
Abstract
Background:
Hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) breast cancer represents the most prevalent molecular subtype but demonstrates pronounced biological and clinical heterogeneity. Homologous recombination deficiency (HRD) and tumor-infiltrating lymphocytes (TILs) have recently emerged as key determinants of prognosis and immune activity, but their interplay in this subtype remains understudied.
Objectives:
To assess the relationship between HRD, TILs, and clinical outcomes in HR+/HER2− breast cancer and validate the prognostic value of HRD.
Design:
Retrospective multicenter cohort study.
Methods:
A total of 365 patients (332 with available TILs data) from three institutions were enrolled. HRD was quantified using Shallow HRD algorithm on low-depth whole-genome sequencing (threshold: score ⩾6). TILs were evaluated by the MD Anderson system (⩾10% classified as high). Spearman correlation, Kaplan–Meier survival analysis, and multivariable Cox regression were performed.
Results:
HRD scores were inversely correlated with TILs (Spearman rho = −0.13, p = 0.031). HRD-high patients had significantly inferior 10-year survival (invasive disease-free survival (IDFS): 31.0% vs 57.9%, hazard ratio (HR) = 2.36; distant recurrence-free survival (DRFS): 34.1% vs 61.1%, HR = 2.48; overall survival (OS): 48.7% vs 79.0%, HR = 2.79; p < 0.0001). HRD was confirmed as an independent prognostic predictor (IDFS HR = 2.03, DRFS HR = 2.16, OS HR = 2.15; p < 0.01). No significant survival benefit from anthracycline-based chemotherapy was observed in HRD-high tumors (HR = 1.32, p = 0.451). High TILs showed no significant association with survival outcomes in this cohort.
Conclusion:
HRD represents a reliable independent prognostic biomarker in HR+/HER2− breast cancer in this cohort, with an inverse association with TILs suggesting immune evasion. Its potential impact on prognosis and treatment requires further validation in prospective clinical trials.
Plain language summary
This study explores how a genetic feature (HRD) and immune cells in tumours (TILs) affect outcomes for patients with HR+/HER2- breast cancer. HR+/HER2- breast cancer varies widely in its biological features; while HRD and TILs both influence patient outcomes and immune activity against cancer, their interaction is not well understood. The researchers conducted a retrospective study, analyzing existing data from 365 HR+/HER2- breast cancer patients across three medical centers. HRD levels were measured using a genetic test, with a high score indicating more genetic damage in cancer cells; TILs were rated by a standard system, where high TILs meant 10 percent or more of tumour tissue consisted of these immune cells. Statistical analysis was used to assess the links between HRD, TILs and patients’ 10-year survival. The study found that higher HRD scores were associated with lower TILs in tumours. Patients with high HRD had significantly worse 10-year survival outcomes compared to those with low HRD, with far fewer remaining free of invasive cancer, free of cancer spread, or alive after 10 years. HRD was confirmed as an independent predictor of survival, meaning it can forecast patient outcomes regardless of other patient or cancer characteristics. Additionally, anthracycline-based chemotherapy did not improve survival for patients with high HRD tumours. High TILs had no clear association with survival in this patient group. The findings confirm that HRD is a reliable independent predictor of survival for HR+/HER2- breast cancer patients in this research group. The link between high HRD and low TILs also suggests that cancer cells with high HRD may be able to evade the body’s immune system. Further forward-looking clinical trials are needed to confirm HRD’s impact on patient outcomes and identify the best treatment approaches for patients with high HRD scores.
Keywords
Introduction
Hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) breast cancer accounts for approximately 60%–70% of breast malignancies, representing the largest disease subtype worldwide. Despite substantial therapeutic progress with endocrine agents, 20%–30% of patients ultimately relapse at distant sites, largely due to genomic instability and mechanisms of immune evasion.1,2
Using a four-omics strategy (genome, transcriptome, methylome, and proteome), the Fudan molecular classification stratifies HR+/HER2− breast tumors into four groups: SNF1 (classic luminal), SNF2 (immune-enriched), SNF3 (proliferative), and SNF4 (receptor tyrosine kinase-driven). 2 The proliferative SNF3 subtype is characterized by prominent homologous recombination deficiency (HRD) enrichment, while the SNF2 subtype is defined by immune activation. Notably, HRD positivity or immune activation can also be detected in the other subtypes. More importantly, this classification did not perform a direct correlation analysis between HRD status and immune infiltration, nor did it address the crosstalk between genomic instability and the tumor immune microenvironment across these subtypes. 2
HRD reflects impaired DNA double-strand break repair and has become an important biomarker in the oncology field. 3 In BRCA-mutant tumors, HRD status predicts sensitivity to poly (ADP-ribose) polymerase inhibitors (PARPi), with the OlympiA trial reporting a marked improvement in progression-free survival (hazard ratio (HR) = 0.58, p < 0.001) for Olaparib. 4 Beyond the context of PARPi, HRD has also been linked to increased responsiveness to DNA-damaging chemotherapy. For example, in breast cancer patients carrying germline DNA damage repair mutations, 11.6% achieved pathological complete response (pCR) following anthracycline-based therapy. 5 Similarly, application of the AcornHRD algorithm revealed that HRD-positive patients were significantly more likely to achieve low residual cancer burden (0/1; odds ratio = 10.29, p = 0.005) compared with HRD-negative counterparts. 6 However, the clinical implications of HRD in unselected HR+/HER2− populations remain poorly defined. Mechanistic studies suggest that HRD not only enhances genomic instability but may also reshape the tumor immune landscape. In estrogen receptor-positive (ER+) breast cancer, APOBEC3B-mediated R-loop accumulation induces immunosuppressive signaling cascades, contributing to immune evasion. 7 Parallel findings in ovarian cancer demonstrate that although HRD increases tumor mutational burden and neoantigen load, it simultaneously promotes expansion of regulatory T cells (Tregs), ultimately suppressing antitumor immunity, which is an effect that can be reversed by PARPi treatment.8,9 Together, these insights raise the possibility that HRD fosters an immunosuppressive microenvironment in HR+/HER2− breast cancer. In parallel, immunotherapy trials are reshaping the therapeutic landscape. KEYNOTE-756 (pembrolizumab) and CheckMate-7FL (nivolumab) demonstrated that immune checkpoint inhibitors (ICIs) significantly increase pCR rates in high-risk HR+/HER2− breast cancer: KEYNOTE-756 reported 24.3% versus 15.6% (p = 0.00005), while CheckMate-7FL reported 24.5% versus 13.8% (p = 0.0021). In CheckMate-7FL, patients with stromal tumor-infiltrating lymphocytes (TILs) >1% achieved pCR rates of 44.4% in the nivolumab group compared with 21.1% in the control arm.10,11 Miglietta et al. identified a modest positive correlation between stromal TILs and the Oncotype Recurrence Score (r = 0.223, p < 0.001), with TIL-high tumors enriched in higher-risk groups (p = 0.006). However, the contribution of HRD to this association remains unaddressed. 12
Most HRD-related studies have focused on triple-negative breast cancer (TNBC). It is reported that HRD-S status was associated with high TIL density in the overall cohort, but the number of HRD-S cases in the non-TNBC subgroup was too small for further stratified analysis. 13 Another study only described HRD prevalence in ER+ breast cancer without further investigation. 14 To date, no large-scale multicenter study has systematically analyzed the relationship between HRD and immune infiltration specifically in HR+/HER2− breast cancer. Our study thus sought to clarify the genomic-immune interplay by jointly evaluating HRD and TIL status in HR+/HER2− breast cancer using shallow whole-genome sequencing (sWGS) for HRD scoring and standardized pathological TIL quantification. By correlating these biomarkers with long-term outcomes, we aim to identify distinct clinically relevant subgroups and clarify their prognostic implications, which may provide a basis for optimizing individualized treatment strategies in future clinical research.
