
Abstract
Background:
The introduction of pertuzumab in mainland China in 2019 has significantly altered the treatment practice for early breast cancer; however, comprehensive real-world data on hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-positive (HER2+) patients in this new era remain limited.
Objective:
To identify the clinicopathological characteristics, (neo)adjuvant treatment patterns, and clinical outcomes in treated patients with HR+/HER2+ early breast cancer in routine clinical practice in China.
Design:
A retrospective, observational study was conducted in patients with HR+/HER2+ early breast cancer who underwent surgery for breast cancer and had post-surgical pathologic reports available. De-identified patient data for this multicenter study were obtained from the National Cancer Information Database (NCID) in China.
Methods:
Patients were treated with neoadjuvant and adjuvant therapy with chemotherapy and/or HER2-targeted regimens in clinical practice. The main outcomes and measures were as follows: (neo)adjuvant treatment patterns, total pathologic complete responses (tpCR), breast pathologic complete responses (bpCR), disease-free survival (DFS), and event-free survival (EFS). Two-year DFS and EFS were evaluated using the Kaplan–Meier method. Multivariable logistic and Cox regression analyses were performed to identify associated factors of pCR and survival outcomes, respectively. The median duration of follow-up for the study was 13.9 months (range: 0.1–48.1).
Results:
A total of 13,323 patients with HR+/HER2+ early breast cancer were included in this analysis. Trastuzumab + pertuzumab (TP) was the most commonly used regimen in both neoadjuvant and adjuvant settings. Neoadjuvant therapy with dual HER2 blockade resulted in significantly higher tpCR rates (49.1% vs 29.9%) and bpCR rates (53.3% vs 34.4%) compared with trastuzumab alone (both p < 0.001), and numerically higher 2-year DFS rates (90.1% vs 87.1%; p = 0.273) and EFS rates (91.1% vs 89.4%; p = 0.297).
Conclusion:
The dual HER2 blockade regimens that were widely adopted in China for HR+/HER2+ early breast cancer have demonstrated effectiveness in improving pCR in routine clinical practice; a longer follow‑up is required to validate survival outcomes.
Trial registration:
None.
Plain language summary
Although the introduction of pertuzumab in mainland China in 2019 has significantly altered the treatment of early breast cancer, comprehensive real-world data on hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-positive (HER2+) patients remain limited. Between 2019 and 2022, we conducted a retrospective, observational study of 13,323 patients diagnosed with HR+/HER2+ early breast cancer from the National Cancer Information Database (NCID) in China. We found that trastuzumab + pertuzumab (TP) was the most commonly used regimen in both neoadjuvant and adjuvant settings. Compared with trastuzumab alone, dual HER2 blockade (TP or trastuzumab + tyrosine kinase inhibitors) yielded significantly improved total pathological and breast pathological complete responses, as well as numerically higher 2-year disease-free survival and event-free survival rates. Overall, dual HER2 blockade is observed to have treatment effectiveness in routine clinical practice.
Keywords
Introduction
Breast cancer (BC) remains a significant public health concern in China, as the second most common cancer in 2022 and the fifth leading cause of cancer-related deaths among females. Estimated new female BC patients reached 357,200, and the age-standardized incidence rate (ASIR) was 33.04 per 100,000. 1
Human epidermal growth factor receptor 2-positive (HER2+) BC is an aggressive subtype associated with poor prognosis if not properly treated. Compared with the hormone receptor-negative (HR−)/HER2+ subgroup, hormone receptor-positive (HR+)/HER2+ BC exhibit distinct cancer driver mutations 2 and often demonstrate reduced responsiveness to neoadjuvant regimens, with lower pathological complete response (pCR) rates due to their unique biological features.3–5 The Chinese Society of Clinical Oncology Breast Cancer (CSCO BC) database showed that HR+/HER2+ BC accounted for 15.9% of 27,964 Chinese patients with stage I–III BC from 2011 to 2021. 6
Global phase 3 clinical trials, including NeoSphere 7 and PEONY, 8 have established pertuzumab plus trastuzumab (TP) as the standard of care for HER2+ early BC, regardless of HR status. The TP regimen has been recommended by both international9,10 and Chinese guidelines.11,12 Since the introduction of pertuzumab in mainland China in 2019, the treatment landscape for early BC has evolved. While some studies have revealed the distinctive disease features and treatment of HR+/HER2+ BC, large-scale clinical studies based on real-world practice remain limited.
