
Abstract
Background:
Determining an optimal treatment strategy after tyrosine kinase inhibitor (TKI) failure remains challenging in oncogene-driven non-small cell lung cancer (NSCLC).
Objectives:
We aimed to evaluate and compare the efficacy and safety of atezolizumab, bevacizumab, carboplatin, and paclitaxel (ABCP) versus pemetrexed plus carboplatin or cisplatin (PC) in patients with progressive NSCLC harboring EGFR, ALK, or ROS1 alterations after TKI failure.
Design:
Multicenter retrospective study.
Methods:
We analyzed 114 patients with NSCLC treated with either ABCP (n = 48) or PC (n = 66) post-TKI failure between November 2016 and July 2023. Treatment response, progression-free survival (PFS), overall survival (OS), and safety profiles were assessed.
Results:
Among 106 evaluable participants, the ABCP arm demonstrated a higher response rate (50.0%) than the PC arm (35.0%). During the median follow-up of 29.9 months, PFS was significantly prolonged in the ABCP arm compared with that in the PC arm (7.3 vs 3.0 months, respectively; hazard ratio (HR) 0.643; p = 0.026), whereas OS showed no significant difference (p = 0.165). Subgroup analysis revealed notable improvements in PFS (7.2 vs 2.1 months, HR 0.235; p < 0.001) and OS (11.0 vs 4.1 months, HR 0.418; p = 0.001) in patients with three or more metastatic sites.
Conclusion:
ABCP significantly improved PFS compared with PC in patients with NSCLC that progressed despite prior TKI therapy. An OS benefit was observed in patients with three or more metastatic sites.
Plain language summary
Why was this study done? Many patients with non-small cell lung cancer (NSCLC) have specific genetic alterations (mutations like EGFR, ALK, or ROS1). The standard first line treatment for this population is targeted therapy. However, many patients discontinue these drugs because cancer eventually gains resistance to the target therapy. There are unmet needs for patients whose target therapies are exhausted since there are no guideline for subsequent treatment. What did the researchers do? This study compared the effectiveness of two different chemotherapy combinations for patients whose cancer grew after taking targeted pills. The researchers retrospectively analyzed data from 114 patients treated between 2016 and 2023. The patients received either: ABCP: A four-drug combination of atezolizumab (immunotherapy), bevacizumab (anti-VEGF therapy), paclitaxel, and carboplatin (cytotoxic chemotherapy) PC: A two-drug cytotoxic chemotherapy regimen (pemetrexed plus carboplatin). What were the results? The study found that the four-drug combination (ABCP) was more effective at controlling the cancer: Delayed Growth: On average, patients on ABCP went 7.3 months before their cancer started growing again, compared to only 3.0 months for those on PC. Tumor Shrinkage: Tumors shrank in 50% of patients taking ABCP, compared to 35% of patients taking PC. Survival: While the overall survival time was similar for both groups, patients with more widespread cancer (spread to 3 or more sites) lived significantly longer if they received the ABCP treatment. What do these findings mean? For patients with NSCLC whose targeted therapy has been exhausted, using the ABCP combination appears to keep the cancer under control significantly longer than PC. It may be a particularly good option for patients whose cancer has spread to multiple parts of the body.
Introduction
Advancements in understanding the oncogenic activation of specific tyrosine kinases in non-small cell lung cancer (NSCLC), particularly epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), and c-ros oncogene 1 (ROS1), have driven the development of targeted therapies. Tyrosine kinase inhibitors (TKIs) constitute standard first-line therapy for patients with NSCLC harboring EGFR, ALK, or ROS1 alterations. 1
The treatment landscape for oncogene-driven NSCLC has evolved substantially over the past decade. In patients with EGFR-mutated NSCLC, first-line osimertinib or lazertinib has become the standard of care based on its demonstrated survival benefit.2,3 Recently, combination therapy of lazertinib with amivantamab or osimertinib with cytotoxic chemotherapy has prolonged PFS and OS even further than monotherapy.4,5 Similarly, patients with ALK-rearranged NSCLC were typically treated with first- or second-generation ALK inhibitors, including crizotinib, alectinib, or lorlatinib6–8 in the first-line setting, while those with ROS1 rearrangements commonly received crizotinib. 9 After progression on these targeted agents, platinum-based chemotherapy with or without immunotherapy was frequently considered. Therefore, the present study reflects real-world treatment patterns in the era when third-generation TKIs were not universally accessible as first-line therapy.
Although TKIs significantly prolong survival, acquired resistance remains inevitable. In most cases of disease progression, platinum-based doublet chemotherapy is the standard treatment, albeit with a dismal prognosis.10–12 Consequently, identifying effective therapeutic strategies for patients with NSCLC experiencing progression even after TKI therapy remains a critical challenge.