Materials and methods
Patients and endpoints
This retrospective analysis included patients diagnosed with HR+/HER2− breast cancer at three Chinese institutions: Zhejiang Cancer Hospital (2002–2021), Jinhua Municipal Central Hospital (2014–2020), and the First Hospital of Jiaxing (2010–2019; Table S1). A total of 365 patients met eligibility criteria, with exclusion of those with secondary malignancies. Among these 365 patients, 301 cases were ER+/PR+, 57 were ER+/PR−, and 7 were ER−/PR+. A total of 332 cases with TIL assessment were derived exclusively (Table 1). The reporting of this retrospective multicenter cohort study confirms to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies 15 (Supplemental File 1). The study protocol received approval from Medical Ethics Committee of Zhejiang Provincial Cancer Hospital (IRB-2020-190), the First Hospital of Jiaxing (2025-LP-324), and written informed consent was obtained from each patient. Jinhua Municipal Central Hospital waived ethical review as all data were collected retrospectively.
Comparison of clinicopathological characteristics between the low HRD group and the high HRD group.

Bold text indicates p values that showed significance.
Invasive special carcinoma with good prognosis included tubular, mucinous, papillary, and cribriform carcinoma.
Other types with poor prognosis included micropapillary carcinoma and carcinoma simplex.
AI, aromatase inhibitor; ALND, axillary lymph node dissection; BMI, body mass index; DRFS, distant recurrence-free survival; ER, estrogen receptor; HRD, homologous recombination deficiency; IDC, invasive ductal carcinoma; IDFC, invasive disease-free survival; ILC, invasive lobular carcinoma; OS, overall survival; PR, progesterone receptor; SLNB, sentinel lymph node biopsy; TAM, tamoxifen; TILs, tumor-infiltrating lymphocytes.
Comprehensive clinicopathological characteristics were abstracted from medical records, including age at diagnosis, body mass index (BMI), tumor size, lymph node status, histological type, grade, vascular invasion, and expression of ER, progesterone receptor (PR), and HER2. Tumors were classified as HR+ if ER and/or PR nuclear staining was ⩾10%. HER2 negativity was defined as immunohistochemistry scores of 0 or 1+, or 2+ with negative confirmation by fluorescence in situ hybridization.
Patients were followed until October 2024. Scheduled follow-up occurred every 3 months during the first 2 years post-surgery, every 6 months for years 3–5, and annually thereafter. Additional visits were performed as needed in response to concerning symptoms or clinical findings.
Three primary endpoints were analyzed for this study, including: (1) invasive disease-free survival (IDFS), measured from surgery to the first occurrence of ipsilateral invasive breast cancer, locoregional recurrence, distant relapse, contralateral invasive breast cancer, second primary invasive malignancy, or death from any cause; (2) distant recurrence-free survival (DRFS), measured from surgery to the first occurrence of distant metastasis; and (3) overall survival (OS), measured from surgery to death from any cause.
Shallow HRD
To evaluate HRD in HR+/HER2− breast cancer, we applied the Shallow HRD algorithm, which has been validated by Eeckhoutte et al. 16 This method utilizes sWGS at approximately 1× coverage to quantify large-scale genomic alterations (LGAs), serving as indicators of HRD.
Genomic DNA was isolated from formalin-fixed, paraffin-embedded tumor tissue. Library construction was performed with 100 ng of input DNA using Agilent reagents, involving ligation, PCR amplification, and AMPure XP bead purification. DNA concentrations were measured with Qubit® kits, and library integrity was confirmed on an Agilent TapeStation. Pre-capture pools at 4 or 1.8 nM were sequenced on the NextSeq 550 S or NovaSeq 6000 platforms to generate 150-bp paired-end reads at a median depth of 1×. 17 Raw reads were trimmed with FASTP, aligned to the GRCh37/hg19 reference genome using BWA-MEM, and duplicate reads flagged with Picard Tools. 16 The Shallow HRD algorithm was then employed to analyze copy number variation profiles, incorporating LGAs and sample quality metrics (including copy-number median absolute deviation) to determine HRD status, with special annotation for borderline or poor-quality samples. 16
To define an HRD threshold appropriate for this HR+/HER2− cohort, LGA scores were calculated for all 365 tumors. Quartile distributions of LGA values were compared against previously reported HRD-positive rates of 21%–27% in HR+/HER2− breast cancer. 18 A cutoff score of 6 was selected, yielding an HRD-high proportion of 23.8% (87/365 cases), which aligned with the published 21%–27% range, 18 and provided clear separation in the quartile-based LGA score distribution. Sensitivity analyses were performed using alternative cutoffs of 4 and 8 to validate the robustness of the chosen threshold. Survival analyses and correlation analyses showed highly consistent results with minimal differences between the cutoffs of 4 and 6. However, the cutoff of 6 exhibited a more favorable HRD-high proportion that better matched the range reported in previous studies. In contrast, the cutoff of 8 resulted in a reduced sample size of the HRD-high subgroup, leading to a decreased statistical power. This threshold was therefore adopted to classify HRD-high (⩾6) and HRD-low (<6) tumors for downstream analyses in this study, enabling robust assessment of genomic-clinical and genomic-immune associations. Detailed results of these sensitivity analyses are presented in Tables S2–S5.
TIL analyses
Uniform TIL assessment protocols were implemented across all three participating institutions. TILs were assessed in the stromal compartment of tumor sections following deparaffinization, rehydration, and routine immunohistochemical staining. All tumor sections were independently scored by two experienced senior pathologists who were blinded to the clinical outcomes and follow-up data. Evaluation was performed under light microscopy in strict accordance with international consensus guidelines and the uniform MD Anderson scoring framework. Inter-observer agreement for TILs scoring was quantitatively validated using the Cohen’s kappa coefficient, with an agreement achieved (κ = 0.71). For cases with discrepant scores, a third senior pathologist with extensive expertise in breast cancer pathology was consulted for an arbitration review, and a consensus score was ultimately reached for statistical analysis. The proportion of stromal area occupied by lymphocytes was quantified as a percentage to assess TIL prevalence. Tumors were classified as low-TILs (<10%) or high-TILs (⩾10%) for statistical analyses.12,19
Statistical analysis
All analyses were conducted with SPSS v26 and R v4.3.0, with a two-sided p < 0.05 being significant. Associations between HRD status and clinicopathological variables were examined using Pearson’s Chi-square test or Fisher’s exact test, as appropriate. The relationship between HRD scores and TILs was tested by Spearman’s rank correlation. Survival distributions were estimated by Kaplan–Meier analysis and compared via log-rank tests. For subgroup analyses, Kaplan–Meier curves and log-rank tests were stratified by HRD status within each treatment category, and in the HRD-high subgroup, outcomes were compared between patients receiving anthracycline-based chemotherapy and those who did not. To investigate the combined prognostic value of genomic and immune features in the main cohort, and to avoid observation bias potentially caused by inter-center differences in TILs assessment, patients from Zhejiang Cancer Hospital with paired HRD and TILs data were stratified into four subgroups by HRD status and TILs status: HRD−/TILs−, HRD+/TILs−, HRD−/TILs+, and HRD+/TILs+. Kaplan–Meier curves were plotted for IDFS, DRFS, and OS in the four subgroups, and log-rank test was used to compare the survival differences among subgroups. Multivariate prognostic effects were determined using Cox proportional hazards regression models, in which censoring was defined as follow-up termination or loss to follow-up with no recurrence or death events observed. The proportional hazards assumption was verified using the Schoenfeld residual test, and the global test yielded p > 0.05 for all models, confirming the models satisfied the assumption. Only adjuvant radiotherapy in the IDFS of the total population, tumor size in the IDFS of the total population and Zhejiang Cancer Hospital cohort, and chemotherapy in the IDFS and DRFS of Zhejiang Cancer Hospital cohort showed minor violations at the individual level, with no impact on the global test for the proportional hazards assumption. For missing or unknown data, a complete case analysis was used in the multivariable models, with cases of unknown values excluded.