This multicenter, nationwide, population-based, real-world study aimed to characterize the clinicopathological features and (neo)adjuvant treatment patterns in patients diagnosed with HR+/HER2+ early BC, and to evaluate clinical outcomes of these regimens in routine clinical practice in China.
Methods
This retrospective study was conducted according to the ethical standards established by the Declaration of Helsinki. Approval for the protocol and any modifications to it was obtained from the Independent Ethics Committees of Henan Cancer Hospital (No. 2023-048-001). All data were sourced from the National Cancer Data Center (NCID), a centralized, de‑identified real‑world database. Henan Cancer Hospital applied for and obtained data access permission from the NCID. Because this study involved only analysis of existing, de‑identified data from a national repository and did not involve direct patient contact or primary data collection at individual hospitals, no additional ethics approvals from the hospitals that originally contributed data to the NCID were required. A waiver of informed consent was granted due to the retrospective observational nature of the study. The patient data were de-identified throughout the analysis to ensure patient privacy and confidentiality. This report followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for observational studies. 13
Study design and patients
This nationwide, observational study utilized de-identified patient data extracted from the NCID, which was established in 2018 and is maintained by the National Health Commission of China. The NCID is the largest cancer database in China, 14 collecting both structured and unstructured patient information from major cancer centers or general hospitals. A rigorous multi-layered quality control system is employed, combining automated monitoring for data continuity with manual cleaning. Data were independently extracted by two analysts and cross-verified to ensure complete consistency. Anonymous individual patient data were retrieved from electronic medical records (EMR) to obtain information on demographics, disease characteristics, clinical features, therapeutic modalities, and outcomes. Data were collected from 51 hospitals (31 cancer centers and 20 general hospitals) across 27 provinces or municipalities in China.
Patients with HR+/HER2+ early BC were included in the analysis if they met the following criteria: (1) they underwent surgery for BC; and (2) they had available post-surgical pathologic reports between January 1, 2019 and May 31, 2022. Patients were excluded if they had (1) concurrent primary cancer diagnoses or (2) an initial diagnosis of metastatic BC. HR+ status was defined as ⩾1% of tumor cell nuclei staining positive for estrogen receptors (ER) and/or progesterone receptors (PR). HER2+ status was defined as an immunohistochemistry (IHC) score of 3+, or an IHC score of 2+ with confirmation by fluorescence in situ hybridization (FISH).
Data collection and outcomes
The following variables were extracted for all eligible patients: age, body mass index (BMI), menopausal status, TN (tumor-node) stages, clinical stage, pre-treatment HER-2 status, Ki67, comorbidities, or medical history, surgical resection type (mastectomy or breast-conserving surgery (BCS)), axillary lymph node dissection (ALND), neoadjuvant and adjuvant therapy regimens (chemotherapy and targeted therapy), and adjuvant radiotherapy.
Total pathologic complete response (tpCR) was defined as the absence of residual invasive cancer in the breast and lymph nodes (ypT0/is, ypN0). Breast pathologic complete response (bpCR) was defined as the absence of invasive neoplastic cells at the microscopic examination of the primary tumor at surgery following primary systemic therapy (ypT0/is). Disease-free survival (DFS) was defined as the time from the date of surgery to the time of local or distant recurrence, or death from any cause. Event-free survival (EFS) was defined as the time from diagnosis to disease progression, local or distant recurrence, or death from any cause. Data were censored at the last follow-up for patients without events.
For comparisons of tpCR and bpCR, patients were grouped by neoadjuvant targeted therapy, including trastuzumab, TP, or trastuzumab + a tyrosine kinase inhibitor (TKI). Two-year DFS and EFS rates, as well as recurrence rate, were calculated according to neoadjuvant trastuzumab or dual HER2 blockade regimens and achievement of tpCR.
