
Abstract
Background:
Immunotherapy has demonstrated limited efficacy in epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC), often due to an immunosuppressive tumor microenvironment (TME). The clinical significance of the CD39-adenosine pathway in this refractory setting remains unclear.
Objective:
To explore the role of the CD39-adenosine pathway, especially CD39, in EGFR-mutant (EGFR-Mu) NSCLC patients who received immunotherapy as a second or later-line treatment.
Design:
In this retrospective study, clinical characteristics, treatment regimens, and efficacy endpoints (progression-free survival (PFS) and objective response rate (ORR)) were collected. We analyzed the correlation between CD39 expression, CD39+CD8+ T cell infiltration, and clinical outcomes.
Methods:
We retrospectively evaluated EGFR-Mu NSCLC patients receiving later-line immune checkpoint inhibitors (ICIs) at Jinling Hospital, alongside The Cancer Genome Altas (TCGA) cohort data. TME phenotyping (CD39, CD73, ADORA1, and CD39+CD8+/PD-1+CD8+ T cell infiltration) was performed using immunohistochemistry and immunofluorescence. Patients were divided into a response group and a non-response group according to the Tumor Efficacy Assessment Criteria (RECIST 1.1). Univariate and multivariate Cox regression analyses were used to explore the factors influencing the survival of EGFR-Mu patients who received ICIs in the second line or later lines.
Results:
Database and clinical samples analyses revealed that expression of CD39 and CD73 was significantly increased in EGFR-Mu NSCLC samples compared to EGFR wild-type (EGFR-WT). However, Immunofluorescence (IF) results showed that the infiltration rate of CD39+CD8+ T cells was significantly lower in EGFR-Mu patients than in EGFR-WT patients. Notably, low overall CD39 expression and high CD39+CD8+ T cell infiltration within the TME were correlated with favorable immunotherapy responses. Among the 19 EGFR-Mu patients receiving ICIs, the overall ORR was 10.5%, and the median PFS for EGFR-Mu patients was 4.53 months. Multivariate Cox regression analysis found brain metastasis as an independent risk factor, while the infiltration of CD39+CD8+ T cells and PD-1+CD8+ T cells independently correlated with prolonged PFS.
Conclusion:
Our exploratory findings suggest that CD39+CD8+ T cell infiltration may serve as a putative biomarker associated with immunotherapy response in EGFR-mutant NSCLC. Evaluating the CD39-adenosine pathway within the TME could inform future personalized treatment strategies, warranting further validation in larger, prospective cohorts.
Plain language summary
Why was this study done? Immunotherapy often fails against EGFR-mutated lung cancer due to immune suppression. We investigated whether a specific group of immune cells (CD39+ CD8+ T cells) could indicate which patients might still benefit from treatment. What did the researchers do? We analyzed tumor samples and clinical records from EGFR-mutated lung cancer patients treated with immunotherapy, alongside data from a public database. we quantified the amount of CD39+ CD8+ T cells in EGFR-mutated lung tumors and compared these counts with patient responses to immunotherapy. What did the researchers find? Patients with a high density of CD39+ CD8+ T cells in their tumors showed much better responses to immunotherapy and experienced significantly longer PFS. What do these findings mean? Our exploratory findings suggest that CD39+CD8+ T cell infiltration may serve as a putative biomarker associated with immunotherapy response in EGFR-mutant NSCLC. Evaluating the CD39-adenosine pathway within the TME could inform future personalized treatment strategies.
Keywords
Introduction
Lung cancer is the leading cause of cancer mortality globally. 1 Non-small cell lung cancer (NSCLC) accounts for 85% of all lung cancers. In NSCLC, epidermal growth factor receptor (EGFR) mutations represent the defining actionable targets, particularly enriched in adenocarcinomas, females, never-smokers, and Asian demographics (15%–50%).2–5 While EGFR-tyrosine kinase inhibitors (TKIs) serve as the standard first-line therapy and substantially improve survival, universal acquired resistance ultimately restricts their long-term efficacy.6,7
Immune checkpoint inhibitors (ICIs), particularly Programmed death-1/Programmed Death Ligand 1 (PD-1/PD-L1) blockade, have transformed the therapeutic landscape of advanced NSCLC.8,9 However, patients with EGFR mutations derive limited clinical benefit from ICIs. Retrospective analyses of landmark trials (e.g., CheckMate 057, KEYNOTE-010, and OAK) show no survival superiority over docetaxel and occasionally exhibit inferior early survival due to crossing hazard curves.10–12 Moreover, concurrent ICIs and EGFR-TKI administration exacerbates toxicity without synergistic efficacy, making the underlying mechanisms of immune evasion a major focus of ongoing translational research.13,14 Despite these challenges, the IMpower150 trial confirmed a survival benefit using a quadriplet regimen (ICI, chemotherapy, and anti-angiogenesis) in EGFR-mutant (EGFR-Mu) cohorts. 15 Similarly, durvalumab retreatment in heavily pretreated EGFR/Anaplastic Lymphoma Kinase (ALK)-mutated patients yields a clinically meaningful survival benefit (Overall Survival (OS): 13.3 months) that positively correlates with PD-L1 expression (⩾25%) rather than driver mutation status. 16
The primary driver of this resistance is the inherently “cold” tumor microenvironment (TME) of EGFR-Mu NSCLC. This suppressive niche is characterized by a uniquely low tumor mutational burden typical of non-smokers, 5 a marked depletion of cytotoxic T lymphocytes accompanied by severe T cell exhaustion, 17 and the preferential recruitment of immunosuppressive cells such as regulatory T cells and myeloid-derived suppressor cells. 18
Accumulating extracellular adenosine serves as a primary immunosuppressive mechanism within the TME, rendering the adenosine pathway a crucial therapeutic target for overcoming immune evasion.19,20 This process relies on the sequential enzymatic activity of CD39 (ATP/ADP hydrolysis to AMP) and CD73 (AMP dephosphorylation to adenosine), culminating in the activation of purinergic receptors (A1R, A2AR, A2BR, and A3R).21,22 Importantly, targeting this axis has been shown to augment the efficacy of ICIs, chemotherapy, targeted therapies, and radiotherapy.23,24 CD73 is upregulated in EGFR-Mu NSCLC, and combined CD73 blockade and immunotherapy restores antitumor activity. 25 Beyond CD73, emerging evidence highlights CD39 as a critical upstream checkpoint that simultaneously coordinates tumor cell proliferation and immune suppression, underscoring its therapeutic potential. 26
Given this biological rationale, we retrospectively analyzed real-world immunotherapy outcomes in EGFR-Mu NSCLC to investigate the clinical relevance of the CD39-adenosine pathway. We sought to determine whether targeting this distinct axis could represent a viable strategy to overcome immune resistance and improve clinical outcomes in this challenging patient population.
Methods
The reporting of this study conforms to the REMARK guidelines 27 (Supplemental Table 1).