Results
Patient and clinicopathological characteristics
A total of 365 patients diagnosed with HR+/HER2− breast cancer between 2002 and 2021 across three hospitals were included (Figure 1). Baseline demographics and tumor characteristics are summarized in Table 1. At diagnosis, the median age was 49 years (range: 28–84 years). Lymph node involvement was present in 65.9% (240/365), invasive ductal carcinoma accounted for 89.3% (326/365), and 93.2% (340/365) were classified as pathological grade II/III. All patients underwent surgical resection. During follow-up, 146 patients developed recurrence or metastasis, while 219 remained disease-free. Regarding adjuvant management, 215 patients (58.9%) received (neo)adjuvant chemotherapy, among whom 6.8% underwent neoadjuvant chemotherapy, 166 (45.5%) received radiotherapy, and 293 (80.3%) received endocrine therapy.

Study design. HR+/HER2− breast cancer patients with sufficient primary tumor tissue (no distant metastasis) were retrospectively included from 2002 to 2021 across three hospitals. They underwent baseline data collection, shallow HRD assessment, TILs detection (subset), long-term follow-up (until October 2024), plus survival, subgroup, and recurrence analyses.
HRD and TILs
HRD analysis was successfully performed using the Shallow HRD algorithm on 365 tumor samples. The median HRD score was 1 (range: 0–29; Figure 2(a)). Based on the predetermined cutoff, 87 cases (23.8%) were classified as HRD-high (⩾6), while 278 (76.2%) were HRD-low (<6). Median follow-up was 76 months (range up to 120 months). Valid TIL evaluation was available for 332 tumors across the three participating centers, with the detailed sample distribution shown in Figure 2(b). Of these, 264 cases (72.3%) were categorized as low-TILs (<10%), and 68 cases (18.6%) as high-TILs (⩾10%). Spearman correlation analysis demonstrated a modest but statistically significant negative correlation between HRD scores and TIL levels in Zhejiang Cancer Hospital cohort (Rho = −0.13, p = 0.031; Figure 2(c)), this inverse association was independently reproduced in other two individual center with consistent directional trends (Jinhua Municipal Central Hospital: Figure 2(d), Spearman Rho = −0.33, p = 0.043; First Hospital of Jiaxing: Figure 2(e), Spearman Rho = −0.22, p = 0.3). In paired samples from eight patients who developed recurrence, HRD scores were consistently higher in metastatic lesions compared with corresponding primary tumors. The most pronounced increase was from a score of 0 in the primary tumor to 28 in the metastatic site (p = 0.012; Figure S1).
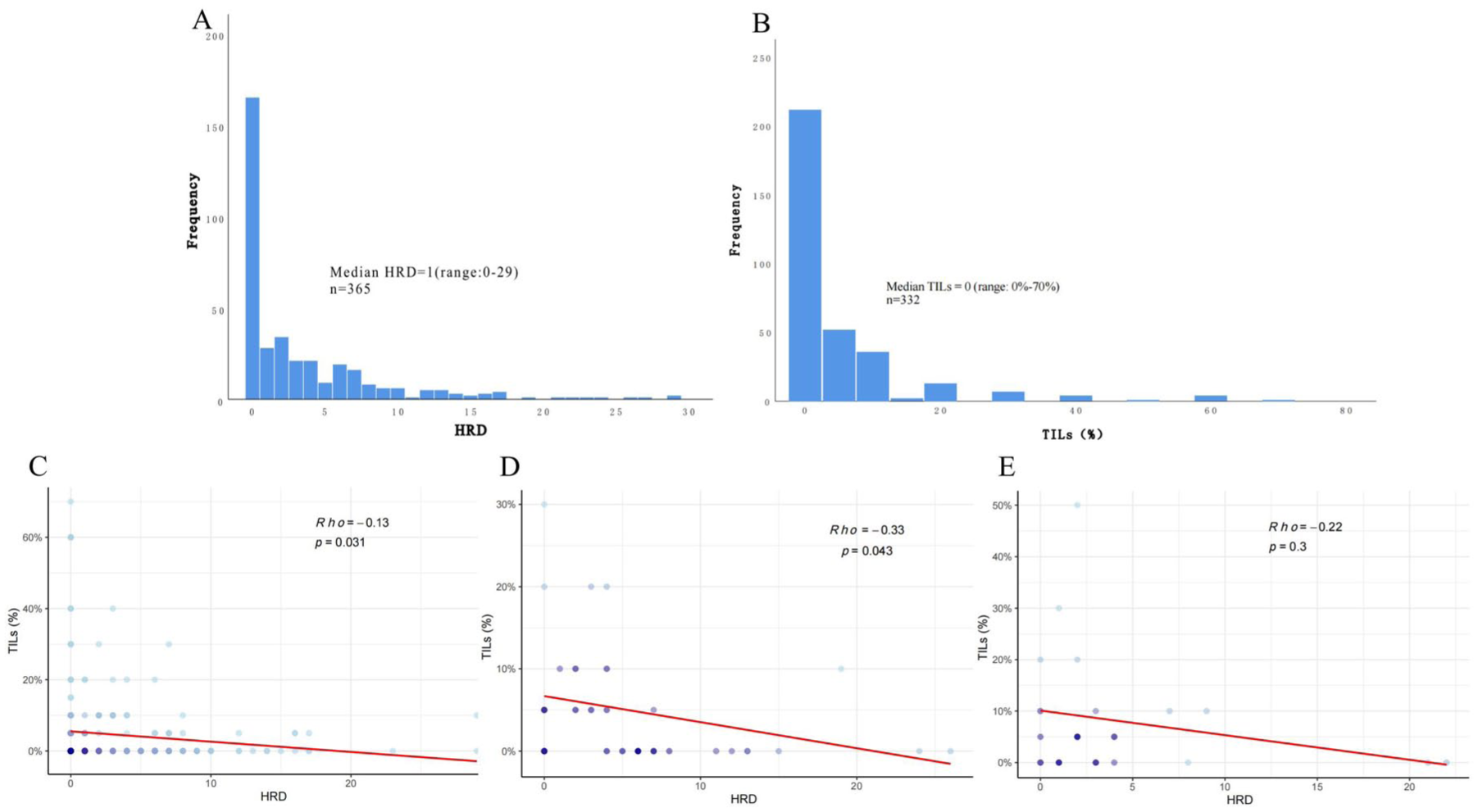
(a) HRD distribution in HR+/HER2− breast cancer patients. (b) TILs distribution in HR+/HER2− breast cancer patients. The correlation between HRD and TILs in (c) Zhejiang Cancer Hospital, (d) Jinhua Municipal Central Hospital, (e) the First Hospital of Jiaxing.
Association between HRD and clinicopathological characteristics
As summarized in Table 1, HRD-high tumors were significantly associated with an earlier age at onset (p = 0.031), a higher pregnancy frequency (p = 0.024), a higher pathological grade (p = 0.015), and reduced TIL infiltration (p = 0.014), but was unrelated to BMI, age at menarche, menopausal status at diagnosis, tumor size, lymph node metastasis, pathological type, vascular invasion, ER status, or PR status. Patients with HRD-high tumors were more likely to develop recurrence or distant metastasis compared with those with HRD-low disease (p < 0.001). In addition, surgical and treatment patterns differed by HRD status: HRD-high patients more frequently underwent mastectomy and axillary lymph node dissection, and they more often received intensive adjuvant therapy, including radiotherapy and anthracycline-based chemotherapy.
