
Abstract
Background:
The efficacy and safety of adebrelimab plus carboplatin and etoposide as first-line therapy in patients with extensive-stage small-cell lung cancer (ES-SCLC) have been investigated in the CAPSTONE-1 study. However, many patients with brain metastases, as well as some with liver metastases and pleural effusion, were excluded.
Objectives:
The present study focuses on exploring the safety and efficacy of adebrelimab in these patients in the real world.
Design:
This was a multicenter, prospective, observational, real-world study.
Methods:
Patients with ES-SCLC and brain metastases, liver metastases, or pleural effusion who were willing to receive adebrelimab-based regimens as first-line therapy were enrolled. The primary endpoint was progression-free survival (PFS). The secondary endpoints included objective response rate, disease control rate, duration of response, overall survival (OS), and safety.
Results:
Between March 2, 2023, and September 3, 2024, a total of 149 patients were enrolled in the present study. Among them, 50 (33.6%) patients had brain metastasis, 60 (40.3%) had liver metastasis, and 85 (57.0%) had pleural effusion. At data cutoff (May 5, 2025), the median PFS (mPFS) was 6.47 months (95% confidence interval (CI): 5.85–7.03), and the median OS (mOS) was 13.77 months (95%CI: 11.30–15.44) in the full analysis set. Additionally, the mPFS were 6.01 months (95%CI: 4.83–7.59), 5.45 months (95%CI: 4.30–6.51 months), and 6.60 months (95%CI: 5.29–7.59 months) in patients with brain metastases, liver metastases, and pleural effusion, respectively. The mOS were 13.77 months (95%CI: 9.67–22.90 months), 10.51 months (95%CI: 8.38–13.44 months), and 12.85 months (95%CI: 9.20–16.39 months) in patients with brain metastases, liver metastases, and pleural effusion, respectively. Grade ⩾3 treatment-emergent adverse events occurred in 63 (42.3%) patients. No new safety signals were found.
Conclusion:
Adebrelimab-based regimens showed effectiveness comparable to clinical trials in special populations such as patients with brain metastases or pleural effusion, and demonstrated an acceptable safety profile. However, the benefit appeared limited in patients with liver metastases.
Plain language summary
This study looked at a treatment combining adebrelimab with chemotherapy for people with a severe type of lung cancer called extensive-stage small-cell lung cancer (ES-SCLC). Among 149 patients, about one-third had brain metastases, 40% had liver metastases, and over half had pleural effusion. The treatment worked well and was generally safe for patients with brain metastases or pleural effusion, but it seemed less effective for those with liver metastases. Overall, adebrelimab plus chemotherapy appears to be a promising and safe option for patients who are often left out of clinical trials.
Keywords
Introduction
Worldwide, lung cancer is the most commonly diagnosed cancer and the leading cause of cancer-related death. 1 In China, small cell lung cancer (SCLC) accounts for approximately 13%–18% of all lung cancers. SCLC is characterized by an aggressive and fast-growing nature and nearly two-thirds of all patients with SCLC present with extensive-stage disease at initial diagnosis.2–5
Currently, the development of immunotherapy has changed the standard of care for first-line therapy of extensive-stage SCLC (ES-SCLC) to a combination of platinum-based chemotherapy and immunotherapy, which is now recommended by several international guidelines.6–8 This recommendation is based on two phase III clinical trials, the IMpower133 study and the CASPIAN study. These studies demonstrated that the combination of platinum-based chemotherapy with programmed cell death ligand 1 (PD-L1) inhibitors showed prolonged overall survival (OS) when compared with chemotherapy alone in patients with ES-SCLC as first-line treatment.9,10
Adebrelimab (SHR-1316) is a humanized IgG4 monoclonal antibody that specifically binds to PD-L1. In 2023, adebrelimab was approved for the first-line treatment of ES-SCLC by the National Medical Products Administration of China based on the results of the CAPSTONE-1 study. 11 The CAPSTONE-1 study was a randomized, double-blind, phase III trial that enrolled patients with ES-SCLC to receive first-line treatment with carboplatin and etoposide plus either adebrelimab or placebo. The results showed that, compared with placebo, the addition of adebrelimab to chemotherapy significantly prolonged median OS (mOS; 15.3 vs 12.8 months; hazard ratio (HR) = 0.72). 12 However, as a phase III clinical trial, CAPSTONE-1 had strict inclusion criteria, resulting in the exclusion of most patients with brain metastasis, as well as some with liver metastasis and pleural effusion. In addition, compared with the IMpower133 and CASPIAN trials, the CAPSTONE-1 enrolled a relatively lower proportion of patients with brain or liver metastases. These differences in study populations may partly contribute to the variations in survival outcomes observed across trials. In real-world settings, approximately 40%–60% of patients with ES-SCLC have brain metastases, 17% have liver metastases, and about 28% have pleural effusion,13–19 leading to a discrepancy between the patient populations in these trials and those encountered in clinical practice. The evidence regarding the efficacy and safety of adebrelimab-based therapies as first-line treatment in ES-SCLC patients with brain metastases, liver metastases, and pleural effusion is still lacking.
