
Abstract
Background:
Long-course induction chemoimmunotherapy (⩾3 cycles) is increasingly used to downstage unresectable non-small-cell lung cancer (NSCLC). However, the optimal definitive local treatment for patients who remain inoperable after induction—definitive radiotherapy (RT) alone versus concurrent chemoradiotherapy (CRT)—remains unclear.
Objectives:
To compare survival and toxicity outcomes between definitive RT and CRT following induction chemoimmunotherapy in unresectable NSCLC.
Design:
This was a single-center retrospective cohort study using stable inverse probability of treatment weighting (sIPTW) to balance baseline characteristics between treatment groups.
Methods:
Consecutive patients with unresectable NSCLC without known actionable driver mutations who remained inoperable after long-course induction chemoimmunotherapy and subsequently received definitive RT or CRT were included. Progression-free survival (PFS) and overall survival (OS) were estimated using Kaplan–Meier methods and compared with weighted Cox proportional hazards models. Treatment-related adverse events were graded according to the Common Terminology Criteria for Adverse Events. An exploratory analysis evaluated the association between consolidation immunotherapy and PFS.
Results:
A total of 153 patients were included (RT, n = 63; CRT, n = 90). At a median follow-up of 25.8 months, the 1- and 2-year PFS rates were 83.5% and 54.3% in the RT group, compared with 82.1% and 61.1% in the CRT group (hazard ratio (HR) = 0.83; 95% confidence interval (CI), 0.51–1.37; p = 0.46). After sIPTW adjustment, PFS remained comparable (HR = 0.80; 95% CI, 0.47–1.35; p = 0.46). OS was also similar between groups. Grade 3–4 hematologic toxicity was more frequent with CRT (24.4% vs 9.5%; p < 0.001). Consolidation immunotherapy was associated with a numerical but non-significant PFS improvement (HR = 0.78; 95% CI, 0.48–1.27; p = 0.32).
Conclusion:
In patients with unresectable NSCLC who remain inoperable after long-course induction chemoimmunotherapy, definitive RT alone provides survival outcomes comparable to CRT while reducing severe hematologic toxicity. RT alone may represent a reasonable definitive option for carefully selected patients in this setting.
Plain language summary
Some patients with non-small-cell lung cancer (NSCLC) cannot undergo surgery even after receiving long-course chemotherapy combined with immunotherapy. For these patients, doctors must choose between radiotherapy alone or adding more chemotherapy at the same time as radiotherapy. In this retrospective study of 153 patients with NSCLC, radiotherapy alone worked just as well as chemoradiotherapy in controlling the cancer and achieving similar survival outcomes. However, adding chemotherapy caused many more severe blood-related side effects, which can lead to infections and delays in treatment. A small number of patients received additional immunotherapy after radiotherapy. This showed a possible benefit, but the improvement was not strong enough to be considered significant. Overall, our findings suggest that for patients who remain unable to undergo surgery after induction chemoimmunotherapy, radiotherapy alone can be an effective and safer treatment option.
Keywords
Background
Stage III non-small-cell lung cancer (NSCLC) represents a biologically and clinically heterogeneous disease. The PACIFIC trial established definitive concurrent chemoradiotherapy (CRT) followed by consolidation immunotherapy as the standard of care for patients with locally advanced, unresectable disease. 1 For resectable NSCLC, perioperative chemoimmunotherapy—demonstrated in the CheckMate 816 trial and supported by other prospective randomized phase III studies—has improved event-free survival and pathological complete response (pCR) compared with chemotherapy alone.2–7 However, approximately 15%–25% of patients fail to achieve surgical eligibility after induction therapy, and the optimal management for this subset remains unclear.
