
Abstract
Background:
Robust real-world evidence supporting the clinical utility of molecular classification in endometrial carcinoma (EC) remains limited.
Objectives:
To investigate the molecular classification-based personalized treatment decision-making for EC by presenting real-world data, including survival outcomes and failure patterns.
Methods:
This retrospective cohort study included patients with International Federation of Gynecology and Obstetrics (FIGO) stage I–III EC who underwent initial surgery and had available molecular classification at Peking Union Medical College Hospital, between December 2017 and April 2025. The primary endpoint was disease-free survival (DFS). We evaluated survival outcomes, visualized dynamic annual hazard rates (AHRs), and compared failure patterns across subgroups. Independent prognostic factors were identified using Cox regression analyses.
Results:
Between December 2017 and April 2025, 267 eligible patients were evaluated. The median age was 55 years, and the median follow-up was 31.10 months. NSMP was the most common molecular subtype (46.8%), followed by MMRd (27.7%), POLEmut (13.1%), and p53abn (12.4%). Endometrioid carcinoma G1-2 was the predominant histological type overall (74.5%). According to FIGO, the 2009 criteria, the stage distribution was as follows: IA (66.7%), IB (20.6%), II (4.5%), and III (12.2%). Restaging under the FIGO 2023 system resulted in upstaging in 20.2% and downstaging in 2.6% of patients. Most patients (56.6%) were classified as low-risk per the ESGO–ESTRO–ESP 2025 risk classification. Although observation alone was used in 45.7% of the entire cohort, intensified treatment was administered to 33.3% of the p53abn subgroup. Excellent 3-year overall survival (OS, 99.2%) and (DFS, 88.4%) were observed in the entire cohort. The p53abn group exhibited the highest recurrence rate (30.3%), frequently presenting as simultaneous multi-site recurrences. No recurrences were observed in the POLEmut group. The p53abn group exhibited the highest recurrence hazard rate (peak: 2.2% at 16.8 months), followed by the MMRd group (peak: 0.8% at 14.0 months) and the NSMP group (peak: 0.3% at 21.0 months). Both the ESGO–ESTRO–ESP 2025 risk classification and FIGO 2023 staging were independent prognostic factors for recurrence.
Conclusion:
This study provides evidence that molecular classification-based personalized treatment decision-making is feasible and can yield excellent survival outcomes in patients with stage I–III EC.
Introduction
Endometrial carcinoma (EC) is a prevalent gynecological malignancy globally and the second most common in China. 1 Traditionally, postoperative management has relied on clinicopathological factors such as age, histologic type, tumor grade, myometrial invasion, and lymphovascular space invasion (LVSI); however, despite standard treatments, approximately 15%–20% of patients remain at risk for recurrence.1–3 This highlights the critical need for more precise risk stratification.
To address this prognostic heterogeneity, molecular risk assessment has evolved from the initial comprehensive genomic characterization by the Cancer Genome Atlas (TCGA) 4 to clinically pragmatic methodologies like the ProMisE 5 and Trans-PORTEC classifiers. 6 These efforts established molecular classification: POLE ultramutated (POLEmut), mismatch repair-deficient (MMRd), p53 mutant (p53abn), and non-specific molecular profile (NSMP). Recognizing its prognostic and predictive value, recent major guidelines, including the 2023 International Federation of Gynecology and Obstetrics (FIGO) staging system as well as the 2025 European Society of Gynecologic Oncology (ESGO), European Society for Radiotherapy and Oncology (ESTRO), and the European Society of Pathology (ESP) guidelines, have formally integrated these molecular profiles to precisely tailor patient management.1,7–9
The clinical utility of molecular classification is strongly supported by the PORTEC trials. Retrospective analyses of PORTEC-1 and -2 revealed limited radiotherapy benefits in the MMRd group. 10 In the PORTEC-3 trial, molecular profiling identified high-risk patients who significantly benefited from chemoradiotherapy (CCRT) over radiotherapy alone (5-year recurrence‑free survival, RFS: 59% vs 36%, p = 0.019), whereas POLEmut patients exhibited excellent RFS without CCRT, highlighting the potential for treatment deescalation. 3 In light of the marked prognostic variations across molecular subgroups, personalized treatment strategies—including both intensified and deescalated approaches—should be considered. PORTEC-4a trial compared individualized adjuvant treatment based on a molecular-integrated risk profile with standard vaginal brachytherapy (VBT) in high-intermediate risk patients with EC.11,12 This study confirmed the safety and efficacy of molecular-integrated personalized treatment, notably allowing 46% of patients with favorable risk profiles to safely omit adjuvant therapy, thereby minimizing overtreatment. 12 Ongoing programs, such as the RAINBO trials, continue to refine these approaches. 13
Despite its inclusion in major guidelines and validation in clinical trials, a significant knowledge gap remains regarding the clinical utility and real-world performance of molecular classification in routine real-world settings. Clinical trials involve highly selected populations, and it remains unclear how molecular-integrated risk profiling translates into actual treatment decision-making, patient compliance, and outcomes in clinical practice. Furthermore, real-world evidence detailing specific failure patterns across molecular subgroups is particularly limited. Therefore, the objective of this study is to evaluate the real-world impact of molecular classification on adjuvant treatment decisions and to characterize the survival outcomes and recurrence patterns in a single-center retrospective cohort of EC patients.
Methods
Study population
Patients with newly diagnosed EC between Dec 2017 and April 2025 at Peking Union Medical College Hospital in China were retrospectively reviewed. The inclusion criteria were: (1) diagnosis of FIGO stage I–III EC, encompassing all histological subtypes (both endometrioid and non-endometrioid), with or without synchronous primary malignancies (synchronous endometrial and ovarian cancers); (2) underwent primary surgical treatment; and (3) availability of complete molecular classification profiling. Patients were excluded if they met any of the following criteria: (1) received neoadjuvant chemotherapy or fertility-sparing treatment; or (2) had incomplete clinical data, such as missing FIGO stage or adjuvant treatment records. Furthermore, regarding the determination of FIGO stage, lymph node status was assessed either surgically—via sentinel lymph node (SLN) biopsy or systematic pelvic/para-aortic lymphadenectomy according to institutional protocols and preoperative risk assessment—or radiologically via imaging evaluation for patients who did not undergo surgical nodal assessment. The clinical and pathological characteristics, including age, CA125 level before surgery, surgery information, pathological results, and adjuvant treatments, were collected. LVSI status was classified into four categories: negative, positive, focal, and extensive. Given peritoneal cytology as a potential prognostic factor, cytology results were also collected. The study was approved by Peking Union Medical College Hospital Review Board (Number I-24PJ2024) and complied with good clinical practice guidelines, the Declaration of Helsinki.
