
Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of malignant lymphoma in older adults. Treatment in this population remains challenging due to heightened genetic heterogeneity and reduced physiological reserve, which increase susceptibility to both treatment-related toxicity and the risk of undertreatment. Comprehensive geriatric assessment is essential to categorize patients as fit, unfit, or frail, enabling individualized therapeutic strategies. Fit patients benefit from standard R-CHOP or Pola-R-CHP regimens, while unfit patients are suitable for dose-reduced regimens. Anthracycline-containing therapy is recommended when feasible; alternatives such as etoposide or gemcitabine may be used when anthracyclines are contraindicated. Frail patients lack standardized treatment protocols, presenting a significant clinical dilemma; however, advances in geriatric assessment tools and novel therapies are expected to shift the management paradigms from purely palliative care to curative‑intent strategies. Current geriatric assessment tools have limitations, and the distinction between unfit and frail remains fluid. Dynamic fitness assessment and pre-phase treatment strategies may enable some patients to “improve” to a higher fitness level. Emerging evidence supports the efficacy of novel targeted agents, including small-molecule inhibitors, bispecific antibodies, and antibody-drug conjugates, which are reshaping first-line treatment paradigms. Nevertheless, their implementation in community settings faces substantial practical barriers, such as the need for cytokine release syndrome monitoring, caregiver burden, financial toxicity, and adherence challenges. This review provides a comprehensive overview of current strategies and emerging directions for managing older adults with DLBCL.
Plain language summary
Treating diffuse large B-cell lymphoma (DLBCL) in older adults is challenging. Many older patients often have other health issues and lower physical reserves, making it harder to tolerate standard chemotherapy. This review discusses how treatment strategies are evolving to better meet the needs of this population. A key step is tailoring treatment based on a patient’s overall health and fitness level, not just their age. Through a geriatric assessment, doctors can better understand how well a patient may handle treatment, helping to determine whether a more aggressive or a gentler approach is appropriate. We also highlight the growing role of newer targeted therapies, including antibody-drug conjugates and bispecific antibodies. These treatments attack lymphoma cells more precisely while sparing healthy tissues. Challenges remain, such as managing treatment side effects, supporting caregivers, and addressing the high cost of new drugs. Nevertheless, by carefully assessing each patient’s health and matching them with the right treatment, clinicians aim to achieve the best possible lymphoma control while preserving quality of life.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most prevalent subtype of non-Hodgkin lymphoma (NHL), accounting for approximately 20%–50% of adult NHL cases by country. 1 Notably, the incidence of DLBCL increases with age. The median age at diagnosis is 66 years, and roughly 30% of cases occur in people over 75 years. 1 Projections indicate that between 2020 and 2025, the incidence in the United States is expected to rise from 29,108 to 32,443 (an 11% increase), while in Western Europe, it is anticipated to grow from 26,078 to 27,981 (a 7% increase). 2 In Asia, DLBCL accounts for 30%–50% of cases in multiple regions including China, Korea, and Taiwan.3–5 Although incidence remains lower than in the West, emerging data from Korea and Indonesia indicate a rising trend. Driven by an evolving epidemiological landscape and a pronounced global demographic shift toward aging populations, the increasing number of elderly patients with DLBCL represents a demographic that demands urgent attention.
Despite considerable advances in the treatment of DLBCL, the management of older patients continues to present substantial uncertainty and challenges. These individuals often exhibit high‑risk tumor features alongside age‑related functional vulnerabilities, collectively contributing to an unfavorable prognosis. High-risk biological characteristics include frequent extranodal involvement 6 and adverse molecular profiles—such as overexpression of BCL2 and MYC, elevated Ki‑67, high genomic complexity, and a higher incidence of TP53 deletion.7–9 Concurrently, functional vulnerabilities encompass heightened susceptibility to treatment‑related toxicities, diminished bone marrow reserve leading to reduced treatment intensity, altered drug pharmacokinetics, and a greater burden of comorbidities. 10 Notably, many contemporary clinical trials in DLBCL systematically exclude older adults owing to these coexisting complexities. 11 Consequently, therapeutic decision‑making in this population must be highly individualized. Accurately distinguishing between these intersecting risk trajectories is essential for delivering effective and tailored clinical management.
In this review, we summarize the current first‑line treatment approaches for elderly DLBCL patients, highlighting the critical role of geriatric assessment (GA) in pre‑treatment evaluation, the potential of novel regimens, and the challenges and future directions in this field.
Method: Literature review
Literature search and identification
This review is a narrative/semi-systematic synthesis of the literature rather than a formal systematic review. A systematic literature search was designed to capture a broad range of publications focusing on DLBCL in the older adult population. Article selection was based on PubMed/MEDLINE database from January 2012 to November 2025. All clinical trials, cohort studies, and reviews dealing with this subject were selected. Reference lists of critical clinical trials published before 2012 and abstracts from recent major conferences (e.g., ASH, EHA) were manually searched for additional relevant studies.
Search strategy: The following search query was executed to ensure high relevance: (“diffuse large B-cell lymphoma”[Title] OR “DLBCL”[Title]) AND (“aged”[Title/Abstract] OR “older”[Title/Abstract] OR “elderly”[Title/Abstract] OR “geriatric”[Title/Abstract] OR “frail” [Title/Abstract])
Study selection and eligibility
The retrieved records underwent a two-step screening process based on pre-defined selection criteria central to this review.
Initial screening: Titles and abstracts were reviewed to exclude publications irrelevant to the primary focus of GA or first-line treatment strategies for older DLBCL patients.
Full-text assessment: The full texts of potentially relevant articles were then evaluated. Emphasis was placed on selecting studies that provided substantive insights into the following: (i) The application, validation, or prognostic value of GA tools in this patient population. (ii) Evidence regarding the efficacy, tolerability, and optimization of frontline therapeutic regimens. (iii) Clinical practice guidelines and major review articles summarizing the field.
Studies exclusively focused on relapsed/refractory disease or lacking specific data for patients aged⩾60 years were excluded.
Data extraction and thematic synthesis
Relevant data were extracted from the full text of the included studies, including study design, patient demographics, intervention details, including assessment tools and treatment protocols, and primary outcomes (e.g., survival, toxicity, prognostic correlation). The extracted evidence was subsequently synthesized thematically to organize the review.
Levels of evidence
Given the narrative/semi-systematic nature of this review, a formal meta-analysis or GRADE assessment was not feasible. To provide a transparent assessment of the evidence base supporting the key treatment recommendations, we adopted a simplified four-level hierarchy based on study design: (i) Level 1, evidence from phase III randomized controlled trials or meta-analyses; (ii) Level 2, evidence from phase II trials or prospective cohort or elderly-specific studies; (iii) Level 3, evidence from prospective single-arm or large retrospective real-world cohorts; (iv) Level 4, evidence from other retrospective studies, case series, or expert consensus. These levels are used in the section ‘Conclusion’ and Supplemental Table 1 to summarize the strength of evidence for each clinical scenario.