Therefore, we conducted this real-world, prospective study involving ES-SCLC patients with brain metastases, liver metastases, and pleural effusion who received adebrelimab-based regimens as first-line therapy, aiming to evaluate the effectiveness and safety of adebrelimab in real-world clinical practice.
Methods
Study design and patients
This was a multicenter, prospective, observational, real-world study conducted in China at five institutions, including Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences; Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology; Qilu Hospital, Shandong University; The Second Affiliated Hospital of Shandong First Medical University; and Binzhou Medical College Affiliated Hospital between March 2, 2023, and September 3, 2024. The study was conducted according to the Declaration of Helsinki and Good Clinical Practice guidelines. The study protocol has been approved by the Ethics Committee of the Affiliated Cancer Hospital of Shandong First Medical University (number: SDZLEC2023-225-02). The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 20 The STROBE checklist is provided in Supplemental Table 1.
Patients were included if they met the following criteria: (1) age ⩾18 years old; (2) ES-SCLC confirmed by histological or cytological examination; (3) with brain metastasis, liver metastasis, or pleural effusion; (4) planning to receive first-line treatment based on adebrelimab. Exclusion criteria included: (1) previous treatment with any T cell co-stimulation or immune checkpoint inhibitors, including but not limited to cytotoxic T lymphocyte-associated antigen-4 inhibitors, PD-1 inhibitors, PD-L1/2 inhibitors, or other T cell-targeting therapies; (2) currently participating in other interventional studies; (3) concurrent malignant tumors; (4) pregnant or lactating patients.
Treatment procedure
Eligible patients received adebrelimab-based regimens as first-line therapy. Adebrelimab was administered at a dose of 1200 mg (intravenously, on day 1, every 3 weeks).
The specific regimens and doses were determined by clinicians according to the actual situation.
Endpoints and clinical assessments
The primary endpoint was progression-free survival (PFS), which was defined as the time from treatment initiation to disease progression or death from any cause. The secondary endpoints included objective response rate (ORR), defined as the percentage of patients with a complete response (CR) or partial response (PR); disease control rate (DCR), defined as the percentage of patients with CR, PR, or stable disease (SD); duration of response (DoR), defined as the time from the first response to disease progression or death; OS, defined as the time from treatment initiation to death from any cause, and safety according to the Common Terminology Criteria for Adverse Events Version 5.0.
Follow-up began when patients started receiving adebrelimab and continued until death, loss to follow-up, withdrawal of informed consent, or study termination, whichever occurs first. Since this study was an observational study, visits and examinations were based on the routine clinical practice. The data for this study primarily came from patients’ routine medical records.
Statistical analysis
Categorical variables were described as numbers and percentages, and their 95% confidence interval (CI) was calculated using the Clopper–Pearson method. Continuous variables were described using medians. The Kaplan–Meier method was used to estimate PFS, OS, and DoR, with the 95%CI of the median time calculated using the Brookmeyer–Crowley method. The full analysis set (FAS) was defined as patients who received at least one dose of adebrelimab.