For patients with initially unresectable stage III NSCLC, recent studies have demonstrated that induction chemoimmunotherapy can successfully downstage a proportion to resectable disease. Data from the 2025 World Conference on Lung Cancer and European Society for Medical Oncology Congress reported encouraging preliminary results from the ongoing PANDA-1, MDT-BRIDGE, and LungMate-013 trials, showing conversion-to-surgery rates of approximately 70%–80%, with pCR rates of around 50%–55%.8–10 A multicenter Chinese study further confirmed a 69.9% conversion rate following long-course (⩾3 cycles) induction immunochemotherapy. 11 Despite these advances, a considerable proportion of patients remain inoperable after long-course induction therapy, and how best to manage these individuals with curative intent remains unresolved.
Therefore, this study aimed to compare survival outcomes and safety between concurrent CRT and radiotherapy (RT) alone, with or without consolidation immunotherapy, in patients with unresectable stage III NSCLC following long-course induction chemoimmunotherapy.
Methods
Study design and patient selection
This was a single-center retrospective cohort study conducted at Beijing Cancer Hospital between January 1, 2021, and December 31, 2024. Clinical data were collected from patients with unresectable stage III NSCLC who had received long-course induction chemoimmunotherapy followed by definitive local treatment. Eligible patients met all of the following criteria: (1) histologically confirmed NSCLC; (2) received at least three cycles of induction chemoimmunotherapy; (3) classified as stage III; and (4) underwent either CRT or RT alone, with or without consolidation immunotherapy. Patients were excluded if they had (1) combined small-cell, neuroendocrine, or sarcomatoid histology; (2) a history of another malignancy within the past 5 years; (3) sensitizing EGFR mutations (L858R or exon 19 deletion); or (4) received only palliative care without definitive RT.
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, and the completed checklist is provided as the Supplemental STROBE checklist.
Treatment and follow-up
All patients received induction chemoimmunotherapy consisting of platinum-based doublet chemotherapy combined with a programmed cell death protein 1 (PD-1) or programmed death ligand 1 (PD-L1) inhibitor. The number of induction cycles varied according to the patient’s clinical response and tolerance. Some patients who did not achieve sufficient tumor regression after initial induction therapy received additional cycles with the intention of achieving surgical eligibility; however, those who remained unresectable proceeded to definitive RT or CRT according to multidisciplinary treatment decisions.
RT was delivered using intensity-modulated or volumetric modulated arc therapy with a total dose of 50.4–60 Gy in 28–30 fractions, with a simultaneous integrated boost to 60–66 Gy. Twelve patients in the RT group received hypofractionated RT consisting of 15–20 fractions with a total dose of 54–60 Gy. In the CRT group, most patients received platinum-based doublet chemotherapy concurrently with RT, and nine patients additionally received concurrent immunotherapy.
Patients were re-evaluated 1 month after completion of RT. Consolidation immunotherapy was commonly considered after definitive RT, particularly in patients who achieved a favorable response to induction treatment, maintained adequate performance status, and experienced manageable toxicities. PD-L1 expression was not a primary determinant of treatment allocation, and consolidation therapy was individualized according to overall clinical condition and patient preference. Follow-up was conducted every 2–3 months during the first 2 years and every 6 months thereafter. Each visit included a physical examination, chest and upper abdomen computed tomography, and laboratory evaluations such as complete blood count, serum biochemistry, and tumor markers. Positron emission tomography–computed tomography was not performed routinely but was reserved for patients with suspected disease recurrence or metastasis.
Endpoints
The primary endpoint was progression-free survival (PFS), defined as the time from the start of induction therapy to radiographic disease progression or death from any cause, whichever occurred first. The secondary endpoints included overall survival (OS), defined as the time from the start of induction therapy to death from any cause, and treatment-related toxicity, graded according to the Common Terminology Criteria for Adverse Events version 5.0.
Statistical analysis
Survival curves for PFS and OS were estimated using the Kaplan–Meier method, and differences between groups were assessed using the log-rank test. PD-L1 expression status, when unavailable, was treated as a separate “unknown” category in all models. To reduce potential selection bias between the RT and CRT groups, stable inverse probability of treatment weighting (sIPTW) was applied. The propensity score was estimated using a logistic regression model including baseline covariates that were clinically relevant and potentially associated with treatment allocation, specifically age, clinical stage, and number of induction cycles. Stabilized weights were calculated using the marginal probability of treatment assignment as the numerator and the individual propensity score as the denominator. The distribution of stabilized weights was examined to assess the presence of extreme values, and weight diagnostics are provided in the Supplemental Material (Figure S1).
Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox proportional hazards models in univariable and multivariable analyses to identify independent prognostic factors. The proportional hazards assumption was assessed using Schoenfeld residual-based tests. In addition to the primary stabilized IPTW analysis, a doubly robust Cox regression model was performed for PFS by incorporating baseline covariates within the weighted framework.
To assess the robustness of the primary findings, several pre-specified sensitivity analyses were conducted. First, given that treatment allocation occurred after completion of induction therapy, an additional analysis redefined the time origin at the start of definitive RT/CRT (allocation-time PFS-RT and OS-RT), and treatment effects were re-estimated using the same sIPTW-weighted Cox framework. Second, stabilized inverse probability weights were trimmed at the 1st and 99th percentiles to evaluate the influence of extreme weights. Third, patients who received concurrent immunotherapy during RT/CRT were excluded to address potential treatment heterogeneity. Finally, patients treated with hypofractionated RT were excluded to determine whether this small subgroup influenced overall treatment effect estimates.
A forest plot was generated to display results from subgroup analyses, evaluating the consistency of treatment effects across clinical subgroups. Additionally, exploratory analyses were performed to assess the association between consolidation immunotherapy and PFS. A landmark analysis at 6 weeks after completion of RT was performed to account for potential immortal time bias. All statistical analyses were conducted using R software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria), and a two-sided p < 0.05 was considered statistically significant.
Results
Baseline characteristics
As shown in Table 1, the cohort included 153 patients with a median age of 63 years (interquartile range, 58–69). Most were male (89.5%) with an Eastern Cooperative Oncology Group performance status of 0 (76.5%). Squamous cell carcinoma was predominant (72.5%), and stage IIIB disease was most common (47.7%). About 40% of patients had PD-L1 expression ⩾1%, whereas nearly half (47.1%) had unknown PD-L1 status. Most patients (89.5%) received PD-1 inhibitors during induction therapy. The median number of induction cycles was 4, and 68.0% achieved a partial response. After local therapy, 58.8% received immunotherapy consolidation.
Baseline characteristics of patients before stable inverse probability of treatment weighting.

CRT, concurrent chemoradiotherapy; ECOG, Eastern Cooperative Oncology Group performance status; IQR, interquartile range; NSCLC, non-small-cell lung cancer; PD-1, programmed cell death protein 1; PD-L1, programmed death ligand 1; RT, radiotherapy alone; WHO, World Health Organization.
Compared with the RT cohort, the CRT group comprised younger patients (p = 0.006), had earlier-stage disease (p = 0.034), and received fewer induction chemoimmunotherapy cycles (p < 0.001). After applying sIPTW (Table S1), all baseline variables achieved good balance between the two groups (all p > 0.05), indicating successful weighting adjustment.
Survival analysis
At a median follow-up of 25.8 months (95% CI, 23.0–38.1), a total of 65 progression events (42.5%) and 38 deaths (24.8%) were observed. In the unweighted cohort, the 1-, 2-, and 3-year PFS rates were 83.5%, 54.3%, and 45.6% in the RT group, and 82.1%, 61.1%, and 53.6% in the CRT group, respectively. There was no significant difference in PFS between the two groups (HR = 0.83, 95% CI, 0.51–1.37, p = 0.46). After applying sIPTW, PFS remained comparable (HR = 0.80, 95% CI, 0.47–1.35, p = 0.46), with 1-, 2-, and 3-year rates of 79.2%, 58.1%, and 52.3% in the RT group and 80.3%, 59.2%, and 50.5% in the CRT group, respectively (Figure 1(a) and (b)).