GA tool
GA is a multidimensional tool that assesses prognosis and identifies intervention targets in older adults with cancer who are undergoing chemotherapy. The GA-based fitness assessment is widely recognized as a critical component for personalizing treatment for older cancer patients, including those with DLBCL. 12 Specifically, GA captures an older individual’s overall health status, encompassing domains of functional status, comorbidities, cognition, psychological state, nutritional status, social support, and current medications. 13 Additionally, a comprehensive geriatric assessment (CGA) considers geriatric syndromes such as osteoporosis, delirium, and incontinence, that are indicative of frailty. While CGA is comprehensive, its time-consuming and inconvenient nature in clinical practice has motivated the development of alternative approaches, ranging from abbreviated multidimensional assessments to the selective use of highly simplified items.
The Italian Lymphoma Foundation (FIL) developed a simplified CGA (FIL-CGA) specifically for evaluating fitness in lymphoma patients. 14 It categorizes older patients as fit, unfit, or frail based on age, activities of daily living (ADL), instrumental activities of daily living (IADL), and cumulative illness rating scale for geriatrics scores (Table 1). 15 Validated in prospective trials, the FIL-CGA is a practical tool that reliably identifies fit older DLBCL patients suitable for curative-intent therapy.14,16 Treatment outcomes stratified by FIL-CGA demonstrate a significant advantage of curative-intent therapy among fit patients, with a 2-year overall survival (OS) rate of 88%, compared with 25% in patients receiving palliative care (p < 0.0001). In contrast, no significant survival benefit was observed among unfit (75% vs 45%) or frail patients (44% vs 39%). 14
Criteria for FIL-CGA.

Patients must meet all Fit criteria to be classified as Fit. Meeting any single unfit or frail criterion is sufficient for classification into the respective group.
ADL, activity of daily living; CIRS-G, Cumulative Illness Rating Score for Geriatrics; FIL-CGA, simplified comprehensive geriatric assessment introduced by the Italian Lymphoma Foundation; IADL, instrumental activity of daily living.
Designed as an enhancement to FIL-CGA, the simplified geriatric assessment (sGA) has demonstrated superior accuracy in identifying fit patients eligible for curative-intent therapy and serves as an independent prognostic factor for OS in the Elderly Project study. 17 As shown in Table 2, fit patients are defined as those aged <80 years with preserved ADL and IADL, and without severe comorbidities. These patients are candidates for standard immunochemotherapy with curative intent. Unfit patients include those who are aged ⩾80 years or those who have mild functional impairment or limited comorbidities that do not meet the criteria for frail. These patients may benefit from reduced‑dose anthracycline‑containing regimens (ACRs) or non‑anthracycline alternatives (non-ACRs), while maintaining curative intent. Frail patients are defined as patients with significant functional dependence or severe comorbidities. Treatment goals for this patient population prioritize quality of life, with palliation or clinical trial enrollment as appropriate options.
Criteria for sGA.
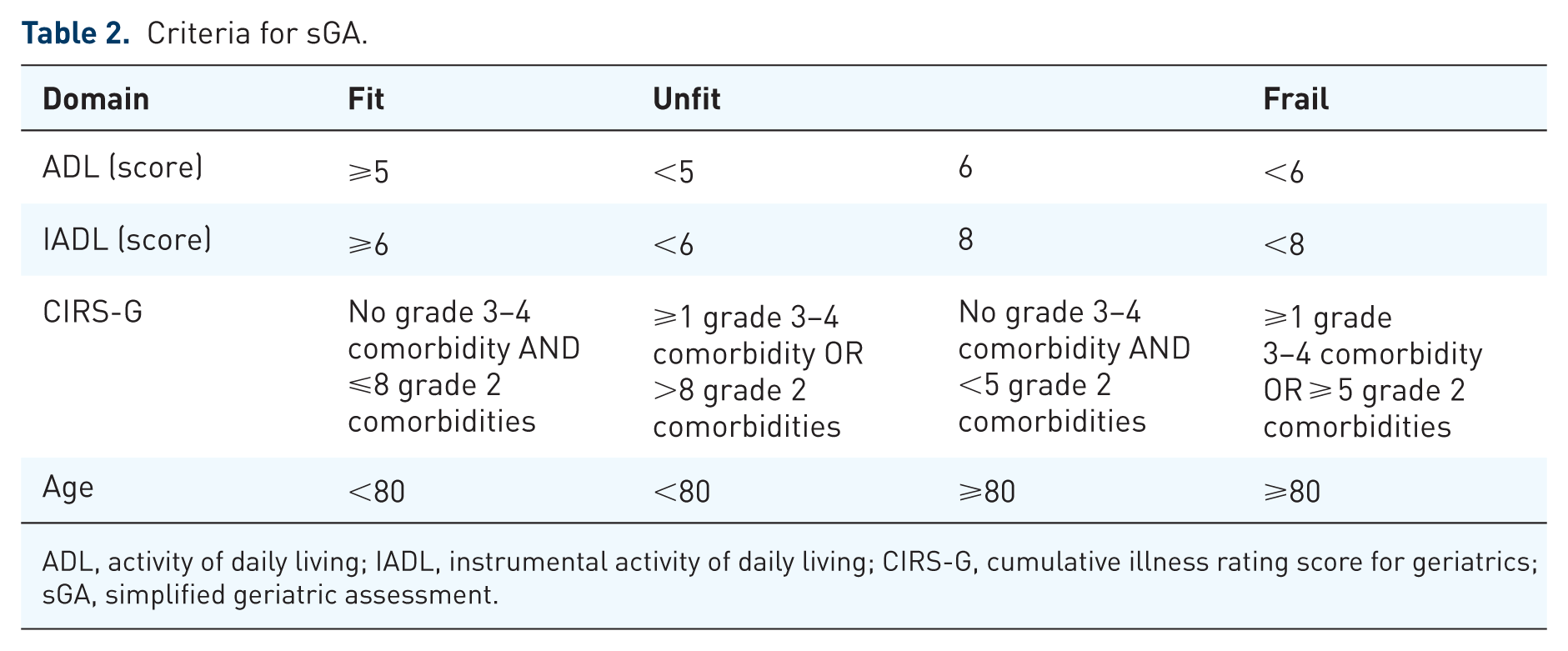
ADL, activity of daily living; IADL, instrumental activity of daily living; CIRS-G, cumulative illness rating score for geriatrics; sGA, simplified geriatric assessment.