All analyses were conducted using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline characteristics
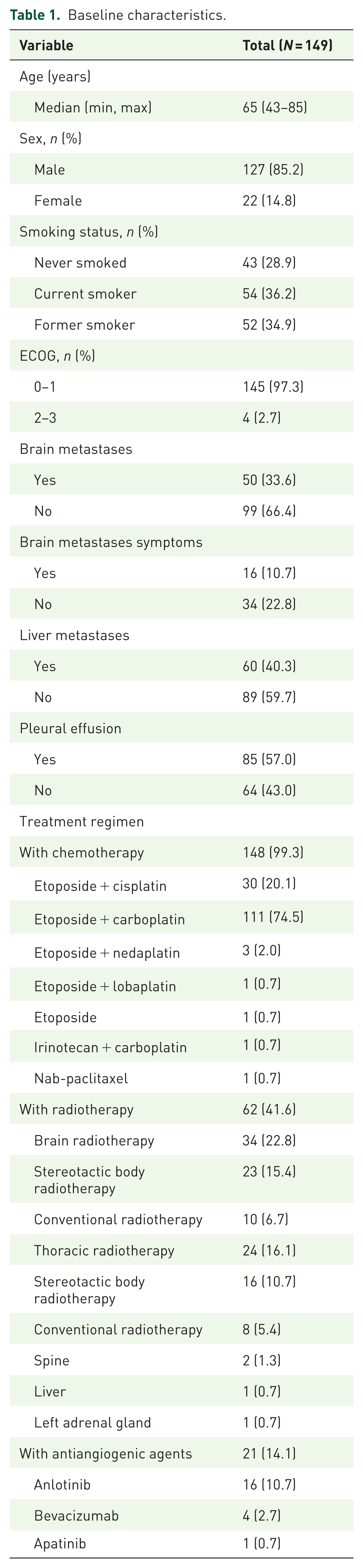
Between March 2, 2023, and September 3, 2024, a total of 149 patients (the FAS population) were enrolled in the present study and received at least one dose of adebrelimab. The median age was 65 years (range: 43–85), with 71 (47.7%) patients under 65 years of age. Among these patients, 127 (85.2%) were male, 106 (71.1%) were current or former smokers, and 4 (2.7%) had an ECOG score of ⩾2. Fifty (33.6%) patients had brain metastases, 60 (40.3%) had liver metastases, and 85 (57.0%) had pleural effusion. Four patients had both brain and liver metastases, 11 had both brain metastases and pleural effusion, 25 had both liver metastases and pleural effusion, and 3 had brain metastases, liver metastases, and pleural effusion. The majority (99.3%) of patients received adebrelimab-based combination therapy with chemotherapy, 62 (41.6%) received combination therapy with radiotherapy, and 23 (15.4%) received combination therapy with anti-angiogenesis therapy. Detailed baseline characteristics are presented in Table 1.
Baseline characteristics.
Effectiveness
In the FAS population, 2 (1.3%) patients achieved CR, 100 (67.1%) patients achieved PR, 11 (7.4%) patients had SD. A total of 102 (68.5%, 95%CI: 60.3–75.8) patients achieved ORR, 129 (86.6%, 95%CI: 80.0–91.6) patients achieved DCR. The median DoR was 6.97 months (95%CI: 6.51–7.59). In patients with brain metastases, the ORR and