Statistical analysis
Descriptive statistics were used to summarize patient characteristics and distributions for the overall cohort and for subgroups who received or did not receive neoadjuvant therapy. Continuous variables were presented as the medians with interquartile ranges (IQRs; first and third quartiles). Categorical variables were presented as frequencies and percentages. Multivariable logistic regression analyses were conducted to detect independent predictors of tpCR and bpCR, and results were expressed as odds ratios (ORs), 95% confidence intervals (CIs), and p-values. Survival probability was computed with the Kaplan–Meier approach. Multivariable Cox proportional hazards regression models were performed to identify significant prognostic factors for DFS and EFS, with estimates shown as hazards ratio (HRs), 95% CIs, and p-values. Neoadjuvant and adjuvant sequential treatment was included as the whole regimen based on the dominant targeted therapy received to handle the heterogeneity in the Cox analysis. All tests were two-sided, and p-values of 0.05 or less were considered statistically significant. All analyses were conducted using SAS 9.4.
Results
Population characteristics
From January 1, 2019, to May 31, 2022, 290,626 Chinese patients were recorded in the NCID. Of these, 121,548 were classified as early BC, and 33,373 (27.5%) were HER2+. Among the HER2+ patients, 18,159 were HR+/HER2+, accounting for 14.9% (18,159/121,548) of all cases, and 54.4% (18,159/33,373) of the HER2+ population (Figure 1). A cohort of 13,323 HR+/HER2+ early BC patients was analyzed. The median duration of follow-up was 13.9 months (range 0.1–48.1).

Patient selection flowchart.
The majority of patients were treated at tertiary hospitals (n = 13,321 (100%)) and cancer centers (n = 11,212 (84.2%)). Patients primarily resided in first-tier (n = 2829 (21.2%)) or secondary-tier cities (n = 10,089 (75.7%)). The median age at BC diagnosis was 50.0 years (IQR 44.0–57.0). A significant majority of patients were premenopausal (n = 9237 (69.3%)). As regards clinical stage, cT2 (58.9%), cN0 (45.8%), and cN1 (35.0%) were the most frequently observed tumors (Table 1).
Demographic and clinical characteristics of the patients analyzed.
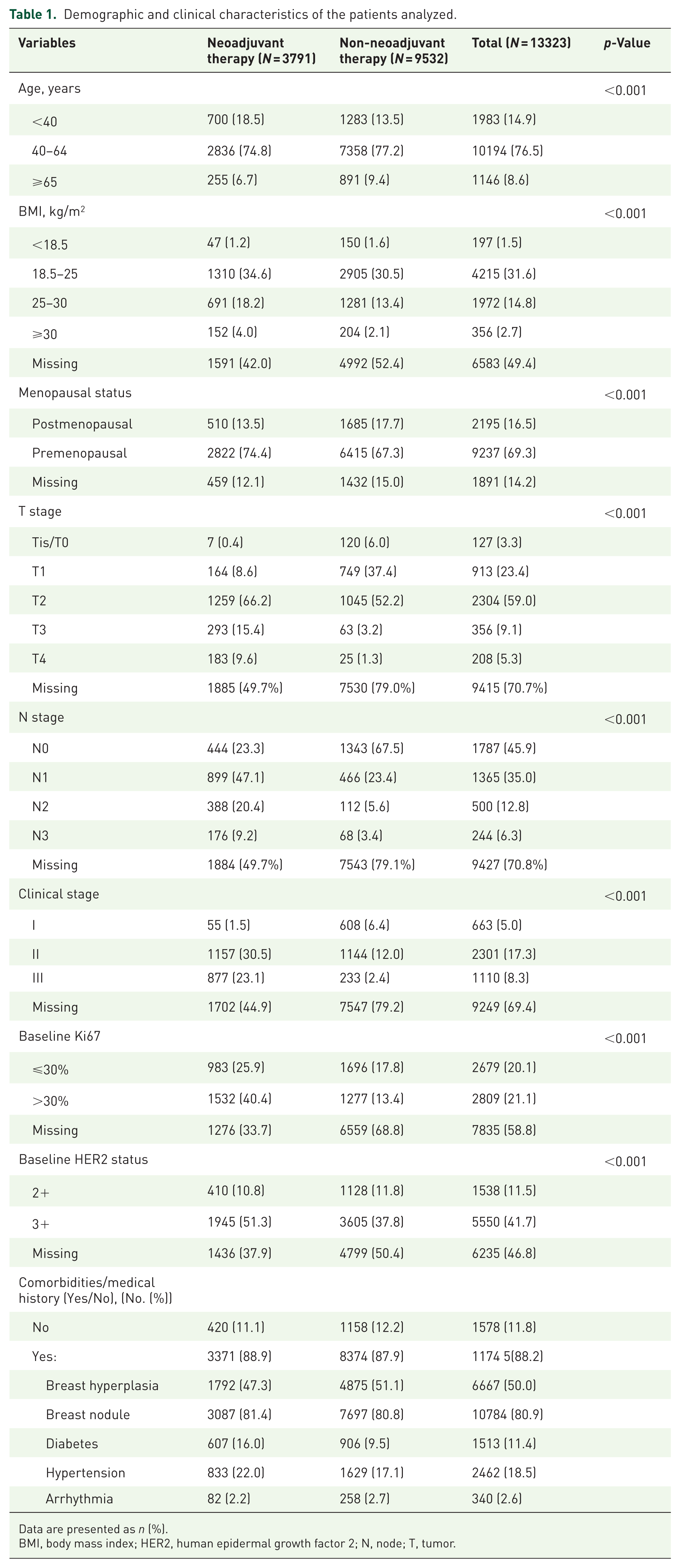
Data are presented as n (%).
