
Abstract
Background:
Receptor conversion, including changes in human epidermal growth factor receptor 2 (HER2) expression, has been reported after neoadjuvant therapy (NAT), but determinants of HER2 changes between baseline biopsy and residual disease remain incompletely understood.
Objective:
To evaluate the rate of HER2 status conversion after NAT and to identify factors associated with these changes in the context of contemporary treatment standards.
Design:
Retrospective analysis of patients with breast cancer (BC) treated with NAT followed by surgery between January 2019 and June 2024.
Methods:
BC was classified as HER2-0, HER2-low, or HER2-positive. HER2 expression before and after NAT was compared. Probabilities of HER2 subtype conversion were estimated, and univariable and multivariable analyses were performed to assess clinicopathological factors associated with HER2 status changes.
Results:
A total of 736 patients were included in the analysis, with HER2 status conversion observed in 34.2% (252/736) patients. The shift in HER2 expression occurred in 38.5% (94/244) of HER2-0, 27.9% (95/340) of HER2-low, and 41.4% (63/152) of HER2-positive tumors. A decrease in HER2 status was significantly more common than an increase (29.7% vs 18.2%; p < 0.001). The acquisition of HER2 positivity from initially HER2-0/low tumors was rare, occurring in only 19/584 (3.3%) cases. Downregulation of HER2 status from HER2-positive to HER2-0/low was more frequently observed in tumors initially classified as HER2 2+ with a positive fluorescence in situ hybridization (FISH) result compared to HER2 3+ tumors (adjusted odds ratio (ORadj) = 2.43, 95% confidence interval (CI): 1.18–5.01; p = 0.017). Similarly, the conversion from HER2-low to HER2-0 was observed more often in tumors initially classified as HER2 1+ compared to HER2 2+ with a negative FISH result (ORadj = 3.14; 95% CI: 1.20–8.22; p = 0.009). Conversely, the acquisition of HER2 positivity was significantly associated with high-grade (G3) tumors (ORadj = 5.50; 95% CI: 2.12–14.3; p < 0.001) and estrogen receptor expression >10% (ORadj = 8.61; 95% CI: 1.09–68.1; p = 0.041).
Conclusion:
HER2 status conversion affects about one-third of BCs after NAT, most commonly as downregulation, supporting HER2 reassessment in residual disease to guide post-NAT treatment decisions.
Plain language summary
Treatment decisions for people living with breast cancer are often guided by specific markers found in the tumor, such as hormone receptors and a protein called HER2. These markers help clinicians choose therapies that are most likely to be effective. In recent years, a new category termed HER2-low has been recognized in breast cancer. HER2-low tumors express low levels of HER2 and are not classified as HER2-positive, but they differ biologically from tumors with no HER2 expression. Traditionally, marker testing is performed at diagnosis, before treatment begins, and the results are assumed to remain unchanged. However, research increasingly shows that tumor markers can change after neoadjuvant therapy, which is treatment given before surgery. In people living with breast cancer who still have cancer cells present at surgery (known as residual disease), the remaining tumor may show different marker profiles compared with the original tumor. These changes may influence which treatments are appropriate after surgery. In this study of 736 patients living with breast cancer, a change in HER2 status was observed in approximately one in three patients after neoadjuvant therapy. These changes were seen across all initial HER2 groups. Importantly, reductions in HER2 expression were more common than increases, while the development of new HER2-positive tumors after treatment was rare. Despite how frequently these changes occur, there are currently no international guidelines that clearly define how tumor markers should be reassessed after neoadjuvant therapy or how such changes should guide further treatment. As a result, post-surgical treatment decisions may vary between hospitals and countries. By showing that tumor marker changes after neoadjuvant therapy affect about one in three people living with breast cancer, this study highlights the importance of reassessing tumor markers after treatment and supports efforts toward more consistent and personalized care.
Introduction
Neoadjuvant systemic therapy (NAT) is currently a recognized standard of care in locally advanced breast cancer (BC) for its benefits in downstaging tumors, determining response to treatment, and achieving a pathological complete response (pCR). NAT is now being applied to early-stage BC to tailor adjuvant treatment according to individual response to initial therapy. 1 The achievement of pCR following NAT is consistently linked to improved long-term outcomes, particularly in the aggressive subtypes of human epidermal growth factor receptor 2 (HER2)-positive BC and triple-negative BC (TNBC).2,3
Recent data demonstrate that receptor expression profiles, including HER2 status, can change following systemic treatment. Receptor conversion may have significant clinical relevance, particularly in the context of post-NAT planning and biological risk stratification.4–6 However, while reassessment of hormone receptor (HR) and HER2 status at disease recurrence is standard clinical practice in metastatic BC, no standardized international guidelines exist for evaluating receptor status in residual disease after NAT. 7 Existing studies describing post-treatment receptor discordance rarely quantify direction-specific transitions. Moreover, a proportion of these studies were conducted in earlier treatment eras, prior to the routine incorporation of contemporary neoadjuvant strategies, including dual HER2 blockade, immunotherapy, and optimized endocrine therapy.8,9 The absence of guidelines has led to significant variability in clinical practice across hospitals and countries. 10 Together, these limitations highlight the need for contemporary, direction-specific analyses of HER2 dynamics in patients treated with modern neoadjuvant regimens.
The emergence of HER2-low BC as an entity has expanded the scope of HER2 assessment. 11 HER2-low tumors, defined by an immunohistochemistry (IHC) score of 1+ or 2+ with negative in situ hybridization, account for approximately 45%–55% of all BCs. 12 The development of trastuzumab deruxtecan (T-DXd), an antibody-drug conjugate (ADC) showing activity beyond traditional HER2 expression thresholds in metastatic HER2-low tumors, has increased interest in accurate characterization of this population.13–15
The dynamic nature of HER2 expression post-NAT and the ability of tumors to convert between HER2 with IHC score 0 (HER2-0), HER2-low, and HER2-positive may render its clinical significance more pronounced in the HER2-low population. The identification of patterns and predictors of HER2 status conversion enhances understanding of tumor biology and the clinical context of HER2 reassessment in precision oncology. Given the clinical relevance of HER2 status conversion and the limited but expanding evidence base, a large retrospective cohort study was conducted to characterize the rate, patterns, and predictors of changes in HER2 status post-NAT in BC. We hypothesized that HER2 status may change between diagnostic biopsy and residual disease following systemic NAT. The primary objective of the study was to evaluate the rate of HER2 status conversion between biopsy and residual disease. Secondary objectives were to identify factors associated with receptor conversion and to assess its clinical context within current NAT practice.