Molecular classification
Specimens for testing were obtained from tumor tissues via biopsy, curettage, or surgical resection. A cost-effective molecular classification procedure was performed prospectively (in real-time) immediately following tissue acquisition as part of standard clinical care by the Department of Pathology, Peking Union Medical College Hospital, China. Consequently, the molecular subtype results were available to the clinical team to inform adjuvant treatment decisions. Based on mismatch repair (MMR) and p53 protein testing, the genetic testing panel conducted a comprehensive evaluation of pivotal cancer-associated genes. The POLE gene analysis focused on the exonuclease domain (exons 3-14) and the partial region of exon 19. For the TP53 gene, the full coding region was sequenced. Furthermore, the panel incorporated an assessment of microsatellite instability (MSI) across 55 loci selected based on previously validated markers and methodological principles. 14
Molecular subtyping was performed according to the recommended sequential algorithm.7,15 First, POLE mutation status was assessed; tumors harboring a pathogenic POLE variant were classified as POLEmut. For tumors with wild-type POLE or non-pathogenic variants, MMR and MSI status were evaluated. Tumors exhibiting deficient MMR (dMMR) protein expression or high-frequency MSI (MSI-H) were classified as MMRd. In cases with proficient MMR (pMMR) or microsatellite stability (MSS, which included low-frequency MSI [MSI-L]), p53 status was subsequently assessed. Tumors demonstrating aberrant p53 protein expression or a TP53 mutation were classified as p53abn. Finally, tumors with wild-type p53 expression and a wild-type TP53 gene were classified as having NSMP.
Stage and risk classification
All eligible patients were staged according to the FIGO 2009, FIGO 2023, and molecular classification-integrated FIGO 2023 staging systems. For patients with stage I–II disease, the identification of p53abn or POLEmut resulted in upstaging (IICmp53abn) or downstaging (IAmPOLEmut), respectively. Patients were stratified into low-, intermediate-, high-intermediate-, high-, and uncertain-risk groups per the ESGO–ESTRO–ESP 2025 risk classification. The uncertain-risk group comprised patients with FIGO 2023 stage III–IVA disease harboring POLEmut, stage IA1/IC disease with NSMP (high-grade and/or estrogen receptor (ER)-negative), and stage IA1/IC disease with p53abn.
Adjuvant treatment
The general adjuvant treatment principles were based on ESGO–ESTRO–ESP 2016 (for patients treated prior to 2021) or ESGO–ESTRO–ESP 2021 (for patients treated in or after 2021) guidelines. In addition, the personalized adjuvant therapy strategy was collaboratively determined through a multidisciplinary approach, involving a senior gynecologist, radiation oncologist, and pathologist, based on integrated clinical, pathological, and molecular classification data. Specifically, treatment principles established by the multidisciplinary team were based on updated clinical guidelines incorporating clinicopathological features, patient tolerance, and molecular subtypes. Molecular classification played a direct and active role in guiding treatment deescalation or intensification. For example, deescalation (e.g., omitting adjuvant radiotherapy or chemotherapy) was strongly considered for patients with POLEmut profiles, even in the presence of conventional high-risk clinicopathological factors. In contrast, treatment intensification (e.g., adding systemic chemotherapy) was routinely recommended for patients with p53abn profiles, regardless of early-stage disease. For patients with MMRd or NSMP profiles, treatment decisions were primarily guided by traditional clinicopathological risk factors, with molecular status serving as a supplementary prognostic reference rather than a direct modifier of treatment choice. The adjuvant therapy modes were as follows: observation, VBT only, external beam radiotherapy (EBRT) only, EBRT + VBT, chemotherapy, as well as chemotherapy + EBRT/VBT.
Usually, radiotherapy starts within 6 or 8 weeks of surgery or is scheduled in relation to chemotherapy (1). The EBRT target encompassed the pelvic lymph node region, parametria, and upper vagina, delivered using intensity-modulated radiotherapy/volumetric modulated arc therapy techniques. The prescribed EBRT dose was 45–50.4 Gy, administered in 25–28 fractions at 1.8 Gy per fraction. VBT targeted the upper half of the vagina or the proximal 3–5 cm, delivered via a multichannel cylinder under computed tomography guidance. For VBT alone, the prescribed D90 dose was 20—30 Gy in 4–6 fractions using high‑dose‑rate brachytherapy. When VBT was administered following EBRT, the dose was 10 Gy delivered in 2 fractions.
Chemotherapy was part of the adjuvant regimen. Patients with aggressive histology, high-grade or extensive LVSI, or p53abn molecular subtype, or stage III were more likely to be recommended chemotherapy. The chemotherapy regimen consisted of paclitaxel (175 mg/m²) and carboplatin (AUC 5–6), administered intravenously every 21 days for a total of 4 to 6 cycles. Adjuvant chemotherapy was typically initiated within 4 to 6 weeks following primary surgery. Dose modifications or schedule delays were permitted based on individual patient tolerance, toxicities, and multidisciplinary team evaluations. The chemotherapy sequence relative to radiotherapy could be sequential or sandwiched.
Follow-up and survival outcome measures
Patients were notified regarding the necessity of long-term follow-up. A personalized follow-up strategy was recommended, with its implementation contingent upon molecular classification.16,17 Specifically, for low-risk patients (e.g., FIGO stage I/II with POLEmut), the follow-up interval was deescalated to every 6 months for the first 2 years, and annually thereafter up to 5 years. Conversely, for intermediate- to high-risk patients, the follow-up frequency was intensified (typically every 3 months for the first 2 years). Routine follow-up visits included physical and pelvic examinations, with imaging studies performed as clinically indicated.
The primary endpoint was disease-free survival (DFS). And the secondary endpoints were overall survival (OS), locoregional recurrence-free survival (LRFS), and distant metastasis-free survival (DMFS). OS was defined as the time interval from surgery to death or the last follow-up point. DFS was defined as the time interval from surgery to any recurrence, death, or last follow-up point. LRFS was defined as the time interval from surgery to the locoregional recurrence, death, or last follow-up time point. DMFS was defined as the time interval from surgery to distant metastasis, death, or the last follow-up time point.
Failure patterns
Recurrence sites were recorded and classified into the following categories: vaginal, pelvic, abdominal, distant, pelvic plus abdominal, pelvic plus distant, abdominal plus distant, and a combination of pelvic, abdominal, and distant. Locoregional recurrences were also evaluated. Lymph node (LN) recurrences were subclassified as locoregional, non-locoregional, or both. In addition, detailed failure patterns for individual patients were delineated.