Programmed cell death 1 (PD-1) and programmed death ligand 1 (PD-L1) checkpoint inhibitors, in combination with platinum-doublet chemotherapy, improve survival in patients with advanced non-squamous NSCLC lacking EGFR or ALK alterations.13,14 Additionally, clinical studies have demonstrated synergistic effects between immune checkpoint inhibitors and anti-angiogenesis therapy targeting the vascular endothelial growth factor (VEGF) signaling pathway. 15 The landmark IMpower150 trial reported significant improvements in progression-free survival (PFS) and overall survival (OS) with atezolizumab (an anti-PD-L1 monoclonal antibody) combined with bevacizumab (an anti-VEGF monoclonal antibody), carboplatin, and paclitaxel in chemotherapy-naive patients with non-squamous NSCLC, irrespective of PD-L1 expression or oncogenic driver mutations. 16 In contrast, the KEYNOTE-789 (NCT03515837) and CheckMate-722 (NCT02864251) trials, which evaluated PD-1 inhibitors combined with chemotherapy versus chemotherapy alone in patients with disease progression after prior EGFR-TKI therapy, failed to demonstrate a survival benefit.17,18 These conflicting trial outcomes highlight the need to define the role of immunotherapy combined with VEGF inhibitors and cytotoxic chemotherapy in patients with oncogenic driver mutations who experience disease progression despite receiving targeted therapy.
Therefore, this study was aimed at evaluating the efficacy and safety of atezolizumab combined with bevacizumab, carboplatin, and paclitaxel (ABCP) compared with pemetrexed and carboplatin or cisplatin (PC) in patients with metastatic NSCLC harboring EGFR, ALK, or ROS1 alterations, whose disease progressed despite prior TKI therapy.
Materials and methods
Patients
The aim of this multicenter, retrospective study was to compare the overall response and survival outcomes in patients with NSCLC harboring EGFR, ALK, or ROS1 alterations. Patients with stage IV NSCLC harboring EGFR, ALK, or ROS1 alterations treated with ABCP or PC therapy at four academic institutions between November 2016 and July 2023 were enrolled in this study. Patients who experienced cancer progression despite prior therapy with one or more TKIs targeting EGFR, ALK, or ROS1 were deemed eligible. Patients who had received cytotoxic chemotherapy, immunotherapy, or anti-angiogenic therapy before the initiation of ABCP or PC therapy were excluded from the study. The patients’ clinical data at the time of NSCLC diagnosis and the initiation of ABCP or PC therapy, including sex, age, smoking history, Eastern Cooperative Oncology Group (ECOG) performance status, oncogenic driver mutations (EGFR, ALK, or ROS1), sites of metastasis, and previous treatments, were obtained from the medical records. This multicenter retrospectively included patients treated at four centers in South Korea: Yonsei Cancer Center, Gangnam Severance Hospital, CHA Bundang Medical Center, and Asan Medical Center. This study adhered to the ethical principles of the Declaration of Helsinki and received approval from the Institutional Review Board (IRB) of each participating institution. The requirement for written informed consent was waived. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 19 The completed STROBE checklist is provided as Supplemental File.
Response and safety evaluation
Patients received ABCP or PC therapy every 21 days. The dosing schedules were generally informed by the treatment regimen reported in the Impower150 study, while dose modifications were implemented according to physician discretion and the patient’s clinical condition in routine practice. In routine clinical practice, patients typically receive four to six cycles of induction chemotherapy, followed by maintenance therapy when clinically appropriate. For patients receiving ABCP, maintenance therapy consisted of atezolizumab and bevacizumab, whereas pemetrexed maintenance was used in the PC group. Treatment exposure was further evaluated by analyzing the number of treatment cycles and initial dose intensity. When dose reductions differed among agents, we calculated relative dose intensity based on paclitaxel in the ABCP group, and pemetrexed in the PC group, as carboplatin dosing is determined by creatinine levels, and thus dose modifications are more likely to be guided by the cytotoxic agents in routine clinical practice. Treatment was discontinued in case of intolerable toxicity or disease progression. Treatment responses were evaluated clinically at each institution using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and classified as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The objective response rate (ORR) was defined as the percentage of patients achieving CR or PR, whereas the disease control rate (DCR) included patients with CR, PR, or SD. All radiologic images were retrospectively reviewed and reassessed by two independent investigators who were not directly involved in the patients’ clinical management. Responses were determined based on available imaging studies to ensure consistent application of RECIST criteria across participating institutions. Baseline physical examinations, laboratory tests, and toxicity assessments were performed before treatment initiation and repeated before each cycle. Treatment-emergent adverse events (TEAEs) were documented throughout treatment and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.0. For adverse events without explicitly recorded CTCAE grades, grade⩾3 TEAEs were operationally defined as events requiring hospitalization, urgent medical intervention, or permanent discontinuation of systemic therapy, consistent with CTCAE grade 3 or higher severity. Subjective adverse events such as fatigue or peripheral neuropathy were included only when clearly documented by the treating physicians and were graded conservatively based on the clinical impact. The data collection cutoff date for the analysis was August 31, 2024.