High HRD is associated with worse patient survival
Kaplan–Meier survival analysis revealed markedly poorer outcomes in the HRD-high group relative to HRD-low patients. Ten-year IDFS was 31.0% in HRD-high tumors versus 57.9% in HRD-low (HR = 2.36, p < 0.0001; Figure 3(a)). DRFS was 34.1% versus 61.1% (HR = 2.48, p < 0.0001; Figure 3(b)). OS was 48.7% versus 79.0% (HR = 2.79, p < 0.0001; Figure 3(c)). Collectively, these results indicate that high HRD burden is a predictor of recurrence, metastasis, and mortality in HR+/HER2− breast cancer.
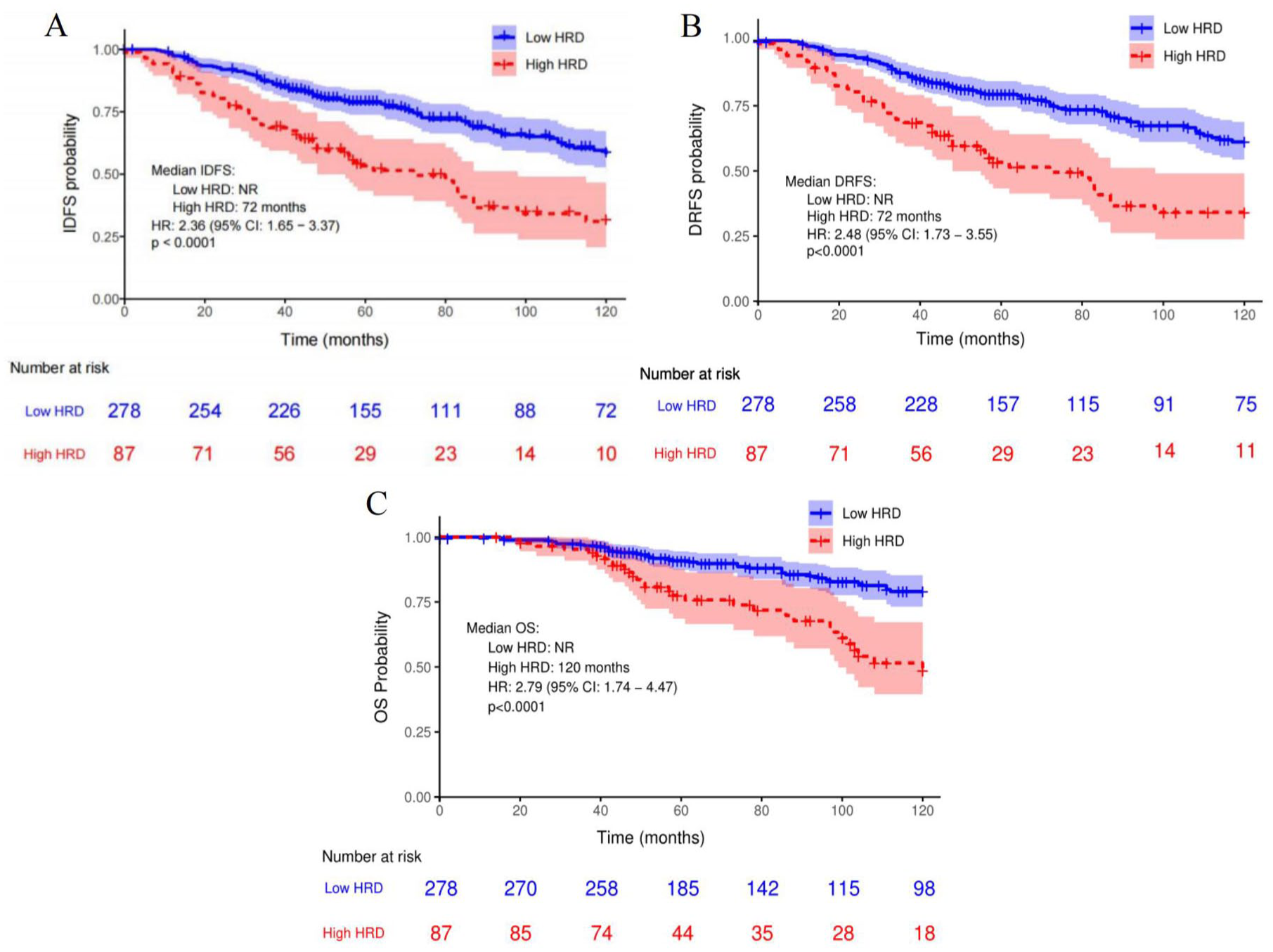
Survival analysis of patients stratified by HRD status. Survival (Kaplan–Meier) as a function of HRD status of patients for (a) IDFS, (b) DRFS, and (c) OS of all patients.
Anthracycline-based drug efficacy in the context of HRD
In patients with HRD-high tumors, outcomes were further examined according to whether they received anthracycline-based chemotherapy. The two groups were generally well balanced with respect to baseline characteristics; however, those treated with anthracycline-based drugs tended to be younger, more frequently premenopausal, and more often received ovarian suppression (Tables S6 and S7). Patients in the anthracycline group also displayed a trend toward more aggressive disease features, although these differences did not reach statistical significance. OS analysis revealed no statistically significant difference between patients treated with anthracycline-based drugs and those who were not (HR = 1.32, 95% confidence interval (CI): 0.64–2.73, p = 0.451; Figure S2). Nevertheless, survival curves began to diverge after approximately 85 months: the non-anthracycline group reached a median survival of 101 months, whereas the anthracycline group did not reach median OS even at 120 months. Within the anthracycline-based drug subgroup, HRD-high status was consistently associated with inferior long-term outcomes, including 10-year IDFS (HR = 2.94, p < 0.0001), DRFS (HR = 2.83, p < 0.0001), and OS (HR = 2.54, p = 0.003; Figure 4), mirroring the adverse prognostic impact observed in the full cohort.