Statistical analysis
The clinical and pathological features, FIGO stage distributions, risk classifications, as well as failure patterns, were described with descriptive statistics using frequencies and percentages for categorical data and median and range for continuous data. A Sankey plot was employed to visualize the transitions from the FIGO 2009 staging system to the FIGO 2023 staging system, FIGO stage 2023 with molecular classification, and the corresponding ESGO–ESTRO–ESP 2025 risk stratification. Survival outcomes were estimated using the Kaplan–Meier method. Pairwise comparisons between subgroups were performed using the Log-rank test, with p‑values adjusted by the Benjamini–Hochberg method. Univariable Cox regression analysis was performed to identify the prognostic factors for recurrence. To construct the multivariable Cox regression model, variable selection was guided by a hybrid approach integrating clinical rationale with statistical optimization. Crucially, established clinical prognosticators (age, FIGO stage) were forced into the model a priori. For the remaining covariates showing marginal significance in the univariable analysis (p < 0.2), a stepwise selection procedure was applied based on the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). 18 Ultimately, the final model successfully retained all clinically mandated variables alongside the statistically optimized covariates. Univariable and multivariable Cox regression analysis results were illustrated by a forest plot. Dynamic annual hazard rate (AHR) curves for recurrence or death were also depicted by the kernel smoothing method combined with the rstpm2 R package. All statistical analyses were performed using SPSS v. 26 (IBM Corp., Armonk, NY, USA) and R v. 3.5.1 (The R Foundation for Statistical Computing, Vienna, Austria). A 2-sided p value <0.05 was indicative of a statistically significant difference.
The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 19 (Supplemental STROBE statement).
Results
The clinical and pathological characteristics of enrolled patients
Initially, a total of 288 patients were screened for this study. Of these, 21 patients were excluded before the final cohort was defined (due to receiving neoadjuvant chemotherapy (n = 2), or fertility-sparing treatment (n = 9), or stage IV (n = 9), or stage information missing (n = 1)). Consequently, 267 eligible patients were enrolled in the final cohort. The screening procedure is presented in Figure 1. Table 1 details the clinical and pathological characteristics, along with adjuvant treatment information per molecular subgroup. The median diagnosis age for the whole cohort was 55 (range: 27–84) years. The most frequent molecular subtype was NSMP (n = 125, 46.8%), followed by MMRd (n = 74, 27.7%), POLEmut (n = 35, 13.1%), and p53abn (n = 33, 12.4%). Laparoscopic surgery accounted for the majority of procedures (83.1%). For lymph node assessment, combined para-aortic and pelvic lymph node dissection (LND) accounted for the highest proportion (41.6%). Notably, MMRd group presented higher proportions of lymph node metastasis (LNM) (8.1%). Histologically, low-grade (G1-2) endometrioid carcinoma (74.5%) was the most common type overall. Conversely, within the p53abn subgroup, high-grade (G3) endometrioid carcinoma (42.4%) was the most frequent. Regarding postoperative management, 45.7% of the entire cohort underwent observation alone. In contrast, patients in the p53abn group were more likely to receive intensified treatments. The regimens included chemotherapy combined with EBRT/VBT (33.3%), EBRT+/-VBT (21.2%), and chemotherapy alone (12.1%). Supplemental Table S1 shows the adjuvant therapy information per molecular subgroup and risk classifications.

The enrollment procedures of FIGO stage I–III endometrial patients with known molecular classification.
The clinical and pathological parameters per molecular subgroup in the retrospective cohort (n = 267).

Non-endometrioid carcinoma in our cohort included mixed carcinoma, undifferentiated carcinoma, mesonephric adenocarcinoma, serous carcinoma, clear cell carcinoma, and squamous cell carcinoma. In the POLE mutation subgroup, one patient had serous carcinoma. In the MMRd subgroup, there was one case of clear cell carcinoma, two of mixed carcinoma, and two of undifferentiated carcinoma. In the p53abn subgroup, there were three cases of serous carcinoma, two of squamous cell carcinoma, and one of clear cell carcinoma. In the NSMP subgroup, there were two cases of mixed carcinoma, two of undifferentiated carcinoma, and two of mesonephric adenocarcinoma.
CA125, cancer antigen; EBRT, external beam radiotherapy; ER, estrogen receptor; G, grade; LND, lymph node dissection; LNM, lymph node metastasis; LVSI, lymphovascular space invasion; MMRd, mismatch repair-deficient; NSMP, non-specific molecular profile; p53abn, p53 mutant; POLEmut, POLE ultramutated; SLN, sentinel lymph node; VBT, vaginal brachytherapy.
FIGO stage migrations and risk classifications
FIGO stage distributions and risk classifications of the whole cohort are shown in Table 2. Stage migrations are illustrated in Figure 2. Under the FIGO 2009 system, the vast majority of patients presented with early-stage disease, predominantly stage IA (66.7%) and IB (20.6%). The transition from the FIGO 2009 to the FIGO 2023 staging system resulted in notable stage migrations. Upstaging occurred in 20.2% of patients (n = 54), primarily driven by high-grade histology or p53abn (shifting patients to stage IIC/IICmp53abn), as well as extensive LVSI. Conversely, 2.6% of patients (n = 7) were downstaged to stage IAmPOLEmut. According to the ESGO–ESTRO–ESP 2025 risk classification, most patients (56.6%) were categorized as low-risk. However, four patients were classified as having uncertain risk, including one case of stage IIIA1 with POLEmut, and three early-stage cases (IA1 or IC) with p53abn.
Stage distribution and risk classification.