Public databases
Differential expression of adenosine pathway genes (CD39, CD73, ADORA1, ADORA2A, and ADORA2B) was analyzed across EGFR-Mu and wild-type (EGFR-WT) lung adenocarcinoma (LUAD) cohorts using TIMER2.0. 28 This comparative transcriptomic analysis was conducted to evaluate the influence of EGFR mutation status on the lung cancer immune microenvironment. Immune infiltration profiles for LUAD were retrieved from the tumor cell immunology Atlas (TCIA) database (https://tcia.at/home), while corresponding EGFR mutation status and transcriptomic data (CD39, CD73, and ADORA1) were sourced from cBioPortal. These disparate datasets were integrated via unique sample identifiers to establish a unified cohort for subsequent immunological analysis.
Clinical patients
A total of 43 patients with NSCLC treated at Nanjing Jingling Hospital were included in this study, comprising 19 patients with EGFR mutations who received ICIs and 24 patients with EGFR wild-type status. Patients were selected through a stepwise procedure based on predefined inclusion and exclusion criteria. Inclusion criteria were: (1) histologically or cytologically confirmed NSCLC; (2) availability of EGFR mutation status determined by tumor tissue or liquid biopsy; (3) received ICI therapy as a second or later-line treatment. Exclusion criteria were: (1) concurrent active malignancies; (2) incomplete follow-up data.
Patient samples were retrospectively identified from the hospital’s clinical database, and eligible cases were consecutively enrolled following the above criteria. Baseline clinical characteristics were collected, including gender, age, tumor stage, pathological subtype, smoking history, EGFR mutation status, distant metastasis, and line of ICIs. In addition, prior treatment history was documented in detail, including systemic therapies (e.g., chemotherapy and targeted therapy) administered before immunotherapy.
Efficacy and survival analysis
Progression-free survival (PFS) was defined as the time from initiation of immunotherapy to disease progression or death from any cause, censoring patients alive and progression-free at last follow-up. The primary clinical endpoint was durable clinical benefit (DCB), defined as the attainment of complete response (CR), partial response (PR), or stable disease (SD) for a minimum duration of 6 months, according to RECIST v1.1 criteria. Patients who experienced progressive disease (PD) or SD for less than 6 months were categorized as having non-durable benefit (NDB). Objective Response was defined strictly as CR or PR. These definitions were utilized consistently for all subsequent correlative analyses between CD39+ CD8+ T cell infiltration and clinical outcomes.
We have explicitly clarified that in this study, patients achieving DCB are referred to as the “Response group,” while those with NDB are categorized as the “Non-response group.”
Ethics statement
This retrospective study was reviewed and approved by the Institutional Medical Ethics Committee of Jinling Hospital (2024DZKY-051-01). The study complies with the ethical standards for research involving human participants, as outlined in the Declaration of Helsinki.
Immunohistochemistry and immunofluorescence
Paraffin-embedded sections of pathological tissue were obtained from the 19 EGFR-mutated and 24 EGFR wild-type patients. All tissue samples were collected at initial diagnosis prior to any immunotherapy treatment. Immunohistochemistry (IHC) was performed to assess the expression of CD39, CD73, and ADORA1. IF staining was conducted to evaluate CD39+ CD8+ T cells, PD-1+ CD8+ T cells, and total CD8+ T cells.
IHC images were acquired using a unified microscopy system under standardized lighting conditions, with 3–5 distinct fields of view selected per slide. Expression levels were quantified using Image-Pro Plus software. The mean optical density was calculated as the integrated optical density (IOD) divided by the total area. IF slides were scanned utilizing a Servicebio immunofluorescence scanner and subsequently analyzed with CaseViewer software. The proportion of CD39+CD8+ T cells was calculated as the percentage of CD39+ cells among total CD8+ T cells; a similar formula was applied for PD-1+ CD8+ T cells. The primary antibodies of immunohistochemical tissue sections are ENTPD1 (Cell Signaling Technology, USA), CD73 (Cell Signaling Technology, USA) and ADORA1 (Cell Signaling Technology, USA). The primary antibodies used in immunofluorescence include CD39 (Abcam, USA), PD-1 (Abcam, USA), and CD8 (Abcam, USA). The secondary antibodies used are AF594 donkey anti-mouse IgG antibody (Abcam, USA) and AF488 donkey anti-rabbit IgG antibody (Abcam, USA). Finally, cell nuclei were counterstained with 4’,6-diamidino-2-phenylindole (DAPI; Abcam, USA) according to the manufacturer’s instructions.
Statistical analysis
Statistical analyses were performed using three software platforms, each selected for its specific strengths. SPSS 26.0 (IBM, Armonk, NY, USA) 29 was used for univariate and multivariate Cox regression analyses, as well as for descriptive statistics and management of baseline clinical data, due to its comprehensive survival analysis module and ease of data organization. GraphPad Prism 9.0 (GraphPad Software Inc., La Jolla, CA, USA) 30 was employed for generating publication-ready figures and for conducting univariate comparisons between groups, owing to its intuitive interface and high-quality graphical output. R version 4.5.2 (R Core Team, New Zealand) 31 was utilized specifically for correlation analyses, as it offers robust and flexible packages for comprehensive correlation matrix generation and visualization.
For comparisons between two independent groups, the Wilcoxon rank-sum test (Mann–Whitney U test) was applied. Normality was assessed using the Shapiro-Wilk test; as the data did not meet the normality assumption required for parametric tests, the non-parametric Wilcoxon rank-sum test was used. For parametric comparisons where assumptions were satisfied, Student’s t-test was used.
Correlation analyses were performed using Pearson’s correlation method. Correlation analyses were conducted using R version 4.5.2 with the following packages: “corrplot” 32 for generating correlation matrices with clustering and color-coded visualization; “ggplot2” 33 for creating customized scatter plots with fitted regression lines; “ggpubr” 34 for automatically adding statistical test results (including correlation coefficients and p-values) to plots; and “GGally” 35 for producing pairwise correlation matrix plots across multiple variables. Effect sizes for Pearson correlations are reported directly as correlation coefficients (r), and for Spearman correlations as Spearman’s ρ.
Univariate and multivariate Cox proportional hazards regression analyses were performed using SPSS 26.0 to identify factors associated with patient outcomes. Variables with p < 0.10 in univariate analysis were included in the multivariate model. Results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
A two-sided p-value < 0.05 was considered statistically significant. All statistical analyses were performed using the software and packages cited above with their appropriate references.
Results
The CD39-adenosine pathway is activated in EGFR mutant NSCLC through database analysis
The expression of CD39, CD73, and ADORA1 in EGFR-Mu NSCLC samples was significantly increased compared with EGFR-WT NSCLC (CD39: p = 0.0085; CD73: p = 0.0036; ADORA1: p < 0.0001; Figure 1(a)–(c)). No significant difference in ADORA2A expression was observed between the two groups (p = 0.7200; Figure 1(d)). ADORA2B expression was higher in EGFR-Mu NSCLC compared to EGFR-WT NSCLC (p = 0.0370; Figure 1(e)). Figure 1(f) shows the expression levels of these genes in EGFR mutant samples compared to EGFR wild-type samples. Log2FC (log2 fold change) measures the magnitude and direction of gene expression changes. In LUAD samples, ADORA1 expression levels differed most between the two groups.