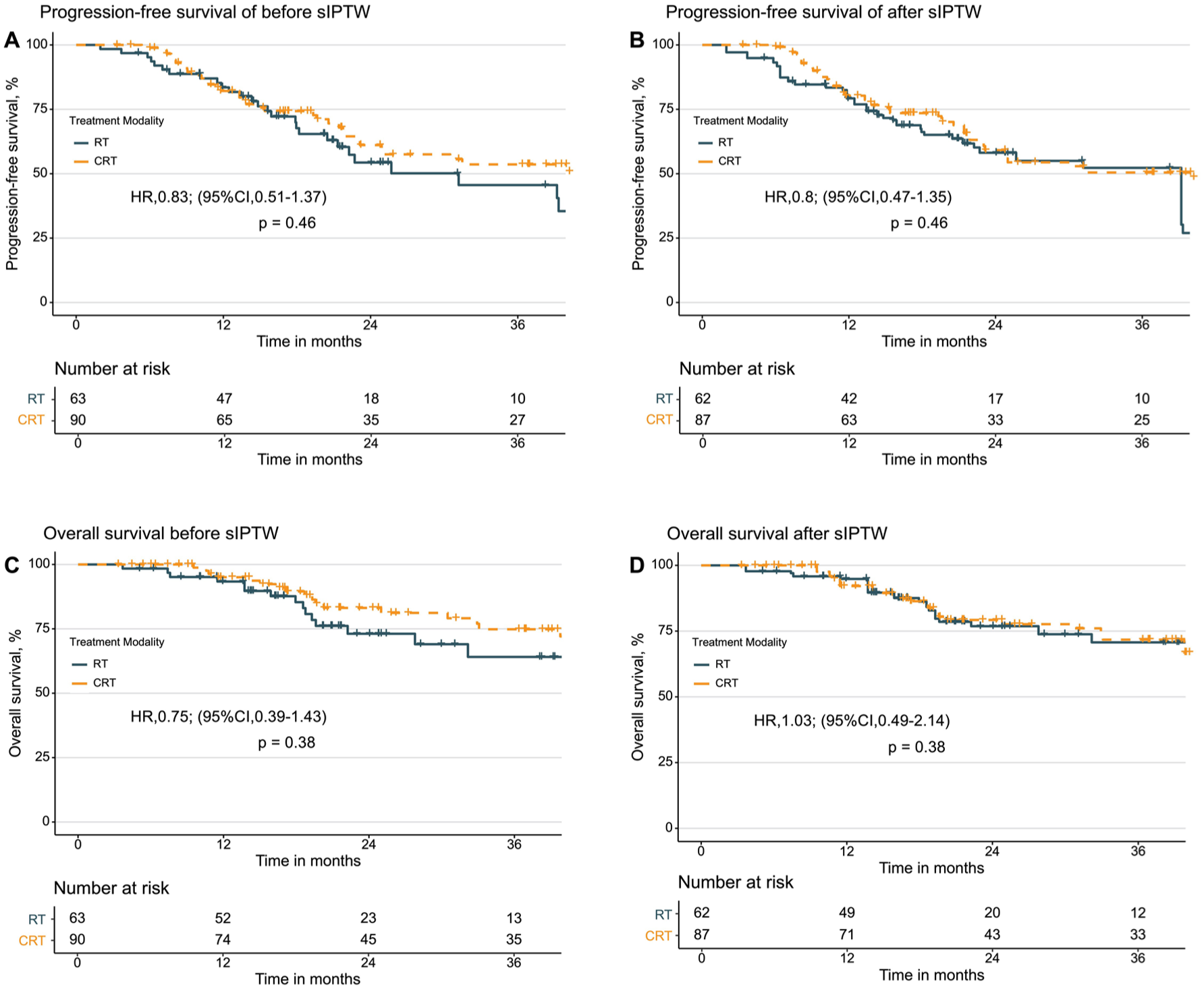
Kaplan–Meier curves of PFS and OS with and without concurrent chemotherapy after induction chemoimmunotherapy. (a, b) PFS before and after sIPTW adjustment. (c, d) OS before and after sIPTW adjustment. HRs and 95% CIs were estimated using Cox proportional hazards models.