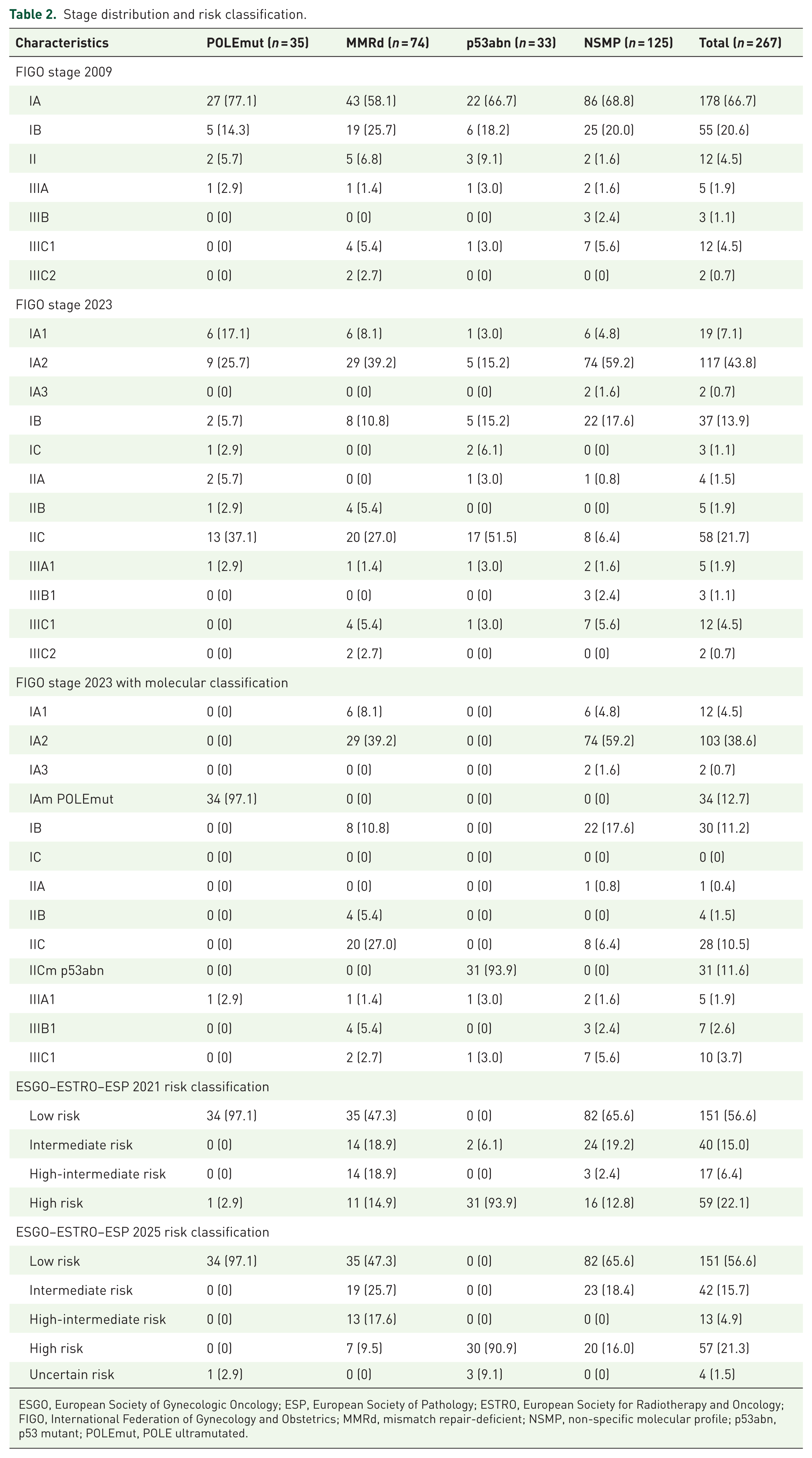
ESGO, European Society of Gynecologic Oncology; ESP, European Society of Pathology; ESTRO, European Society for Radiotherapy and Oncology; FIGO, International Federation of Gynecology and Obstetrics; MMRd, mismatch repair-deficient; NSMP, non-specific molecular profile; p53abn, p53 mutant; POLEmut, POLE ultramutated.
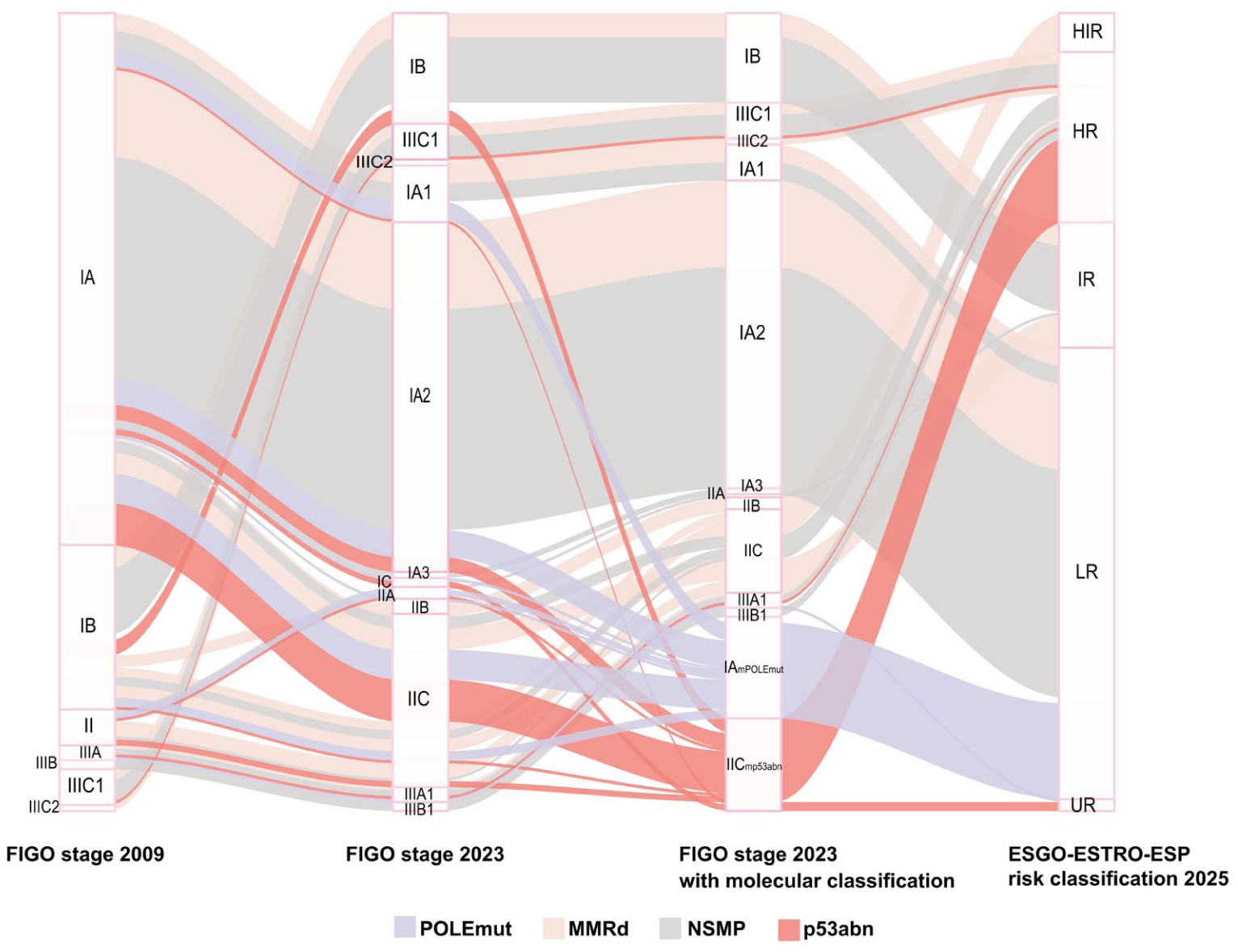
Sankey plot about FIGO stage migrations and ESGO–ESTRO–ESP 2025 risk classification.