Statistical analysis
Categorical variables were summarized as counts and percentages, and differences between groups were assessed using the χ 2 test. Continuous variables were expressed as means with standard deviations (SD) and compared using the independent t-test. PFS was defined as the time from treatment initiation to either disease progression or death, whereas OS was defined as the time from treatment initiation to death from any cause. PFS and OS outcomes were estimated using the Kaplan–Meier method, and subgroup differences were evaluated using the log-rank test. The median follow-up time was estimated using the reverse Kaplan–Meier method. A Cox proportional hazards regression model was generated to calculate hazard ratios (HRs) with 95% confidence intervals (CIs) for survival analysis. Two-tailed p-values < 0.05 were considered statistically significant. All statistical analyses and data visualization were conducted using GraphPad Prism (version 8.0, GraphPad Software) and SPSS (version 23.0, SPSS Inc.).
Results
Patient characteristics
A total of 114 patients were enrolled in this study, 48 of whom received ABCP and 66 received PC (Table 1). The patients’ median age was 62 years (range, 38–83 years). The majority of patients were women (62.3%) and nonsmokers (67.5%). Approximately one-quarter of the cohort had an ECOG performance status of 2 or 3, a higher proportion than those reported in previous prospective20–23 and retrospective studies24–26 (Supplemental Table 1). EGFR mutations were the most prevalent, detected in 107 patients (93.9%), followed by ALK rearrangements (4.4%) and ROS1 rearrangements (1.8%). Brain metastases were identified in 38 patients (33.3%), whereas liver metastases were present in 22 (19.3%) patients. Detailed characteristics of patients with EGFR mutation were described in Supplemental Table 2. Specifically, among 17 patients with confirmed T790M mutation, most received either osimertinib or lazertinib. Two patients did not receive third-generation EGFR TKIs because they died before osimertinib became available in Korea. The distribution of EGFR mutation subtypes (Supplemental Table 3) and metastatic burden (Supplemental Table 4) were comparable between the ABCP and PC groups. The majority of patients (63.2%) received ABCP or PC as second-line therapy.
Baseline characteristics of the patients.
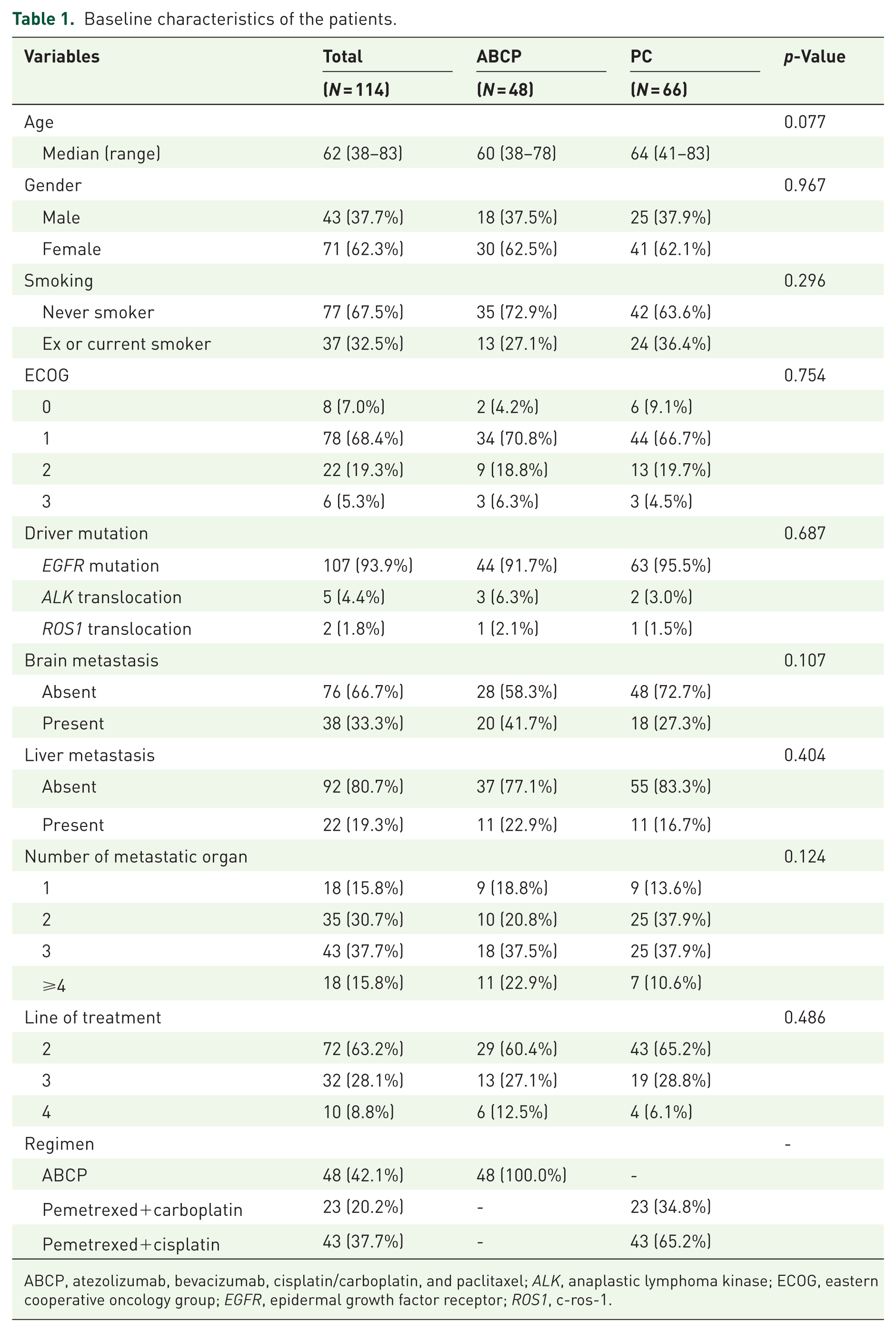
ABCP, atezolizumab, bevacizumab, cisplatin/carboplatin, and paclitaxel; ALK, anaplastic lymphoma kinase; ECOG, eastern cooperative oncology group; EGFR, epidermal growth factor receptor; ROS1, c-ros-1.
Response
Treatment response was assessed in 106 patients: 46 in the ABCP arm and 60 in the PC arm. The ORR was 50.0% (95% CI: 35.0–65.0%) in the ABCP arm and 35.0% (95% CI: 22.6–47.4%) in the PC arm (p = 0.120; Figure 1(a)). The DCRs were 87.0% (95% CI: 76.8–97.1%) and 75.0% (95% CI: 63.7–86.3%) in the ABCP and PC arms, respectively (p = 0.126; Figure 1(b)). Tumor shrinkage was achieved in 87.0% of patients receiving ABCP and 65.0% of those receiving PC (p = 0.010; Figure 1(c)). Consequently, based on the RECIST criteria, the reduction in the sum of the target lesions was significantly higher in the ABCP arm than in the PC arm (mean tumor reduction: −26.8% vs −12.8%, p = 0.041).