The 1-, 2-, and 3-year OS rates were 93.4%, 73.1%, and 64.1% in the RT group, and 95.0%, 83.1%, and 74.8% in the CRT group, respectively (HR = 0.75, 95% CI, 0.39–1.43, p = 0.38). After sIPTW adjustment, OS remained similar (HR = 1.03, 95% CI, 0.49–2.14, p = 0.38), with corresponding 1-, 2-, and 3-year rates of 94.8%, 76.9%, and 70.7% in the RT group and 92.1%, 79.2%, and 71.7% in the CRT group, respectively (Figure 1(c) and (d)).
Sensitivity analyses
Redefining the time origin at the start of definitive RT/CRT yielded results consistent with the primary induction-based analysis. In the allocation-time analysis, the sIPTW-weighted Cox model demonstrated comparable outcomes for both PFS (HR = 0.82, 95% CI, 0.48–1.39; p = 0.454; Figure S3) and OS (HR = 1.05, 95% CI, 0.50–2.19; p = 0.896), indicating that guarantee-time bias did not materially influence the findings.
Trimming stabilized inverse probability weights at the 1st and 99th percentiles resulted in HR estimates comparable to the main weighted analysis (PFS: HR = 0.81, 95% CI, 0.48–1.36, p = 0.43; OS: HR = 1.0, 95% CI, 0.48–2.06, p = 0.99), suggesting that extreme weights did not drive the observed associations. In addition, excluding patients who received concurrent immunotherapy (n = 9) did not materially alter the treatment effect estimates (PFS: HR = 0.72, 95% CI, 0.42–1.25, p = 0.25; OS: HR = 0.80, 95% CI, 0.37–1.72, p = 0.57). Similarly, excluding patients treated with hypofractionated RT yielded consistent results (PFS: HR = 0.80, 95% CI, 0.46–1.41, p = 0.45; OS: HR = 0.91, 95% CI, 0.42–1.96, p = 0.80).
Cox regression analysis
Cox proportional hazards regression identified disease stage as an independent prognostic factor for PFS (Table S2). Schoenfeld residual-based tests did not indicate violation of the proportional hazards assumption for either endpoint (Figure S2). In addition to the primary stabilized IPTW analysis, a doubly robust weighted Cox model incorporating baseline covariate adjustment further confirmed that concurrent chemoradiotherapy was not independently associated with PFS (HR = 0.86, 95% CI, 0.47–1.57, p = 0.63). The corresponding adjusted survival curves are shown in Figure S4.
Subgroup analysis
A subgroup analysis was conducted to assess the consistency of treatment effects between the CRT and RT groups (Figure 2). The results were consistent across all examined subgroups, with no significant interactions observed (all p for interaction >0.05). These findings indicate that no specific subgroup derived a distinct PFS benefit from CRT compared with RT.

Subgroup analysis of PFS comparing CRT versus RT after long-course induction chemoimmunotherapy.
Exploratory analysis of consolidation immunotherapy
An exploratory analysis evaluated the impact of consolidation immunotherapy after local treatment (Figure 3). The 1-year PFS rates were 87.3% in the consolidation immunotherapy group and 75.9% in the observation group, respectively. Patients receiving consolidation immunotherapy showed a numerically longer PFS, although the difference was not statistically significant (HR = 0.78, 95% CI, 0.48–1.27, p = 0.32).