Materials and methods
Study design and study population
This was a retrospective cohort study of consecutive patients with invasive BC receiving NAT followed by surgical resection from January 2019 to June 2024 at the Maria Sklodowska-Curie National Research Institute of Oncology in Warsaw, Poland. The study was approved by the Institutional Review Board, which reviewed the protocol for compliance with ethical and regulatory standards governing research involving human participants. Patients were eligible for inclusion if invasive BC was pathologically confirmed, NAT was completed, and subsequent surgery demonstrated residual invasive disease. Additional inclusion criteria comprised the availability of a pre-treatment biopsy and post-treatment surgical specimens for HER2 assessment, alongside sufficient clinical and pathological information. Patients with pCR or missing either pre- or post-NAT receptor status data were excluded from the analyses. The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 16
HER2 assessment and classification
HER2 assessment was performed within routine clinical practice by a single experienced breast pathology team throughout the study period. HER2 status was determined using standardized protocols, in accordance with the latest American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines. 17 For IHC, the HercepTest (Dako, Glostrup, Denmark) was used to determine HER2 status, first in the biopsy specimen and later in the resected tumor. HER2 IHC results were scored as 0, 1+, 2+, or 3+, based on the intensity and completeness of the membrane staining. When IHC results scored 2+, fluorescence in situ hybridization (FISH) assays were performed using the HER2 FISH pharmDx Kit (Dako). FISH was considered positive if average of HER2 signals/cell was ⩾4.0 with a HER2/CEP17 ratio of ⩾2.0 and negative if average of HER2 signals/cell was <4.0 with a HER2/CEP17 ratio of <2.0. Other combinations of average of HER2 signals/cell and a HER2/CEP17 ratio were interpreted according to ASCO/CAP guidelines. Tumors were then categorized as either: (1) HER2-0 if IHC result was 0; (2) HER2-low if IHC result was either 1+ or 2+ with negative FISH; (3) HER2-positive if IHC was either 3+ or IHC 2+ with positive FISH. 17 The same antibody clone, staining platform, and scoring criteria were applied consistently throughout the study period. No additional blinded dual scoring or centralized re-evaluation beyond routine diagnostic practice was performed.
Pathological examination
All specimens were handled according to standard protocols, by which formalin fixation and paraffin embedment were involved. Pathological assessment included the following: histological type (classified as no special type (NST), lobular, or other), histological grade (according to the Nottingham grading system: G1–G3), as well as Ki67 antigen and receptor expression (estrogen receptor (ER), progesterone receptor (PR), and HER2). ER and PR were considered positive if ⩾1% of tumor cells showed nuclear staining based on the ASCO/CAP guideline.17,18 On this basis, BC was classified as HR-positive, if ER and/or PR ⩾1%, otherwise as HR-negative. Expression of ER and PR was categorized into low-level (⩽10% of tumor cells showing nuclear staining) and high-level (>10%). BCs were classified as luminal (ER and/or PR-positive, HER2-0 or low), HER2-positive, and triple-negative BC (TNBC; ER and PR-negative, HER2-0 or low). Luminal BC was classified as B-like if PR expression was <20% or Ki67 expression >20%, otherwise as A-like. 19 Simplified initial clinical staging into stage I, II, and III was used. Data on Residual Cancer Burden and quantitative residual tumor cellularity were not routinely recorded and were not available for the entire cohort, precluding their inclusion in the analysis.
Statistical analysis
Categorical variables were presented as frequencies (n) and proportions (%) in groups or entire study population and compared between groups with the maximum likelihood G test (unpaired groups) or McNemar’s test (paired groups). The 95% confidence intervals (95% CIs) for proportions and for the difference between compared proportions were calculated using Wilson’s score method and Newcombe’s method, respectively. 20 Probability of conversion between HER2-subtypes in residual disease (post-NAT) was calculated as the number of patients whose BC converted divided by the number of patients in whom such a conversion was possible. The chance-corrected agreement in HER2 status between baseline biopsy and residual disease was determined using two weighted agreement coefficients for tests yielding categorical results in ordinal scale—Cohen’s weighted kappa (wK) and Gwet’s AC2, each with two systems of weighting—linear (wKl and AC2l, respectively) and quadratic (wKq and AC2q, respectively). 21 The chance-corrected agreement was arbitrarily classified as poor to fair if the coefficient was <0.4, moderate to good if the coefficient was 0.4–0.8, and very good if the coefficient was >0.8. 22 Numerical variables were examined for normality of distribution using the normal probability Q–Q plots and the Shapiro–Wilk W test. As the normality assumption was violated in all cases, numerical variables were summarized with the median, interquartile range (IQR), and range, and compared between groups with the Mann–Whitney U test (2 groups) or the Kruskal–Wallis H test (>2 groups). Correlations between numerical and ordinal variables were examined using the Spearman’s rank-order correlation coefficient (Rs). When investigating associations between potential explanatory variables and HER2 status conversions, the variables with p < 0.1 in the univariable analysis were entered into the multivariable analysis. The multivariable analysis was performed using backward stepwise logistic regression as an exploratory variable selection approach to identify the most relevant clinically meaningful predictors. The overall sample size and number of observed events were considered adequate in relation to the number of variables included in the multivariable models. Model performance was evaluated using measures of discrimination (area under the receiver operating characteristic curve) and goodness-of-fit (Hosmer–Lemeshow χ2 test and Nagelkerke’s pseudo-R2 coefficient). 23 The strength of association was expressed as the odds ratio (OR)—crude OR in the univariable analysis and adjusted OR (ORadj) in the multivariable analysis, and categorized as follows (presented only for positive associations): OR >1–2—weak, OR >2–5—moderate, OR >5–10—strong, OR >10—very strong association. All p-values were two-sided and the significance level (α) was set at 0.05. Statistical analysis was performed using TIBCO Statistica 13.3 (TIBCO Software Inc., Palo Alto, CA, USA). No imputation was performed; all analyses were conducted on complete cases.
Results
Patient and tumor characteristics
In total, 736 patients met eligibility criteria, of whom 5 were men (0.7%). The process of patient selection is detailed in the flowchart (Figure 1). Baseline clinical characteristics and treatment approaches are presented in Table 1. Age of patients at time of diagnosis ranged from 26 to 94 years with the median (IQR) of 62 (49–70) years. The majority of patients presented with stage II disease (478/736 (65.0%) patients), followed by stage III (210/736 (28.5%) patients) and stage I (48/736 (6.5%)). Two-thirds of patients had luminal BC (487/736 (66.2%) patients; predominantly luminal B-like—304/487 (62.4%) patients), followed by HER2-positive (152/736; 20.6%; mostly ER/PR-positive—126/152 (82.9%) patients), and TNBC (97/736 (13.2%) patients). Of 487 luminal BC and 97 TNBC patients, 340/584 patients were classified as HER2-low (58.2%), and 244/584 patients as HER2-0 (41.8%).