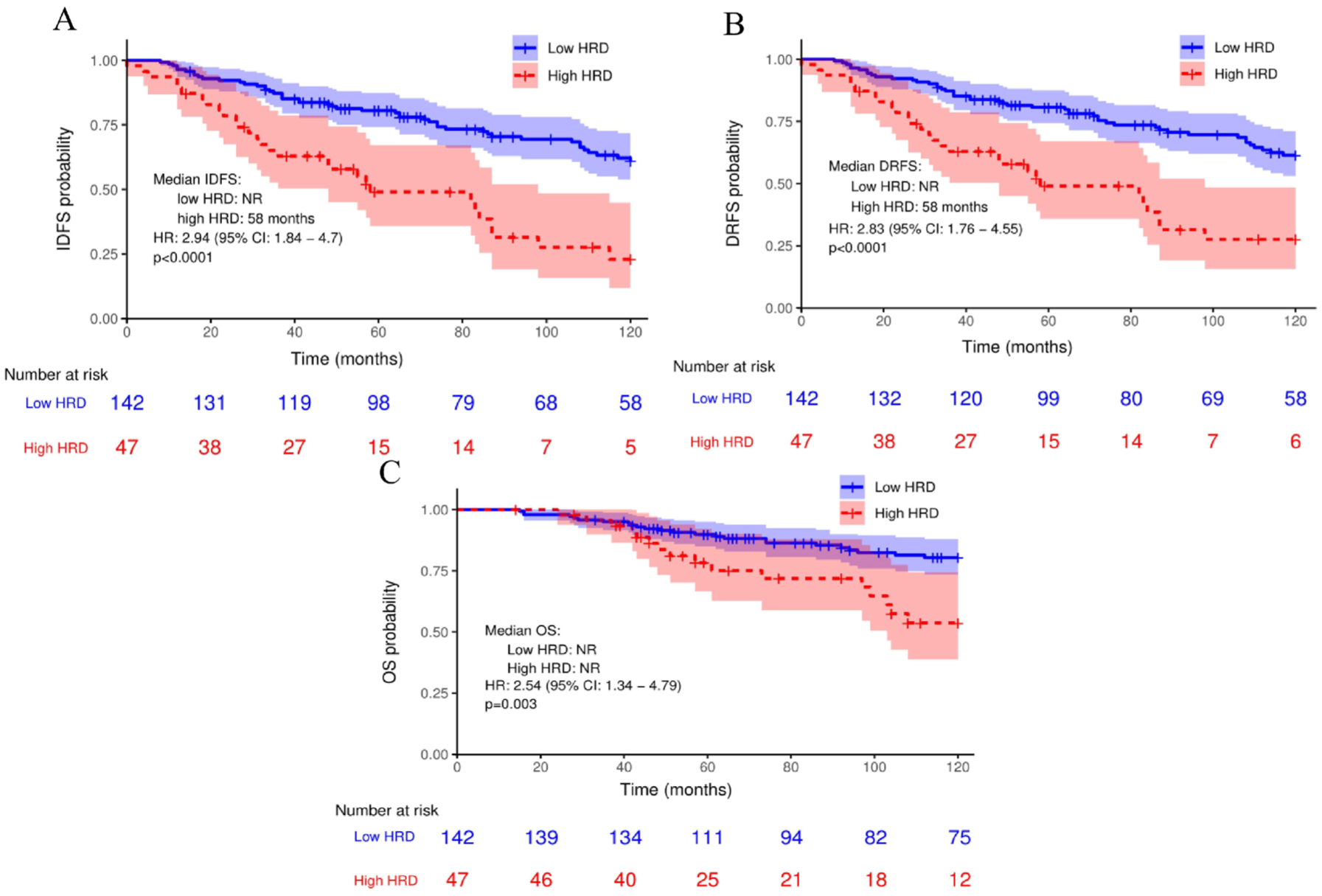
Survival analysis of patients received anthracycline-based drugs stratified by HRD status. Survival (Kaplan–Meier) as a function of HRD status of patients received anthracycline-based drugs for (a) IDFS, (b) DRFS, and (c) OS of all patients.
High TILs may indicate a better prognosis
Survival analyses stratified by stromal TIL levels showed non-significant but favorable trends for patients with high TILs compared to those with low TILs. Kaplan–Meier curves indicated improved IDFS (HR = 0.62, p = 0.153), DRFS (HR = 0.64, p = 0.184), and OS (HR = 0.59, p = 0.263; Figure 5) in the high-TILs group. Although these results did not reach statistical significance, the consistent directional trend suggests a potentially beneficial effect of elevated TILs infiltration on clinical outcomes in HR+/HER2− breast cancer.
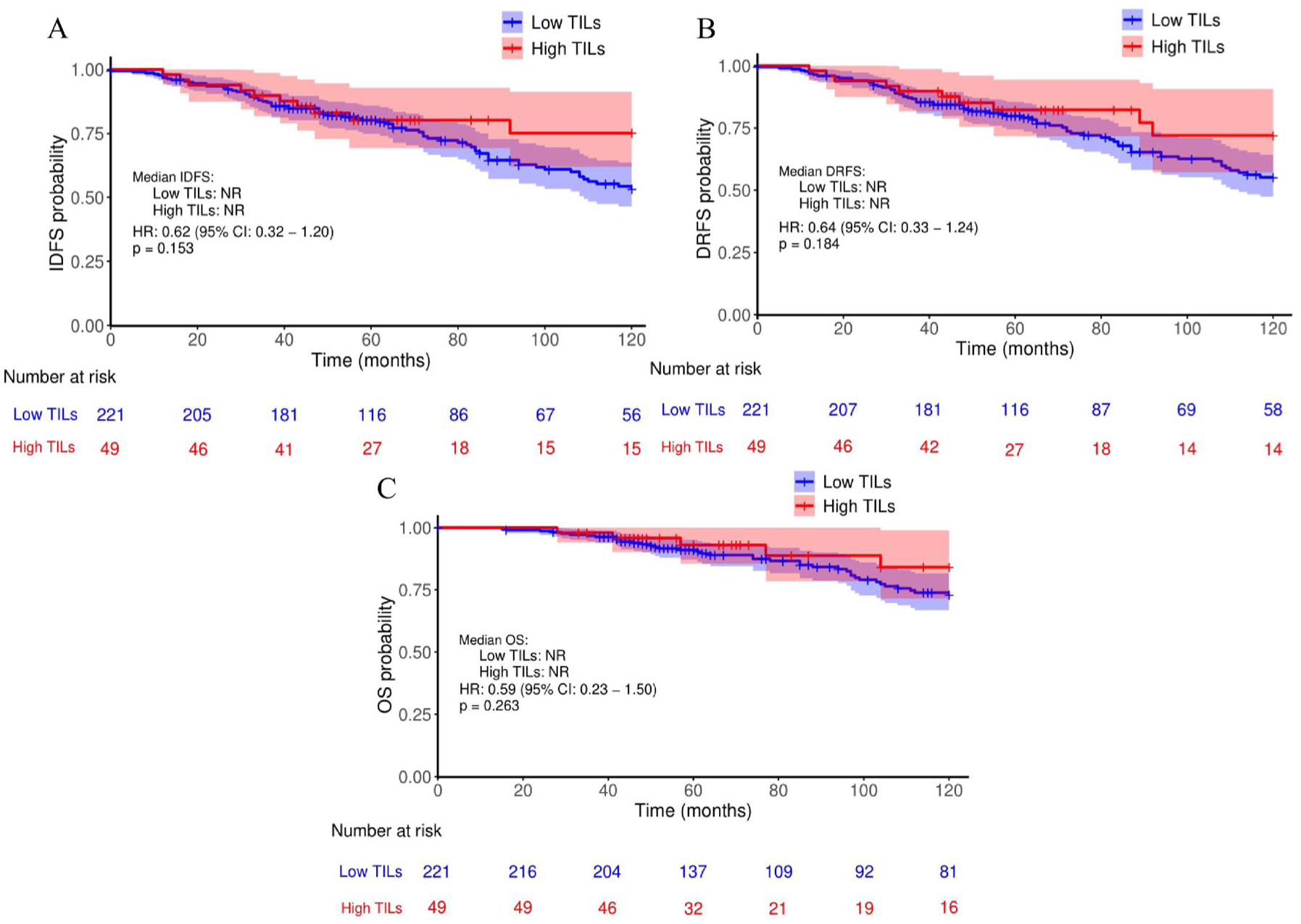
Survival (Kaplan–Meier) as a function of TILs status of patients in Zhejiang Cancer Hospital. Survival (Kaplan–Meier) as a function of TILs status of patients recruited in Zhejiang Cancer Hospital for (a) IDFS, (b) DRFS, and (c) OS of all patients.
HRD and TILs combined stratification defines distinct prognostic subgroups
To clarify the genomic-immune interplay and its prognostic value, we performed a four-layer stratification analysis based on HRD and TILs status in patients from Zhejiang Cancer Hospital with paired data. The four subgroups showed significantly different IDFS, DRFS, and OS probabilities (p < 0.001). Detailed pairwise comparisons of the three survival endpoints among the four subgroups, including the HRs, 95% CIs, and corresponding Log-rank p-values, are summarized in Table S8. The baseline sample size of the HRD+/TILs+ subgroup was only four cases; due to the small sample size, the statistical power for this subgroup is limited, and thus the core prognostic gradient analysis was focused on the remaining three subgroups.