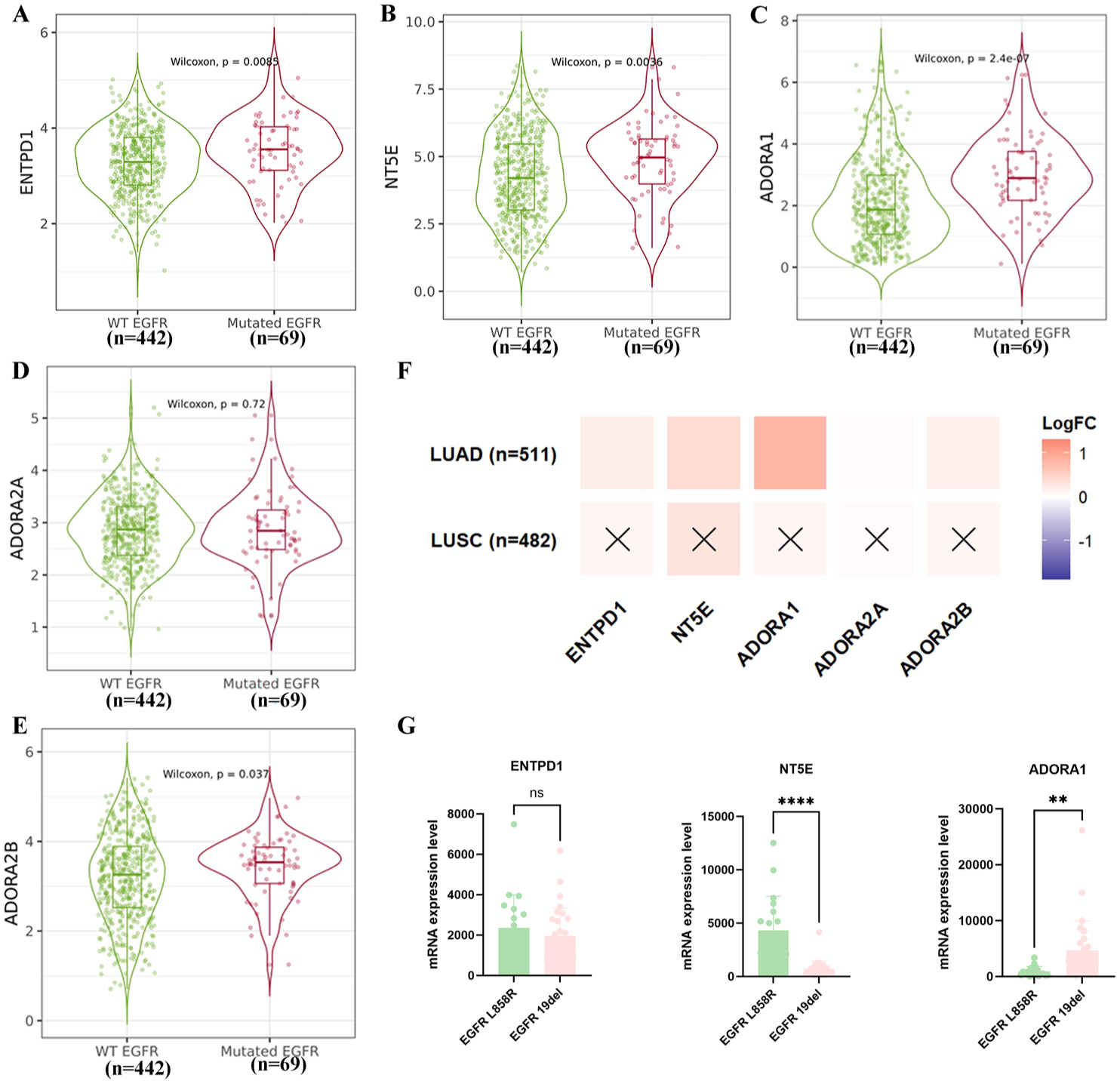
Activation of the CD39-adenosine signaling pathway in EGFR-Mu NSCLC samples. (a–e) Violin plots showing expression of CD39, CD73, ADORA1, ADORA2A, and ADORA2B in EGFR-Mu and EGFR-wild-type (EGFR-WT) samples. Data are presented as median ± IQR. p-Values were calculated using the Wilcoxon rank-sum test. (f) The heatmap shows the log2 fold changes of the differential expression of CD39, CD73, ADORA1, ADORA2A, and ADORA2B for LUAD and LUSC. Red represents a higher level in the mutant sample, and blue represents a lower level in the mutant sample. The deeper the color, the more significant the change. (g) Expression of CD39, CD73, and ADORA1 in EGFR L858R and EGFR 19del samples.
Regarding EGFR mutation subtypes, CD39 showed no significant difference in expression between EGFR L858R and 19del samples (median difference = −381.3, 95% CI: −1257 to 494.6, p = 0.3854). CD73 exhibited higher expression in EGFR L858R samples compared to 19del samples (median difference = −3608, 95% CI: −4845 to −2372, p < 0.0001). ADORA1 demonstrated higher expression in EGFR 19del samples compared to L858R samples (median difference = 3774, 95% CI: 1313–6236, p = 0.0340; Figure 1(g)).
CD39 correlated with immune cell infiltration in EGFR mutant NSCLC
Immune cells constitute the most critical component of the tumor immune microenvironment.36,37 We have identified that the adenosine signaling pathway is activated in patients with EGFR-mutated lung cancer. Consequently, we further investigated the correlation between CD39, CD73, and ADORA1 expression levels and the infiltration levels of various immune cells.
We obtained all EGFR-Mu sample information from the cBioPortal database, matching it with CD39, CD73, and ADORA1 expression data and immune cell infiltration data (Supplemental Table 2). Results revealed that in EGFR-Mu LUAD samples, CD39 expression was positively correlated with M2 macrophage infiltration (corr: 0.435, 95% CI: 0.28–0.59, p = 0.0002); No correlation was observed between CD39 expression and CD8 T cell infiltration (corr: −0.178, 95% CI: −0.38 to 0.04, p = 0.0890) or M1 macrophage infiltration (corr: −0.030, 95% CI: −0.24 to 0.18, p = 0.7200). No significant differences were observed in the correlation between CD73 and ADORA1 and immune cell infiltration (Figure 2).