By integrating sGA with the International Prognostic Index (IPI) and hemoglobin levels, the Elderly Prognostic Index (EPI) was established as the first prognostic score specifically for older patients with DLBCL, effectively stratifying patients into three risk groups with distinct survival outcomes. 17
Although both sGA and EPI effectively predict OS, their ability to predict progression‑free survival (PFS) has been inconsistent across studies. In the original Elderly Project cohort, sGA and EPI were strongly associated with OS. However, subsequent analyses revealed that sGA failed to demonstrate independent predictive value for PFS, whereas EPI retained significant prognostic value for PFS, particularly in very elderly populations. 18 This discrepancy stems from several key factors. First, sGA captures functional status (ADL, IADL) and comorbidity burden (CIRS‑G), which are strongly associated with non‑lymphoma‑related deaths—a major competing risk in older patients. In the Elderly Project, treatment‑related and non‑lymphoma deaths accounted for over 20% of mortality, diluting the association between sGA and PFS. 17 Conversely, EPI incorporates lymphoma‑specific factors (IPI) and anemia, which more directly influence disease progression, thereby enhancing its predictive value for PFS.
To overcome the limitations of sGA in predicting PFS, a modified model, termed sGA‑A, was developed by incorporating albumin levels into the assessment within a Chinese patient cohort. 19 This adaptation not only improved PFS prediction but also exhibited superior predictive performance for OS and early mortality in this cohort of older patients with DLBCL.
The Society of Lymphoma Treatment in Japan has created a prognostic model called the age, comorbidities, and albumin (ACA) index. This model considers three factors: age ⩾75 years, albumin levels <3.7 g/dL (hypoalbuminemia), and a Charlson comorbidity index (CCI) score ⩾3. The ACA index enables prognostic stratification, predicts both drug tolerance and treatment adherence, and guides personalized therapy selection for elderly patients with DLBCL receiving R-CHOP. 20 The IADL-incoporated ACA (IACA) index, a modified version of the ACA index, predicts both the overall response rate (ORR) and PFS, and shows potential utility in elderly Chinese patients. 21
Other GA tools, including the prognostic model, 22 the Simplified Frailty Score, 23 the Geriatric 8,24,25 the Flemish version of the Triage Risk Screening Tool, 26 the Global Risk Indicator, 27 the Electronic FRAIL score, 28 the Trail score, 29 and the Frailty Assessment, 30 have been developed and investigated for addressing various aspects of diagnosis, prognosis, and treatment planning in older patients with DLBCL. However, all these tools are awaiting validation in larger studies (Table 3).
Geriatric assessment tools for clinical trials.
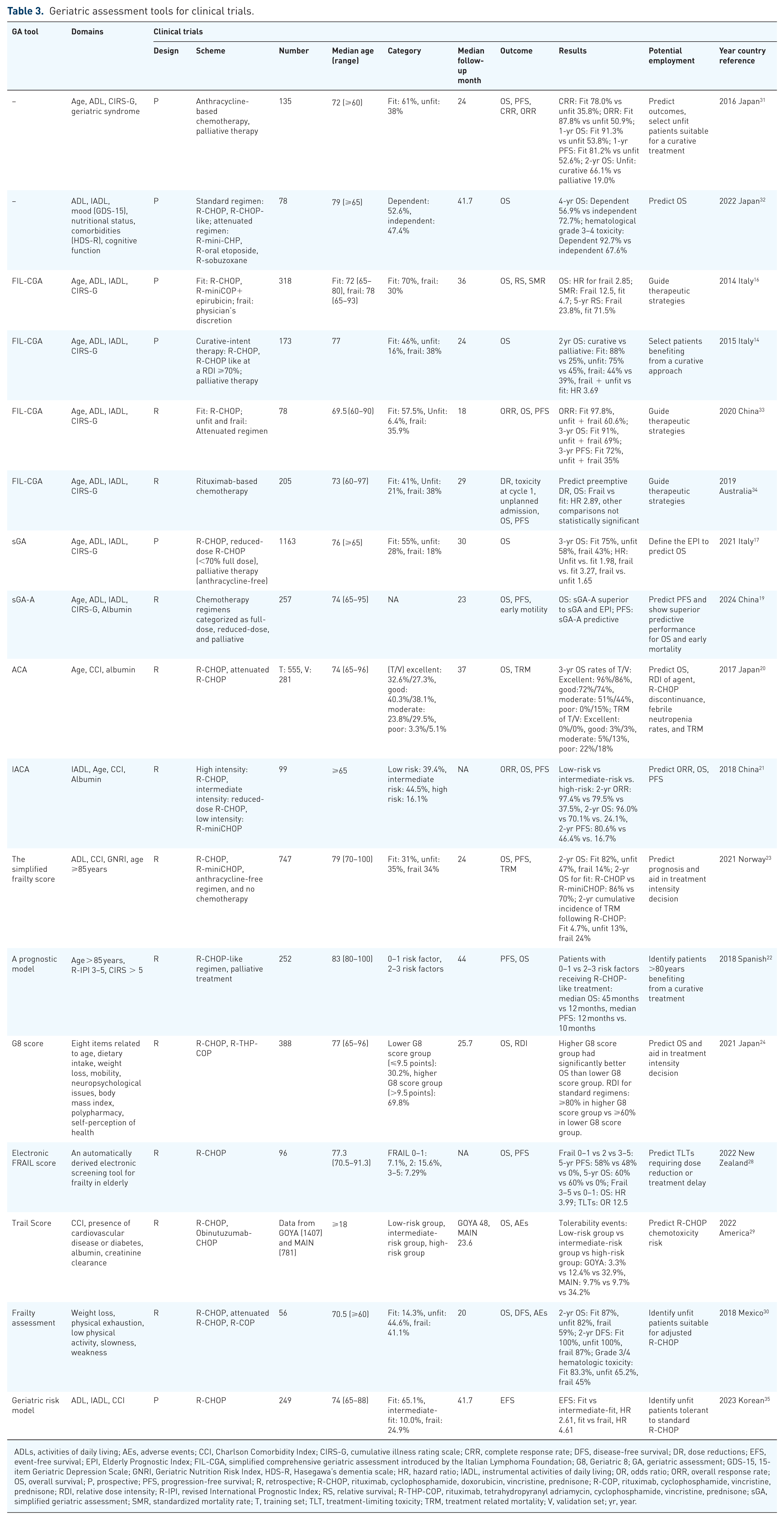
ADLs, activities of daily living; AEs, adverse events; CCI, Charlson Comorbidity Index; CIRS-G, cumulative illness rating scale; CRR, complete response rate; DFS, disease-free survival; DR, dose reductions; EFS, event-free survival; EPI, Elderly Prognostic Index; FIL-CGA, simplified comprehensive geriatric assessment introduced by the Italian Lymphoma Foundation; G8, Geriatric 8; GA, geriatric assessment; GDS-15, 15-item Geriatric Depression Scale; GNRI, Geriatric Nutrition Risk Index, HDS-R, Hasegawa’s dementia scale; HR, hazard ratio; IADL, instrumental activities of daily living; OR, odds ratio; ORR, overall response rate; OS, overall survival; P, prospective; PFS, progression-free survival; R, retrospective; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-COP, rituximab, cyclophosphamide, vincristine, prednisone; RDI, relative dose intensity; R-IPI, revised International Prognostic Index; RS, relative survival; R-THP-COP, rituximab, tetrahydropyranyl adriamycin, cyclophosphamide, vincristine, prednisone; sGA, simplified geriatric assessment; SMR, standardized mortality rate; T, training set; TLT, treatment‑limiting toxicity; TRM, treatment related mortality; V, validation set; yr, year.