DCR were 62.0% and 80.0%. The median DoR was 5.16 months. In patients with liver metastases, the ORR was 63.3%, and the DCR was 83.3%. The median DoR was 4.80 months. In patients with pleural effusion, the ORR and DCR were 69.4% and 84.7%, with a median DoR of 5.36 months. The detailed results are shown in Table 2.
Antitumor response.
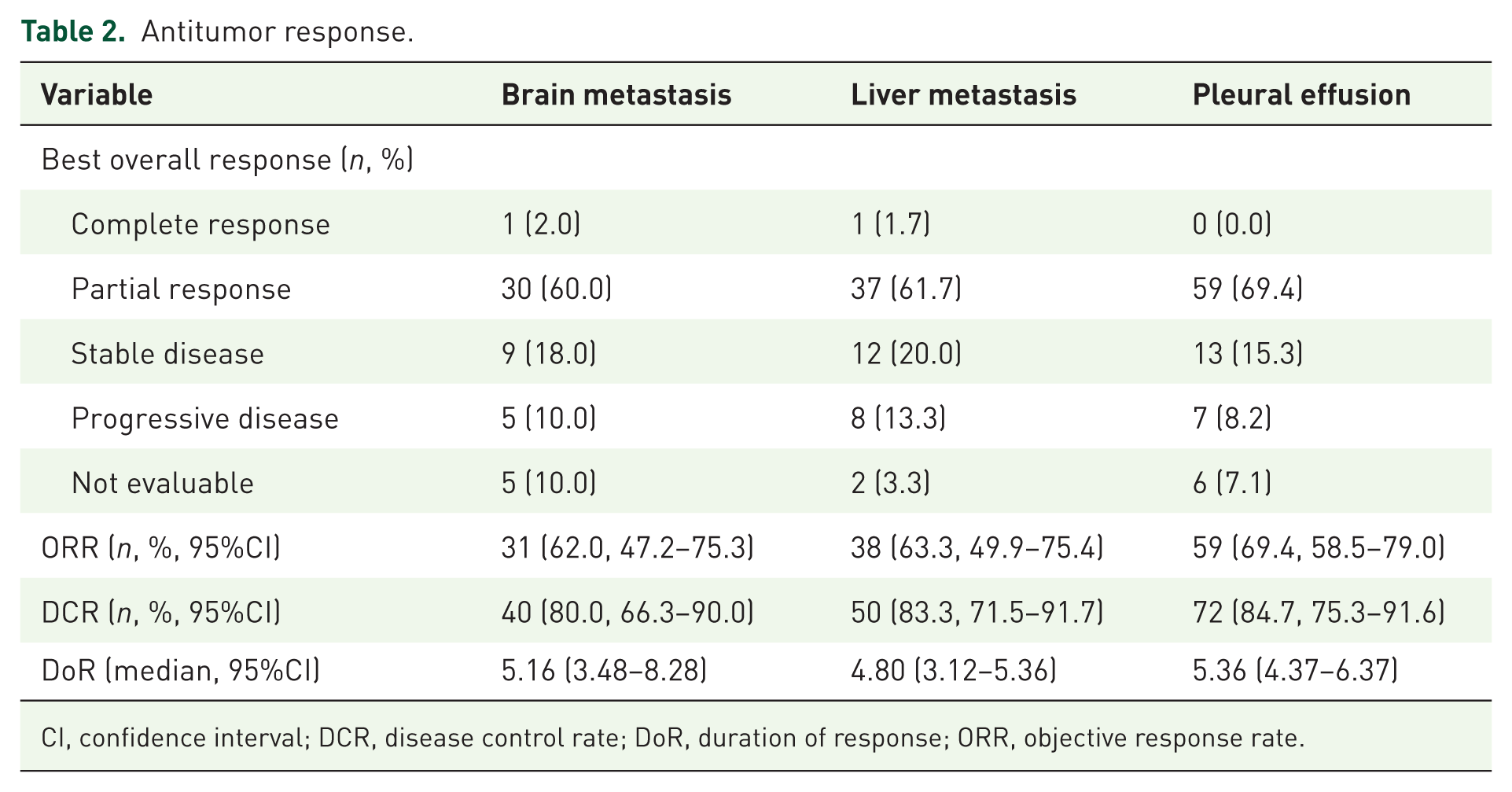
CI, confidence interval; DCR, disease control rate; DoR, duration of response; ORR, objective response rate.
At data cutoff (May 5, 2025), the median follow-up was 11.3 months (range: 7.6–14.5 months). In the FAS population, the median PFS (mPFS) was 6.47 months (95%CI: 5.85–7.03), and the mOS was 13.77 months (95%CI: 11.30–15.44). The mPFS were 6.01 months (95%CI: 4.83–7.59), 5.45 months (95%CI: 4.30–6.51), and 6.60 months (95%CI: 5.29–7.59) in patients with brain metastases, liver metastases, and pleural effusion, respectively (Figure 1(a) and (b)). The mOS were 13.77 months (95%CI: 9.67–22.90), 10.51 months (95%CI: 8.38–13.44), and 12.85 months (95%CI: 9.20–16.39) in patients with brain metastases, liver metastases, and pleural effusion, respectively (Figure 1(c) and (d)). In addition, survival outcomes stratified by radiotherapy were analyzed. The mPFS was 7.23 and 5.91 months in patients receiving and not receiving radiotherapy, respectively (HR = 0.75, 95%CI: 0.52–1.07). The mOS was 14.39 and 12.48 months in patients receiving and not receiving radiotherapy, respectively (HR = 0.91, 95%CI: 0.58–1.42; Supplemental Figure 1(A) and (B)).