Survival outcomes
Figure 3 presents the survival outcomes for the entire cohort. The median follow-up time was 31.10 months (95% CI: 30.00–33.37 months). Among all patients, 2 died, 27 experienced disease progression, 16 had locoregional recurrences, and 24 developed distant metastases. The 3-year survival rates were as follows: 99.2% (95% CI: 0.98–1.00) for OS, 88.4% (95% CI: 0.84–0.93) for DFS, 93.4% (95% CI: 0.90–0.97) for LRFS, and 89.6% (95% CI: 0.86–0.94) for DMFS.
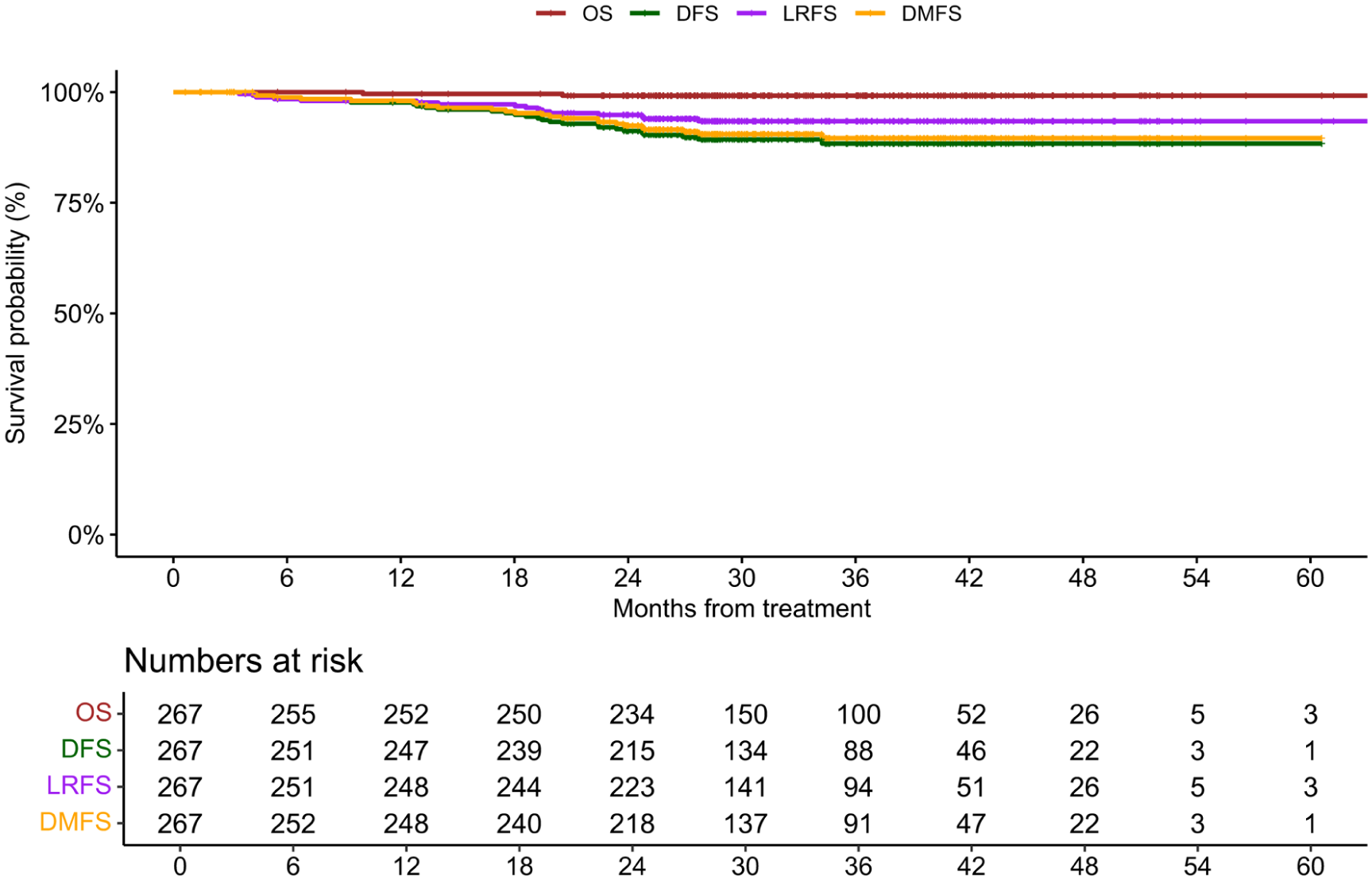
Survival outcomes for the entire cohort (n = 267).
Figure 4 shows the survival outcomes across molecular subgroups. The 3-year OS rate was 93.7% (95% CI: 0.86–1.00) in the p53abn subgroup and 100.0% in the other molecular subgroups. A statistically significant difference in OS was observed between the p53abn and NSMP groups (adjusted p = 0.034), while no significant OS differences were found among the remaining groups (all adjusted p > 0.05).

Survival outcomes for POLEmut, MMRd, NSMP, and p53abn subgroups. (a) OS. (b) DFS. (c) LRFS. (d) DMFS.
The 3-year DFS rates were: 100.0% in the POLEmut group, 87.2% (95% CI: 0.80–0.95) in the MMRd group, 97.2% (95% CI: 0.87–0.98) in the NSMP group, and 65.6% (95% CI: 0.50–0.86) in the p53abn group. Significant differences in DFS were identified between the p53abn group and the POLEmut (adjusted p = 0.001), MMRd (adjusted p = 0.040), and NSMP groups (adjusted p < 0.001).
For LRFS, the 3-year rates were: 100.0% in the POLEmut group, 91.5% (95% CI: 0.85–0.98) in the MMRd group, 95.7% (95% CI: 0.92–0.99) in the NSMP group, and 81.6% (95% CI: 0.68–0.98) in the p53abn group. Comparisons between the p53abn group and the POLEmut or NSMP groups showed borderline significance (adjusted p = 0.0536 for both). No other significant differences in LRFS were observed among the groups.
The 3-year DMFS rates were 100.0% in the POLEmut group, 90.0% (95% CI: 0.83–0.97) in the MMRd group, 92.9% (95%CI: 0.88–0.98) in the NSMP group, and 65.6% (95% CI: 0.50–0.86) in the p53abn group, respectively. Significant differences in DMFS were found between the p53abn group and the POLEmut (adjusted p = 0.001), MMRd (adjusted p = 0.010), and NSMP groups (adjusted p < 0.001).