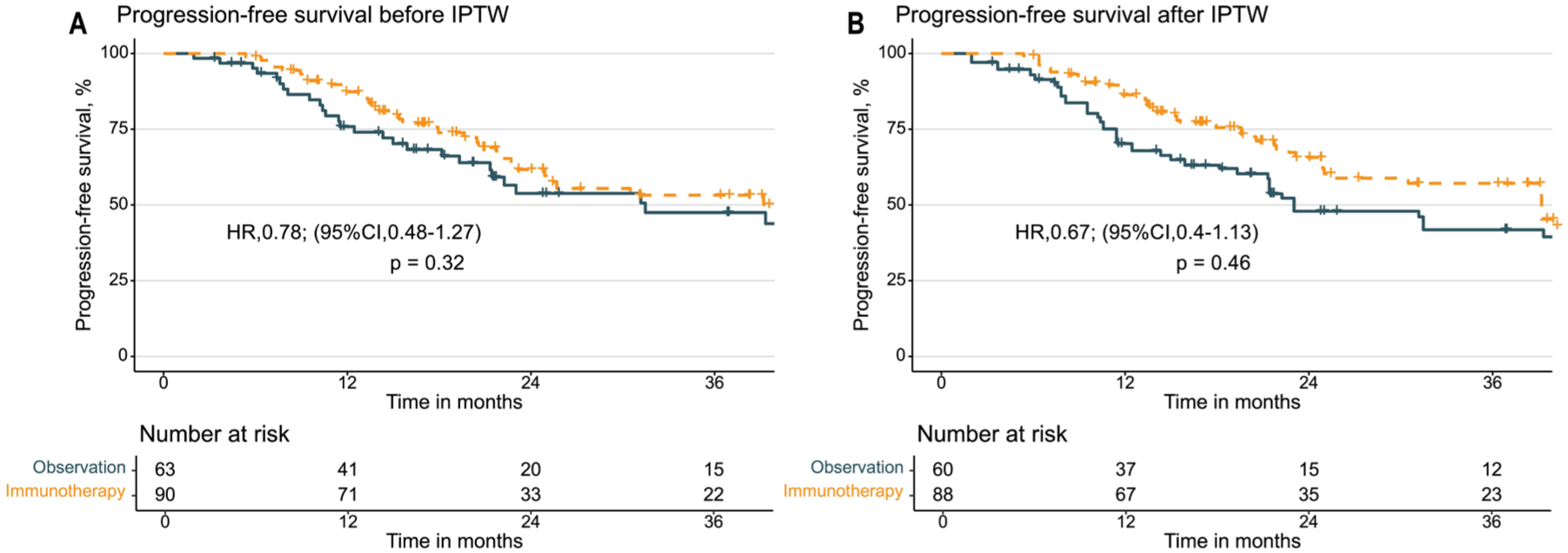
Kaplan–Meier curves of PFS with or without consolidation immunotherapy. (a) PFS before sIPTW adjustment. (b) PFS after sIPTW adjustment. HRs and 95% CIs were estimated using Cox proportional hazards models.
After applying sIPTW, this trend persisted (HR = 0.67, 95% CI, 0.40–1.13, p = 0.46), with 1-year PFS rates of 86.3% and 70.2%, respectively. Although not statistically significant, consolidation immunotherapy showed a consistent trend toward improved PFS in the matched cohort. Besides, landmark analysis at 6 weeks after RT/CRT yielded consistent findings (HR = 0.80, 95% CI, 0.48–1.32, p = 0.38).
Treatment-related toxicities
Treatment-related toxicities are summarized in Table 2. Both regimens were generally well tolerated, with most adverse events being grade 1–2. Compared with the RT group, patients in the CRT group experienced significantly higher rates of hematologic toxicity (p < 0.001), particularly grade 3–4 hematologic events, which occurred in 24.4% of CRT patients versus 9.5% of RT patients (p < 0.001). The incidence of severe leukopenia, neutropenia, and thrombocytopenia was also higher in the CRT group (p < 0.05 for all), whereas anemia rates were similar (p = 0.980). Esophagitis did not differ significantly between groups (p = 0.597).
Comparison of treatment-related toxicities between RT and CRT groups.

Toxicities were graded according to CTCAE version 4.0. p Values were calculated using the χ2 or Fisher’s exact test as appropriate.
CRT, concurrent chemoradiotherapy; CTCAE, Common Terminology Criteria for Adverse Events; RT, radiotherapy alone.