For the three major subgroups with sufficient sample size, the survival probabilities presented a clear hierarchical trend that HRD−/TILs+ subgroup had the highest IDFS, DRFS, and OS probabilities, while HRD+/TILs− subgroup had the lowest survival probabilities across all endpoints, and HRD−/TILs− subgroup exhibited an intermediate prognostic status. The dynamic changes in the number of at-risk patients at each follow-up time point further confirmed the prognostic differences of the combined stratification, with the HRD+/TILs− subgroup showing the most significant reduction (Figure 6).
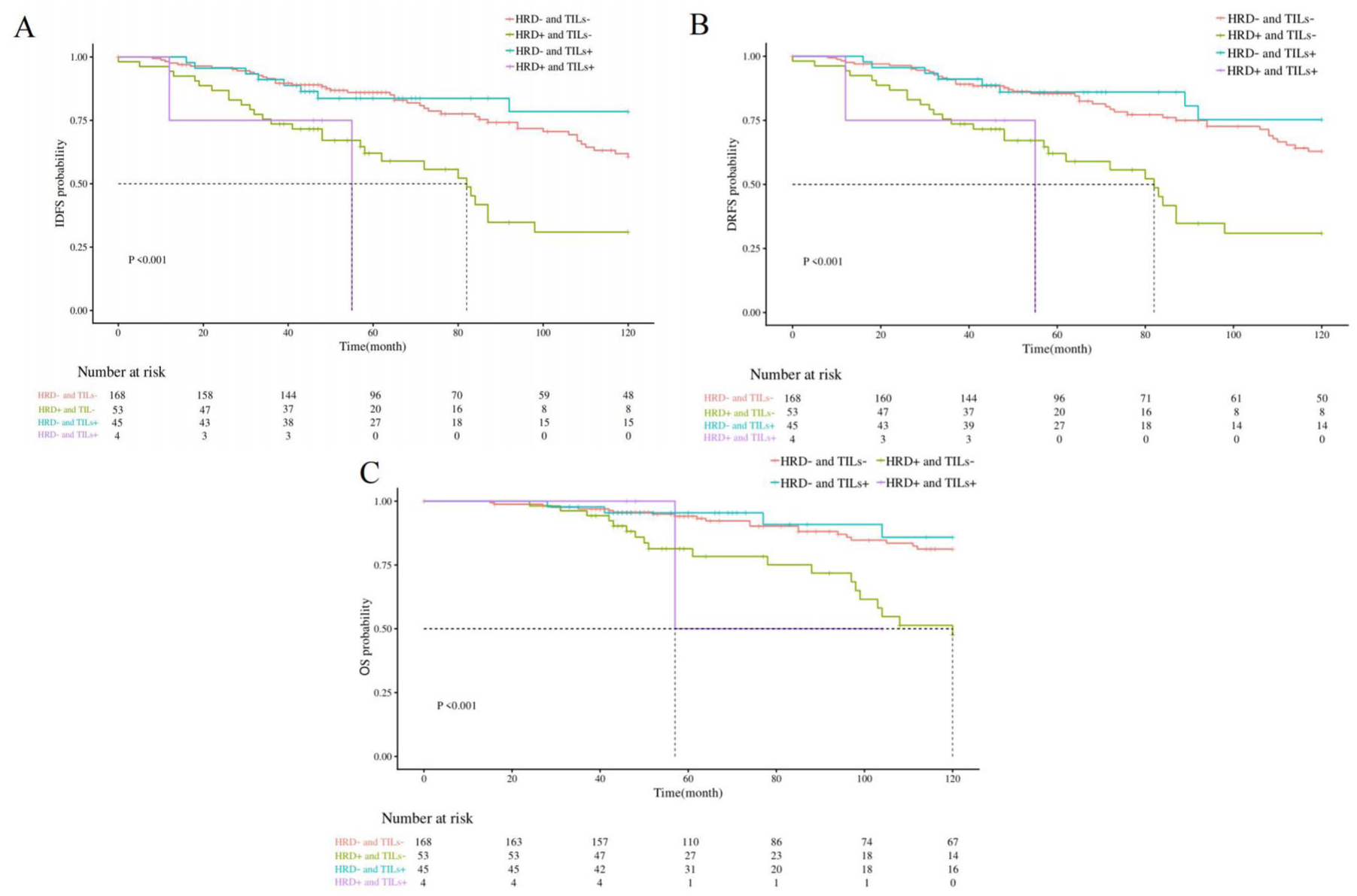
Kaplan–Meier survival analysis of patients with HR+/HER2− breast cancer stratified by combined HRD and TILs status in Zhejiang Cancer Hospital. (a) IDFS, (b) DRFS, and (c) OS were compared among four subgroups: HRD−/TILs−, HRD+/TILs−, HRD−/TILs+, and HRD+/TILs+.
Further pairwise comparison of the two most clinically representative subgroups (HRD+/TILs− vs HRD−/TILs+) revealed statistically significant differences in IDFS, DRFS, and OS (p < 0.001, p < 0.001, p = 0.003), with the HRD−/TILs+ subgroup presenting a markedly superior survival advantage over the HRD+/TILs− subgroup (Table S8).
HRD as an independent prognostic indicator
Univariate Cox regression analysis (Table 2) identified multiple variables associated with unfavorable outcomes. For IDFS, significant predictors included HRD-high status (HR = 2.83, p < 0.01), age at diagnosis <35 years (HR = 3.64, p < 0.01), BMI < 24 (HR = 1.71, p = 0.03), ⩾4 positive lymph nodes (HR = 4.16, p < 0.01), adverse molecular subtype (HR = 2.45, p = 0.04), vascular invasion (HR = 2.20, p < 0.01), PR negativity (HR = 2.25, p < 0.01), mastectomy (HR = 2.80, p = 0.03), axillary lymph node dissection (HR = 2.85, p = 0.04), and lack of endocrine therapy (HR = 3.67, p < 0.01). For DRFS, HRD-high (HR = 2.90, p < 0.01), age <35 (HR = 3.65, p < 0.01), BMI <24 (HR = 1.67, p = 0.03), tumor size >2 cm (HR = 1.95, p = 0.02), ⩾4 positive nodes (HR = 4.06, p < 0.01), vascular invasion (HR = 2.11, p < 0.01), PR negativity (HR = 2.09, p < 0.01), mastectomy (HR = 2.78, p = 0.03), axillary dissection (HR = 3.88, p = 0.02), no endocrine therapy (HR = 3.27, p < 0.01) were associated with poorer prognosis, whereas chemotherapy was associated with a protective effect (HR = 0.45, p = 0.03). For OS, significant predictors included HRD-high (HR = 3.35, p < 0.01), ⩾4 positive nodes (HR = 3.44, p < 0.01), vascular invasion (HR = 2.86, p < 0.01), absence of endocrine therapy (HR = 3.30, p = 0.01), and radiotherapy (HR = 1.88, p = 0.04).
Univariate parameter Cox regression analysis between clinicopathological features and survival-related endpoints.

Bold text indicates HRs that showed significance.
Invasive special carcinoma with good prognosis included tubular, mucinous, papillary, and cribriform carcinoma.
Other types with poor prognosis included micropapillary carcinoma and carcinoma simplex.
AI, aromatase inhibitor; ALND, axillary lymph node dissection; BMI, body mass index; CI, confidence interval; DRFS, distant recurrence-free survival; ER, estrogen receptor; HR, hazard ratio; HRD, homologous recombination deficiency; IDC, invasive ductal carcinoma; IDFS, invasive disease-free survival; ILC, invasive lobular carcinoma; OS, overall survival; PR, progesterone receptor; SLNB, sentinel lymph node biopsy; TAM, tamoxifen; TILs, tumor-infiltrating lymphocytes.