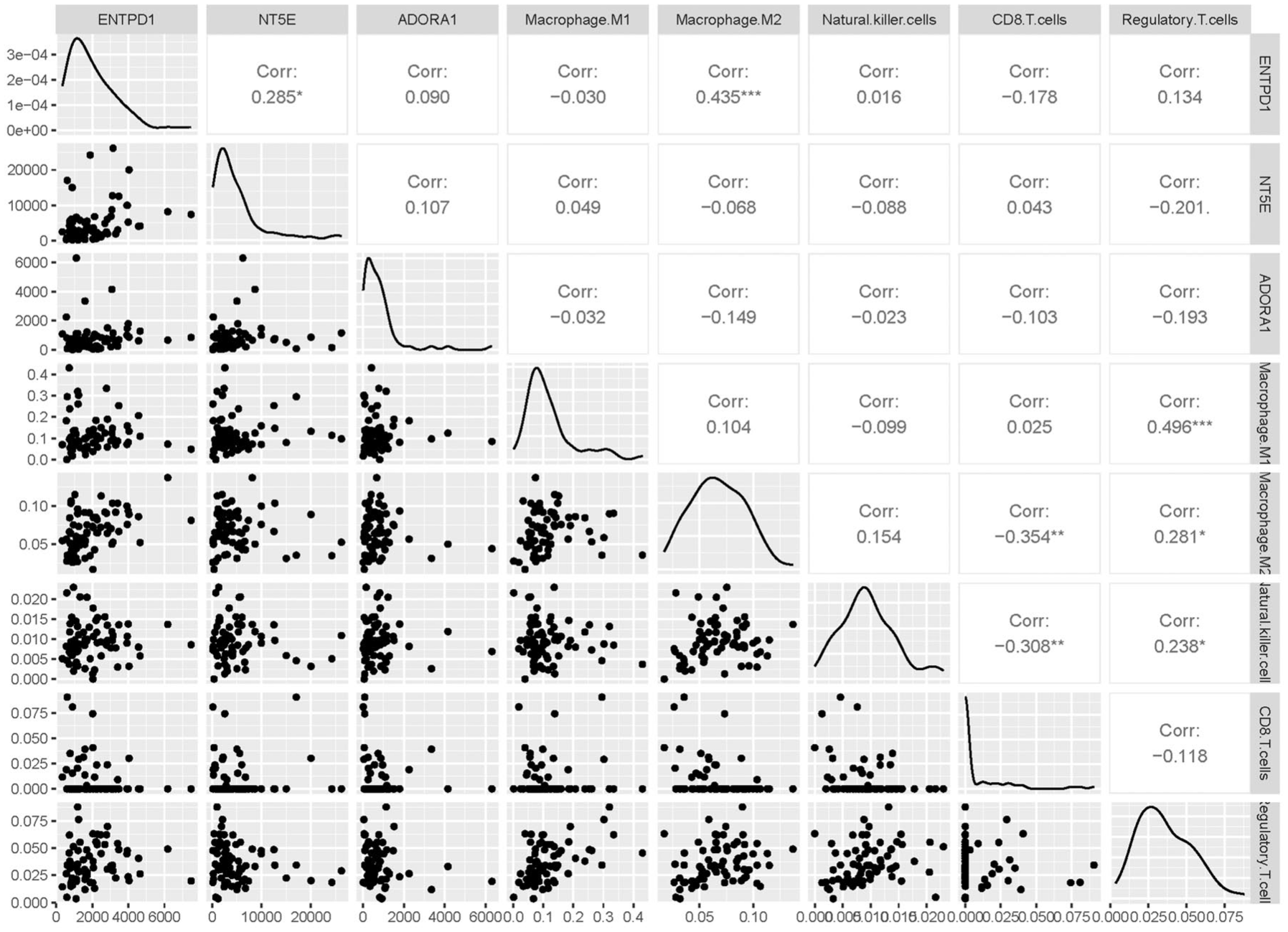
Correlation plot of CD39, CD73, and ADORA1 expression with immune cell (M1 macrophages, M2 macrophages, NK cells, CD8 T cells, and Treg cells) infiltration.
Total CD39 expression and CD39+CD8+ T cells infiltration in EGFR mutant NSCLC patients
To further validate the results of the database, we analyzed tumor specimens from real-world patients with NSCLC. The patient screening process is shown in Figure 3, and we ultimately included 19 EGFR-mutated (EGFR-Mu) patients and 24 EGFR wild-type (EGFR-WT) patients who met the criteria for this study. The basic clinical characteristics are shown in Table 1.
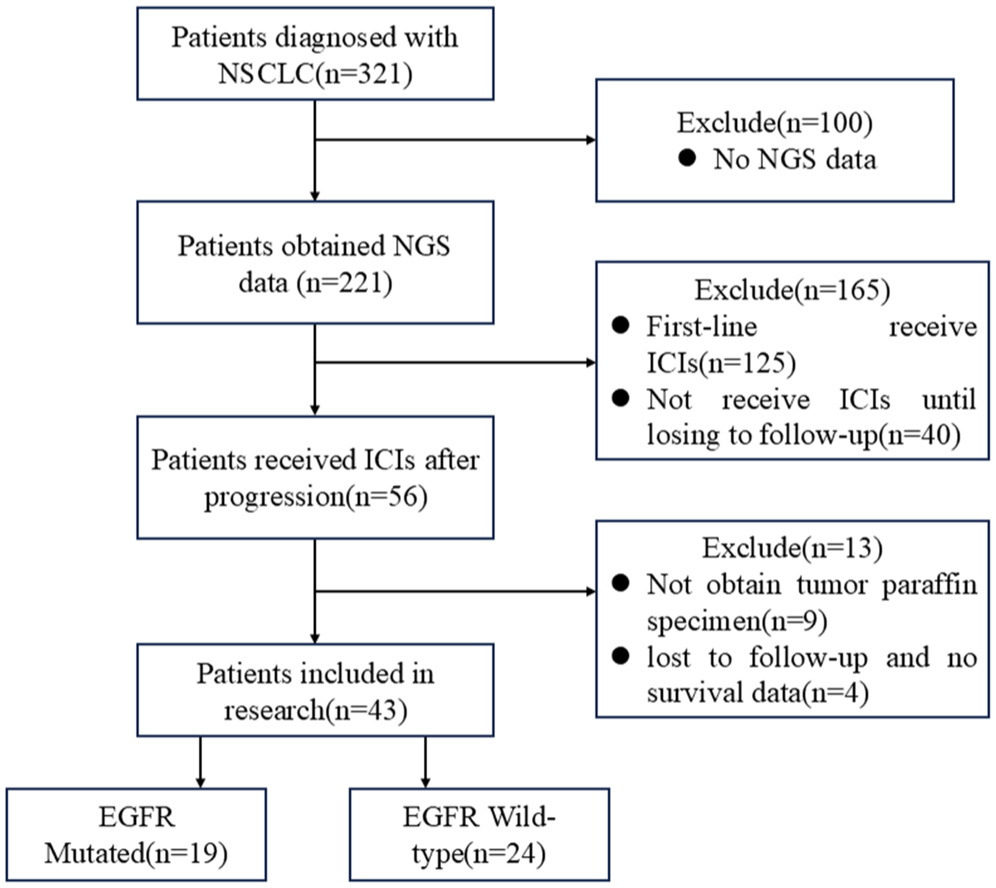
CONSORT flow diagram.
Baseline characteristics of enrolled patients.