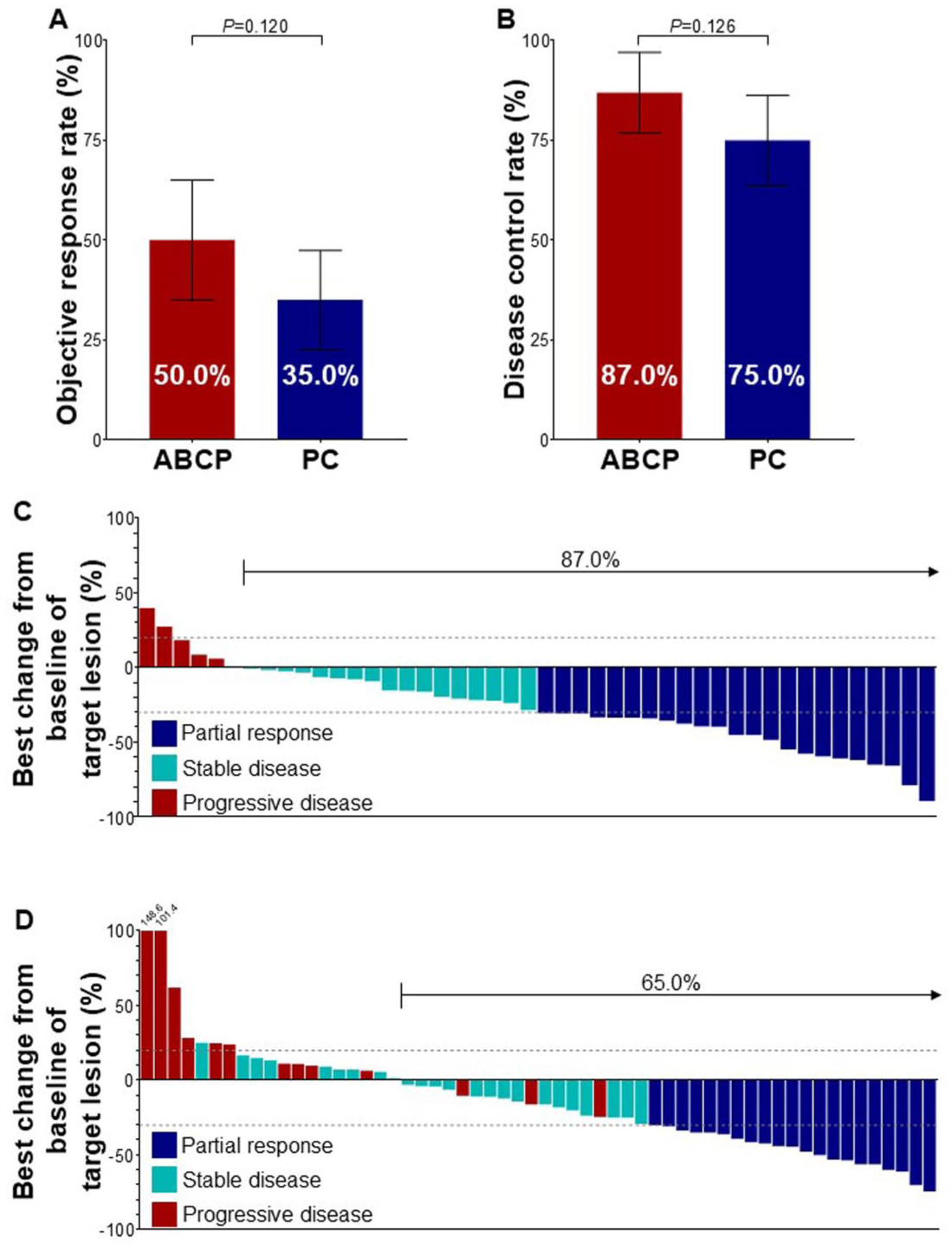
Efficacy of ABCP and PC based on the treatment. (a) Objective response rate. (b) Disease control rate. (c) Waterfall plot showing the individual treatment responses in patients treated with ABCP. (d) Waterfall plot showing the individual treatment responses in patients treated with PC.
Survival
The median follow-up time, estimated using the reverse Kaplan–Meier method, was 29.9 months (95% CI: 27.7-not reached) in the overall population. The median follow-up time was 30.1 months (95% CI: 28.6-not reached) in the ABCP group, and 25.0 months (95% CI: 22.7–not reached) in the PC group. During the follow-up periods, cancer progression and mortality were documented in 108 and 97 patients, respectively. The median PFS was 7.3 months (95% CI: 4.3–10.3 months) in the ABCP arm and 3.0 months (95% CI: 1.4–4.6 months) in the PC arm (Figure 2(a)), with an HR of 0.643 (95% CI: 0.436–0.949, p = 0.026). The 6-month PFS rates were 56.1% for ABCP and 34.8% for PC, whereas the 12-month PFS rates were 25.9% and 9.2%, respectively. The median OS was 10.6 months (95% CI: 7.5–13.7 months) in the ABCP arm and 7.2 months (95% CI: 4.5–10.0 months) in the PC arm (Figure 2(b)), with an HR of 0.750 (95% CI: 0.499–1.128, p = 0.165). The 6-month OS rates were 75.0% for the ABCP arm and 59.0% for the PC arms, whereas the respective 12-month OS rates were 45.0% and 33.8%. Overall, ABCP demonstrated a significant advantage over PC in terms of PFS, whereas the difference in OS was not statistically significant.