BMI, body mass index; HER2, human epidermal growth factor 2; N, node; T, tumor.
Treatment patterns
Among the 13,323 HR+/HER2+ early BC patients, 3791 (28.5%) patients received neoadjuvant therapy, while 9532 did not. Of the patients who received neoadjuvant therapy, 2700 (71.2%) received anti-HER2 neoadjuvant treatment with chemotherapy. Dual HER2 blockade with TP + chemotherapy (1970/3791 (52.0%)) was the most frequently adopted regimen. Trastuzumab + chemotherapy was received by 649 (17.1%) patients (Figure 2). The median cycle of neoadjuvant therapy received was 4.0 (IQR 3.0–5.0). Detailed neoadjuvant regimens are listed in Supplemental Table 1.

Neoadjuvant treatment patterns in patients with HR+/HER2+ early breast cancer. Others include regimens not specified in the chart.
Mastectomy was the most frequently chosen type of surgical procedure for the primary tumor (n = 11,454, 86.0%), while BCS was chosen for 11.8%. ALND was performed in more than half of the patients (n = 7332, 55.0%; Supplemental Table 2).
tpCR and bpCR
Dual HER2 blockade (including TP and T + TKI) as neoadjuvant targeted therapy yielded a significantly higher tpCR (49.1% vs 29.9%) and bpCR (53.3% vs 34.4%) rates than trastuzumab + chemotherapy (both p < 0.001). The pCR with the TP regimen was numerically higher than with trastuzumab + TKI therapy (tpCR: p = 0.700; bpCR: p = 0.673; Figure 3).
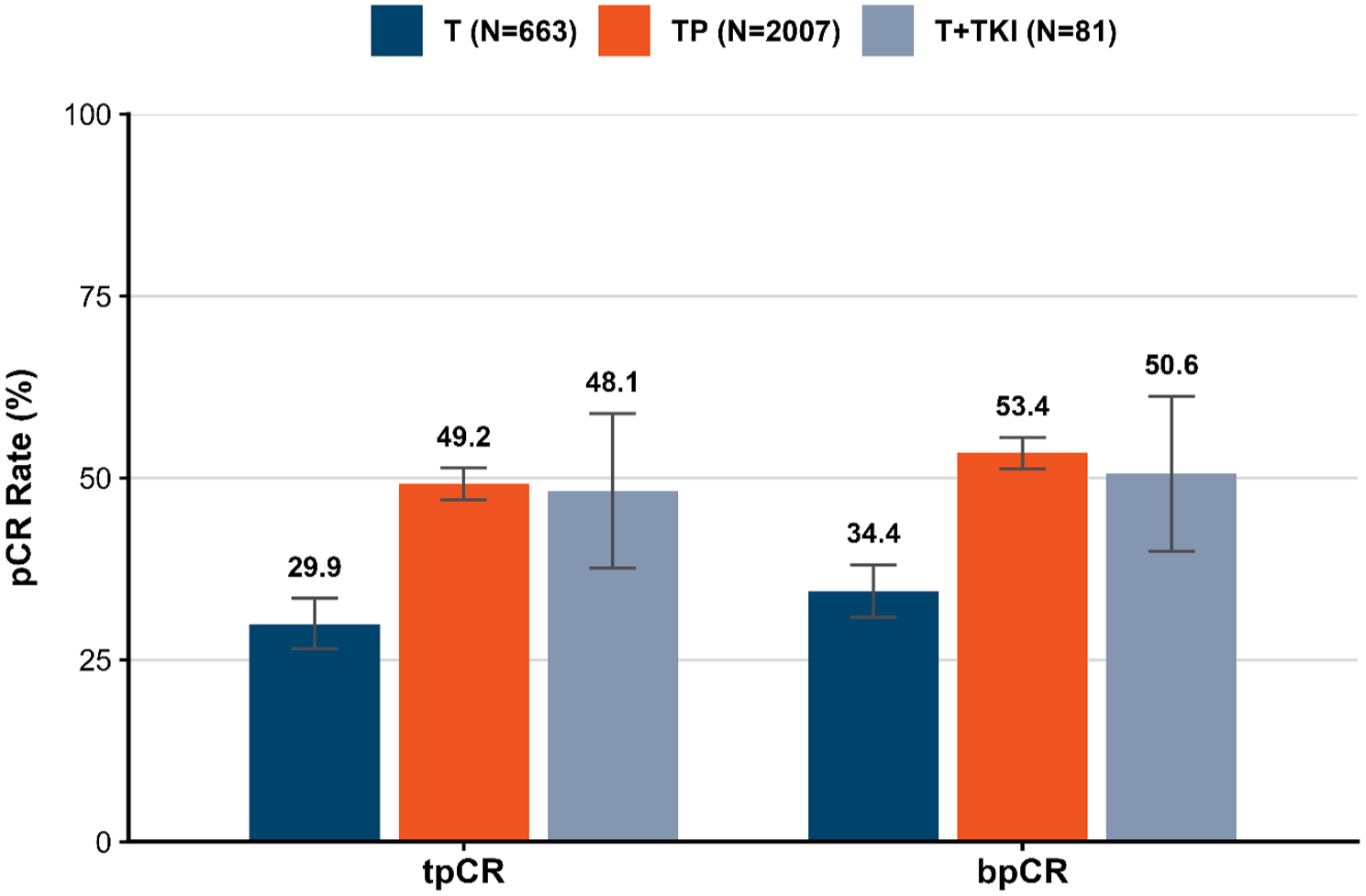