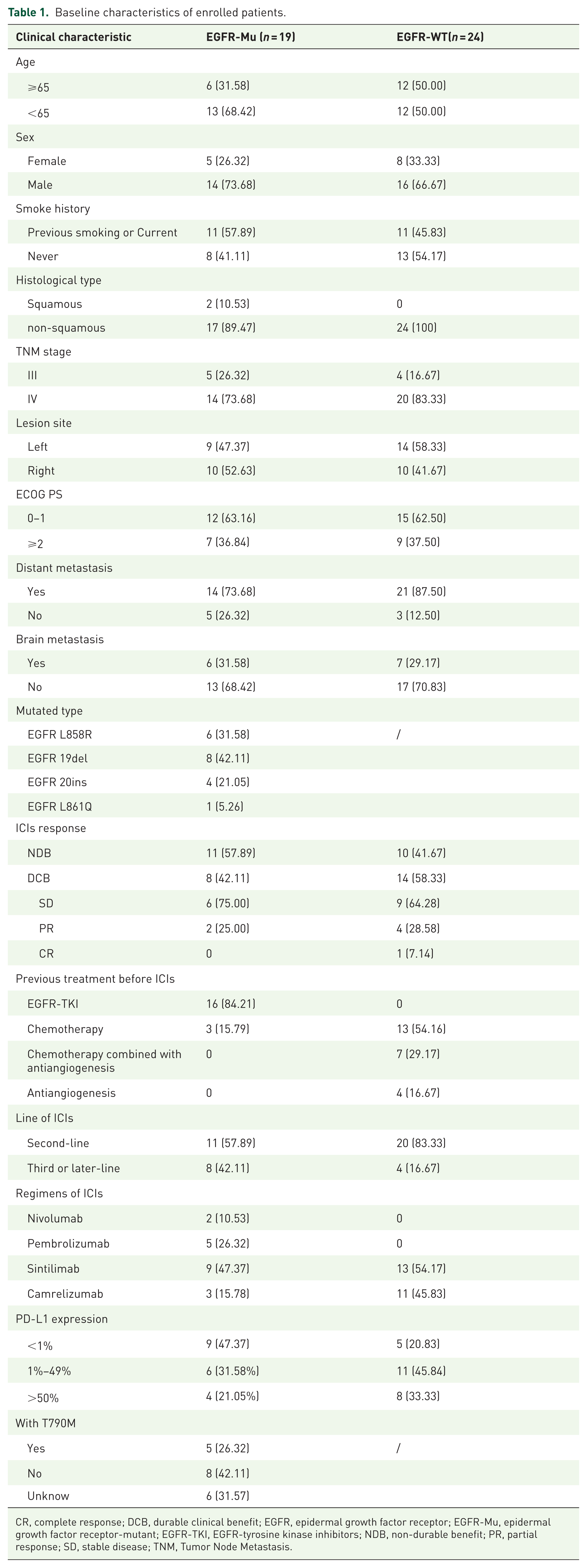
CR, complete response; DCB, durable clinical benefit; EGFR, epidermal growth factor receptor; EGFR-Mu, epidermal growth factor receptor-mutant; EGFR-TKI, EGFR-tyrosine kinase inhibitors; NDB, non-durable benefit; PR, partial response; SD, stable disease; TNM, Tumor Node Metastasis.
Immunohistochemistry analysis of clinical specimens confirmed that CD39 expression was significantly higher in EGFR-Mu patients compared to EGFR-WT patients (p < 0.0001), as was CD73 expression (p = 0.0008). ADORA1 expression showed no statistically significant difference between groups (p = 0.3900; Figure 4(a) and (b)). Immunofluorescence analysis revealed that CD39+CD8+ T cell infiltration was lower in EGFR-Mu patients compared to EGFR-WT patients (p = 0.0020). PD-1+CD8+ T cells infiltration showed no significant difference (p = 0.4100). Total CD8+ T cell infiltration was significantly lower in EGFR-Mu patients (p = 0.0260; Figure 4(c) and (d)).
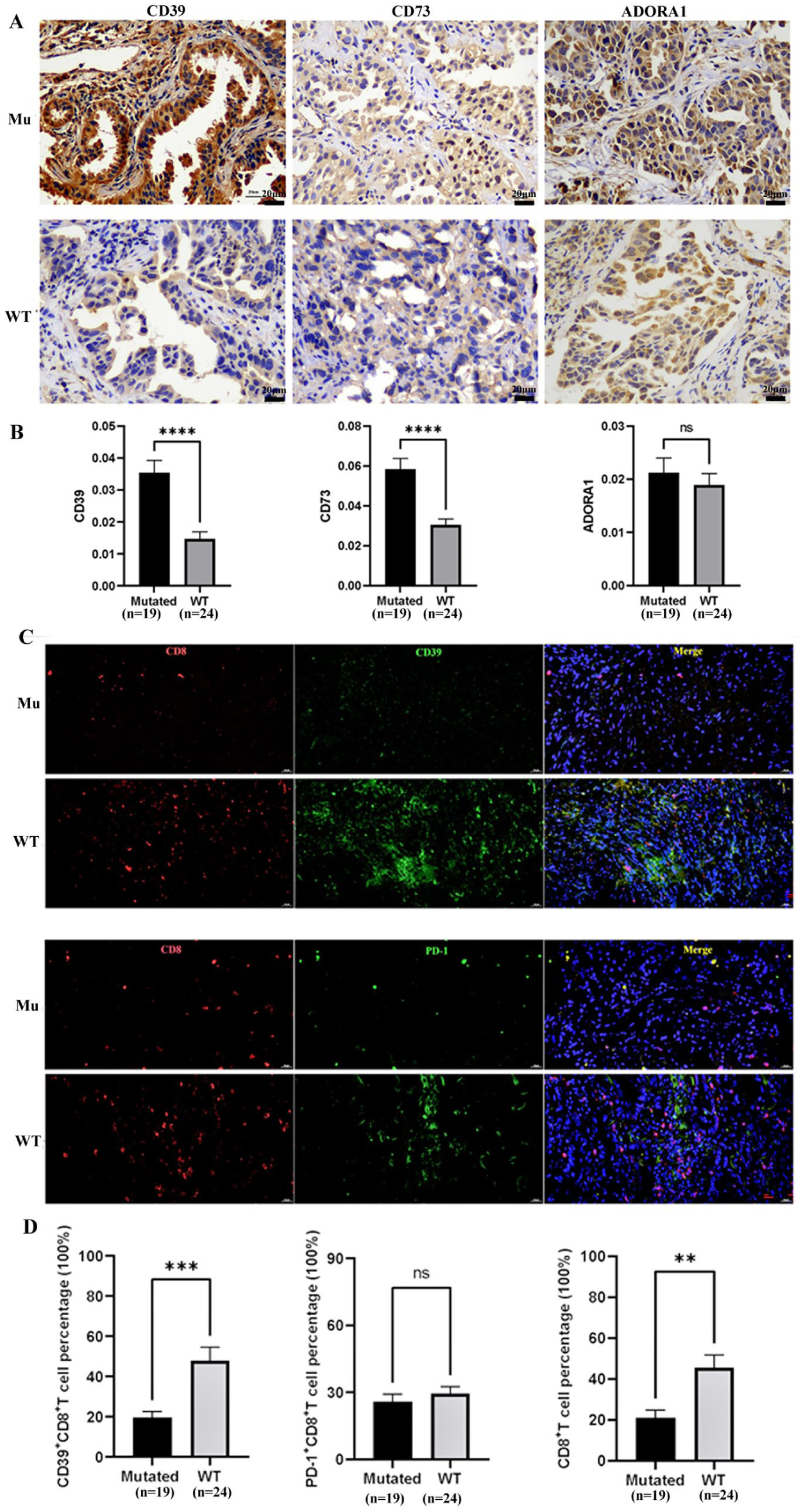
CD39 as a potential target in EGFR-Mu NSCLC patients. (a) Representative IHC staining of CD39, CD73, and ADORA1 in EGFR-Mu and EGFR-WT NSCLC patients. Scale bar = 20 μm. (b) Quantitative analysis of CD39, CD73, and ADORA1 IHC scores. Data are presented as mean ± SD. (c) Representative IF staining of CD39+CD8+ T cells and PD-1+CD8+ T cells in EGFR-Mu and EGFR-WT NSCLC patients. Scale bar = 20 μm. (d) Quantitative analysis of CD39+CD8+ T cells, PD-1+CD8+ T cells and total CD8+ T cells IF intensity (mean fluorescence intensity).
