoracolumbar screening as defined by the study's specific criteria (four or more thoracolumbar screening items) before establishing an SIJ pain diagnosis, using many unreliable and unvalidated tests instead. 21 More recently, Cornelis et al. 34 identified that over 13% of patients presenting with knee pain had somatic referred pain originating from hip pathology, an oversight the authors noted is common in routine orthopedic practice. The findings of this study are just as concerning when considering properly diagnosing LET. Specifically, the reviewers found that the majority of studies in this review (95%) did not include or report any form of CT screening before diagnosing LET, based on the predefined criteria established for this review. For example, Abdelmonem et al. 35 made the diagnosis strictly on pain with wrist extension, while Jain et al. 36 and De-la-Cruz-Torres et al. 37 relied solely on the location of pain and varying forearm special tests, such as Maudsley's and Mills’ tests, without clear CT screening processes. Despite their common use, these forearm provocative tests lack consistent diagnostic validity and reliability.3–8 Although not recommended as standalone confirmatory tests for LET, they were the primary methodology used in most reviewed trials.3–8,38 A comprehensive differential diagnosis process is essential when evaluating suspected LET to identify potential differential diagnoses or concomitant contributors, such as cervical somatic referred pain, which accounts for up to 48% of upper extremity cases and as much as 83% when the elbow and forearm present with symptoms. 14 Studies that do not include comprehensive evaluation and examination techniques for all possible sources of pain within the lateral elbow may lead to clinicians omitting crucial information, possibly leading to an inaccurate diagnosis and treatment. It is appropriate to question whether clinicians are accurately diagnosing and choosing appropriate interventions to address true impairments. Given the supporting evidence regarding regional interdependence between these two body regions of the elbow and cervical spine,4,9,12,39,40 and the fact that only four of 208 trials conducted a thorough CT screening (defined in this review as ≥4 physical examination items) before diagnosing LET, this distinction warrants careful examination and clinical reasoning. This rigor is consistent with the APTA CPG by Lucado et al., 8 which advocates for cervical spine screening to differentiate symptoms that may mimic LET and rule out diagnoses such as cervical radiculopathy using specific physical examination findings. While some may question if these criteria are overly stringent, this review maintains that the predefined criteria represent an appropriate screening process for RCTs (≥4 items of a screening process reported), given that spinal-mediated pain can present as LET in up to 83% of cases. 14 Objective verification is essential to ensure participant homogeneity and diagnostic accuracy.
With previous studies incorporating treatment directed to the CT region for LET, it is important to question whether the observed improvements are truly due to regional interdependence, 12 or possibly reflect a specific clinical subgroup (e.g. LET with comorbid cervical pain) that responds more favorably to spinal-directed care, or if they may be inadvertently addressing an unrecognized CT spinal-mediated nociceptive pain mimicking LET symptoms. For example, Cleland et al. 9 completed a retrospective review comparing elbow-only treatment to combined elbow and cervical manual therapy, which found similar long-term success rates, with the group receiving cervical interventions requiring significantly fewer visits. This warrants further consideration of whether improvements attributed to regional interdependence may instead reflect treatment of an unrecognized CT contributor to LET. Another RCT compared cervical versus thoracic manipulation in individuals with LET, finding that cervical manipulation produced significantly greater increases in pressure pain threshold in the elbow, while neither approach changed pain-free grip strength. 39 These findings highlight the potential importance of cervical contributions to symptom modulation in LET, while also raising questions about whether observed clinical improvements stem from regional interdependence or untreated CT involvement, particularly without screening for cervical spine involvement beforehand. 39 Additionally, a recent international survey by Heales et al. 22 further highlights this gap, reporting that cervical spine special tests are not routinely used by physiotherapists during the assessment of LET. This lack of routine cervical assessment in clinical practice, combined with the poor screening reported in clinical trials, suggests that clinicians may not be accurately identifying referred cervical somatic pain, leading to the selection of interventions that do not address the primary driver of the patient's impairment. 22
To address these systemic diagnostic gaps, future research should not only prioritize a standardized CT screening process but also establish formal reporting RCT guidelines for proper inclusion and exclusion criteria, rather than leaving vague definitions that the reviewers commonly encountered. Many studies reported exclusion based on “cervical radiculopathy” or excluded based on “neck pain,” but did not report in depth as to whether there were any items the researchers were doing to effectively rule it out beyond a patient history/subjective examination. Such proposed guidelines may help to ensure that RCTs explicitly document their screening criteria, making it clear to readers whether the reported evidence applies to a “pure LET population,” a specific clinical subgroup of LET with comorbid spinal contributors, or true CT spinal referred pain mimicking LET, as well as improving transparency for clinical utility amongst clinicians. Standardizing these reporting practices would be a necessary step toward improving the transparency and clinical utility of LET research.