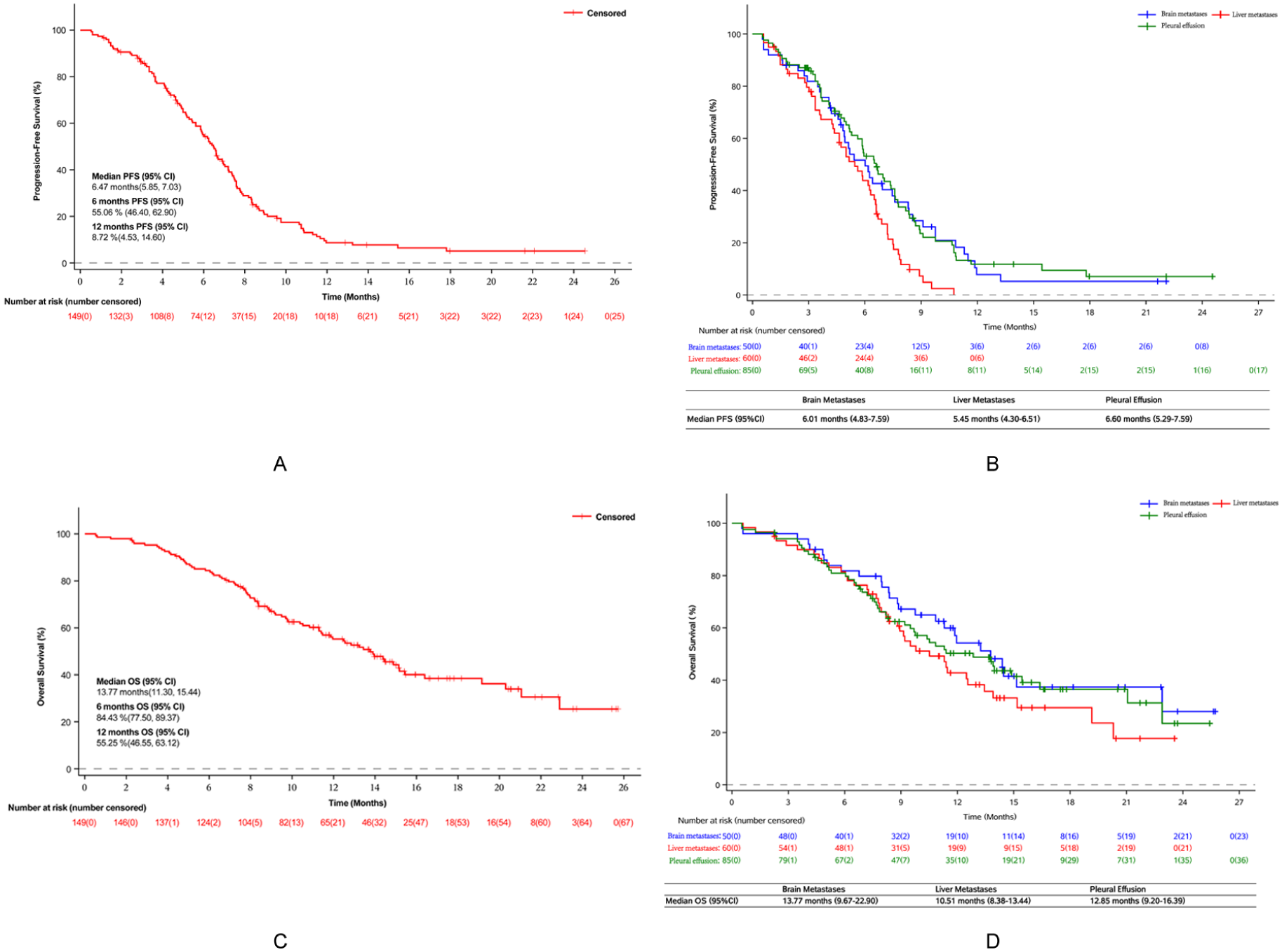
Kaplan–Meier analysis of the PFS in the FAS population (a) and in ES-SCLC patients with brain metastases, liver metastases, and pleural effusion (b). Kaplan–Meier analysis of the OS in the FAS population (c) and in ES-SCLC patients with brain metastases, liver metastases, and pleural effusion (d).