Variables significant in univariate analyses were incorporated into multivariate Cox regression models with all variables adjusted for study site. HRD-high remained an independent predictor of shorter IDFS (HR = 2.03, p < 0.01), DRFS (HR = 2.16, p < 0.01), and OS (HR = 2.15, p < 0.01; Figure 7). Other independent prognostic factors identified in the adjusted multivariate models were as follows: for IDFS, ⩾4 positive lymph nodes predicted poorer prognosis (HR = 2.54, p < 0.01), absence of vascular invasion was associated with better prognosis (HR = 0.63, p = 0.03), and lack of endocrine therapy indicated poor prognosis (HR = 2.92, p < 0.01); for DRFS, ⩾4 positive lymph nodes (HR = 1.99, p < 0.05) and lack of endocrine therapy (HR = 2.57, p < 0.01) both predicted poorer prognosis.
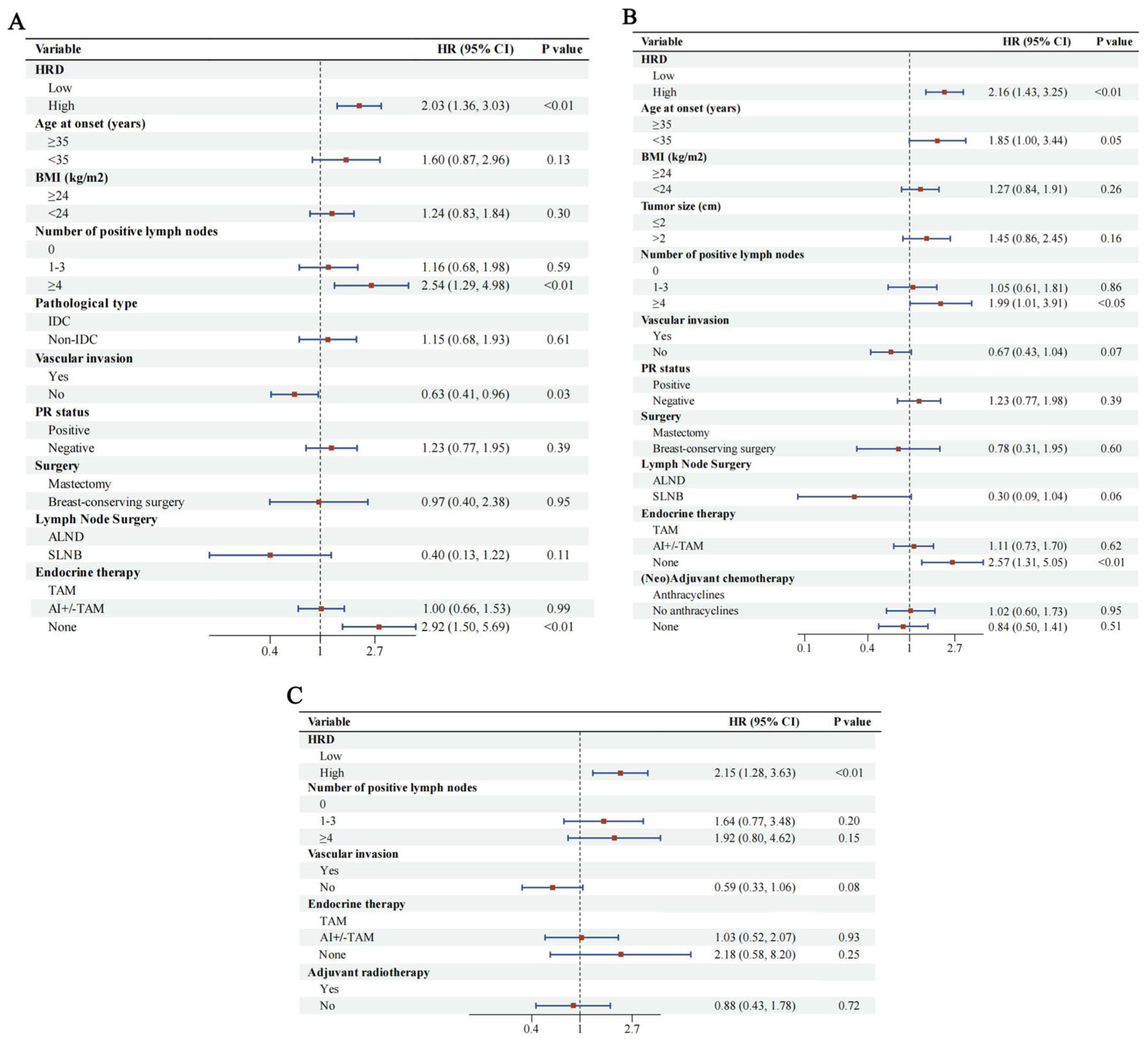
Multiple-parameter Cox regression forest plots. Evaluation of HRD and clinicopathological characteristics using multiple-parameter Cox regression forest plots with HR, 95% CI, and p-values for (a) IDFS, (b) DRFS, and (c) OS.
Sensitivity analysis was further performed using multivariate Cox regression restricted to patients from Zhejiang Cancer Hospital, with the detailed results displayed in Figure S3. Consistent with the total population analysis, HRD-high remained an independent predictor of poorer IDFS, DRFS, and OS in this single-center cohort (p < 0.01). Lack of endocrine therapy also retained its prognostic value for unfavorable IDFS and DRFS in the primary center, while PR negativity was an additional independent factor for poorer IDFS and DRFS. For OS in this cohort, absence of vascular invasion and administration of aromatase inhibitors with or without tamoxifen were identified as protective factors for clinical outcomes, and ⩾4 positive lymph nodes showed a consistent trend for poorer prognosis.
Discussion
Our findings underscore the complex interplay between HRD, TILs, and clinical outcomes in HR+/HER2− breast cancer. The observation that HRD correlates with lower TILs suggests a paradoxical biological relationship in HR+/HER2− breast cancer. While genomic instability could theoretically enhance tumor immunogenicity by generating neoantigens, it may simultaneously foster immunosuppressive mechanisms that dampen anti-tumor responses. Similar patterns have been documented in ovarian cancer, where HRD has been linked to PD-L1 upregulation and increased regulatory T cell infiltration.8,9 In ER+ breast tumors, APOBEC3B-mediated R-loop formation has been implicated in activation of immunosuppressive pathways. 7 Zhang et al. 20 have further described how Treg-driven immune regulation and metabolic reprogramming shape an inhibitory immune microenvironment in breast cancer. We further verified the genomic-immune interplay by conducting a four-layer combined stratification analysis of HRD and TILs, which explicitly evaluated the prognostic value of the composite metric of HRD and TILs for the first time in HR+/HER2− breast cancer. The results showed that the four subgroups defined by HRD and TILs status had highly significant differences in IDFS, DRFS, and OS, but the subgroup analysis revealed that the level of TILs did not allow for stratification of the prognosis based on different HRD statuses (Table S8). HRD remains the dominant and independent prognostic factor regardless of TILs status. To date, most HRD-related research has been concentrated in TNBC. Only a limited number of small-sample studies have focused on HR+ breast cancer: one only reported HRD prevalence without exploring immune correlates, 14 while another identified an association between HRD-S and high TILs in an unselected overall breast cancer cohort, but lacked sufficient sample size for stratified analysis in the HR+/HER2− subgroup. 13 These insights suggest that in HR+/HER2− disease, HRD may be associated with a biphasic immune state consisting of initial activation through neoantigen load followed by adaptive resistance through immune evasion. Preclinical research has noted that PARPi can activate the STING pathway and promote dendritic cell infiltration, with subsequent effects on T cell recruitment in the tumor microenvironment, 21 while ICI monotherapy has been explored in breast cancer models with high TIL infiltration, with its biological effects yet to be fully characterized in HR+/HER2− disease. 19 The ongoing clinical trial NCT06254066 (registered at ClinicalTrials.gov, first posted on 2024-02-12; responsibility retained by Zhejiang Cancer Hospital) is investigating PARPi-ICI combinations in HR+/HER2− breast cancer, a research direction built on ovarian cancer data demonstrating that PARP inhibition can deplete immunosuppressive regulatory T cells and enhance cytotoxic CD8+ T cell activity, thereby remodeling the tumor immune microenvironment. 9
HRD demonstrates an independent prognostic relevance in HR+/HER2− breast cancer, regardless of traditional clinicopathological variables. This is evident from the HR for OS, which decreased from 3.35 in the univariate model (p < 0.01, Table 2) to 2.15 in the multivariate analysis (p < 0.01, Figure 7(c)). This finding is consistent with the chromosomal instability signature of the aggressive SNF3 molecular subtype. 2 The Fudan classification defined SNF3 as an HRD-enriched subtype and recognized SNF2 as a separate immune-enriched subgroup, but did not integrate HRD status with immune characteristics. Our study complements this classification by validating the independent prognostic value of HRD and further linking it to the tumor immune microenvironment in HR+/HER2− breast cancer.