During RT, treatment interruption or death occurred in 5.2% of all patients, with 7.9% in the RT group and 3.3% in the CRT group (p = 0.208). Severe radiation pneumonitis occurred in 13.7% of the overall cohort, including 19.0% in the RT group and 10.0% in the CRT group (p = 0.109).
Discussion
An optimal local treatment strategy after long-course induction chemoimmunotherapy remains uncertain for patients with unresectable stage III NSCLC. In this study, we compared CRT and RT in this setting and found that adding concurrent chemotherapy did not improve PFS or OS. These findings remained consistent after sIPTW adjustment and across all clinical subgroups. However, CRT was associated with a higher incidence of severe hematologic toxicity. Therefore, RT alone may represent a more favorable option in selected patients, although this hypothesis requires confirmation in larger or prospective studies.
Historically, RTOG 9410 established concurrent CRT as the standard treatment for locally advanced NSCLC. 12 In our study, adding concurrent chemotherapy after long-course induction chemoimmunotherapy did not improve PFS, and no subgroup derived benefit. The 1-year PFS (~80%) was comparable to that reported in the PACIFIC trial 1 and consistent with the 87% observed by Liu et al. 13 for patients receiving induction chemoimmunotherapy followed by RT alone. As expected, severe hematologic toxicity was more frequent with CRT. In contrast, Guan et al. 14 analyzed patients who received CRT or RT after a median of four induction cycles and found that the 1-year PFS increased from 71% with RT to 93% with CRT, although OS remained similar. Therefore, whether concurrent chemotherapy confers additional benefit after long-course induction chemoimmunotherapy requires validation in prospective studies. Accordingly, these findings support treatment selection should be individualized, balancing hematologic toxicity risk against post-induction performance status, bone marrow reserve, and overall treatment tolerance.
Consolidation immunotherapy after definitive CRT has become the standard of care for unresectable stage III NSCLC. The prospective CA209-7AL study led by Liu et al. 15 further evaluated post-CRT nivolumab consolidation following induction nivolumab plus chemotherapy. Consolidation therapy significantly prolonged PFS compared with observation (HR = 0.49; 95% CI, 0.30–0.81; p = 0.003). Subgroup analysis revealed that patients achieving a partial response during induction derived the greatest benefit, whereas those with stable disease showed no significant improvement, suggesting that the initial response to induction chemoimmunotherapy may serve as an early indicator of consolidation efficacy. In our cohort, PFS showed a numerical but not statistically significant improvement with consolidation immunotherapy. Landmark and sensitivity analyses yielded results consistent with the primary findings. This modest effect may reflect the biological characteristics of our population—patients remaining unresectable after ⩾4 cycles of induction chemoimmunotherapy—who are likely less responsive to immune-based treatment. Nevertheless, consolidation immunotherapy remains a reasonable option in appropriately selected patients and should be considered within individualized clinical decision-making. Molecular residual disease (MRD) has emerged as a promising biomarker for post-treatment risk stratification. Recent studies have shown that MRD dynamics can predict recurrence and immunotherapy benefit earlier than radiologic assessment. 16 Patients achieving MRD clearance after definitive therapy demonstrate significantly improved survival, suggesting its potential role in guiding consolidation decisions.
Future research should focus on optimizing systemic induction and local treatment strategies for patients with unresectable or borderline resectable stage III NSCLC. For potentially resectable disease, the Society of Thoracic Surgeons consensus recommends that surgical resectability be determined upfront, and patients deemed unresectable should not routinely receive neoadjuvant therapy solely to achieve conversion. 17 Nevertheless, several ongoing trials are investigating conversion strategies for initially unresectable stage III NSCLC, reporting conversion-to-surgery rates of approximately 70%–80%.8,9 Notably, in LungMate-013, 50 converted patients were randomized to surgery or definitive RT, demonstrating a significant improvement in event-free survival (HR = 0.38, 95% CI, 0.14–1.01) but no difference in OS. 10 In our view, for patients with potentially resectable disease, reassessing surgical eligibility after two cycles of induction chemoimmunotherapy may represent an optimal window. Those who remain unresectable at that point could proceed directly to definitive concurrent CRT, when both performance status and bone-marrow reserve are generally preserved. For patients remaining unresectable after prolonged induction, definitive hypofractionated RT offers a promising approach. Moderate hypofractionation may enhance immunogenic tumor cell death and better preserve circulating lymphocytes due to fewer treatment fractions.18–21 In the CA209-7AL trial, hypofractionated RT followed by consolidation immunotherapy achieved favorable efficacy and acceptable toxicity, with exploratory analyses suggesting improved disease control compared with standard fractionation. 15 Similarly, 12 patients in our study received hypo-RT with good tolerance and local control.