In this review, we adopt the sGA criteria to define “fit,” “unfit,” and “frail,” given their prospective validation and widespread acceptance in the field. When discussing individual studies that use different classification criteria, we report the specific definitions used by the original authors to maintain fidelity to the original findings.
First-line treatment: Fit patients
The standard treatment for patients with DLBCL is R-CHOP, a regimen that combines rituximab (an anti-CD20 monoclonal antibody) with CHOP chemotherapy (cyclophosphamide, vincristine, doxorubicin, and prednisone), administered every 21 days for six cycles. 36 The high efficacy of this regimen persists in older populations, with 5-year OS and PFS rates of 58% and 54%, respectively. 37 Fit older patients selected by sGA who receive the standard full-dose R-CHOP achieve long-term survival outcomes comparable to those of younger patients, supporting its use as the standard of care in this population. 14 To further enhance first-line treatment outcomes, several studies have sought to optimize the current approach.
Two large phase III trials showed no significant benefit of R-CHOP14 over R-CHOP21, even in higher-risk patients.38,39 Furthermore, the RICOVER-60 trial demonstrated that extending treatment beyond six cycles of R-CHOP increased toxicity without yielding improved outcomes in elderly patients. 40 A subsequent subgroup analysis in that trial focused on patients aged 61–80 years who achieved complete response (CR) or PR following six cycles. The analysis demonstrated that consolidative radiotherapy significantly improved both PFS and OS among those with bulky disease. 41
A phase III trial conducted in China assessed the substitution of epirubicin for doxorubicin in the R-CHOP regimen for patients aged 60 years or older. While the 2‑year PFS was comparable between the two groups, the use of epirubicin was associated with a lower risk of cardiac dysfunction. R‑COP plus epirubicin (70 mg/m²) may represent a less cardiotoxic alternative to standard R‑CHOP (50 mg/m² doxorubicin) in older patients. 42
In the phase III POLARIX trial, polatuzumab vedotin combined with rituximab, cyclophosphamide, doxorubicin, and prednisone (Pola-R-CHP) demonstrated superior PFS compared with R-CHOP, particularly in the subgroup of patients aged ⩾70 years. 43 In this age group, Pola-R-CHP reduced the risk of progression, relapse, or death by 37% versus R-CHOP, albeit with slightly higher toxicity. A trend toward improved PFS was also observed in patients aged ⩾70 years with an IPI score of 2. 44
Traditionally, an abbreviated course of three to four cycles of R-CHOP, followed by consolidative radiation therapy, has been the preferred approach to mitigate chemotherapy-associated toxicity in patients with limited-stage DLBCL without bulky disease. 45 Similarly, this approach has demonstrated efficacy in older patients with early-stage DLBCL. 46
First-line treatment: Unfit and frail patients
Anthracycline-containing regimens
The standard of care for elderly or medically fragile patients with DLBCL, who are unable to tolerate standard R-CHOP, remains uncertain. However, among older adults for whom curative-intent chemoimmunotherapy is deemed appropriate, relapse rates do not increase with advancing age. 47 The FIL-led Elderly Project demonstrated that patients aged ⩾85 years receiving anthracyclines achieved superior outcomes compared with those receiving palliative care. Reduced-dose anthracyclines are preferred for unfit patients, as their efficacy is comparable to that of full-dose regimens. 18 Consequently, given the compromised health status of this population and the crucial role of anthracyclines in improving cure rates, modified R-CHOP-like regimens are recommended.
For patients older than 80 years without significant comorbidities, a dose-reduced R-miniCHOP regimen is a widely used and effective therapeutic strategy. This regimen has demonstrated favorable survival outcomes and an acceptable toxicity profile, as supported by both prospective and retrospective studies.47–53 Additionally, Peyrade et al. investigated the R-miniCHOP and ofatumumab-miniCHOP regimens, both incorporating an approximate 50% dose reduction in patients aged ⩾80 years.54,55 The latter study, which employed a pre-phase treatment, indicated that this approach was associated with a higher CR rate and reduced risks of early mortality and toxicity compared with historical R-miniCHOP outcomes.
In a prospective, multi-institutional phase II trial enrolling patients with DLBCL aged 70–89 years, a regimen of four R-CHOP cycles followed by rituximab consolidation demonstrated no significant difference in PFS or OS compared with the standard six-cycle R-CHOP regimen. These results indicate that shortening the R-CHOP regimen to four cycles, followed by rituximab consolidation, may represent an effective treatment option for very elderly patients. 56
Pegylated liposomal doxorubicin (PLD) offers a lower risk of cardiotoxicity and enhanced targeted therapeutic efficacy, positioning it as an attractive alternative in DLBCL therapy. Studies have indicated that PLD-containing R-CHOP regimens may improve long-term survival in elderly patients with stage III–IV DLBCL while concurrently mitigating chemotherapy-induced cardiotoxicity. 57 Substituting doxorubicin with non-PLD in the R-CHOP regimen (R-COMP) has also demonstrated similar efficacy while offering an improved safety profile.58,59 R-COMP is recommended as a potentially curative treatment for older patients with intermediate- or high-risk EPI, even in the presence of pre-existing cardiopathy. 60 Recent insights from a FIL cohort study demonstrated that the R-miniCOMP regimen has efficacy comparable to that of the standard R-miniCHOP in sGA-defined unfit and frail older patients with DLBCL. Moreover, older patients classified as intermediate risk by EPI may benefit from the R-miniCOMP regimen. 61 These findings warrant confirmation in larger studies.