Furthermore, survival outcomes in patients with brain metastasis and liver metastasis were analyzed according to symptoms and the number of metastatic lesions. In patients with brain metastases, no significant differences in mPFS and mOS were observed between symptomatic and asymptomatic patients (symptomatic vs asymptomatic: mPFS: 8.34 vs 5.42 months, HR = 0.56, 95%CI: 0.29–1.10; mOS: 14.39 vs 13.24 months, HR = 0.70, 95%CI: 0.30–1.63) or between patients with oligometastatic brain metastases (1–3 metastases) and those with multiple brain metastases (>3 metastases; oligometastatic vs multiple: mPFS: 6.01 vs 6.18 months, HR = 0.89, 95%CI: 0.49–1.64; mOS: 11.30 vs 15.15 months, HR = 0.68, 95%CI: 0.31–1.47; Figure 2(a)–(d)). Among patients with liver metastases, no significant differences were found in mPFS and mOS between patients with a single metastatic lesion and those with multiple metastatic lesions (single metastatic lesion vs multiple metastatic lesions: mPFS: 7.20 vs 5.45 months, HR = 0.72, 95%CI: 0.38–1.36; mOS: 12.55 vs 8.94 months, HR = 0.72, 95%CI: 0.35–1.49; Figure 2(e) and (f)).

Kaplan–Meier analysis of PFS and OS according to different subgroups. PFS (a) and OS (b) in patients with symptomatic versus asymptomatic brain metastases; PFS (c) and OS (d) in patients with oligometastatic versus multiple brain metastases; and PFS (e) and OS (f) in patients with single versus multiple liver metastases.
Safety
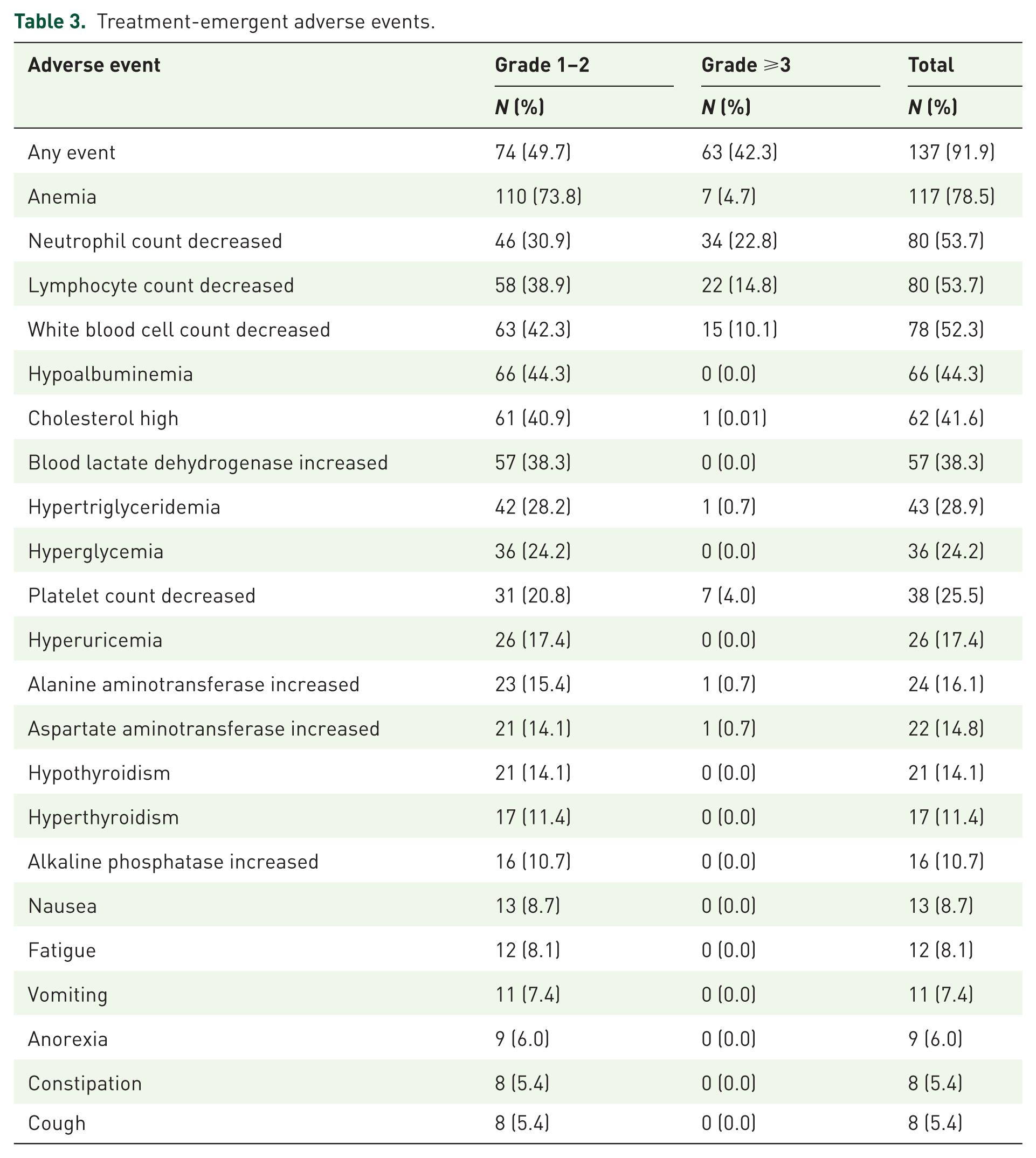
Collectively, 137 (91.9%) patients experienced treatment-emergent adverse events (TEAEs), among them, 63 (42.3%) patients experienced grade ⩾3 TEAEs. The most common TEAEs were anemia (78.5%), followed by neutrophil count decreased (53.7%) and lymphocyte count decreased (53.7%). The most commonly grade ⩾3 TEAEs were neutrophil count decreased (22.8%), followed by lymphocyte count decreased (14.8%), and white blood cell count decreased (10.1%; Table 3).