Short-term outcomes. The TP group (N = 2007) includes 37 patients who lacked chemotherapy records and were excluded from the “Chemo + TP” group in Figure 2 (N = 1970).
In the multivariable logistic regression analysis, improved tpCR was independently positively associated with postmenopausal status (OR = 1.47; 95% CI 1.19–1.81; p < 0.001), receipt of neoadjuvant dual HER2 blockade (reference: trastuzumab, OR = 2.17; 95% CI 1.79–2.64; p < 0.001), and baseline Ki67 > 30% (reference: Ki67 ⩽ 30%, OR = 1.32; 95% CI, 1.11–1.57; p = 0.002), but negatively associated with age ⩾65 years (reference: age 40–64 years, OR = 0.73; 95% CI 0.55–0.98; p = 0.037), neoadjuvant chemotherapy alone (reference: chemotherapy + trastuzumab, OR = 0.56; 95% CI 0.44–0.70; p < 0.001), and clinical stage III (reference: stage II, OR = 0.80; 95% CI 0.66–0.96; p = 0.019; Supplemental Table 3). Postmenopausal status, receipt of neoadjuvant dual HER2 blockade, and Ki67 > 30% were independent positive factors associated with a better bpCR, while age ⩾65 years and neoadjuvant chemotherapy alone were independent negative factors in the multivariable model (Supplemental Table 4).
DFS and EFS
As regards 2-year DFS and EFS rates, dual HER2 blockade as neoadjuvant therapy was observed to be numerically superior to a trastuzumab alone regimen (2-year DFS: 90.1% (95% CI 87.5%–92.7%) vs 87.1% (95% CI 83.9%–90.4%), p = 0.273; 2-year EFS: 91.1% (95% CI 89.5%–92.7%) vs 89.4% (95% CI 86.7%–92.1%), p = 0.297).