Non-anthracycline regimens
For patients with severe cardiac dysfunction (e.g., left ventricular ejection fraction (LVEF) <50%), anthracycline-free regimens are generally recommended. However, in the absence of randomized comparative data, no established standard of care exists for newly diagnosed DLBCL patients ineligible for anthracycline therapy.
Gemcitabine serves as an acceptable substitution for anthracycline in the R-GCVP regimen. A multicenter phase II trial evaluated this regimen in 62 patients with a median age of 76.5 years. Of these, 43.5% had an LVEF of ⩽50%, and the remainder had a borderline ejection fraction and other cardiac risk factors. The regimen achieved a 2-year PFS rate of 49.8% and a 2-year OS rate of 55.8%, grade ⩾3 hematologic toxicities occurred in 34 patients. 62 Gemcitabine-oxaliplatin combined with rituximab (R-GemOx) was evaluated in a single-arm phase II trial in elderly patients with DLBCL. The majority of enrolled patients (77%) were aged over 70 years, and over half had a CCI of 5 or greater. R-GemOx achieved a CR rate of 56% and a 3-year OS rate of 67%. 63
The substitution of doxorubicin by etoposide to form the R-CEOP regimen represents another non-ACR strategy utilized in clinical practice. Studies have shown that R-CEOP achieved 10-year PFS, disease-specific survival, and relative survival rates comparable to those of R-CHOP, despite being linked to inferior OS. 64 The observed difference in OS is likely driven by the higher burden of comorbidities among patients selected to receive R-CEOP, rather than the diminished anti-lymphoma efficacy of the regimen itself. However, prospective studies and subgroup analyses in specifically elderly populations remain scarce, which limits the robustness of the existing evidence.
In the absence of head-to-head trials, the choice between R-CEOP and R-GemOx relies on their distinct evidence profiles. R-GemOx is supported by a prospective single-arm study reporting an ORR of 75% and a favorable 3-year OS, with grade ⩾3 toxicities being primarily hematologic. 63 In contrast, R-CEOP has been evaluated in a large retrospective real-world cohort with extended follow-up, showing 10-year PFS and disease-specific survival comparable to R-CHOP. Although detailed ORR and toxicity data are not available for R-CEOP, the study’s findings are regarded as reliable. Thus, R-GemOx offers prospectively collected efficacy data with manageable hematologic risk, while R-CEOP provides robust long-term outcome evidence from real-world practice. A recent smaller retrospective study suggests that the efficacy of R-CEOP may be significantly associated with cell-of-origin, with notably better outcomes for the germinal center B-cell (GCB) subtype. 65 These results highlight the need for further prospective studies to define the optimal anthracycline-free strategy in this understudied population.
The multicenter phase II B-R-ENDA trial demonstrated that bendamustine plus rituximab is a feasible and effective option for vulnerable older patients with DLBCL who are intolerant of standard CHOP-based therapy. 66 Specifically, patients older than 80 years had 2-year PFS and OS rates of 45% and 46%, respectively. In patients aged 61–80 years with an elevated CIRS score (>6), the corresponding rates were 32% for PFS and 37% for OS.
The all-oral metronomic DEVEC regimen, comprising prednisolone (or deltacortene), vinorelbine, etoposide, cyclophosphamide, and rituximab, offers a convenient option for frail elderly DLBCL patients. In a study of 22 such patients, 21 were classified as frail based on FIL-CGA; the regimen achieved an ORR and a CR rate of 64%, with 2‑year OS and event-free survival rates of 54%. These results support DEVEC as a viable alternative for patients who are unsuitable for curative-intent treatment. 67
Novel approaches
Antibody-drug conjugates
Polatuzumab vedotin
Following the promising efficacy of polatuzumab vedotin in frontline DLBCL therapy as demonstrated in the POLARIX study, preliminary safety data from the ongoing phase III POLAR BEAR trial have been reported for Pola-R-miniCHP in untreated elderly or frail patients with DLBCL. 68 The study enrolled 127 patients who were aged either ⩾80 or 75–80 years with frailty as defined by the FIL-CGA criteria. Compared with standard R-mini-CHOP (NCT04332822), Pola-R-miniCHP demonstrated a manageable toxicity profile with no significant differences in grade 3/4 hematological toxicities, infections, or peripheral neuropathy. However, gastrointestinal adverse events (AEs) occurred more frequently in the Pola-R-miniCHP arm, underscoring the need for careful monitoring in this vulnerable population. The trial is ongoing, with a target enrollment of 300 patients. 68
The chemo-light regimen consisting of polatuzumab, zanubrutinib, and rituximab (Pola-ZR) was evaluated in a prospective trial (NCT06203652) enrolling untreated elderly patients with DLBCL aged ⩾70 years or 60–69 years with an ECOG performance status of 2–4. With a median follow-up of 10.2 months among the first 24 patients, the regimen yielded a CR rate and an ORR both of 83%, along with a favorable safety profile. 69
Brentuximab vedotin
A pilot study evaluated brentuximab vedotin (BV) combined with rituximab and dose-attenuated CHP (BV-R-miniCHP) in 22 patients aged >75 years with newly diagnosed DLBCL. Among these patients, 77% completed the full course of six cycles. The regimen achieved an ORR of 80% (8/10) in CD30‑positive patients and 91% (10/11) in CD30‑negative patients. The corresponding CR rates were 70% (7/10) and 64% (7/11), respectively. Given its manageable toxicity profile, BV-R-miniCHP represents a promising option for elderly patients and warrants further investigation. 70
Bispecific antibodies
Bispecific anti-CD20xCD3 monoclonal antibodies, which have demonstrated efficacy in relapsed or refractory DLBCL,71,72 are now being explored as a first-line treatment for elderly or unfit patients. In a phase I/II trial (NCT03677154), mosunetuzumab monotherapy was assessed in untreated, unfit DLBCL patients (defined as age ⩾80 years, or age 60–79 years with functional impairments or organ dysfunction precluding full‑dose chemotherapy). Despite a high‑risk baseline profile—56% with stage III–IV disease and 81% with an IPI score ⩾2—the regimen achieved an ORR of 58% and a CR rate of 42%, with a favorable safety profile. The 1‑year PFS rate was 39%. 73
A phase II trial (EudraCT Number: 2022-003398-51) is investigating the chemo-light combination of glofitamab, rituximab, and polatuzumab vedotin (R-Pola-Glo) for newly diagnosed older adults with DLBCL who are ineligible for full-dose R-CHOP-like regimens. 74 Notably, 70% of enrolled patients have a high‑intermediate or high‑risk IPI, underscoring the high‑risk nature of this cohort. Preliminary safety data appear favorable. 74
Two recent trials evaluated epcoritamab‑based regimens in older patients with DLBCL. The phase II trial (NCT05660967) of epcoritamab monotherapy enrolled older (⩾75 years), anthracycline-ineligible patients, of whom over half had stage IV disease and an IPI score ⩾3. The trial reported an ORR of 74% (29/39), and a CR rate of 64% (25/39). Treatment-related AEs occurred in 20% of patients, with cytokine release syndrome (CRS) as the most common (68%). CRS events were primarily low-grade and resolved in 97% of affected patients. 75 Another phase Ib/II trial (NCT04663347) evaluated epcoritamab plus R-miniCHOP as a first-line therapy for vulnerable older adults with DLBCL. The enrolled cohort (n = 28) had a median age of 81 years and a high prevalence of cardiac comorbidities. Most patients exhibited high-risk features: 68% presented with an IPI score of 3–5, 54% with stage IV disease, and 39% with bulky disease (⩾ 7 cm). After a median follow-up of 16.8 months, the regimen achieved an ORR of 89% and a CR rate of 82%. The estimated 12-month PFS and OS rates were 88% and 96%, respectively. Treatment-related CRS occurred in 45% of patients and resolved in all cases except one. 76
Small-molecule targeted drugs and immune modulators
Most trials that combined R-CHOP with targeted agents did not meet their primary endpoints in phase III studies, although some showed promise in specific subgroups or in early-phase trials (Table 4). For instance, the PHOENIX trial found that the addition of ibrutinib improved survival in younger patients but increased toxicity in older individuals. This heightened toxicity compromised the delivery of R-CHOP, leading to inferior outcomes in the older population. 77
Novel agents as first-line therapy for older patients with DLBCL.