Treatment-emergent adverse events.
Discussion
The present study was the first prospective, observational, real-world study focused on evaluating the efficacy and safety of adebrelimab-based regimens in ES-SCLC patients with brain metastases, liver metastases, and pleural effusion. This study aimed to provide real-world clinical evidence on the use of adebrelimab-based regimens as first-line treatment for specific ES-SCLC patient populations in China. Although the phase III CAPSTONE-1 study explored the efficacy and safety of adebrelimab in combination with carboplatin and etoposide as first-line therapy for patients with ES-SCLC, many patients with liver or brain metastases, commonly seen in real-world clinical settings, were excluded due to severe symptoms at baseline. Moreover, some specific patient populations, such as those with pleural effusion, were neither reported in baseline characteristics nor included in subgroup analyses.
In the present study, regarding efficacy, the ORR was 68.5% in our study, comparable to the 70.4% reported in the CAPSTONE-1 study. Moreover, the mPFS and mOS were also comparable to those in the CAPSTONE-1 study (mPFS: 6.47 vs 5.8 months; mOS: 13.77 vs 15.3 months). 12
Only 2% of patients (10 patients) with brain metastases were included in the CAPSTONE-1 study, as patients with symptomatic brain metastases, involvement beyond the supratentorial region and cerebellum, or evidence of CNS progression were excluded. While in our study, a total of 50 patients with brain metastases were included, among whom 16 patients were symptomatic. The mPFS and mOS for patients with brain metastases were 6.01 and 13.77 months, respectively. The J-TAIL-2 study was a prospective, real-world study that compared the efficacy and safety of atezolizumab combined with carboplatin and etoposide in Impower-133-like and unlike populations. The results showed that the mPFS and mOS between patients with and without brain metastases (mPFS: 4.9 vs 5.2 months; mOS: 18.4 vs 16.2 months) were similar. 21 In another real-world study, ES-SCLC patients with brain metastases were treated with first-line atezolizumab in combination with platinum-based chemotherapy; the mOS was 21.9 months. 22 Differences in baseline characteristics across real-world studies should be considered when interpreting survival outcomes. Compared with the J-TAIL-2 study, our cohort included relatively younger patients, a lower proportion of patients with ECOG performance status ⩾2, and a higher proportion of never smokers, highlighting the heterogeneity among real-world study populations. These studies demonstrated comparable efficacy of immunotherapy combined with chemotherapy in ES-SCLC patients with brain metastases and those without.
A total of 32% of patients in the CAPSTONE-1 study had liver metastases. Subgroup analyses showed that, at the data cutoff, the proportion of deaths was higher in patients with liver metastases than in patients without. 12 Similar results were observed in the Impower-133 study, 23 the KEYNOTE-604, 24 and other phase III studies.25,26 In the present study, the mOS in patients with liver metastases was 10.51 months (95%CI: 8.38–13.44 months). Liver metastases have been identified as an independent risk factor for poor survival in ES-SCLC patients who received immunotherapy combined with chemotherapy. 27 This finding may be associated with the immunosuppressive microenvironment of the liver. 28 However, it may also reflect the more aggressive tumor biology and poorer baseline prognosis commonly observed in patients with liver metastases. In addition, a network meta-analysis, which included 7 randomized clinical trials, demonstrated that, compared with chemotherapy alone, immunotherapy combined with chemotherapy showed better efficacy as first-line therapy for ES-SCLC patients with liver metastases. 29 Further prospective clinical studies with large sample sizes were needed to assess the anti-tumor effect of immunotherapy combined with chemotherapy in this population.