Limitations
Several limitations should be considered when interpreting these results. First, this review included no formal universal CT spinal screening process identified when examining forearm symptoms for LET. Although it is reasonable to expect RCTs to screen adjacent regions, the absence of consensus-based screening items meant that the criteria used in this study, while based on existing literature, 18 had to be established by the reviewers. This lack of a universal standard may lead to variability in how “appropriate screening” is defined across different RCTs; however, this limitation further highlights the study's finding that a standardized, validated screening protocol is needed to ensure diagnostic homogeneity in upper and lower extremity research and clinical practice.18,19,21 Similar to the work by Walker et al. 19 and the subsequent Delphi study by Requejo-Salinas et al., 18 which aimed to more clearly delineate shoulder from cervical spine pathology, we propose a similar approach for the elbow. Establishing such a standard would not replace clinical reasoning but would instead provide researchers and clinicians with a validated framework to ensure the primary pain driver is identified, ensuring the inclusion of more homogeneous participant populations in future trials. Second, only RCTs published in the English language were used, excluding 18 additional studies. Third, this review exclusively investigated RCTs involving conservative management for LET. Consequently, studies investigating surgical interventions were not included in the search process, as they may have very similar examination processes before surgical interventions. Fourth, this review included seven non-physical therapy studies (e.g. injections or “wait-and-see”). This broader scope demonstrates that the lack of CT screening is a systemic research issue, not limited to one discipline. Additionally, one study was excluded because its full text lacked sufficient diagnostic and intervention details for accurate data extraction. Fifth, 34 full-text articles were unable to be retrieved during the search process (e.g. interlibrary loan), which is a limitation, as these studies may have contained relevant data on CT screening that could have influenced our overall findings. Sixth, the criteria used to categorize screening levels may be viewed as a limitation. This review intentionally excluded subjective history/patient interviews from the total count for screening categories if it was performed in isolation. While the reviewers acknowledge that the subjective interview is a cornerstone of clinical reasoning, the decision to prioritize objective physical examination items likely resulted in lower reported screening rates. However, this was deemed necessary because research demonstrates that isolated subjective reports of “no neck pain” (e.g. simple absence of local cervical symptoms or history of neck pain) frequently fail to rule out a cervical source of extremity symptoms. 14 This distinction matters because simply asking whether neck pain is present does not provide the depth of a thorough subjective history, which may capture pain behavior, aggravating factors, and related symptoms, and lead to proper screening items. The findings of this review potentially reflect the prevalence of objective diagnostic verification when clinical suspicion of CT involvement exists rather than overall clinical suspicion. Finally, this study excluded non-RCT designs and may overlook diagnostic reporting outside of these study designs.
Conclusion
This review identifies a gap in the diagnostic methodology of LET research, characterized by a near-universal lack of performing and/or reporting on any CT screening items. Given the high prevalence of spinal contributors to LET, this diagnostic oversight may prevent clinicians from distinguishing between true LET, LET with comorbid CT spinal-referred pain, or isolated undiagnosed CT spinal-mediated pain mimicking LET. Future research should consider adopting standardized screening protocols and formal reporting of RCT inclusion/exclusion criteria guidelines to ensure diagnostic homogeneity of LET as a diagnosis and provide clearer evidence for targeted interventions. Prioritizing these practices is essential to move toward more precise and effective management for all clinical phenotypes of lateral elbow pain.
Supplemental Material
sj-docx-1-sel-10.1177_17585732261467932 - Supplemental material for Inadequate cervicothoracic assessment is nearly universal for screening participants with lateral elbow tendinopathy: A systematic review of 208 randomized controlled trials
Supplemental material, sj-docx-1-sel-10.1177_17585732261467932 for Inadequate cervicothoracic assessment is nearly universal for screening participants with lateral elbow tendinopathy: A systematic review of 208 randomized controlled trials by Matthew R. Schumacher, Emma K. Bakken, Kaitlyn P. Reynolds, Dylan R. Elletson and Jody L. Eckert in Shoulder & Elbow
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.