Patients classified as HRD-high experienced significantly shorter survival across all endpoints, including IDFS (HR = 2.36, p < 0.0001, Figure 3(a)), DRFS (HR = 2.48, p < 0.0001, Figure 3(b)), and OS (HR = 2.79, p < 0.0001, Figure 3(c)). This underscores the utility of HRD as a unique biomarker for prognostic stratification. Previous work suggested that HRD-high tumors, due to defective DNA repair capacity, should respond favorably to anthracycline-based chemotherapy, leading to improved outcomes.5,6 Notably, however, our subgroup analysis did not confirm this expectation. Within the HRD-high cohort, survival outcomes did not differ significantly between patients who received anthracycline-based agents and those who did not (HR = 1.32, 95% CI: 0.64–2.73, p = 0.451; Figure S2). A delayed divergence in survival curves was noted: after approximately 85 months, the non-anthracycline-based drug group reached a median OS of 101 months, while the anthracycline-based drug group had not yet reached median survival by 120 months. Although this trend did not achieve statistical significance, it suggests that larger cohorts may be necessary to assess potential late-phase benefits. More critically, within the anthracycline-based drug subgroup, HRD-high status remained strongly associated with worse long-term outcomes (10-year IDFS: HR = 2.94, p < 0.0001; DRFS: HR = 2.83, p < 0.0001; OS: HR = 2.54, p = 0.003; Figure 4), mirroring the overall cohort results. These findings indicate that the adverse prognostic impact of HRD in HR+/HER2− breast cancer is not mitigated by anthracycline treatment, paralleling ovarian cancer observations in which HRD serves as a more powerful predictor of prognosis than chemotherapy exposure. 8 The inability of standard chemotherapy to counteract this effect emphasizes the need to investigate mechanisms of resistance in this subgroup. 22 Supporting this, the TBCRC 030 phase II trial in TNBC reported no correlation between HRD and cisplatin sensitivity, reinforcing the limited predictive value of HRD for anthracycline-based drug efficacy. 23 Consequently, therapeutic strategies specifically targeting HRD biology, such as PARP inhibition, potentially in combination with immunotherapy,24,25 may be more effective, and prospective trials are required to determine whether these approaches can translate the observed delayed survival trends into meaningful clinical improvements for HRD-high patients.
The modest but consistent prognostic trends associated with TILs (Figure 5) are consistent with phase III trials in HR+ breast cancer, which have linked TIL enrichment with improved pCR rates.10,11 These associations likely reflect functional heterogeneity within TIL populations. In TNBC, higher levels of stromal TILs, CD4+, and CD8+ T cells have been associated with better prognosis, higher pCR rates, and longer OS in a cohort of 195 patients. 26 Similarly, in HR+/HER2− disease, a study of 987 patients reported that increased TIL density correlated with improved distant disease-free survival (HR = 0.52, 95% CI: 0.33–0.83, p = 0.006), particularly in tumors with Ki-67 ⩾20% (HR = 0.50, p = 0.01). Interestingly, higher TILs also correlated with adverse pathological features such as high-grade, suggesting that high-risk subsets of HR+/HER2− tumors may paradoxically exhibit greater immunogenicity. This raises the possibility that these patients could be potential candidates for immunotherapeutic approaches. 19 However, it remains unclear which subsets of stromal T cells dominate in this subtype, and their functional roles within the tumor microenvironment are not fully understood. Our findings highlight the need for more refined methodologies, such as multiplex immunohistochemistry or spatial TIL analysis, as recommended by the International Immuno-Oncology Biomarker Working Group, 27 to distinguish TIL subsets and assess whether they represent abortive immune activation or effective cytotoxic responses.
Another important observation is the progressive increase in HRD scores in recurrent lesions, highlighting the value of dynamic monitoring (Figure S1). Circulating tumor DNA-based HRD profiling, which has been shown in ovarian cancer to predict treatment response and track clonal evolution, 28 is now being explored in breast cancer.
Despite these advances, several limitations remain. The HRD threshold employed in our study (⩾6) was cohort-specific and requires external validation. We only enrolled patients with ER expression >10% and did not perform luminal A/B subclassification, both due to the historical limitations of clinical detection criteria and the technical infeasibility of retesting long-stored samples. This precludes the investigation of HRD’s prognostic value in low ER expression subgroups and different luminal subtypes. Moreover, the retrospective nature of the study constrains causal inference. Mechanistic studies should also address pathways such as STING inactivation in HRD-high/TILs-low tumors, a potential driver of immune evasion in breast cancer. 21
Conclusion
In summary, our findings identify HRD as a dual biomarker in HR+/HER2− breast cancer, serving as both a marker of genomic instability and a correlate of immune suppression. The dominant prognostic role of HRD highlights the potential value of genomic profiling for risk stratification in this patient population, while the additive prognostic contribution of TILs within HRD-defined subgroups warrants further validation in larger cohorts. As precision oncology advances, incorporating HRD status and immune metrics such as TILs may provide a framework for future personalized treatment strategies to reduce recurrence risk and improve outcomes in this clinically heterogeneous population.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261456794 – Supplemental material for Homologous recombination deficiency correlates with tumor-infiltrating lymphocytes and predicts patient outcomes in hormone receptor-positive/HER2-negative breast cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359261456794 for Homologous recombination deficiency correlates with tumor-infiltrating lymphocytes and predicts patient outcomes in hormone receptor-positive/HER2-negative breast cancer by Shu-Jie Zhang, Jian-Fei Fu, Cui-Cui Li, Lan Wang, Xin Zhao, Xin-Yu Zhu, Zi-Liang Qian, Wen-Yong Sun, Lin-Feng Zheng, Xiang-Yi Chen, Xiang Lu and Wen-Ming Cao in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261456794 – Supplemental material for Homologous recombination deficiency correlates with tumor-infiltrating lymphocytes and predicts patient outcomes in hormone receptor-positive/HER2-negative breast cancer
Supplemental material, sj-docx-2-tam-10.1177_17588359261456794 for Homologous recombination deficiency correlates with tumor-infiltrating lymphocytes and predicts patient outcomes in hormone receptor-positive/HER2-negative breast cancer by Shu-Jie Zhang, Jian-Fei Fu, Cui-Cui Li, Lan Wang, Xin Zhao, Xin-Yu Zhu, Zi-Liang Qian, Wen-Yong Sun, Lin-Feng Zheng, Xiang-Yi Chen, Xiang Lu and Wen-Ming Cao in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.