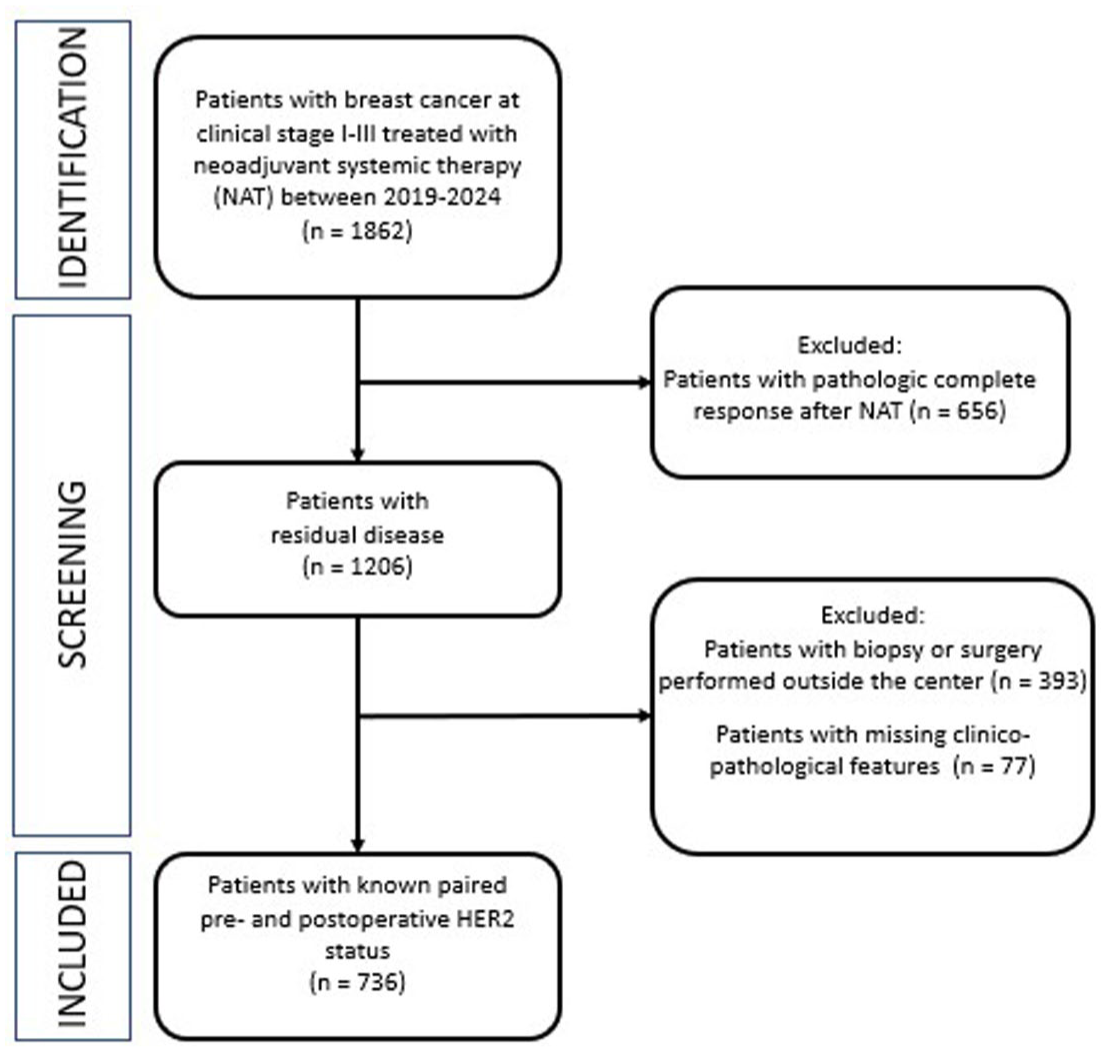
Study cohort selection flowchart.
Baseline clinicopathologic characteristics of 736 patients included in the study.

Presented as the median, IQR, and range.
Significant difference bolded.
ER, estrogen receptor; FISH, fluorescence in situ hybridization; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; IQR, interquartile range; NST, no special type; PR, progesterone receptor; TNBC, triple-negative breast cancer.
Regarding HR status, 610/736 (82.9%) tumors were ER-positive (593/610 (97.2%) patients were ER-high), and 507/736 (68.9%) were PR-positive (423/507 (83.4%) patients were PR-high). Most HER2-low BCs were IHC 1+ (293/340 (86.2%) patients) and most HER2-positive BC were IHC 3+ (110/152 (72.4%) patients).
NATs were selected based on the patient and tumor characteristics. The most common NAT regimens were anthracycline and taxane combinations regimen (42.2%) or taxane and carboplatin regimens (23.4%). Of 152 HER2-positive patients, 92 patients (60.5%) received trastuzumab alone, while 60 patients (39.5%) were given dual HER2 blockade with trastuzumab and pertuzumab. Among patients with luminal BC, neoadjuvant chemotherapy was administered more commonly than neoadjuvant endocrine therapy, although the difference was minimal (294/487 (53.7%) vs 193/487 (46.3%) patients). For patients with TNBC, carboplatin was used in 59/97 patients (60.8%), with 22/97 patients (22.7%) receiving immunotherapy (pembrolizumab).
HER2 status of study population before and after neoadjuvant therapy
Following NAT, the proportion of patients with HER2-positive BC decreased by 6.0% (95% CI: 3.6%–8.4%; p < 0.001) from 20.6% (152/736 patients) to 14.6% (108/736 patients) while the proportion of patients with HER2-low BC increased by 5.6% (95% CI: 1.5%–9.6%; p = 0.009) from 46.2% (340/736 patients) to 51.8% (381/736 patients). The proportion of patients with HER2-0 BC remained stable accounting for 33.2% of patients (244/736 patients) before NAT and 33.6% (247/736 patients) after NAT (p = 0.885; Figure 2(a)). These changes indicate a redistribution of HER2 categories at the population level following NAT.

Distribution of HER2-0, HER2-low, and HER2-positive categories at baseline biopsy (Pre-NAT) and in residual disease (Post-NAT). While overall group proportions appear stable in (a), substantial internal transitions between HER2 categories are observed, as illustrated in (b). (a) Proportion of patients with a particular HER2 category at baseline (Pre-NAT) and in residual disease (Post-NAT). (b) HER2 categories in residual disease—the pie chart shows proportions of patients whose HER2 category remained unchanged compared to baseline biopsy and proportion of patients whose HER2 category changed (discordant results); the adjacent bar chart details the type of change which led to a discordant result.
However, despite this seemingly stable overall picture, significant patient transitions were observed between HER2 status groups. Even though sizes of groups did not differ much, their composition markedly changed. The HER2 status remained the same before and after NAT in 65.8% (484/736) of patients (Figure 2(b)). The chance-corrected agreement was moderate across all commonly accepted classification systems (Table S1). This level of agreement reflects substantial individual-level variability in HER2 classification between baseline and residual disease.
A change in HER2 status following NAT was observed in 214 of 613 patients with HR-positive disease (34.9%; 95% CI: 31.2%–38.8%) and in 38 of 123 patients with HR-negative disease (30.9%; 95% CI: 23.4%–39.5%; p = 0.389). Detailed subgroup results are provided in Table S2. Changes in HER2 receptor status in the overall study population and according to HR expression are presented in Figure 3 and Figure S1(A) and (B).