ABC, activated B-cell-like; BTKi, bruton tyrosine kinase inhibitor; BV R-miniCHP, brentuximab vedotin, attenuated cyclophosphamide, doxorubicin, vincristine and prednisone; CGA, comprehensive geriatric assessment; CI, confidence interval; CIRS-G, Chronic Illness Rating Scale- Geriatric; CRR, complete response rate; CRS, cytokine release syndrome; DEL, double-expressor lymphoma; G8, Geriatric 8; GA, geriatric assessment; GCB, germinal center B-cell; HR, hazard ratio; IADL, instrumental activities of daily living; ICANS, immune effector cell-associated neurotoxicity syndrome; IPI, International Prognostic Index; IR2, ibrutinib, rituximab, lenalidomide; MHG, molecular high-grade; MNA, mini-nutritional assessment; NA, not available; ORR, overall response rate; OS, overall survival; PFS, progression free survival; Pola-ZR, polatuzumab, zanubrutinib, and rituximab; R2, rituximab and lenalidomide; R2-CHOP, lenalidomide, rituximab, cyclophosphamide, vincristine, doxorubicin, prednisone; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; RIT, radiation radioimmunotherapy; sGA, simplified geriatric assessment; 90Y-IT, 90Y-ibritumomab tiuxetan; yr, year; ZR2, zanubrutinib, rituximab, lenalidomide.
The phase III REMoDL-B trial evaluated the efficacy of adding the proteasome inhibitor bortezomib to R-CHOP (RB-CHOP) in patients with untreated DLBCL, including elderly patients eligible for full-dose chemotherapy. While no benefit was observed in the overall population, significant clinical improvement was demonstrated among patients with the activated B-cell-like (ABC) subtype or the molecular high-grade DLBCL. 81 In the ABC subgroup, the 5-year OS increased from 67% with R-CHOP to 80% with RB-CHOP (HR, 0.58; 95% CI, 0.35–0.95; p = 0.032). In patients with molecular high‑grade lymphomas, the 5-year PFS increased from 29% with R-CHOP to 55% with RB-CHOP (HR, 0.46; 95% CI, 0.26–0.84). Although an analysis in the older subgroup was not performed, the favorable tolerability of RB-CHOP and the high‑risk profile of older patients suggest that they may still derive clinical benefit.
The randomized phase III ROBUST study demonstrated that lenalidomide plus R-CHOP (R2-CHOP) did not improve survival in the overall population of patients with ABC-type DLBCL or in the elderly subgroup. However, R2-CHOP showed a favorable trend in PFS among patients with an IPI score ⩾3. 79
Several studies have explored chemo‑free approaches as a potential treatment strategy for frail older patients with DLBCL. The FIL-ReRi study, a two‑stage single‑arm trial, assessed the efficacy of rituximab plus lenalidomide (R2) in untreated, frail patients with DLBCL aged ⩾ 70 years (according to CGA). The R2 doublet showed only modest activity, with an ORR of 50.8%, a CR rate of 27.7%, and 2-year PFS and OS rates of 40.5% and 48.2%, respectively. 84
The triplet regimen comprising rituximab, lenalidomide, and a BTKi demonstrated high activity in patients with DLBCL. In newly diagnosed, unfit or frail patients aged ⩾ 75 years (as defined by FIL‑CGA), the combination of ibrutinib, rituximab, and lenalidomide (IR2) yielded an ORR of 66.7% and a CR rate of 56.7%. 85 With a median follow-up of 27.6 months, the 2-year PFS and OS rates were 53.3% and 66.7%, respectively. These encouraging results suggest that the chemo-free strategy may offer comparable efficacy to R-miniCHOP, supporting the rationale for a comparative phase III trial (NCT05179733).
The SMART-START trial demonstrated that the SMART (rituximab, lenalidomide, and a BTKi) regimen is an effective and safe treatment option for untreated older patients with DLBCL. Furthermore, the SMART-START regimen can be administered to patients unfit for intensive chemotherapy at diagnosis, typically as an initial two to three cycles of SMART alone followed by the addition of chemotherapy. The 1-year PFS rates were encouraging in the SMART and SMART-START groups, at 81% and 84%, respectively. 86 In addition, a single-center prospective study found that zanubrutinib combined with rituximab and lenalidomide (ZR2) provided comparable efficacy and improved safety compared with an R-CHOP-like regimen in newly diagnosed elderly patients with DLBCL. 87 Notably, MYD88 and CD79b mutations, which are characteristic of the MCD subtype, predicted a favorable response to ZR2, whereas the CARD11 mutation was associated with ZR2 resistance in this study.
Initial findings from the phase II CAVALLI trial showed promise for combining venetoclax with R-CHOP as first-line therapy for DLBCL. 90 Compared with the GOYA study, 91 the addition of venetoclax to the standard regimen showed a trend toward improved PFS and OS, particularly in high-risk patients with Bcl-2 positivity by immunohistochemistry. However, the CAVALLI trial also reported higher rates of grade 3 and 4 AEs. The median age of the patient cohort was 65 years (range, 18–85 years), but the older patient subgroup was not analyzed.