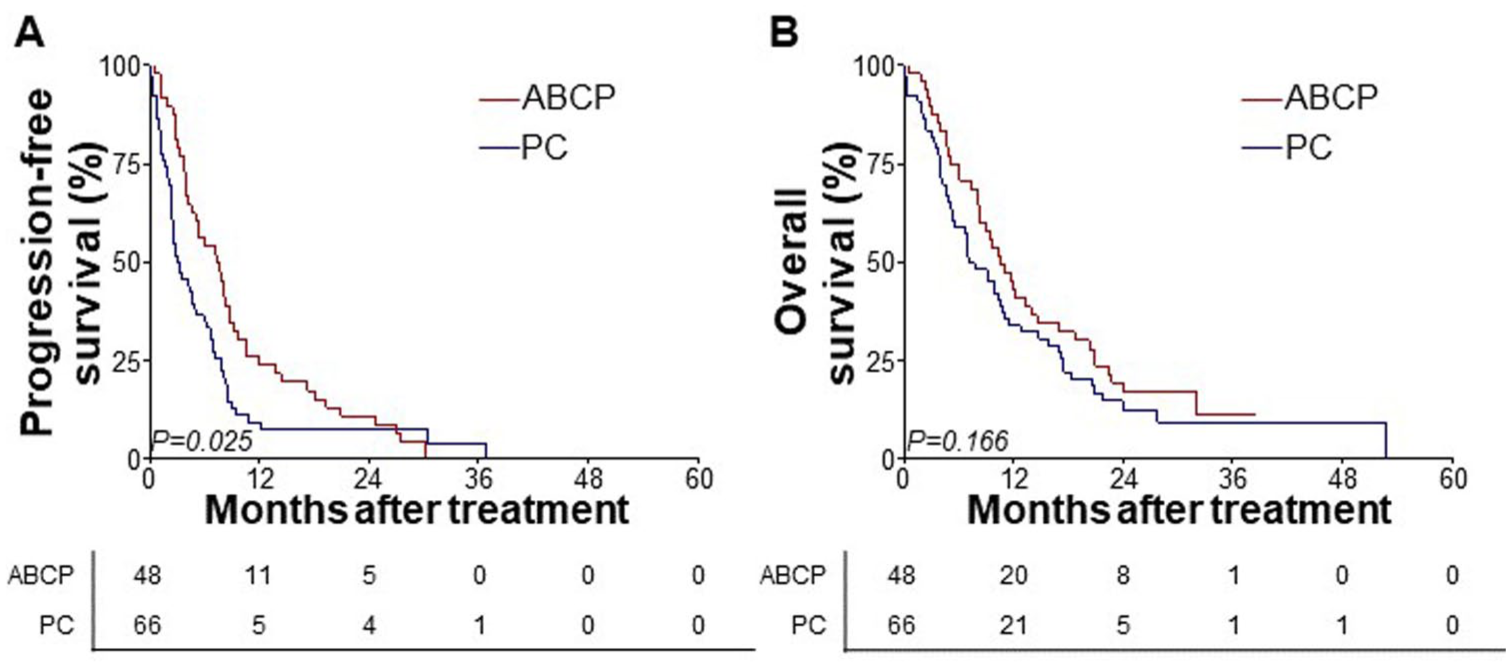
Survival outcomes based on the treatment. (a) Kaplan–Meier plot of progression-free survival. (b) Kaplan–Meier plot of overall survival.
Subgroup analysis by metastatic organs
Subgroup analyses were performed to explore whether the treatment effect differed according to baseline clinical characteristics (Figure 3(a) and (b)) The treatment effect of ABCP versus PC was generally consistent across most clinical subgroups, including age, sex, smoking status, ECOG performance status, driver mutation type, presence of brain or liver metastases, and line of previous therapy, with no significant interaction observed (all interaction p > 0.05). Furthermore, when the number of metastatic organs was modeled as a continuous variable in a Cox hazards model, each additional metastatic organ was associated with a significantly increased risk of progression in the overall population (HR, 1.53; 95% CI, 1.25–1.88; p < 0.001), and death (HR, 1.60; 95% CI, 1.29–1.99; p < 0.001). Among patients with metastases at three or more sites at treatment initiation, both PFS (Figure 3(c)) and OS (Figure 3(d)) were significantly longer in the ABCP arm than in the PC arm (7.1 vs 2.2 months, p < 0.001 for PFS, 10.8 vs 4.1 months, p = 0.001 for OS). Among patients with one or two metastatic sites, PFS and OS (7.7 vs 6.8 months, p = 0.500 for PFS, 9.2 vs 15.5 months, p = 0.521 for OS) did not differ significantly between the treatment arms (Supplemental Figure 1(a) and (b)). When alternative cutoffs for metastatic burden were applied, the PFS benefit of ABCP remained consistently greater in patients with higher metastatic burden (Supplemental Figure 2(a) and (b)).

Subgroup analysis. (a) Forest plot of progression-free survival. (b) Forest plot of overall survival. (c) Kaplan–Meier plot of progression-free survival in patients with three or more metastatic sites. (d) Kaplan–Meier plot of overall survival in patients with three or more metastatic sites.
Exploratory subgroup analyses stratified by EGFR mutation subtype (Exon 19 deletion, L858R, and uncommon mutations) showed a generally consistent pattern with the overall cohort, with numerically longer PFS observed in the ABCP group across mutation subtypes (Supplemental Figure 3(a)–(h)).
Treatment exposure
Treatment exposure according to treatment group is summarized in Supplemental Table 5. The median number of treatment cycles was higher in the ABCP group than in the PC group (8.5 (IQR, 3–15.5) vs 5 (IQR, 2–10); p = 0.028). The mean initial dose intensity was lower in the ABCP group compared with the PC group (90.1% (SD, 13.74) vs 96.8% (SD, 9.23); p = 0.004). Initial dose reduction at treatment initiation occurred more frequently in the ABCP group than in the PC group. (37.5% vs 12.1%; p = 0.0028).