The impact of adjuvant treatment modalities and risk classification on survival outcomes varied across molecular subgroups. As detailed in Supplemental Table S2, no recurrence or death events were observed in the POLEmut group. Within the MMRd subgroup, no significant survival differences were identified among patients receiving different adjuvant treatments or stratified by the ESGO–ESTRO–ESP 2025 risk classification (p > 0.05). In contrast, for the NSMP subgroup, survival outcomes significantly differed according to both adjuvant treatment and ESGO–ESTRO–ESP 2025 risk classification (p < 0.05). Patients who received chemotherapy with or without radiotherapy showed inferior survival compared to those under observation, specifically in terms of DFS (HR: 24.23, 95% CI: 2.64–222.4, p = 0.005) and DMFS (HR: 16.27, 95% CI: 1.67–158.7, p = 0.016). In addition, chemotherapy alone was associated with worse outcomes in DFS, LRFS, and DMFS compared to observation (all p < 0.05). Furthermore, significant differences in DFS, LRFS, and DMFS were observed across risk categories, suggesting that the ESGO–ESTRO–ESP 2025 risk classification may serve as a useful prognostic tool for the NSMP subgroup. In the p53abn subgroup, a significant difference in LRFS was observed between high-risk and uncertain-risk patients (HR: 6.34, 95% CI: 1.04–38.66, p = 0.045).
Failure patterns
The failure patterns across molecular subgroups are presented in Table 3. Supplemental Table S3 details the individual recurrence profiles, salvage treatments, and clinical outcomes for the 27 patients. During the follow-up period, a total of 27 patients experienced recurrence. Overall, distant metastasis was the most frequent site for both the first and any recurrence, followed by combined multisite involvement (such as pelvic plus abdominal, or including distant sites). Nearly half of the recurrent cases (n = 13) involved LNM.
Failure patterns after treatment in different subgroups.
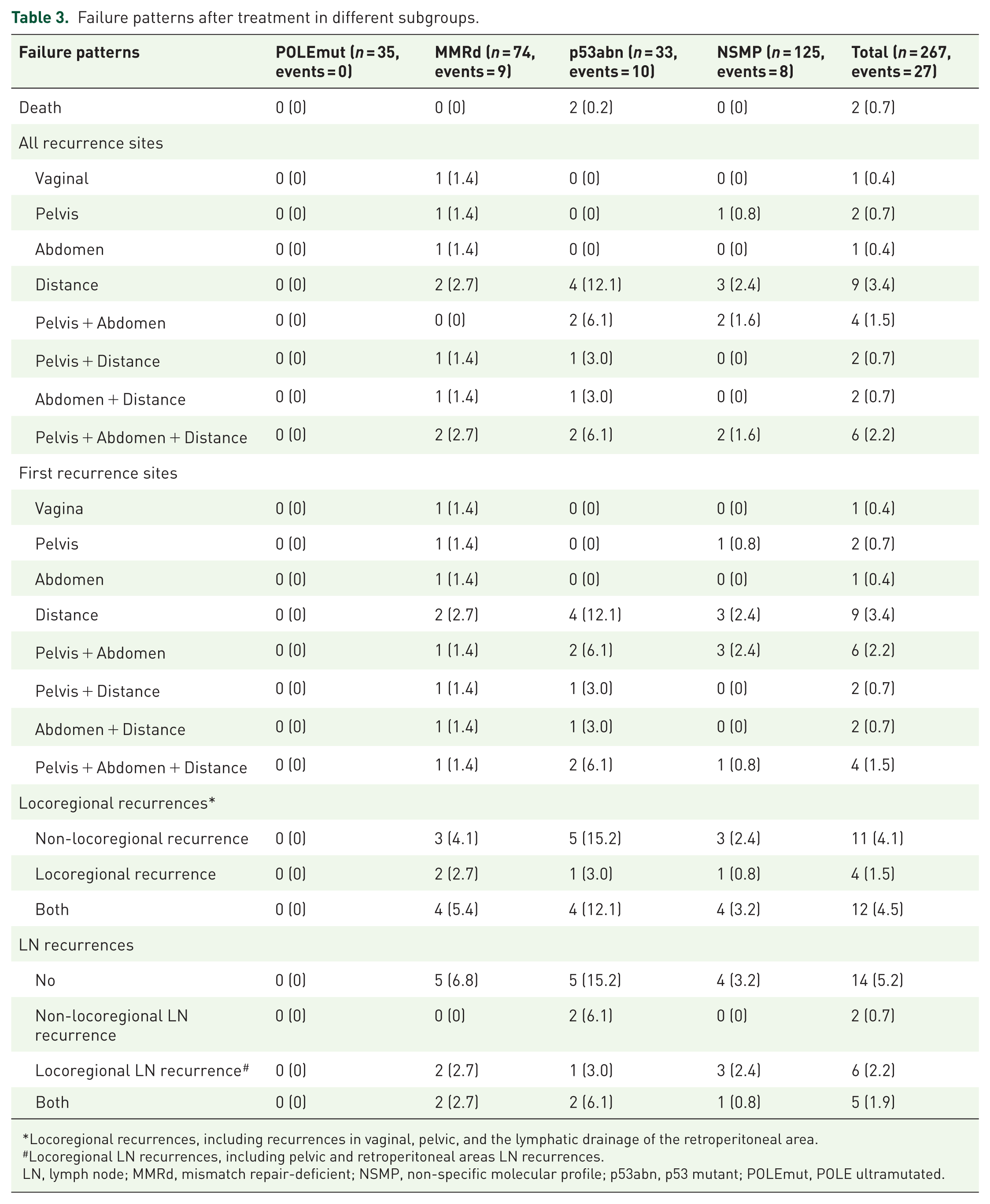
Locoregional recurrences, including recurrences in vaginal, pelvic, and the lymphatic drainage of the retroperitoneal area.
Locoregional LN recurrences, including pelvic and retroperitoneal areas LN recurrences.
LN, lymph node; MMRd, mismatch repair-deficient; NSMP, non-specific molecular profile; p53abn, p53 mutant; POLEmut, POLE ultramutated.
Recurrence rates and patterns varied significantly across molecular subgroups. The highest recurrence rate was observed in the p53abn group (30.3%), whereas no recurrences occurred in the POLEmut group. The MMRd (12.2%) and NSMP (6.4%) groups exhibited intermediate recurrence rates. Regarding specific failure patterns, MMRd and NSMP recurrences were heterogeneously distributed across locoregional, non-locoregional, and combined sites. In contrast, recurrences in the p53abn group frequently presented as aggressive, simultaneous multisite involvements. Detailed failure patterns for patients receiving adjuvant treatment and observation are provided in Supplemental Tables S4 and S5, respectively.