Selinexor, a selective inhibitor of exportin 1, has been approved for the treatment of DLBCL based on its demonstrated efficacy and acceptable safety profile. 92 However, its use in elderly patients remains under-investigated. A retrospective analysis of 16 elderly patients with DLBCL treated with first-line selinexor-based regimens reported an ORR of 93.8% and a CR rate of 81.3%, with a manageable toxicity profile. Notably, all five patients receiving chemotherapy-free regimens in this cohort achieved CR. Updated data from this analysis revealed a 1-year PFS rate of 79.6%. 93
Epigenetic agents
Histone deacetylase inhibitors are potent anti-lymphoma agents that exhibit synergistic activity with rituximab. 94 In a phase II trial, the addition of tucidinostat to R-CHOP improved 2-year PFS and OS in elderly patients with newly diagnosed DLBCL and appeared to mitigate the poor prognosis associated with CREBBP/EP300 mutations in double‑expressor lymphoma. 82 A recent real-world study further reported that the combination of chidamide and R-CHOP improved survival in newly diagnosed double-expressor DLBCL. Subgroup analysis indicated that patients aged >60 years achieved a 5-year OS rate comparable to that of younger patients, despite having inferior 5-year PFS. 83
Given elevated tumor methylation in older patients, the oral hypomethylating agent azacitidine is under investigation as a therapeutic option for specific DLBCL subgroups. An ongoing randomized phase II/III trial (S1918) is evaluating R-miniCHOP combined with azacitidine versus R-miniCHOP alone in untreated patients with DLBCL aged ⩾75 years. 95 This prospective study integrates baseline GA and circulating tumor DNA analysis, and has the potential to refine standard care for elderly patients based on molecular biomarkers.
EZH2, a histone methyltransferase and the catalytic subunit of PRC2, is mutated in approximately 25% of DLBCL cases. The EpiRCHOP trial (NCT02889523) assessed the efficacy of adding the EZH2 inhibitor tazemetostat to R‑CHOP in elderly patients with previously untreated, high‑risk (age‑adjusted IPI 2–3) DLBCL. In the phase Ib segment, R-CHOP plus tazemetostat was well tolerated, with an acceptable safety profile. 96 The phase II segment demonstrated estimated 18-month PFS and OS rates of 77.7% and 88.8%, respectively. 88
Other strategies
Radioimmunotherapy with 90Y-ibritumomab tiuxetan (90Y-IT) delivers targeted radiation to exert a cytotoxic effect. This conjugate consists of the anti-CD20 antibody ibritumomab linked to the chelator tiuxetan and radiolabeled with 90Y. 97 In a multicenter phase II trial, 55 elderly patients with DLBCL received four cycles of R-CHOP followed by one course of 90Y-IT, achieving an ORR of 80%. At a median follow‑up of 7.9 years, the OS rate was 38.9%, suggesting favorable efficacy and safety, particularly for patients ineligible for full-dose chemotherapy. 89
The phase II VERLen trial (NCT04974216) assessed tafasitamab (an anti-CD19 antibody), lenalidomide, and rituximab in untreated patients with DLBCL aged older than 80 years. 98 After a median follow-up of 16 months, the 1-year PFS and OS rates were estimated to be 52% and 82%, respectively. However, the study was terminated early due to a high incidence of serious AEs, including grade 3/4 neutropenia (44%) and infections (29%).
A schematic overview of the major novel agent classes and their targets is provided in Supplemental Figure 1.
Logistical challenges of novel immunotherapies for older patients in community practice
Although novel immunotherapies, such as bispecific antibodies (BsAbs), antibody-drug conjugates (ADCs), and oral targeted agents, have expanded treatment options for older patients with DLBCL, their implementation in real-world community practice faces substantial practical and logistical challenges that warrant thorough evaluation.
Toxicity monitoring and management challenges
BsAbs such as epcoritamab and glofitamab require intensive monitoring for CRS and immune effector cell-associated neurotoxicity syndrome (ICANS). The EPCORE NHL-2 trial enrolled elderly patients with a median age of 81 years. The incidence of CRS was 61%. The majority of CRS events were low-grade. Tocilizumab was required in 29% of patients, and corticosteroids were used in 14%. Neither ICANS nor tumor lysis syndrome was observed. 76 Although CRS is generally manageable, its high incidence poses significant challenges for older patients. This is particularly true for those with limited social support. Furthermore, BsAbs-induced immunosuppression, combined with age-related immunosenescence, increases the risk of severe infections, including cytomegalovirus and Pneumocystis jirovecii pneumonia. These challenges are amplified in community settings, where access to multidisciplinary care and intensive care is often limited.
Logistics and medication management challenges
Novel immunotherapies pose distinct logistical challenges. Regimens such as epcoritamab require weekly administration during initial cycles, which imposes a substantial travel burden on patients with limited mobility and their caregivers. 99 Polypharmacy further complicates management. Elderly patients commonly take multiple medications, such as antihypertensives, anticoagulants, and hypoglycemic agents, which may interact with immunotherapies. Corticosteroids used for CRS prophylaxis can compromise glycemic control, while tocilizumab interferes with CYP450 enzymes, affecting the metabolism of drugs such as warfarin.100,101 These interactions demand meticulous medication reconciliation and coordination among oncologists, primary care physicians, and pharmacists—a particular challenge in fragmented community healthcare systems.
Financial toxicity and adherence challenges
Oral targeted regimens like IR2 present unique adherence challenges. Although this combination has shown encouraging results in unfit or frail patients, it requires long-term adherence to multiple oral agents in a population already coping with high pill burdens for comorbid conditions. 85 Ibrutinib-associated toxicities—atrial fibrillation, bleeding, diarrhea—may be poorly tolerated, leading to dose reductions or discontinuation. 102 Furthermore, the financial toxicity of long-term oral therapy, driven by insurance co-pays and coverage gaps for novel agents, can disproportionately impact older patients and compromise adherence.
Conclusion and future direction
Managing older patients with DLBCL is challenging due to significant heterogeneity within this population. Unfavorable biological characteristics, reduced treatment intensity, comorbidities, declining organ function, and impaired chemotherapy metabolism collectively contribute to inferior survival outcomes and an increased risk of toxicity. Although most patients are candidates for curative-intent therapy, treatment decisions should not be based solely on age. A comprehensive pretreatment evaluation is essential to identify candidates suitable for standard R-CHOP or adapted regimens. Figure 1 illustrates a proposed treatment framework for older patients with DLBCL receiving first-line therapy.

The authors’ preferred first-line management for older patients with DLBCL.