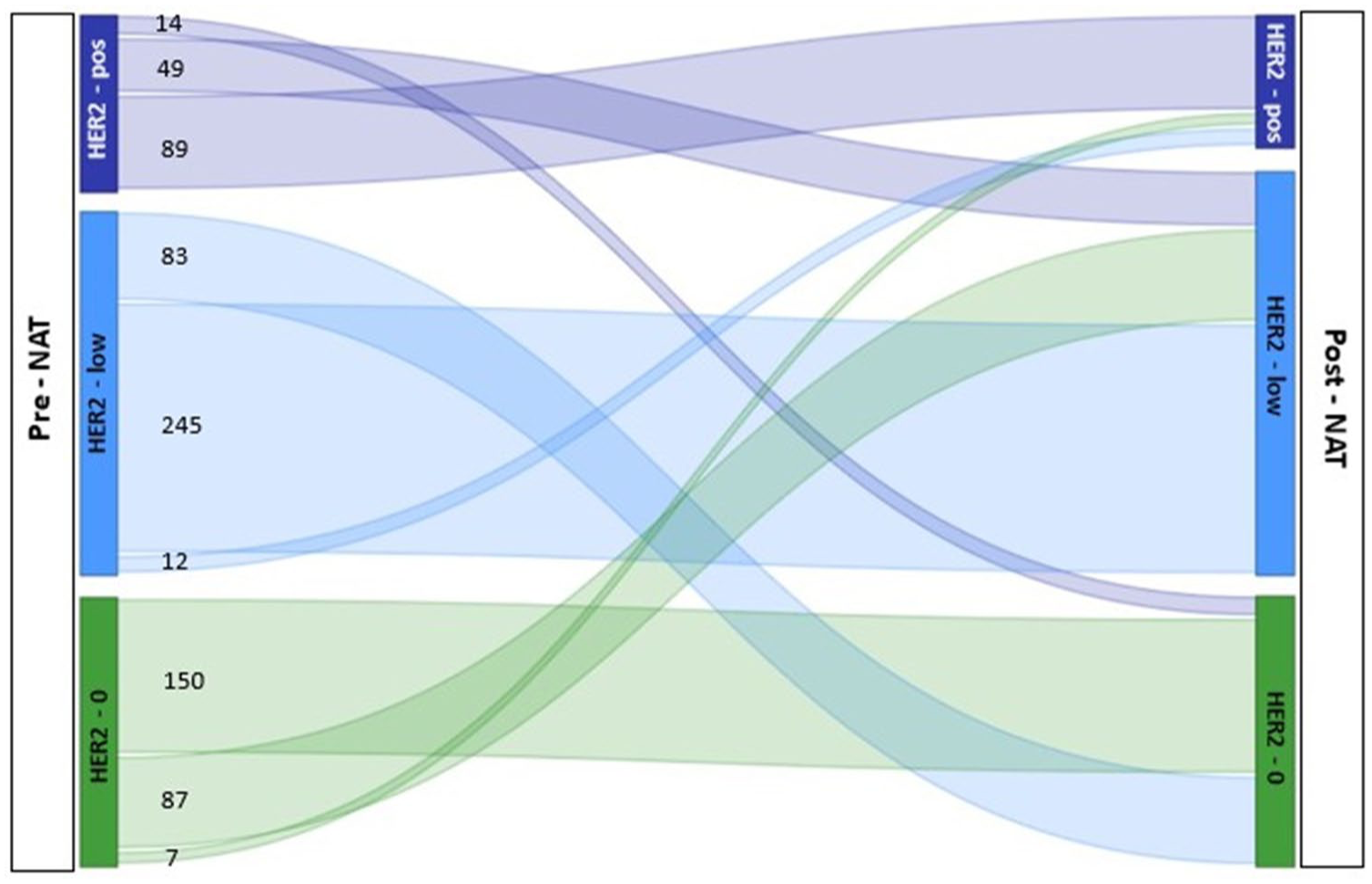
Sankey diagram illustrating the evolution of HER2 expression from baseline biopsy (Pre-NAT) to residual disease after neoadjuvant therapy (Post-NAT). Flow width represents the number of patients transitioning between HER2 categories, with numerical labels showing absolute counts.
Patterns of HER2 status conversion
HER2 status conversion was observed in 252 of 736 patients (34.2%, 95% CI: 30.9%–37.7%). HER2 status change was significantly less likely in patients with HER2-low tumors (95/340 patients; 27.9%; 95% CI: 23.4%–32.9%) compared to patients with HER2-0 BCs (94/244 patients; 38.5%; 95% CI: 32.6%–44.8%; p = 0.003) and patients with HER2-positive BCs (63/152 patients; 41.4%; 95% CI: 33.9%–49.4%; p = 0.007). No significant difference was observed in the probability of shift between the latter two groups (p = 0.563). These findings indicate that baseline HER2 category influences the probability of post-treatment HER2 status change.
Downregulation of HER2 expression occurred in 146/492 patients with HER2-positive or HER2-low tumors (29.7%; 95% CI: 25.8%–33.9%) and was a significantly more common phenomenon than upregulation of HER2 expression, which occurred in 106/584 patients with HER2-0 or HER2-low tumors (18.2%; 95% CI: 15.2%–21.5%; p < 0.001).
Detailed analysis of HER2 status conversion
Among 244 patients with HER2-0 tumors, 94 (38.5%) converted to either HER2-low (87/244 (35.7%) patients) or HER2-positive (7/244 (2.9%) patients). From 340 patients with HER2-low tumors, 95 (27.9%) converted to either HER2-0 (83/340 (24.4%) patients) or HER2-positive (12/340 (3.5%) patients). In turn, 63 of 152 patients with HER2-positive tumors (41.4%) converted to either HER2-low (49/152 (32.2%) patients) or HER2-0 (14/152 (9.2%) patients; Table 2; Figure 3).
Conversion of HER2 status between baseline and residual disease.
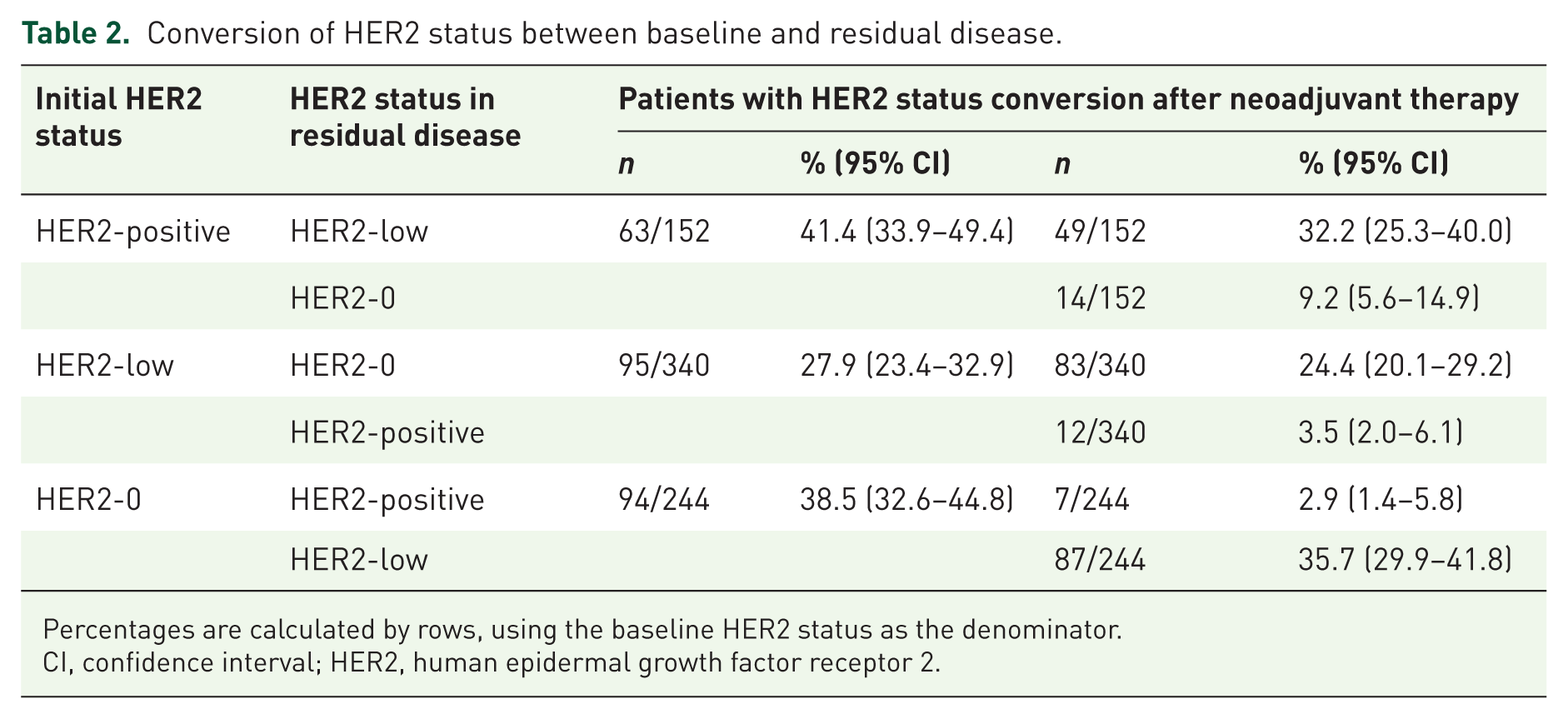
Percentages are calculated by rows, using the baseline HER2 status as the denominator.