Annual hazard rate among different molecular subgroups
Figure 5 illustrates the dynamic hazard rates across the molecular subgroups. The p53abn group exhibited the highest overall recurrence hazard rate (peaking at 2.2% at 16.8 months), followed by the MMRd group (peak: 0.8% at 14.0 months) and the NSMP group (peak: 0.3% at 21.0 months). While the temporal patterns of the distant metastasis hazard rates were similar across subgroups, the onset of the locoregional recurrence hazard varied notably. It occurred earliest in the NSMP group (5.3 months), followed by the MMRd (9.1 months) and p53abn groups (22.4 months). Overall, the p53abn group consistently demonstrated the highest hazard rates for overall recurrence, as well as for both locoregional and distant failures.

The dynamic hazard rates for MMRd, NSMP, and p53abn subgroups. (a) Recurrence hazard rate. (b) Locoregional hazard rate. (c) Distant metastasis hazard rate.
Univariable and multivariable analysis
Our study found that clinical and pathological variables (endometrioid carcinoma G3, non−endometrioid carcinoma, FIGO 2023 stage III, high-intermediate/high/uncertain risk, laparotomy route, and lower uterine segment invasion) were unfavorable factors associated with recurrence (p < 0.05) (shown in Figure 6). When comparing to the p53abn group, the NSMP group and MMRd group had significantly lower recurrence hazard ratios (HR 0.18, 95% CI: 0.07−0.47 and HR: 0.35, 95% CI: 0.14−0.92, all p < 0.05). Based on the results of multivariable Cox regression analysis, ESGO–ESTRO–ESP 2025 risk classification was identified as the only independent prognostic factor for recurrence when using the AIC method (shown in Supplemental Figure S1(A)), whereas the FIGO 2023 staging system was selected as the only independent risk factor under the BIC method (shown in Supplemental Figure S1(B)). However, due to the limited number of survival events in our current cohort, discrepancies were observed between the AIC and BIC values, indicating potential model instability. Therefore, these comparative hazard modeling results are exploratory and should be interpreted with caution.

Forest plot of univariable Cox regression analysis results.
Discussion
Molecular classification-based personalized treatment decision-making is feasible and yields excellent survival outcomes in patients with stage I–III EC, with 3-year OS and DFS rates of 99.2% and 88.4%, respectively. Notably, recurrences were most frequent among patients with the p53abn subtype, while none were observed in the POLEmut group.
Molecular classification, while recommended, remains largely unavailable in many settings—particularly in low- and middle-income countries. 20 In this study, we implemented a cost‑effective and reliable molecular classification profile in testing for TP53 and MMR abnormalities, as well as POLE mutations, utilizing a combination of molecular sequencing and immunohistochemistry. The most common molecular subtype was NSMP. Stage adjustments—upstaging noted in 20.2% of cases and downstaging in 2.6%—were driven by high‑grade histology, p53abn, extensive LVSI, or POLEmut, consistent with previously published reports (which reported upstaging rates of 20%—30%).20–23 A significantly higher proportion of cases underwent upstaging compared to downstaging. Consequently, most upstaged patients might be considered for treatment intensification and could benefit from aggressive management. 21 Critically, this real-world stage migration underscores the limitation of relying solely on traditional morphologic features, as molecular integration successfully unmasks biologically aggressive tumors that would otherwise be undertreated under the previous FIGO 2009 framework.
However, the enrollment period of this retrospective study, spanning December 2017 to April 2025, encompassed a notable shift with the proposal of the FIGO 2023 staging system. Although not yet incorporated into the NCCN guidelines, the new staging system has begun to subtly shape clinicians’ therapeutic decision-making. In our study, personalized treatment strategies were developed through multidisciplinary discussions among gynecologists, radiation oncologists, and pathologists. As a result, varying adjuvant therapies—including both overtreatment and undertreatment—were administered among patients classified within the same risk group (Supplemental Table S1). For instance, three patients in the low-risk group received chemotherapy with or without radiotherapy (two with the POLEmut subtype because of having stage I, grade 3 disease, and one with the NSMP subtype who received only one cycle of chemotherapy before molecular classification was available). In contrast, nine patients in the high-risk group were managed with observation alone (six with the p53abn subtype and FIGO 2009 stage IA/IB, and three with the NSMP subtype along with grade 3 or ER‑negative status). Paradoxically, throughout this interval of guideline evolution (including ESGO–ESTRO–ESP updates), EC management continued to rely significantly on traditional clinicopathological principles—a situation complicated by inter-guideline discrepancies that frequently presented challenges for clinical practitioners.
To further investigate whether failure patterns differed among patients stratified into the same ESGO‑ESTRO‑ESP 2025 risk group but receiving varied treatments, we analyzed their survival outcomes. Our findings support treatment deescalation for patients with the POLEmut subtype, regardless of their clinical risk group, consistent with previous reports. 24 In the high‑risk p53abn subgroup, two patients who underwent observation developed recurrence—one with distant metastasis and another with pelvic‑abdominal recurrence—supporting the need for intensified treatment. Among high‑risk NSMP patients managed with observation alone, no recurrences were observed, suggesting a potentially different prognostic profile compared to high‑risk p53abn cases.
Supplemental Table S2 details the survival outcomes across molecular subgroups. Within the MMRd group, neither adjuvant treatment modality nor risk classification showed a significant association with survival differences. Conversely, in the NSMP group, hazard ratios were significantly elevated both in patients receiving adjuvant therapy compared to those under observation and in intermediate-/high-risk patients relative to the low-risk group. It is crucial to note that the observed association between chemotherapy ± radiotherapy and worse survival outcomes in the NSMP cohort should not be interpreted causally. Because treatment allocation in our real-world cohort was non-random, this finding strongly reflects confounding by indication. In clinical practice, intensified therapies are naturally prescribed to patients who inherently possess higher-risk clinicopathological features at baseline (e.g., advanced stage, higher tumor grade, deep myometrial invasion, or extensive LVSI). Therefore, the inferior survival in this treated subgroup reflects their underlying aggressive disease biology rather than a detrimental effect of the treatment itself. Setting aside this treatment confounder, the data suggest that the ESGO–ESTRO–ESP 2025 risk classification retains strong prognostic value in NSMP patients. However, the inherent heterogeneity of the NSMP subtype may still limit the precision of current risk‑stratified treatment guidance, underscoring the urgent need to identify additional independent prognostic factors for this specific group. 25 Moving forward, interaction analyses are warranted to clarify the joint effects of risk classification, molecular features, and treatment modalities on survival outcomes.