In addition, we conducted a subgroup analysis of EGFR mutant subtypes and the presence or absence of the T790M mutation. The results found that only the expression of CD39 was significantly different in EGFR 19del and EGFR 20ins patients (Supplemental Figure 1(A); p = 0.0119). While the expression of CD73 and infiltration of CD39+CD8+ T cells, PD-1+CD8+ T cells, and total CD8+ T cells were not significantly different between EGFR-mutated subtypes and T790M groups (Supplemental Figure 1(B)–1(J); all p > 0.05). The above findings are consistent with database conclusions, suggesting that CD39 may serve as an important therapeutic target for patients with EGFR-mutated NSCLC patients.
CD39 and CD39+CD8+ T cells correlate with the efficacy of immunotherapy in EGFR mutant NSCLC patients
Among EGFR-Mu NSCLC patients receiving second- or later immunotherapy, we classified patients into response and non-response groups according to clinical outcomes, with baseline patient characteristics presented in Supplemental Table 3. Patients in the response group exhibited significantly lower levels of CD39 expression than those in the non-responder group (p = 0.0094). No statistically significant differences were observed for CD73 (p = 0.5400) or ADORA1 (p = 0.7300) between the response groups and the Non-response group (Figure 5(a) and (b)). CD39+CD8+ T cell infiltration was significantly higher in response groups than in the non-response group (p = 0.005). PD-1+CD8+ T cell infiltration was also higher in response groups (p = 0.007; Figure 5(c) and (d)).
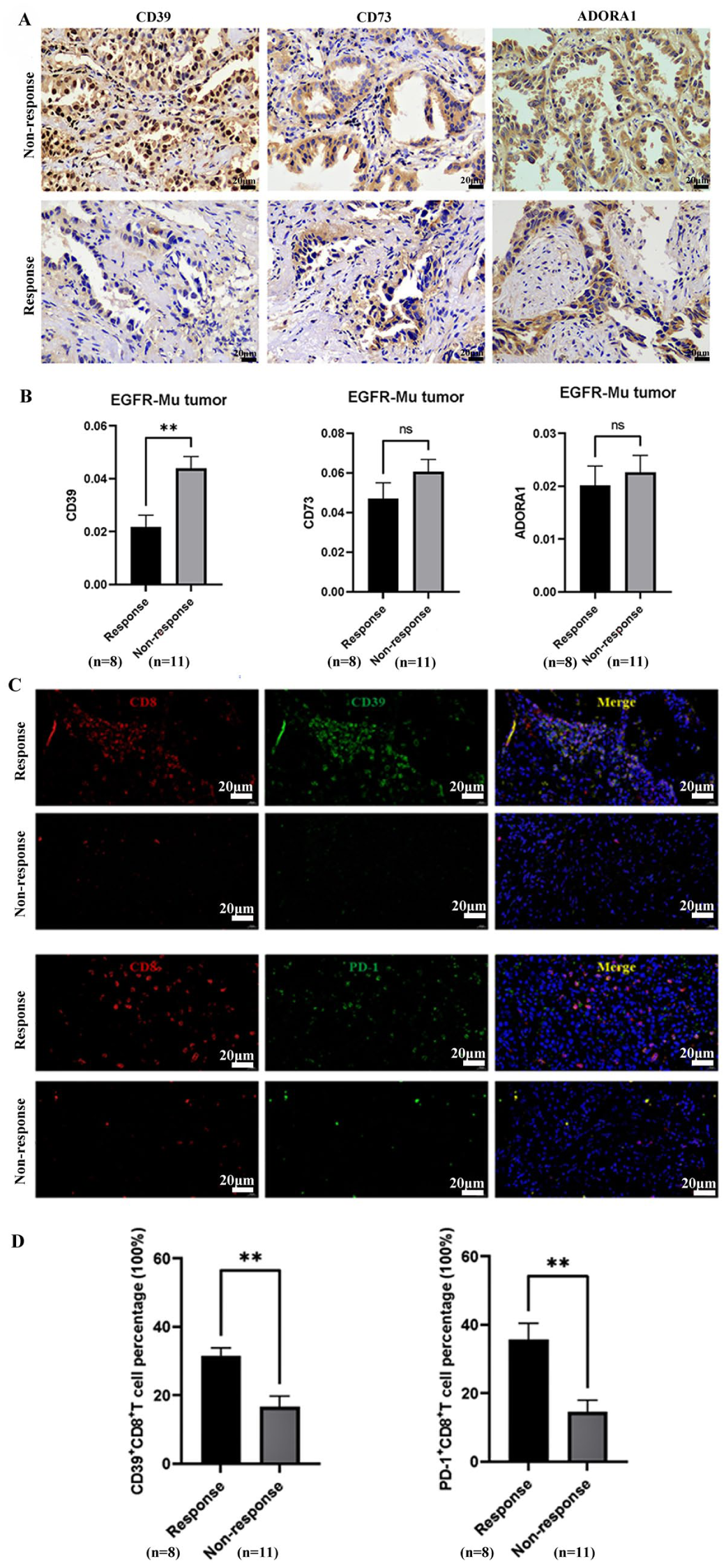
CD39 and CD39+CD8+ T cells were associated with immunotherapy response in EGFR-Mu NSCLC patients. (a) Representative IHC staining of CD39, CD73, and ADORA1 in EGFR-Mu NSCLC patients receiving immunotherapy, stratified by response (DCB) versus non-response (NDB). Scale bar = 20 μm. (b) Quantitative analysis of CD39, CD73, and ADORA1 IHC scores in response vs. non-response groups. Data are presented as mean ± SD. (c) Representative IF staining of CD39+CD8+ T cells and PD-1+CD8+ T cells in EGFR-Mu NSCLC patients receiving immunotherapy, stratified by response vs. non-response. Scale bar = 20 μm. (d) Quantitative analysis of CD39+CD8+ T cells and PD-1+CD8+ T cells IF intensity in response versus non-response groups.