CI, confidence interval; HER2, human epidermal growth factor receptor 2.
From the total group of 252 patients whose HER2 status changed after NAT, the most common phenomenon was the flow of patients between HER2-0 and HER2-low (both directions), followed by the flow of patients from HER2-positive to HER2-low, with the move of patients between two extreme groups (HER2-positive to HER2-0 and vice versa), being the least prevalent pattern of receptor change (Figure 2(b)).
One- and two-level HER2 status conversions
A one-level decrease in HER2 status (from HER2-positive to HER2-low or from HER2-low to HER2-0) was much more likely (132/492 (26.8%) patients) than a two-level decrease from HER2-positive to HER2-0 (14/152 (9.2%) patients; p < 0.001). Probabilities of transition from HER2-positive to HER2-low (49/152 (32.2%) patients) and HER2-low to HER2-0 status (83/340 (24.4%) patients) did not significantly differ (p = 0.070; Table 2, Figure 3).
Similarly, a one-level increase in HER2 status (from HER2-0 to HER2-low and from HER2-low to HER2-positive) was considerably more common (99/584 (17.0%) patients) than a two-level increase from HER2-0 to HER2-positive (7/244 (2.9%) patients; p < 0.001). However, the probability of increase from HER2-0 to HER2-low (87/244 (35.7%) patients) was significantly higher than the probability of increase from HER2-low to HER2-positive (12/340 (3.5%) patients; p < 0.001; Table 2, Figure 3).
A two-level shift between the extreme HER2 status groups was very unlikely (21/396 (5.3%) patients). However, a two-level decrease remained significantly more frequent (14/152 (9.2%) patients) than a two-level increase (7/244 (2.9%) patients; p = 0.007; Table 2, Figure 3).
Factors associated with HER2 status conversion
Exploratory analyses were performed to identify clinicopathological factors associated with HER2 status conversion. The only characteristic of HER2-positive BCs that appeared to be associated with a higher probability of conversion to HER2-0/low was IHC 2+/FISH+ pattern. Such HER2-positive tumors had approximately 2.4-fold higher odds of conversion (ORadj = 2.43, 95% CI: 1.18–5.01; p = 0.017; Table 3). High PR expression approached statistical significance in the univariable analysis, most likely because it was significantly and positively correlated with the IHC 2+/FISH+ pattern (high PR expression was observed in 30/42 (71.4%) IHC 2+/FISH+ tumors, compared to only 47/110 (42.7%) IHC 3+; p = 0.001); therefore, it was not an independent factor (Figure S2).
Univariable and multivariable analysis of associations between baseline clinicopathologic characteristics of patients with HER2-positive breast cancer and the conversion to HER2-0/HER2-low status after neoadjuvant therapy.
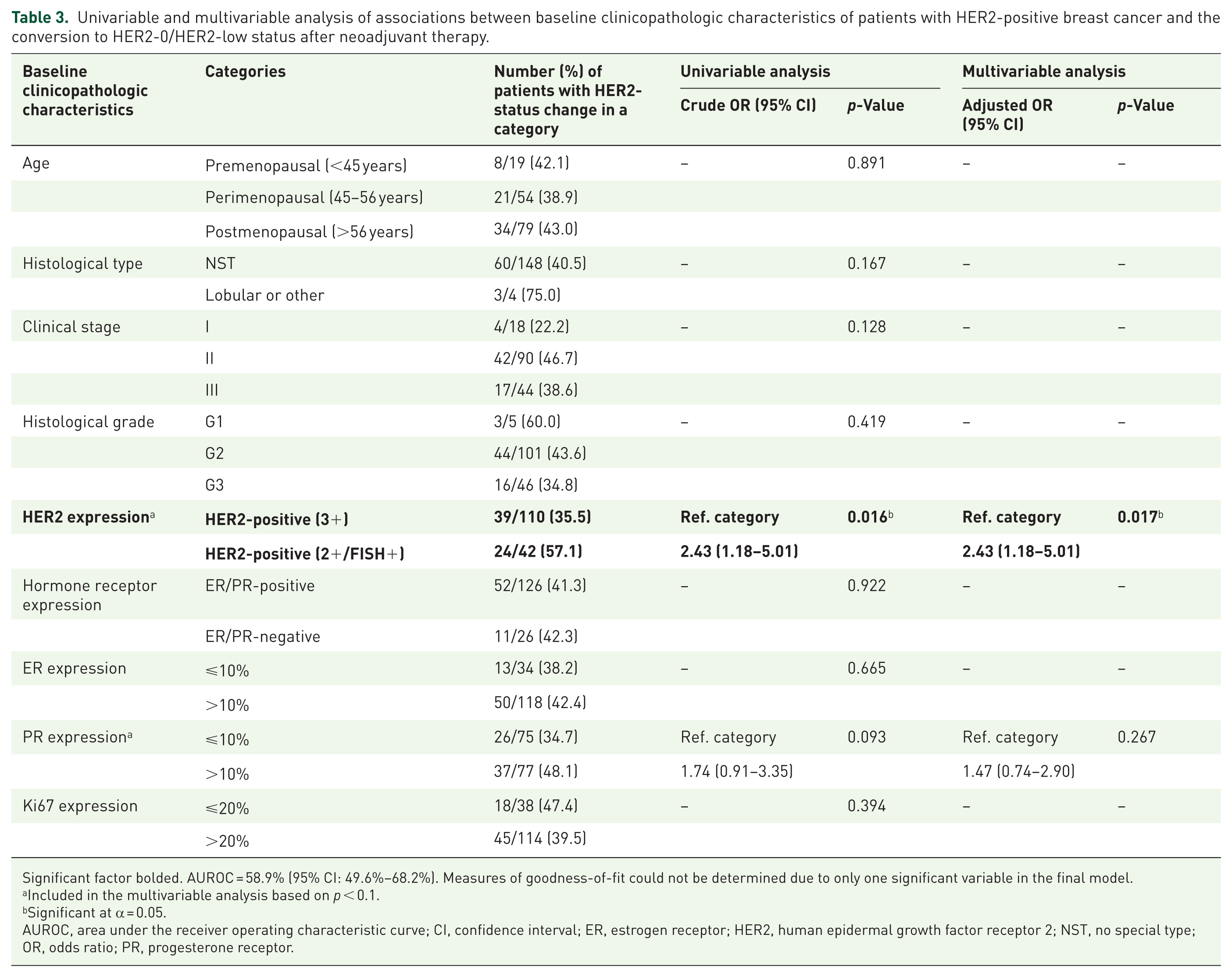
Significant factor bolded. AUROC = 58.9% (95% CI: 49.6%–68.2%). Measures of goodness-of-fit could not be determined due to only one significant variable in the final model.