Current curative-intent strategies for older patients with DLBCL are guided by GA stratification, with practical tools such as the FIL-CGA and sGA widely adopted. The EPI score is the first prognostic tool developed for this population, while the ACA and IACA indices provide simple, effective stratification for risk‑oriented R‑CHOP dose adjustment in elderly patients. Notably, frailty affects nearly half of the patients and is associated with reduced survival and greater toxicity. 35 However, a subset of frail patients may still achieve meaningful survival outcomes with curative-intent therapy, highlighting the urgent need for more refined predictive tools. 103
The limitations of current GA tools are increasingly recognized. Key domains such as nutritional status and social support—factors of growing critical importance in the era of novel immunotherapies (e.g., BsAbs)—are not captured by the sGA. Malnutrition or inadequate social support may thus render patients ineligible for curative-intent options, underscoring the need for more comprehensive frameworks.
Dynamic fitness assessment is increasingly critical, especially in the era of novel agents. Following pre-phase therapy with steroids or vincristine, and targeted interventions, disease-related confounding factors can be unmasked, and initial frailty status may become modifiable. Serial assessments at different time points facilitate more informed clinical decision-making. The SMART-START approach exemplifies this paradigm: administering targeted agents prior to chemotherapy enables some unfit patients to achieve sufficient functional improvement to subsequently tolerate curative-intent regimens. 86 This strategy allows a subset of patients to “improve” from unfit to fit, or from frail to unfit, expanding access to potentially curative therapies while minimizing initial toxicity. Although prospective data on dynamic GA in lymphoma remain limited, ongoing trials (NCT06156774) have demonstrated the role of reassessing frailty status in enhancing treatment efficacy in patients with multiple myeloma. 104 Future efforts should prioritize refining GA tools to incorporate nutrition and social support, developing structured pre-phase treatment programs, and validating dynamic GA-guided treatment algorithms to optimize outcomes in older populations.
Treatment stratification based on sGA is currently a widely accepted practice (Supplemental Table 1). For fit patients, the standard immunochemotherapy regimen R-CHOP remains the cornerstone of treatment (level 1 evidence), supported by multiple phase III randomized controlled trials. Pola-R-CHP, a newer regimen that demonstrated improved outcomes in the phase III POLARIX trial, represents an emerging option (level 1 evidence), especially for patients aged ⩾70 years. For unfit patients, reduced‑dose ACRs (e.g., R‑miniCHOP, R‑COMP) serve as appropriate alternatives (level 2 evidence), supported primarily by phase II studies and prospective elderly cohorts. For patients with cardiac comorbidities or anthracycline intolerance, non‑ACRs such as R‑GCVP, R‑GemOX, or R-CEOP may be utilized (level 2–3 evidence), supported by a multicenter phase II trial, a prospective single-arm study, and a large retrospective real-world cohort, respectively. Although the evidence supporting these approaches is less robust than for anthracycline-containing regimens, treatment decisions rely heavily on individualized clinical assessment.
Frail patients, however, represent a distinct clinical challenge in the absence of standardized treatment protocols. Notably, the therapeutic paradigm is evolving from palliation toward curative-intent strategies. This shift is supported by refined GA tools and novel, low-toxicity regimens, including attenuated chemotherapy and innovative drug combinations.
Prospective studies have demonstrated that a regimen combining rituximab, lenalidomide, and a BTKi provides non-inferior efficacy relative to traditional R-CHOP in older populations, along with improved tolerability. 87 ADCs such as polatuzumab vedotin have also shown promise. In patients aged >80 years or those with frailty, the ongoing phase III trial evaluating Pola-R-miniCHP demonstrates a safety profile similar to that of R-miniCHOP, whereas efficacy outcomes await further follow-up. The chemo-light Pola-ZR regimen has achieved favorable response rates in prospective studies. Other novel agents, including BsAbs (e.g., mosunetuzumab, epcoritamab, glofitamab), have shown high response rates with manageable safety profiles, suggesting their potential as a therapeutic option for higher‑risk or frail patients with DLBCL. However, these promising data are derived from first‑line phase II/Ib studies of highly selected patients with short follow‑up periods, warranting cautious interpretation. Despite these limitations, the findings underscore the potential of these agents in future clinical practice.
Against this backdrop of novel agents, parallel efforts are exploring precision treatment strategies guided by clinical and molecular biological characteristics. Subgroup analysis of the POLARIX study revealed that patients aged over 60 years with ABC DLBCL and an IPI score of 3–5 derived the greatest benefit. 43 The non-GCB subtype derived significant benefit from the ZR2 regimen, whereas patients with gastrointestinal DLBCL appeared to benefit more from conventional R-CHOP. 87 Patients harboring MYD88 and CD79b mutations exhibit favorable responses to ZR2, while CARD11 mutations are associated with resistance. 87 Additionally, adding tucidinostat to R-CHOP improved outcomes in patients with CREBBP/EP300 mutations in double‑expressor DLBCL, 82 while adding bortezomib to R-CHOP enhanced efficacy in ABC-type or molecularly defined high-grade lymphoma. 105 The continued refinement of genetic subtyping (e.g., MCD, BN2, EZB) is increasingly informing treatment selection, enabling biologically rational approaches even in older populations. 106 Collectively, these advances are expanding the therapeutic landscape and paving the way for more precise treatment strategies in older patients with DLBCL.
Future efforts should focus on integrating GA with tumor biology to optimize treatment selection in this heterogeneous population. The prospective trial SWOG 1918, which incorporates both GA and biomarkers, is evaluating this integrated paradigm. 95 Furthermore, addressing practical considerations, including facilitating remote monitoring technologies, strengthening logistical supportive care, and optimizing healthcare systems in community settings, will be essential to maximize the benefits of novel immunotherapies in the growing number of older patients with DLBCL.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261457855 – Supplemental material for Management of diffuse large B∑cell lymphoma in older adults: current strategies and emerging directions
Supplemental material, sj-docx-1-tam-10.1177_17588359261457855 for Management of diffuse large B∑cell lymphoma in older adults: current strategies and emerging directions by Jie Zhang, Yaping Zhang, Yongning Jiang, Jianyong Li and Wenyu Shi in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-2-tam-10.1177_17588359261457855 – Supplemental material for Management of diffuse large B∑cell lymphoma in older adults: current strategies and emerging directions
Supplemental material, sj-pdf-2-tam-10.1177_17588359261457855 for Management of diffuse large B∑cell lymphoma in older adults: current strategies and emerging directions by Jie Zhang, Yaping Zhang, Yongning Jiang, Jianyong Li and Wenyu Shi in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank Cindy Zhu, Department of Psychology, University of California, Los Angeles (UCLA), Los Angeles, CA, USA, for reviewing and editing the English language of this manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.