Factors associated with PFS in EGFR-Mu NSCLC patients receiving immunotherapy
Among the 19 EGFR-Mu patients receiving ICIs, the overall ORR was 10.5%, the median PFS for EGFR-Mu patients was 4.53 months (0.3–11.0 m), with the median PFS for the response group being 7.2 months (6.53–11.0 m) and the median PFS for the non-response group being 2.96 months (0.3–4.8 m). To identify factors associated with PFS in EGFR-Mu NSCLC patients receiving immunotherapy, univariate and multivariate Cox regression analyses were performed. The results are summarized in Table 2.
Univariate and multivariate Cox regression analysis of PFS in EGFR-Mu patients.
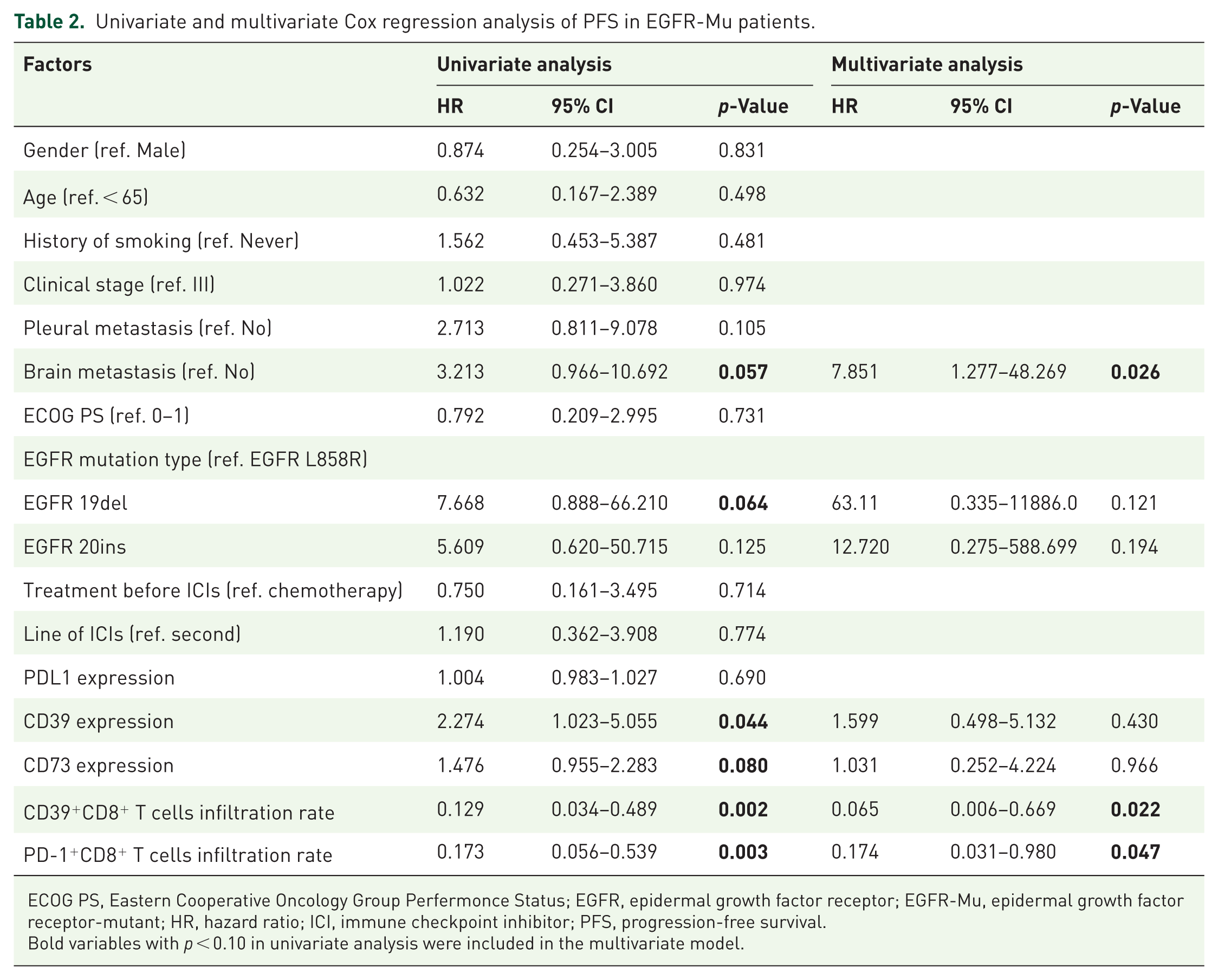
ECOG PS, Eastern Cooperative Oncology Group Perfermonce Status; EGFR, epidermal growth factor receptor; EGFR-Mu, epidermal growth factor receptor-mutant; HR, hazard ratio; ICI, immune checkpoint inhibitor; PFS, progression-free survival.
Bold variables with p < 0.10 in univariate analysis were included in the multivariate model.
In univariate analysis, brain metastasis showed a trend toward association with worse PFS (HR = 3.213, 95% CI: 0.966–10.692, p = 0.057). The EGFR 19del mutation was associated with a trend toward poorer prognosis compared to the EGFR L858R mutation (HR = 7.668, 95% CI: 0.888–66.210, p = 0.064). CD39 expression was significantly associated with shorter PFS (HR = 2.274, 95% CI: 1.023–5.055, p = 0.044), and CD73 expression showed a trend toward association with worse PFS (HR = 1.476, 95% CI: 0.955–2.283, p = 0.080). In contrast, higher infiltration rates of CD39+CD8+ T cells (HR = 0.129, 95% CI: 0.034–0.489, p = 0.002) and PD-1+CD8+ T cells (HR = 0.173, 95% CI: 0.056–0.539, p = 0.003) were significantly associated with prolonged PFS.
In the multivariate model, brain metastasis remained independently associated with worse PFS (HR = 7.851, 95% CI: 1.277–48.269, p = 0.026). CD39+CD8+ T cell infiltration (HR = 0.065, 95% CI: 0.006–0.669, p = 0.022) and PD-1+CD8+ T cell infiltration (HR = 0.174, 95% CI: 0.031–0.980, p = 0.047) were independently associated with prolonged PFS. However, CD39 expression (HR = 1.599, 95% CI: 0.498–5.132, p = 0.430) and CD73 expression (HR = 1.031, 95% CI: 0.252–4.224, p = 0.966) were not independent predictors after adjustment for other covariates. These findings suggest that higher infiltration of CD39+CD8+ T cells and PD-1+CD8+ T cells, but not the expression levels of CD39, was independent protective factors for PFS in EGFR-Mu NSCLC patients receiving immunotherapy. Conversely, brain metastasis is an independent risk factor for shorter PFS.
Due to the limited cohort size (n = 19) and the resulting low events per variable (EPV) ratio, these multivariable Cox regression results should be considered exploratory. The potential for model instability necessitates a cautious interpretation of the identified independent predictors.