Included in the multivariable analysis based on p < 0.1.
Significant at α = 0.05.
AUROC, area under the receiver operating characteristic curve; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NST, no special type; OR, odds ratio; PR, progesterone receptor.
High ER expression and G3 are two factors that were found to be significantly and independently associated with the opposite conversion from HER2-0/low to HER2-positive (Table 4). Both associations were strong, tumors with high ER expression had approximately 9-fold higher odds of conversion (ORadj = 8.61; 95% CI: 1.09–68.1; p = 0.041), and those with G3 approximately 6-fold higher odds (ORadj = 5.50; 95% CI: 2.12–14.3; p < 0.001). Ki67 expression >20%, which was significant in the univariable analysis, lost its significance in the multivariable model when ER expression and histological grade were included, likely because, in HER2-0/low BCs, Ki67 was significantly negatively correlated with ER expression (Rs = −0.32, p < 0.001) and positively with histological grade (Rs = 0.54, p < 0.001; Figure S3).
Univariable and multivariable analysis of associations between baseline clinicopathologic characteristics of patients with HER2-0/HER2-low breast cancer and the conversion to HER2-positive status after neoadjuvant therapy.
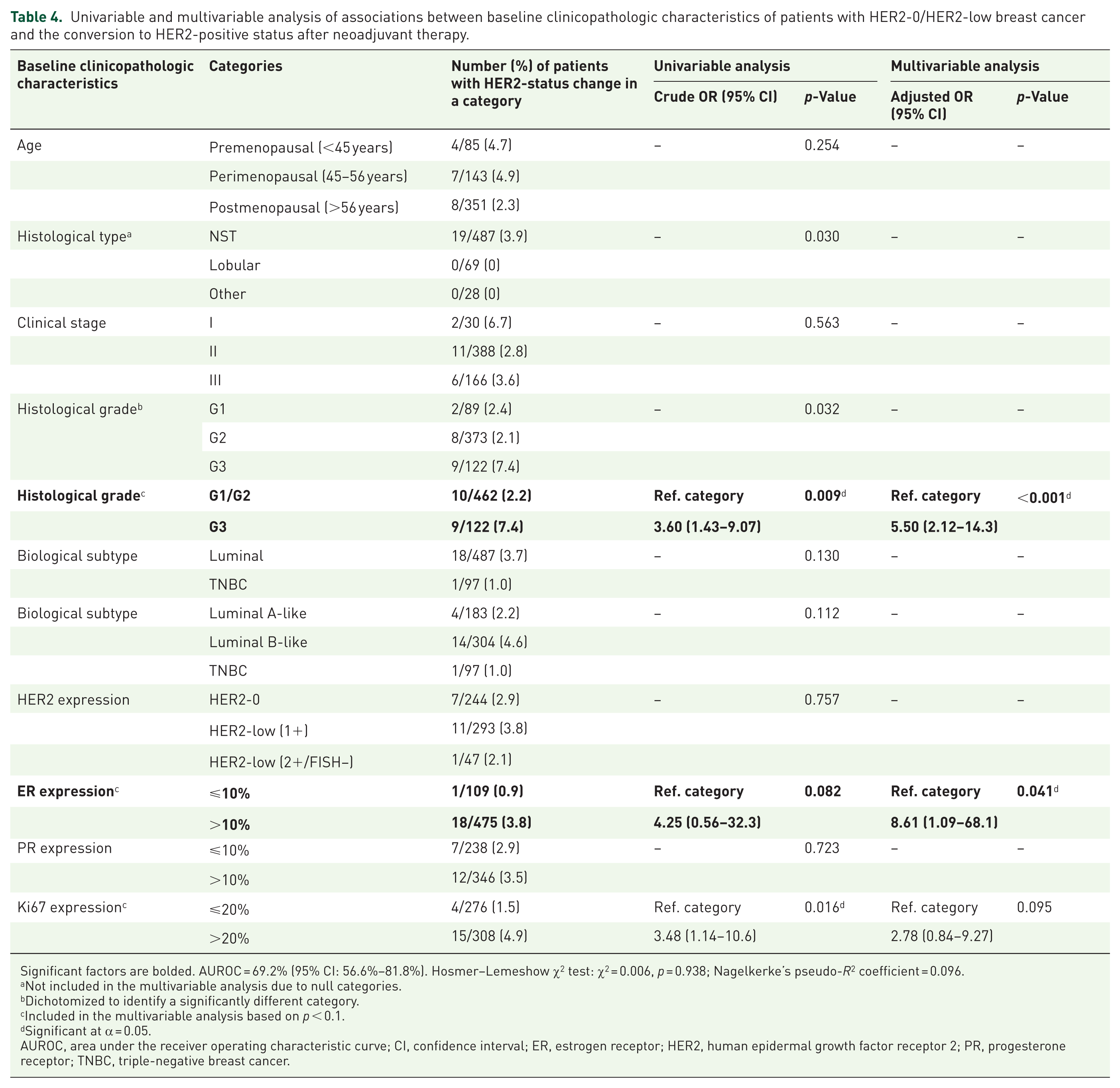
Significant factors are bolded. AUROC = 69.2% (95% CI: 56.6%–81.8%). Hosmer–Lemeshow χ2 test: χ2 = 0.006, p = 0.938; Nagelkerke’s pseudo-R2 coefficient = 0.096.
Not included in the multivariable analysis due to null categories.
Dichotomized to identify a significantly different category.
Included in the multivariable analysis based on p < 0.1.
Significant at α = 0.05.
AUROC, area under the receiver operating characteristic curve; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; TNBC, triple-negative breast cancer.
The analysis of conversions between three HER2 groups (HER2-positive, HER2-low, and HER2-0) confirmed that HER2 downregulation followed a relatively straightforward pattern, whereas upregulation appeared more complex.
The only factors significantly and positively associated with HER2 downregulation were those IHC/FISH patterns which were closer to the subtype into which an initial subtype tended to shift; that is, HER2-positive BC with IHC 2+/FISH+ pattern was significantly more likely to change to HER2-low than those with an IHC 3+ pattern (ORadj = 2.72; 95% CI: 1.26–5.87; p = 0.011; Table S3) and HER2-low BC with IHC 1+ pattern was significantly more likely to change to HER2-0 than those with IHC 2+/FISH− pattern (ORadj = 3.14; 95% CI: 1.20–8.22; p = 0.009; Table S4). Both associations were moderate. No factor was identified as significantly associated with the most extreme downregulation from HER2-positive to HER2-0 (Table S5).