In the multivariable Cox regression analysis of DFS, clinical stage III was associated with a higher risk compared with clinical stage II (HR 1.73 (95% CI 1.22–2.44), p = 0.002; Supplemental Table 5). Cox regression analysis of EFS showed similar results (HR 1.69 (95% CI 1.25–2.30), p < 0.001; Supplemental Table 6)).
Among all patients who received neoadjuvant treatment, the TP-based regimen was the most frequently used therapy in both neoadjuvant and adjuvant settings. In patients who received TP in both the neoadjuvant and adjuvant stages, the recurrence rate was 2.5% for those who achieved tpCR and 5.6% for those who did not. Overall, patients who achieved tpCR had a lower recurrence rate compared with those who did not (Table 2).
Recurrence and 2-year DFS rates by neoadjuvant/adjuvant therapy and tpCR status.
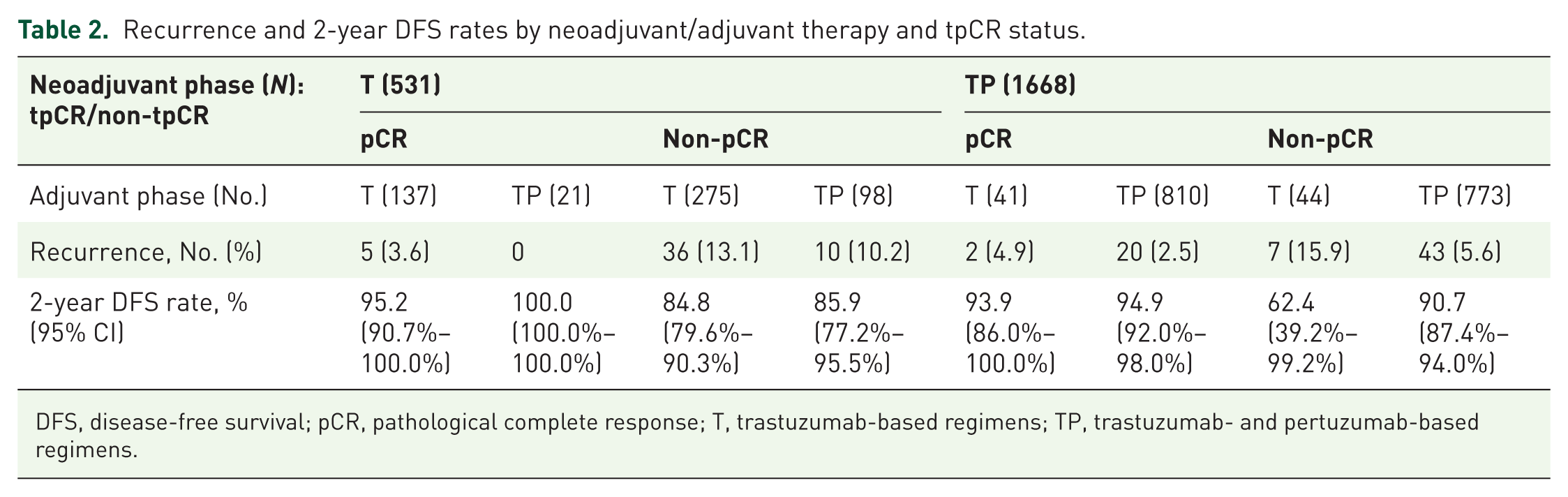
DFS, disease-free survival; pCR, pathological complete response; T, trastuzumab-based regimens; TP, trastuzumab- and pertuzumab-based regimens.
Discussion
This is the first and largest nationwide real-world study demonstrating treatment patterns and clinical outcomes for HR+/HER2+ early BC patients in routine clinical practice in China. Following the introduction of pertuzumab in mainland China in 2019, TP-based regimens were rapidly adopted as the standard of care, resulting in clinical benefits for these patients. This study’s comprehensive geographic distribution of hospitals and large sample size suggested these findings accurately reflect contemporary treatment strategies in China.