Discussion
The efficacy of immunotherapy in EGFR-Mu NSCLC remains severely limited, making the identification of reliable biomarkers within its immunosuppressive TME an ongoing priority. In this exploratory, retrospective pilot study, we investigated the association between the CD39-adenosine pathway and clinical outcomes. Our findings suggest that infiltration of CD39+CD8+ T cells may be associated with clinical benefit from ICIs in a subset of patients with EGFR-Mu NSCLC. Consistent with prior reports, we observed significant upregulation of the CD39-adenosine pathway in EGFR-Mu tumors compared with EGFR wild-type tumors, supporting an immunosuppressive TME that facilitates tumor progression. However, while high CD39 expression has traditionally been associated with poor outcomes, our exploratory data suggest a more nuanced picture in which the cellular source and context of CD39 expression within the TME may influence clinical outcomes. Specifically, although total CD8+ T cell infiltration was generally sparse in EGFR-Mu NSCLC, consistent with a “cold” phenotype, the subset of CD8+ T cells expressing CD39 showed an association with prolonged progression-free survival following ICIs.
CD39 has previously been characterized as a marker of CD8+ T cell exhaustion, with high surface expression linked to reduced secretion of IFN-γ, TNF-α, and IL-2, and increased expression of co-inhibitory receptors such as PD-1, TIM-3, and LAG-3.38–40 Our study reveals that the expression of CD39 on CD8+ TILs varies significantly among lung cancer patients, with the proportion of CD39+CD8+ T cells correlating with EGFR mutation status. In addition, previous research has shown that higher enrichment of CD39-CD8+ TILs in EGFR-Mu patients predicts poor responses to anti-PD-1 therapy 38 ; Furthermore, Yeong et al. observed that a higher proportion of CD39+CD8+ T cells in the tumor was associated with better objective response rates in NSCLC patients treated with PD-1/PD-L1 inhibitors. 41 In contrast, similar findings have not been observed in melanoma, where a higher ratio of CD39+CD8+ T cells correlated with worse outcomes and shorter survival, potentially related to upregulation of TIM-3. 40 In peripheral blood analyses of NSCLC, elevated CD39+CD8+ T cells were linked to shorter PFS, whereas high PD-1+CD8+ T cell proportions correlated with improved efficacy. 42 These divergent findings underscore the need for standardized, prospective biomarker studies.
In our exploratory cohort, we observed a distinct patient subset characterized by low overall CD39 expression but relatively high CD39+CD8+ T cell infiltration. We hypothesize that this phenotype might represent a transitional, partially immune-competent state within the inherently “cold” EGFR-Mu TME. It is possible that in these patients, the presence of CD39+CD8+ T cells—despite their exhausted phenotype—reflects a pre-existing, albeit suppressed, anti-tumor immune response that could be reactivated by ICIs, potentially contributing to the observed longer PFS. Conversely, patients with high overall CD39 expression, potentially driven by other cellular sources such as regulatory T cells or myeloid cells,43–45 may reside in a more profoundly immunosuppressed state that is less responsive to therapy. Recently, a landmark large-cohort study by Chow et al. analyzed over 440 patients and established that CD39+CD8+ T cell infiltration is robustly associated with response to immune checkpoint blockade in broader lung cancer populations. 46 Our preliminary findings align with and extend this concept to the specific, challenging niche of EGFR-Mu NSCLC. Rather than a paradox, the correlation between an exhaustion marker and therapeutic benefit implies that an exhausted but T cell-infiltrated microenvironment remains a preferable substrate for therapeutic intervention compared to an entirely “cold” tumor devoid of T cells. 47
Our study has several limitations. The retrospective design, small sample size (n = 43), and lack of an independent validation cohort or predefined cut-offs restrict our ability to definitively establish CD39+CD8+ T cells as a predictive biomarker. Furthermore, our multivariable model should be viewed as exploratory rather than definitive. The limited cohort size yielded an EPV ratio below the standard threshold of 10, which potentially affects the stability of the Cox regression. While these preliminary findings underscore the significance of CD39+CD8+ T cells, multivariable associations should be considered hypothesis-generating only because of the small sample size and risk of model instability/overfitting, and the independent prognostic utility of this subset necessitates rigorous validation in larger, prospective cohorts. Selection bias and baseline confounding factors, such as the disparity in prior treatment lines between the EGFR-Mu and wild-type cohorts, may influence the results and must be acknowledged. However, it is imperative to emphasize that our mechanistic interpretations remain strictly speculative. The current study provides descriptive, phenotypic data based on IHC and immunofluorescence, lacking direct functional validation. Without comprehensive functional cytokine assays, reinvigoration experiments, or single-cell transcriptional profiling, the hypothesis that CD39+CD8+ T cells represent a “rescuable” or functionally competent population cannot be definitively confirmed. In addition, future single-cell profiling is needed to elucidate the functional landscape and reinvigoration capacity of these exhausted T cells.
In summary, our results suggest that CD39+CD8+ T cell infiltration may be a putative biomarker for predicting immunotherapy response in patients with EGFR-Mu NSCLC, which warrants further validation in larger, independent retrospective cohorts before prospective, randomized controlled trials. Given the retrospective design, small sample size, lack of independent validation, and absence of functional mechanistic validation, these findings should be considered preliminary. If confirmed, this distinct T cell subset may inform future patient stratification and targeted therapeutic strategies in oncogene-driven lung cancer.
Conclusion
Our findings suggest that CD39+CD8+ T cell infiltration is associated with immunotherapy response in EGFR-Mu NSCLC. However, given the exploratory nature of this study, these results remain hypothesis-generating and require definitive confirmation in future prospective trials.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261458240 – Supplemental material for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359261458240 for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer by Wanjun Lu, Qiuxia Wu, Zimu Wang, Qinpei Cheng, Xueying Zuo, Xin Liu, Jiawen Lv, Yong Song, Fang Zhang and Tangfeng Lv in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261458240 – Supplemental material for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer
Supplemental material, sj-docx-2-tam-10.1177_17588359261458240 for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer by Wanjun Lu, Qiuxia Wu, Zimu Wang, Qinpei Cheng, Xueying Zuo, Xin Liu, Jiawen Lv, Yong Song, Fang Zhang and Tangfeng Lv in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359261458240 – Supplemental material for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer
Supplemental material, sj-docx-3-tam-10.1177_17588359261458240 for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer by Wanjun Lu, Qiuxia Wu, Zimu Wang, Qinpei Cheng, Xueying Zuo, Xin Liu, Jiawen Lv, Yong Song, Fang Zhang and Tangfeng Lv in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tiff-1-tam-10.1177_17588359261458240 – Supplemental material for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer
Supplemental material, sj-tiff-1-tam-10.1177_17588359261458240 for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer by Wanjun Lu, Qiuxia Wu, Zimu Wang, Qinpei Cheng, Xueying Zuo, Xin Liu, Jiawen Lv, Yong Song, Fang Zhang and Tangfeng Lv in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261458240 – Supplemental material for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer
Supplemental material, sj-pdf-1-tam-10.1177_17588359261458240 for CD39+CD8+ T cell infiltration is associated with clinical outcomes of subsequent immunotherapy in advanced EGFR-mutant non-small cell lung cancer by Wanjun Lu, Qiuxia Wu, Zimu Wang, Qinpei Cheng, Xueying Zuo, Xin Liu, Jiawen Lv, Yong Song, Fang Zhang and Tangfeng Lv in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to thank our patients and their families for their support of this study.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.