Upregulation of HER2 expression from HER2-0 to HER2-low was significantly more likely in tumors with high ER expression (ORadj = 2.04; 95% CI: 1.07–3.90; p = 0.031) and in clinical stage III (ORadj = 2.13; 95% CI: 1.18–3.86; p = 0.013; Table S6). Both associations were weak. In the univariable analysis, the conversion was also significantly more likely in luminal BCs, however the luminal subtype was by definition strongly associated with ER expression and therefore did not remain an independent factor in the multivariable analysis. The subsequent step of upregulation, from HER2-low to HER2-positive, was strongly and positively associated with higher Ki67 expression (ORadj = 6.14; 95% CI: 1.32–28.6; p = 0.021; Table S7). In the univariable analysis, G3 was also positively associated with this conversion; however, due to a strong correlation between histological grade and Ki67 expression (Rs = 0.55, p < 0.001), only the latter remained significant in the multivariable model. The most extreme upregulation from HER2-0 to HER2-positive was a very rare event (observed only in 7 women) and occurred mostly in perimenopausal patients aged 45–56 years, which was the only factor significantly and strongly associated with this conversion (ORadj = 8.53; 95% CI: 1.58–45.9; p = 0.013). Interpretation of this finding is limited by the small number of events. Clinical stage III remained significant in the univariable analysis and was borderline significant in the multivariable analysis (Table S8).
Overall, multivariable analyses demonstrated distinct and asymmetric patterns of factors associated with HER2 downregulation versus upregulation after NAT, and the models demonstrated acceptable discrimination (area under the receiver operating characteristic curve = 60%–75%) and good fit.
Discussion
This large, contemporary real-world study of 736 BC patients across the full HER2 spectrum (0/low/positive) provides a detailed characterization of receptor dynamics after NAT. HER2 conversion occurred in approximately one-third of patients with residual disease (34.2%), confirming that HER2 expression is a dynamic and biologically structured feature rather than a fixed trait.
Frequency and patterns of HER2 conversion
Several large analyses have recently adopted a tri-level HER2 framework encompassing HER2-0, HER2-low, and HER2-positive categories. The studies by Tarantino et al., 8 Baez-Navarro et al., 24 Boman et al., 25 and Zhu et al. 26 collectively established the overall magnitude of HER2 discordance after NAT to be typically around 30% and confirmed that the majority of conversions occurred between HER2-0 and HER2-low groups. In contrast, selected Asian series have reported lower rates, likely reflecting differences in methodology and treatment era.27,28 Most of these large studies primarily provided descriptive estimates of discordance, without addressing determinants of HER2 change. Zhu et al. 26 identified ER positivity as a factor associated with HER2 loss, whereas Sung et al. 29 found that nodal involvement, ER and PR expression, and lower baseline HER2 scores predicted conversion. Still, all of these analyses were conducted in cohorts treated exclusively with chemotherapy and, when indicated, anti-HER2 therapy, without inclusion of endocrine therapy or immunotherapy.
Our study differs substantially in this regard. Conducted in a fully modern treatment context, it includes patients managed with regimens integrating dual HER2 blockade, immune checkpoint inhibitor (pembrolizumab), and endocrine therapy for HR-positive disease, reflecting the therapeutic landscape of 2020–2024. By combining tri-level HER2 assessment with within-low stratification (IHC 1+ vs 2+/FISH-negative) and multivariable, direction-specific modeling, this analysis extends beyond descriptive work and provides an updated, clinically relevant view of HER2 dynamics under contemporary treatment conditions. These findings reflect receptor dynamics in the residual disease setting, while patterns in patients achieving pCR remain largely undefined.
Predictors of HER2 status conversion
Several clinicopathological factors were associated with HER2 status conversion in this cohort. The baseline HER2 IHC score emerged as the strongest predictor: tumors with intermediate baseline expression (IHC 2+)—irrespective of FISH status—were significantly more likely to undergo conversion than those classified as IHC 3+. This observation is biologically plausible, as tumors with borderline HER2 expression may represent a less stable state along the HER2 axis, prone to either amplification loss or gain depending on intrinsic clonal heterogeneity. A similar pattern was described by Katayama et al. 30 and Lee et al., 9 supporting the concept that HER2 modulation is more frequent in tumors with intermediate receptor activity.
HER2 upregulation was associated with high histological grade (G3) and with tumors showing ER expression above 10%. While high grade reflects increased proliferative potential and genomic instability, the link with ER positivity likely represents a distinct mechanism. In ER-positive tumors, HER2 gain may reflect adaptive signaling cross-talk between the ER and HER2 pathways; however, this remains a biological hypothesis rather than a confirmed mechanism. In the study by Sung et al., 29 nodal involvement was the only clinicopathological feature significantly associated with HER2 conversion, although the direction of this change was not specified.
Importantly—and in contrast to our findings—Zhu et al. 26 reported that HER2 loss occurred more frequently in ER-positive tumors. In our cohort, HER2 gain was enriched among ER-positive cancers (ER >10%), while HER2 loss was most frequent in baseline IHC 2+/amplified tumors. Divergent findings across studies may reflect differences in treatment era, therapeutic exposure, and methodological approaches, including assay methods, scoring systems, and sampling strategies and the distribution of intermediate phenotypes.
Taken together, these results indicate that HER2 modulation is context-dependent and shaped by both intrinsic tumor biology and treatment environment. By providing direction-specific risk estimates, our analysis identifies which baseline phenotypes are most prone to HER2 loss (IHC 2+/amplified) or gain (G3, ER >10%), which may support a more risk-adapted approach to receptor reassessment. These findings reinforce the need for systematic HER2 retesting after NAT and provide a biological rationale for optimizing the use of ADCs in early BC.
Clinical implications in the ADC era
The expanding use of ADCs has redefined the clinical relevance of HER2 evaluation. DESTINY-Breast04 established T-DXd as the standard of care for HER2-low metastatic BC, while DESTINY-Breast05 and DESTINY-Breast11, presented recently, extended this paradigm to early HER2-positive disease.13,31,32 In DESTINY-Breast05, T-DXd outperformed T-DM1 even without reassessment of HER2 in residual disease—an effect likely driven by its bystander activity against HER2-low and ultralow tumor cells. 32
In this context, HER2 status conversion after NAT may potentially influence eligibility for ADC-based strategies, which are currently guided by baseline HER2 assessment.
Early-phase neoadjuvant trials such as TRIO-US B-12 TALENT (T-DXd ± endocrine therapy in HR-positive, HER2-low tumors) achieved high objective response rates (63%–75%) but low pCR levels (~5%), suggesting persistent biological heterogeneity within HER2-low disease. 33 Similarly, exploratory studies such as SURVIVE-HERoes are evaluating T-DXd in the early disease setting, extending ADC use beyond the metastatic context. 34
These developments highlight a key gap: current ADC trials rely exclusively on baseline HER2 assessment, without accounting for receptor modulation during or after NAT. Our study addresses this gap by characterizing real-world, direction-specific HER2 dynamics across the full expression spectrum in patients treated with modern regimens. This biological context complements clinical trial evidence, suggesting that systematic reassessment of HER2 in residual disease may optimize patient selection for emerging ADC strategies.
Patients with baseline IHC 2+/amplified tumors warrant particular vigilance for HER2 loss, which may alter post-neoadjuvant eligibility for anti-HER2 or ADC-based therapy. Conversely, HER2 gain in G3 or ER-positive tumors could expand therapeutic options. Recognizing HER2 as a dynamic continuum rather than a binary marker may have implications for trial design, drug sequencing, and the development of adaptive treatment algorithms in early BC.