Despite the limited follow-up period, we observed that 27 patients developed recurrences. In our study, we first depicted the dynamic hazard rate of recurrence or death in a real-world EC cohort with known molecular classification. A previous study reported that the most recurrences were diagnosed in the first 3 years of follow-up in high-risk and advanced patients. 26 In our study, the p53abn subgroup exhibited the highest recurrence hazard rate (peak: 2.2% at 16.8 months), followed by the MMRd group (peak: 0.8% at 14.0 months) and the NSMP group (peak: 0.3% at 21.0 months). From a clinical perspective, these distinct hazard peaks critically indicate that the 14- to 21-month postoperative window is a high-vulnerability period. Therefore, rather than routine symptom-directed follow-up, our findings advocate for scheduling comprehensive imaging evaluations specifically during this critical timeframe, particularly for p53abn patients who frequently present with simultaneous multi-site recurrences. Although intensified follow-up has not been shown to improve survival outcomes, even in high-risk patients, 27 our findings could inform personalized surveillance strategies in the coming era of molecular classification.
While landmark clinical trials (such as PORTEC-3 and PORTEC-4a) have robustly established the prognostic value of molecular subtypes in EC, real-world data remains crucial to bridge the gap between controlled trial settings and clinical practice. To address this, we investigated survival outcomes and failure patterns in a single-center real-world cohort of molecularly classified stage I–III EC. The novel contribution of our study extends beyond confirming established paradigms. First, we provided an initial exploration of the FIGO 2023 and ESGO–ESTRO–ESP 2025 frameworks, observing their prognostic relevance within an unselected clinical cohort. Second, we quantify the direct clinical impact of molecular integration, revealing a significant stage migration effect (20.2% upstaging and 2.6% downstaging) that fundamentally alters treatment trajectories. Third, by mapping real-world treatment adherence and specific relapse dynamics—such as the propensity for simultaneous multisite recurrences in the p53abn subtype—our study offers practical insights into personalized EC management. Ultimately, these findings could greatly facilitate the adoption, translation, and generalization of the updated FIGO and ESGO–ESTRO–ESP systems worldwide.
Currently, robust evidence regarding the utility of the FIGO 2023 staging system and the ESGO–ESTRO–ESP 2025 guidelines is lacking. 28 To identify the independent prognostic factors for recurrence, we developed a rigorous multivariable Cox regression analysis based on both AIC and BIC methods. Our results demonstrated that both the ESGO–ESTRO–ESP 2025 risk classification and the FIGO 2023 staging system served as independent prognostic factors for recurrence. Furthermore, due to the limited number of cases across rare histological subtypes, hazard ratios could not be estimated for each individually; thus, they were uniformly categorized as “non-endometrioid carcinoma” for the primary survival analysis.
However, several limitations should be acknowledged. First, this was a single-center, retrospective cohort study with a relatively short median follow-up of 31.1 months. Because routine molecular testing has only recently been widely implemented, long-term survival data are not yet mature. Notably, with only two death events observed in our cohort, the statistical power for OS analysis is inherently limited; therefore, these specific findings should be considered exploratory. Longer follow-up is necessary to fully capture late recurrences and confirm the durability of the observed survival benefits. Additionally, the limited number of survival events restricted the statistical power of our hazard modeling, preventing a definitive statistical conclusion regarding which system (FIGO 2023 vs ESGO-ESTRO-ESP 2025) offers superior prognostic accuracy. Second, an inherent selection bias exists due to the strict requirement for available molecular classification data. Clinically, this criterion favored the inclusion of patients who underwent primary surgical resection with sufficient tissue yield, effectively excluding those with advanced, unresectable disease or poor performance status (resulting in a cohort with <10% stage III cases). Practically, as universal molecular testing was gradually phased in during the study period, individuals who did not receive testing—because of early-period practices, financial constraints, or physician preference—were excluded. This selection bias likely skewed the distribution of molecular subtypes and contributed to the exceptionally high survival outcomes observed (3-year OS of 99.2% and DFS of 88.4%). Consequently, both subtype frequencies and survival estimates should be interpreted with caution. Third, the validation of the ESGO–ESTRO–ESP 2025 risk classification is partially confounded by real-world clinical heterogeneity. Surveillance bias may exist because standard-of-care follow-up protocols were not uniformly applied; varying intensities of postoperative surveillance (e.g., advanced imaging vs routine clinical exams) could lead to detection bias, influencing the observed recurrence timing. Furthermore, adjuvant therapies administered in this real-world cohort evolved significantly over time, resulting in heterogeneous treatment approaches even within the same risk group. Therefore, larger, multicenter prospective cohorts with extended follow-up are required before the FIGO 2023 staging system and ESGO–ESTRO–ESP 2025 risk stratifications can be definitively evaluated and universally implemented.
Conclusion
In this real-world cohort, integrating molecular classification provided valuable prognostic insights for stage I–III EC. Notably, the POLEmut subtype demonstrated excellent outcomes, supporting potential treatment deescalation. Conversely, the p53abn subtype was associated with a high risk of multi-site recurrence despite adjuvant therapies, underscoring the ongoing clinical challenge in optimizing treatments for this high-risk group. Furthermore, the FIGO 2023 staging and ESGO–ESTRO–ESP 2025 risk classification served as independent prognostic factors for recurrence, though larger prospective cohorts are warranted to validate these findings.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261459107 – Supplemental material for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study
Supplemental material, sj-docx-1-tam-10.1177_17588359261459107 for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study by Lingxia Xin, Kang Ren, Zihan Yan, Yunlong Sheng, Yaqi Wang, Yihan Zhang, Xiaorong Hou, Huanwen Wu and Fuquan Zhang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261459107 – Supplemental material for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study
Supplemental material, sj-docx-2-tam-10.1177_17588359261459107 for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study by Lingxia Xin, Kang Ren, Zihan Yan, Yunlong Sheng, Yaqi Wang, Yihan Zhang, Xiaorong Hou, Huanwen Wu and Fuquan Zhang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-3-tam-10.1177_17588359261459107 – Supplemental material for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study
Supplemental material, sj-pdf-3-tam-10.1177_17588359261459107 for Exploring the molecular classification-based personalized treatment decision-making in FIGO stage I–III endometrial carcinoma after surgery: a population-based real-world study by Lingxia Xin, Kang Ren, Zihan Yan, Yunlong Sheng, Yaqi Wang, Yihan Zhang, Xiaorong Hou, Huanwen Wu and Fuquan Zhang in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank the contributions and assistance of hospital personnel in the Department of Radiation Oncology and in the Department of Pathology, Peking Union Medical College Hospital.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.