This study has several limitations. First, its retrospective and single-center design may have introduced inherent selection bias despite the use of sIPTW adjustment. In routine practice, treatment selection between RT and CRT after induction therapy is influenced by post-induction performance status and hematologic reserve, factors that may not be fully captured in retrospective data. Although robust statistical approaches, including sIPTW and multiple sensitivity analyses, were applied, residual confounding due to unmeasured variables cannot be entirely excluded. Second, the sample size was relatively small, limiting the statistical power for subgroup and exploratory analyses. The width of the CIs indicates that while large treatment effects are unlikely, moderate differences cannot be definitively ruled out. Third, treatment regimens were heterogeneous, particularly regarding induction cycles, concurrent chemotherapy protocols, and the use of consolidation immunotherapy. In addition, the follow-up duration was insufficient to fully assess long-term survival outcomes. Therefore, these findings should be interpreted cautiously and warrant validation in larger, prospective multicenter studies.
Conclusion
In patients with stage III NSCLC who remain unresectable after long-course induction chemoimmunotherapy, adding concurrent chemotherapy during definitive RT did not improve survival outcomes, while increasing hematologic toxicity. Definitive RT alone may therefore represent a reasonable and less toxic option for selected patients. Consolidation immunotherapy showed only a modest, non-significant benefit in this setting. Future prospective studies incorporating biomarkers such as MRD are warranted to refine patient selection and optimize local–systemic treatment strategies.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261447969 – Supplemental material for Definitive radiotherapy provides comparable survival with lower toxicity compared with concurrent chemoradiotherapy after long-course induction chemoimmunotherapy in unresectable non-small-cell lung cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359261447969 for Definitive radiotherapy provides comparable survival with lower toxicity compared with concurrent chemoradiotherapy after long-course induction chemoimmunotherapy in unresectable non-small-cell lung cancer by Xiao Chang, Huifang Liang, Jiayi Xiao, Dan Yang, Jiayi Yu, Jiahui Shan, Xin Dong, Wei Deng, Yuting Zhao, Leilei Jiang, Liuhua Long, Yue Teng, Huiming Yu, Rong Yu, Shaohua Ma and Anhui Shi in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261447969 – Supplemental material for Definitive radiotherapy provides comparable survival with lower toxicity compared with concurrent chemoradiotherapy after long-course induction chemoimmunotherapy in unresectable non-small-cell lung cancer
Supplemental material, sj-docx-2-tam-10.1177_17588359261447969 for Definitive radiotherapy provides comparable survival with lower toxicity compared with concurrent chemoradiotherapy after long-course induction chemoimmunotherapy in unresectable non-small-cell lung cancer by Xiao Chang, Huifang Liang, Jiayi Xiao, Dan Yang, Jiayi Yu, Jiahui Shan, Xin Dong, Wei Deng, Yuting Zhao, Leilei Jiang, Liuhua Long, Yue Teng, Huiming Yu, Rong Yu, Shaohua Ma and Anhui Shi in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank all clinicians, nurses, and research coordinators for their contributions to patient care and data collection.
Declarations
Supplemental material
Supplemental material for this article is available online.
Declaration of generative AI and writing assistance
During the preparation of this manuscript, the authors used ChatGPT to improve the clarity and readability of the language. After using this tool, the authors reviewed and edited the content and take full responsibility for the accuracy and integrity of all aspects of the manuscript. No external medical writer or editorial service was involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.