A recent cross-sectional study performed by the CSCO BC Committee Database Collaborative Group reported that the proportion of the HER2+ subgroup in early (stage I–III) BC patients in China was 30.2% (8446 of 27,964), 6 which was close to our finding of 27.5% (33,373 of 121,548). In the CSCO study, the percentages of HR+/HER2+ patients were reported as 15.9% (4439 of 27,964) in all early BCs, and 52.6% (4439 of 8446) in HER2+ cases. 6 The results in our study were similar, and the numbers were 14.9% and 54.4%, respectively. Our study found that patients were mostly diagnosed between 40 and 64 years old (median age 50 years), and clinical stage II was the most dominant status (excluding unknown status), which is consistent with the results from the HER2+ population in the CSCO study. 6 Both studies collected patient data from the hospital-based national database, and our study further confirms the young and high proportion of late-stage characteristics in the Chinese population among patients with the HER2+/HR+ subtype.
In China, the proportion of neoadjuvant therapy in patients with HER2+ early breast cancer was reported to increase from 15.9% (2011) to 25.3% (2021) with a 10-fold increase in the trastuzumab-based regimen. 6 Our study showed that 28.5% (3791 of 13,323) of patients with an initial diagnosis of HR+/HER2+ early BC received neoadjuvant therapy in clinical practice, of which 71.2% (2700 of 3791) patients received anti-HER2 therapy + chemotherapy. Although there have been few studies targeting the HR+/HER2+ population, a prospective observational multicenter study in Italy (BRIDE) reported that neoadjuvant systemic therapy was administered to 27.9% (46/165) of HR+/HER2+ early BC patients, and 84.8% (39/46) of those patients received anti-HER2 therapy + chemotherapy. 15 Real-world data from German-certified BC centers showed that 26.5% of HR+/HER2+ early BC patients were treated with neoadjuvant chemotherapy. 16 Similar results from real-world studies in this population suggest a simultaneous neoadjuvant treatment trend globally.
Of note, the Chinese BC population was diagnosed at a younger age (median age 50 years in our study, compared with 64 years in a US early BC population 6 ), which highlights a greater need as well as the potential to improve the quality of life (including physical image and psychosocial well-being). Patients of younger age at presentation may benefit substantially from BCS. Our data revealed a BCS rate of 11.8% and an ALND rate of 55.0%. Without neoadjuvant therapy, the CSCO study reported a 20.8% BCS rate in Chinese patients with cT1 tumors across all molecular subtypes. 6 A recent nationwide cross-sectional survey in China reported the median BCS rate following neoadjuvant BCS increased from 5% in 2017 to 20% in 2022. 17 And in 2022, 38% of surveyed hospitals reported a post‑neoadjuvant BCS rate of ⩽10%. 17 Our observed BCS rate of 11.8% falls within this range and is consistent with the real‑world practice pattern. Gori et al. 15 reported that 41.5% of BC patients who received neoadjuvant therapy underwent BCS, while 31.9% of patients received only ALND, and 15.6% had ALND following sentinel lymph node biopsy. HR+/HER2+-specific patient-level data regarding surgical approaches and axillary evaluations were unavailable in these two studies. Previous studies have shown that neoadjuvant therapy can significantly reduce tumor burden in the breast, resulting in high conversion rates to breast conservation. 18 Surgery, including BCS and ALND, varied substantially across countries and institutions and is influenced by patient preference. Our study cohort was derived predominantly from tertiary hospitals (84.2%), which typically manage more complex cases with higher baseline tumor burden (54.1% with N stage>0). Although aligned with Chinese practice, the initial diagnosis of BC usually occurs at a tertiary hospital; further investigations are needed on the overall breast cancer surgery statistics in China.