Safety
TEAEs were reported in 97.4% of the patients (Table 2). Grade 3 or higher TEAEs occurred in 52.1% of patients in the ABCP arm and 42.4% of those in the PC arm. Overall, TEAEs were more frequent in patients receiving ABCP than in those receiving PC, except for edema (10.4% vs 25.8%, p = 0.040). Endocrinopathies (hypothyroidism and adrenal insufficiency), skin toxicities (pruritus and skin rash), bleeding events (hemoptysis and epistaxis), thromboembolic events, and hypertension were significantly more frequent in the ABCP arm. In the ABCP arm, the most prevalent TEAEs were anemia (89.6%), constipation (75.0%), and lymphopenia (66.7%), whereas anemia (92.4%), lymphopenia (50.0%), and nausea (42.4%) were observed most frequently in the PC arm. The most common grade 3/4 TEAEs included lymphopenia (31.3%), neutropenia (25.0%), and febrile neutropenia (14.6%) in the ABCP arm and lymphopenia (19.7%), anemia (12.1%), and neutropenia (9.1%) in the PC arm. No treatment-related deaths were reported in either group.
Treatment-emergent adverse events.

ABCP, atezolizumab, bevacizumab, cisplatin/carboplatin, and paclitaxel; PC, pemetrexed and cisplatin/carboplatin.
Discussion
The treatment landscape of oncogene-driven NSCLC has evolved rapidly with the development of TKIs, leading to improved clinical outcomes. However, despite these advances, acquired resistance to targeted therapy remains inevitable in most patients and optimal subsequent treatment strategies remain an area of active investigation.
The aim of this multicenter study was to assess the efficacy and safety of ABCP compared with PC in patients with NSCLC harboring EGFR, ALK, or ROS1 alterations and acquired resistance to prior TKI therapy. ABCP was associated with a significant improvement in PFS, whereas no OS benefit was observed. TEAEs occurred more frequently in the ABCP arm than in the PC arm. Notably, the incidence of grade ⩾3 TEAEs tended to be higher in the ABCP group compared with the PC group (52% vs 42%). This finding underscores the clinical trade-off: improved disease control and prolonged PFS may come at the cost of increased toxicity. These results align with those of the phase III ATTLAS (NCT03991403) 21 and ORIENT-31 (NCT03802240) 22 trials, which demonstrated superior PFS outcomes but no OS with ABCP over platinum-doublet chemotherapy after TKI failure. Taken together, our results provide real-world evidence supporting the role of ABCP in this setting, while underscoring the importance of careful patient selection and toxicity monitoring.
Preclinical and clinical studies have consistently demonstrated the synergistic interaction between anti-angiogenic agents and immune checkpoint inhibitors. 15 A phase II study (NCT03971474; Lung-MAP S1800A study) comparing pembrolizumab plus ramucirumab versus standard-of-care treatment showed a significant OS benefit and a prolonged tail in the PFS curve for the pembrolizumab plus ramucirumab arm. 27 Various combination strategies have been explored owing to the poor prognosis of NSCLC after TKI failure. For instance, the ATTLAS study evaluated atezolizumab plus bevacizumab and chemotherapy in patients with EGFR- or ALK-mutated NSCLC, showing a significant PFS benefit with ABCP over PC. 21 Similarly, the phase III ORIENT-31 trial reported prolongation of PFS with sintilimab, an anti-human PD-1 monoclonal antibody, when administered either as monotherapy or in combination with bevacizumab biosimilar (IBI305) plus chemotherapy. 22 These findings highlight the clinical significance of combining anti-angiogenic agents with checkpoint inhibitors. In contrast, trials evaluating PD-1 inhibitors with chemotherapy such as CheckMate-722 17 and KENOTE-789 18 trials, failed to demonstrate survival benefits. This underscores the synergistic effect of anti-VEGF(R) and anti-PD-L1 antibodies in NSCLC treatment.
In our exploratory subgroup analysis, the survival benefit of ABCP appeared to be more pronounced in patients with ⩾3 metastatic sites. The cutoff has been used in previous studies evaluating tumor burden from FLAURA2 study, which suggested greater benefit from intensified systemic therapy with osimertinib plus chemotherapy in patients with ⩾3 metastatic sites. 28 Notably, patients in the ABCP group tended to have a higher metastatic burden at treatment initiation suggesting that the observed benefit was unlikely to be explained by more favorable baseline disease characteristics. Although treatment patterns such as dose reduction and cycle number varied in routine clinical practice, the lower initial dose intensity and more frequent dose reduction in the ABCP group suggest that these differences are unlikely to fully account for the observed survival benefit. Given that ABCP was not reimbursed during the study period, its use may have been influenced by physician judgment and patient-related factors.