The proportion of patients with pleural effusion in the CAPSTONE-1 study was unknown. Although malignant pleural effusion has been recognized as a poor prognostic factor in patients with ES-SCLC, 30 no studies to date have focused on immunotherapy in ES-SCLC patients with pleural effusion. The OS of patients with pleural effusion in the present study was 12.85 months, suggesting a promising clinical efficacy. Further exploration of immunotherapy in this patient population is warranted.
Notably, we compared survival outcomes between patients who received radiotherapy and those who did not. Thoracic radiotherapy was not allowed in phase III clinical trials investigating the efficacy of immunotherapy and chemotherapy as first-line treatment for patients with ES-SCLC, but many real-world studies have demonstrated improved prognosis when radiotherapy was added to immunochemotherapy.31–34 In the present study, patients receiving radiotherapy showed a trend toward prolonged PFS and OS compared with those who did not receive radiotherapy. This might partially explain why these specific populations with risk factors achieved a prognosis comparable to that of the general population.
Regarding safety, no previously unreported adebrelimab-related AEs were observed. The AEs from this study are consistent with those in the CAPSTONE-1 study. The results suggest that adebrelimab, as a first-line treatment, has an acceptable safety profile in the ES-SCLC patient population in clinical practice.
The study had several limitations. First, as a real-world, observational study, selection bias was inevitable. Second, the follow-up time was short. Third, only TEAEs were reported, preventing an in-depth comparative analysis with the safety profile in the CAPSTONE-1 study. Fourth, only Chinese patients were included in the present study, which limits the generalizability of the findings to other ethnic populations. Fifth, subgroup analyses of patients with brain metastases, including symptomatic versus asymptomatic disease and oligometastatic versus multiple brain metastases, were limited by the relatively small sample sizes, which restricted further interpretation of these findings. Finally, some detailed treatment-related variables, including concomitant corticosteroid use and radiotherapy indication, dose, and technique, were not fully available in this real-world study, which may have resulted in potential confounding factors.
Conclusion
Adebrelimab-based regimens demonstrated effectiveness comparable to that observed in clinical trials among specific patient populations such as patients with brain metastases and pleural effusion. However, the therapeutic benefit in patients with liver metastases appeared to be limited. In addition, this first-line treatment regimen has an acceptable safety profile.
Supplemental Material
sj-docx-2-tam-10.1177_17588359261458300 – Supplemental material for Adebrelimab-based regimens as first-line treatment for ES-SCLC in specific populations: a real-world study in Chinese patients
Supplemental material, sj-docx-2-tam-10.1177_17588359261458300 for Adebrelimab-based regimens as first-line treatment for ES-SCLC in specific populations: a real-world study in Chinese patients by Liyang Jiang, Junxu Wen, Shuangbing Xu, Ling Meng, Nailiang Zhai, Zhenyu Shao, Peizhu Wu, Kaikai Zhao, Lingling Kong, Jianfeng Peng, Zhaoqin Huang and Xiangjiao Meng in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-1-tam-10.1177_17588359261458300 – Supplemental material for Adebrelimab-based regimens as first-line treatment for ES-SCLC in specific populations: a real-world study in Chinese patients
Supplemental material, sj-jpg-1-tam-10.1177_17588359261458300 for Adebrelimab-based regimens as first-line treatment for ES-SCLC in specific populations: a real-world study in Chinese patients by Liyang Jiang, Junxu Wen, Shuangbing Xu, Ling Meng, Nailiang Zhai, Zhenyu Shao, Peizhu Wu, Kaikai Zhao, Lingling Kong, Jianfeng Peng, Zhaoqin Huang and Xiangjiao Meng in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to acknowledge the patients and their families, the study investigators, and the clinical site staff. We thank Wenqing Zhu (Department of Medical Affairs, Jiangsu Hengrui Pharmaceuticals Co., Ltd.) for statistical support, Yunning Yang (Department of Medical Affairs, Jiangsu Hengrui Pharmaceuticals Co., Ltd.) for medical writing assistance; Kangle Zhu (Department of Medical Affairs, Jiangsu Hengrui Pharmaceuticals Co., Ltd.) for data interpretation.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.