Randomized controlled trials7,19 –22 have shown that neoadjuvant TP + chemotherapy results in pCR rates of 26.0%–57.3% in HR+/HER2+ patients, with pCR rates appearing to increase with the number of neoadjuvant therapy cycles. The PHEDRA study 23 that investigated pyrotinib, a TKI developed in China that targets EGFR/HER2, given in combination with trastuzumab and chemotherapy in a neoadjuvant setting, was associated with a pCR rate of 41.0% in Chinese HER2+ BC, and 29.9% in the HR+/HER2+ subgroup. pCR rates were highest after 8–9 cycles of neoadjuvant therapy (51.0%–57.3%) in the BERENICE 19 and TRAIN-2 20 studies, followed by six cycles (46.2%–48.6%) in TRYPHAENA 21 and 4 cycles (26.0%–33.3%) in the NeoSphere 7 and PEONY 8 studies. In our study, patients received a median of 4.0 cycles of TP prior to surgery, with 71.2% receiving ⩾4 cycles. Considering the study period between 2019 and 2022, the four-cycle regimen was predominant until more studies with longer cycles released their results later. While a direct comparison across different clinical trials should be interpreted with caution, our tpCR rate (49.1%) was in broad agreement with the trends observed across randomized controlled trials, supporting the observed treatment effect in clinical practice in a real-world setting.
Neoadjuvant dual HER2 blockade yielded significantly higher tpCR (49.1% vs 29.9%) and bpCR (53.3% vs 34.4%) than trastuzumab + chemotherapy, but no significant difference was found between neoadjuvant regimens of TP and trastuzumab + TKI, which might be explained by the lower number in the trastuzumab + TKI group. The multivariable Cox regression analyses were exploratory in nature due to missing values in relevant clinical variables and insufficient follow-up time. In addition, as an observational real‑world study, our comparisons between dual HER2 blockade and trastuzumab alone are subject to residual confounding and selection bias. Although we adjusted for available covariates, unmeasured factors (e.g., patient awareness, socioeconomic status, or institutional practice patterns) may still influence the results. Therefore, whether the tpCR advantage of TP over trastuzumab alone translates into improvements in EFS or DFS cannot be determined from the current data. A longer follow‑up is required to assess whether the pCR advantage of dual blockade leads to improved survival outcomes.
Five-year follow-up of the PEONY study showed a trend toward improved DFS with TP in the HR+ subgroup, although the median DFS was not reached. 8 Our data supplement this finding with real-world experience of 2-year DFS data in the unique HR+/HER2+ subgroup. However, multivariable analysis failed to detect a difference between various treatment regimens, after controlling for clinical features, due to the small number of DFS or EFS events in our study.
Strengths and limitations
The most notable strength of our study is the use of individual patient-level data from the comprehensive NCID database, which covers 70% of administrative regions geographically and is therefore representative of demographics and treatment patterns in this distinct BC population in China. In addition, our findings of the early adoption period of pertuzumab in China (2019–2022) provide a real-world baseline for this specific subgroup.
The limitations of the study include its retrospective nature; the inherent potential bias arising from missing, incomplete, or inaccurately logged data; the secondary use of electronic medical records; and uncertainty regarding whether data were missing at random, which may limit the overall robustness of our results. Moreover, the short follow-up precludes the validation of benefits for DFS or EFS, and the multivariable analyses were exploratory in nature. Furthermore, due to the termination of data access permissions, we were unable to perform additional sensitivity analyses (e.g., multiple imputation or formal tests of missingness mechanisms) to further address the high proportion of missing data. Therefore, the findings should be interpreted with caution, particularly the multivariable models, which are based on a subset of the full cohort. And due to the tertiary center dominance, our results may not be generalizable to lower-tier hospitals or rural populations.
Conclusion
Our real-world study provides key insights into the disease burden, (neo)adjuvant therapy patterns, and clinical outcomes in HR+/HER2+ early BC in routine clinical practice in China. Dual HER2 blockade demonstrated significantly higher pCR rates compared with trastuzumab alone. The TP regimen has been widely adopted as the standard of care in the (neo)adjuvant treatment in China, while longer follow-up is needed to fully evaluate long-term survival benefits.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261461748 – Supplemental material for (Neo)adjuvant therapy patterns and outcomes in patients with HR+/HER2+ early breast cancer: a real-world study using the national cancer information database in China
Supplemental material, sj-docx-1-tam-10.1177_17588359261461748 for (Neo)adjuvant therapy patterns and outcomes in patients with HR+/HER2+ early breast cancer: a real-world study using the national cancer information database in China by Jiujun Zhu, Dechuang Jiao, Chengzheng Wang, Zhenduo Lu, Xiuchun Chen, Lianfang Li, Xianfu Sun, Chongjian Zhang, Jianghua Qiao, Min Yan and Zhenzhen Liu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.