Previous studies have suggested that liver metastases are associated with reduced infiltration of CD8+ T cells in patients with NSCLC lacking EGFR mutations. 29 In contrast, other studies have reported upregulation of CD8+ T cell infiltration after TKI treatment. 30 In our study, ABCP demonstrated a consistent PFS benefit, irrespective of liver or brain metastasis, aligning with previous studies. 29 Subgroup analyses revealed that patients with a higher tumor burden derived greater survival benefits from ABCP. A higher tumor burden has traditionally been associated with poor outcomes after immune checkpoint inhibitor therapy.31,32 These findings suggest that the combination of PD-L1 and VEGF inhibition may help overcome the adverse impact of high tumor burden, warranting further investigation.
Ivonescimab (SMT112/AK112), a bispecific PD-1/VEGF antibody, has demonstrated promising efficacy in patients with NSCLC in early-phase clinical trials (NCT04047290 and NCT04900363).33,34 In a pivotal phase III randomized trial (HARMONi-A, NCT06396065), ivonescimab combined with chemotherapy significantly improved PFS and OS in patients with advanced NSCLC who had progressed after prior EGFR-TKI therapy, along with a higher ORR compared with chemotherapy alone.35,36 This dual-targeting approach holds promise in improving both antitumor immunity and vascular normalization in oncogene-driven NSCLC, requiring further validation in real-world settings.
Although ABCP was associated with improved PFS, this did not translate into a significant OS benefit. One possible explanation is the impact of subsequent therapies administered after disease progression. In real-world setting, limited treatment options after progression on ABCP may have influenced treatment sequencing, thereby attenuating potential OS differences despite earlier disease control.
Re-evaluation of tumor molecular status may also be considered after progression on targeted therapy. Liquid biopsy including circulating tumor DNA analysis, provides a non-invasive approach to capture tumor evolution and may help identify actionable alterations following TKI failure. 37 However, its clinical utility in guiding treatment selection in this setting requires further validation.
In interpreting these findings, potential confounding factors inherent to retrospective studies should be considered. During the study period, first-line osimertinib and lazertinib were not reimbursed in Korea. Consequently, most patients with EGFR mutations received first- or second- generation EGFR TKIs, such as gefitinib or afatinib, as initial therapy, except in cases with confirmed T790M-mediated resistance. Furthermore, during the study period in Korea, pemetrexed based chemotherapy was reimbursed, whereas ABCP regimen was not covered by national insurance system. Consequently, treatment selection was influenced not only by clinical considerations but also by reimbursement status and patient access to self-funded therapies. This real-world reimbursement environment should be considered when interpreting comparative outcomes between treatment groups.
Several limitations of this study should be acknowledged. First, this was a retrospective multicenter analysis, which is inherently subject to potential selection bias and unmeasured confounding. In particular, treatment allocation was not randomized and may have been influenced by both clinical factors and reimbursement status, as ABCP was not reimbursed during the study period. Second, detailed treatment exposure data, such as dose intensity and subsequent treatment, were not consistently available across institutions, which may have affected comparisons of treatment outcomes. Third, the study population consisted predominantly of EGFR-mutated NSCLC, with only a small number of ALK-, and ROS1- rearranged cancers. Therefore, findings of this study should be interpreted cautiously.
In conclusion, ABCP improved PFS compared with PC in patients with non-squamous NSCLC after TKI therapy, without a corresponding OS benefit in the overall cohort. Notably, patients with three or more metastatic sites derived greater PFS and OS benefits with ABCP. These findings highlight the need to identify patient subgroups that may benefit from intensified treatment strategies, while emerging agents, including bispecific antibodies, may further improve outcomes in this setting.
Conclusion
This multicenter real-world study provides insight into treatment outcomes after TKI failure in oncogene-driven NSCLC. While ABCP was associated with improved PFS compared to PC, no significant OS difference was observed. These findings should be interpreted cautiously due to retrospective design and potential confounding factors. Nevertheless, they suggest that ABCP may be considered as a treatment option in selected patients with higher metastatic burden, particularly when treatment intensification is feasible.
Supplemental Material
sj-docx-2-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-docx-2-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-docx-3-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-4-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-jpg-4-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-5-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-jpg-5-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-6-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-jpg-6-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261458751 – Supplemental material for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure
Supplemental material, sj-pdf-1-tam-10.1177_17588359261458751 for Atezolizumab and bevacizumab plus chemotherapy versus chemotherapy in non-small cell lung cancer after tyrosine kinase inhibitor failure by Moonki Hong, Junho Choi, Seoyoung Lee, Yun Beom Sang, Min Hee Hong, Ja Hyun Yeo, Joo-Hang Kim, Shinkyo Yoon, Chang Gon Kim and Hye Ryun Kim in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We extend our gratitude to all patients and healthcare practices who contributed their data, enabling the successful completion of this research. The interpretation and conclusions drawn in this study are solely those of the authors.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.