Importantly, a recently published meta-analysis of 22 studies confirmed that receptor status conversions significantly affect patient outcomes: both gain and loss of HER2 expression were associated with reduced disease-free survival, whereas overall survival was significantly worse only among patients who lost HER2 expression. 4
Despite growing evidence, standards for HER2 reassessment remain undefined, leading to variability in clinical practice. Consequently, lack of retesting may lead to suboptimal post-neoadjuvant treatment, particularly in cases of receptor gain. In this context, the present findings, demonstrating frequent and direction-specific HER2 status changes after NAT, provide biological context for considering post-treatment reassessment in selected clinical scenarios. Prospective studies are therefore warranted to determine how reassessment should be implemented and how biological conversion should guide therapy adaptation. Predictive models integrating clinical and molecular features could help identify patients most likely to benefit from retesting.
Finally, the dynamic nature of HER2 expression highlights opportunities for real-time biomarker monitoring using circulating tumor DNA and liquid biopsy. In the future, these approaches may enhance detection of receptor evolution and enable personalized, adaptive treatment strategies in early BC. 35
Technical considerations
Potential technical factors that could contribute to apparent HER2 conversion include pre-analytical issues such as fixation time, tissue processing, or storage conditions, as well as analytical variability related to antibody clones or detection systems. Sampling differences between core biopsy and surgical specimens may also lead to discordant results due to spatial heterogeneity. 36 The reproducibility of HER2-low classification, particularly for IHC 1+ and 2+ categories, is a recognized challenge and has been shown to be affected by interobserver variability, especially near decision thresholds.37,38 Recent CAP-led reproducibility initiatives and interobserver variability studies have highlighted these limitations. 39
However, in our study, both biopsy and resection specimens were evaluated by the same pathology team using uniform methodology and validated assays, which minimizes analytical noise. The high internal consistency across subgroups and reproducibility of the findings further support the methodological robustness of the analysis. The consistent and directionally structured nature of observed changes, together with their alignment with biological features such as histological grade and ER expression, supports the interpretation that the observed HER2 status changes likely reflect a combination of true biological modulation, intratumoral heterogeneity, and analytical variability, rather than a single underlying mechanism. In particular, within the HER2-low range, some observed conversions may reflect borderline immunohistochemical differences rather than true biological shifts.
Strengths and limitations
This study has several notable strengths. It represents one of the largest single-institution series exploring HER2 dynamics after NAT, combining a uniform pathology workflow with a tri-level HER2 assessment and within-low stratification (IHC 1+ vs 2+/FISH−). The inclusion of direction-specific multivariable modeling provides a nuanced understanding of receptor modulation across the HER2 axis. Importantly, the cohort reflects a contemporary therapeutic landscape, encompassing patients treated with dual HER2 blockade, immunotherapy, and endocrine therapy, thereby enhancing clinical relevance and generalizability to modern practice.
Limitations include the retrospective and single-center design, which may limit external validity and reflect center-specific practice patterns, potentially affecting the generalizability of the findings, and the absence of long-term outcome data, precluding correlation of receptor conversion with survival endpoints. Given the exploratory nature of the analyses, no formal correction for multiple comparisons was applied because we did not want to reduce power of statistical analyses. Moreover, due to observational character of the study, we did not have influence on the number of patients with a certain outcome (i.e., change of receptor) which were included. This resulted in violation of generally accepted requirements regarding sample size (i.e., minimum of 10 events per variable analyzed in logistic regression analysis) in some of our models. 40 Therefore, their results should be interpreted with caution and the potential risk of overfitting and model instability associated with stepwise procedures and limited sample size in some of the models should be taken into account. While survival outcomes were not assessed, the study was designed to address biological dynamics rather than prognostic impact, precluding any direct inference regarding clinical outcomes or treatment recommendations. Moreover, treatment-specific variables were intentionally not analyzed to avoid confounding across biologically distinct subtypes. Nevertheless, the large, methodologically consistent cohort ensures robust internal validity, and the comprehensive, direction-based approach provides an essential biological context that complements and extends prior multicenter and registry-based studies. Altogether, the study bridges biological insights with real-world therapeutic relevance in the ADC era.
Conclusion
HER2 conversion after NAT is frequent, affecting approximately one-third of patients, and follows reproducible, direction-specific patterns. Down-regulation predominated over up-regulation, with HER2 loss most common among baseline IHC 2+/amplified tumors, whereas HER2 gain was observed primarily in high-grade and ER-positive cancers. Within the HER2-low category, approximately one-quarter of tumors transitioned to HER2-0, highlighting the biological variability of low-level HER2 expression.
By integrating full-spectrum HER2 classification, contemporary therapeutic exposure, and direction-specific modeling, this study complements and advances previous large tri-level analyses. The findings support the concept of HER2 as a dynamic biological feature rather than a static biomarker and provide a framework for interpreting HER2 status changes in residual disease after NAT. Further prospective studies are warranted to clarify the clinical significance of HER2 reassessment and to determine how post-neoadjuvant receptor dynamics may be appropriately incorporated into future treatment algorithms.
Supplemental Material
sj-jpg-1-tam-10.1177_17588359261451850 – Supplemental material for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis
Supplemental material, sj-jpg-1-tam-10.1177_17588359261451850 for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis by Katarzyna Pogoda, Magdalena Czopowicz, Agata Bak, Wojciech Olszewski, Michal Czopowicz, Monika Durzynska, Dorota Najmrocka, Paulina Halasa, Anna Borowiec, Zbigniew Nowecki and Anna Niwinska in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-2-tam-10.1177_17588359261451850 – Supplemental material for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis
Supplemental material, sj-jpg-2-tam-10.1177_17588359261451850 for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis by Katarzyna Pogoda, Magdalena Czopowicz, Agata Bak, Wojciech Olszewski, Michal Czopowicz, Monika Durzynska, Dorota Najmrocka, Paulina Halasa, Anna Borowiec, Zbigniew Nowecki and Anna Niwinska in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-3-tam-10.1177_17588359261451850 – Supplemental material for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis
Supplemental material, sj-jpg-3-tam-10.1177_17588359261451850 for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis by Katarzyna Pogoda, Magdalena Czopowicz, Agata Bak, Wojciech Olszewski, Michal Czopowicz, Monika Durzynska, Dorota Najmrocka, Paulina Halasa, Anna Borowiec, Zbigniew Nowecki and Anna Niwinska in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-4-tam-10.1177_17588359261451850 – Supplemental material for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis
Supplemental material, sj-jpg-4-tam-10.1177_17588359261451850 for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis by Katarzyna Pogoda, Magdalena Czopowicz, Agata Bak, Wojciech Olszewski, Michal Czopowicz, Monika Durzynska, Dorota Najmrocka, Paulina Halasa, Anna Borowiec, Zbigniew Nowecki and Anna Niwinska in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-5-tam-10.1177_17588359261451850 – Supplemental material for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis
Supplemental material, sj-pdf-5-tam-10.1177_17588359261451850 for Dynamics of HER2 status following neoadjuvant systemic therapy in breast cancer: a large single-center cohort analysis by Katarzyna Pogoda, Magdalena Czopowicz, Agata Bak, Wojciech Olszewski, Michal Czopowicz, Monika Durzynska, Dorota Najmrocka, Paulina Halasa, Anna Borowiec, Zbigniew Nowecki and Anna Niwinska in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
This study was supported by the Maria Sklodowska-Curie National Research Institute of Oncology, Warsaw, Poland, which acted as the funding institution and covered the article processing charge. This work has been previously presented as a poster (39P) at ESMO Breast Cancer Congress 2025.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.