
Abstract
Hepatocellular carcinoma (HCC) continues to pose a significant global health challenge. In recent years, immunotherapy has emerged as a critical component of HCC treatment, demonstrating encouraging outcomes in a subset of patients. Nevertheless, the overall response rate to immune checkpoint inhibitors (ICIs) remains modest. Deficient immunogenicity and the consequent failure to adequately activate antitumor immunity are widely regarded as central constraints on immunotherapy efficacy. Unlike previous reviews focusing on immune escape or clinical outcomes, this review centers on tumor immunogenicity as the key determinant of immunotherapy response. We systematically summarize the major mechanisms regulating HCC immunogenicity and outline current strategies to enhance and remodel it. By conceptualizing immunogenicity as the principal determinant of immunotherapy efficacy, we propose a unified framework centered on immunogenicity that integrates intrinsic tumor characteristics, microenvironmental regulation, and diverse therapeutic interventions. Within this framework, we highlight representative immunogenicity‑enhancing strategies, including epigenetic restoration of antigen presentation capacity, induction of immunogenic cell death through local or systemic therapies, and vaccine‑based approaches aimed at amplifying antitumor immunity. Collectively, this review offers a systematic and coherent perspective on immune tolerance in HCC through the lens of immunogenicity remodeling, thereby providing a conceptual foundation for the rational design of future immunotherapy strategies.
Plain language summary
Hepatocellular Carcinoma remains a serious health problem worldwide. Immunotherapy, a treatment that uses the body’s immune system to fight cancer, has become an important option. However, it often does not work well for many liver cancer patients. The main reason is that the cancer is good at hiding from the immune system. This hiding ability comes from problems both inside and outside the cancer cells. Inside, the cells may lack the right “tags” that the immune system needs to recognize them, or they may not display these tags properly. Outside, the tumor creates a protective environment that weakens and disables any immune cells that try to attack it. Understanding these hiding tactics is key to making immunotherapy more effective. This article explains these different hiding methods and describes new strategies being developed to make the cancer more visible to the immune system. These new approaches include using drugs to force the cancer cells to show the right “tags,” using treatments like radiation or special viruses to kill cancer cells in a way that alerts the immune system, and developing cancer vaccines to train the body’s defenses to target the tumor better. Together, these methods show great promise for helping the immune system successfully fight liver cancer. They provide important ideas for improving treatment results and could lead to better survival for patients in the future.
Introduction
Hepatocellular carcinoma (HCC) constitutes 75%–85% of primary liver cancers and is the sixth most prevalent malignancy and the third leading cause of cancer-related mortality worldwide, with its incidence on a consistent upward trajectory. 1 Despite ongoing advancements in the comprehensive management of HCC, guided by the Barcelona Clinic Liver Cancer (BCLC) staging system, and improvements in imaging surveillance, surgical resection, interventional therapies, and systemic treatments, the majority of patients are diagnosed at intermediate or advanced stages, where curative interventions are no longer viable. As a result, the overall prognosis remains poor 2 (Figure 1).
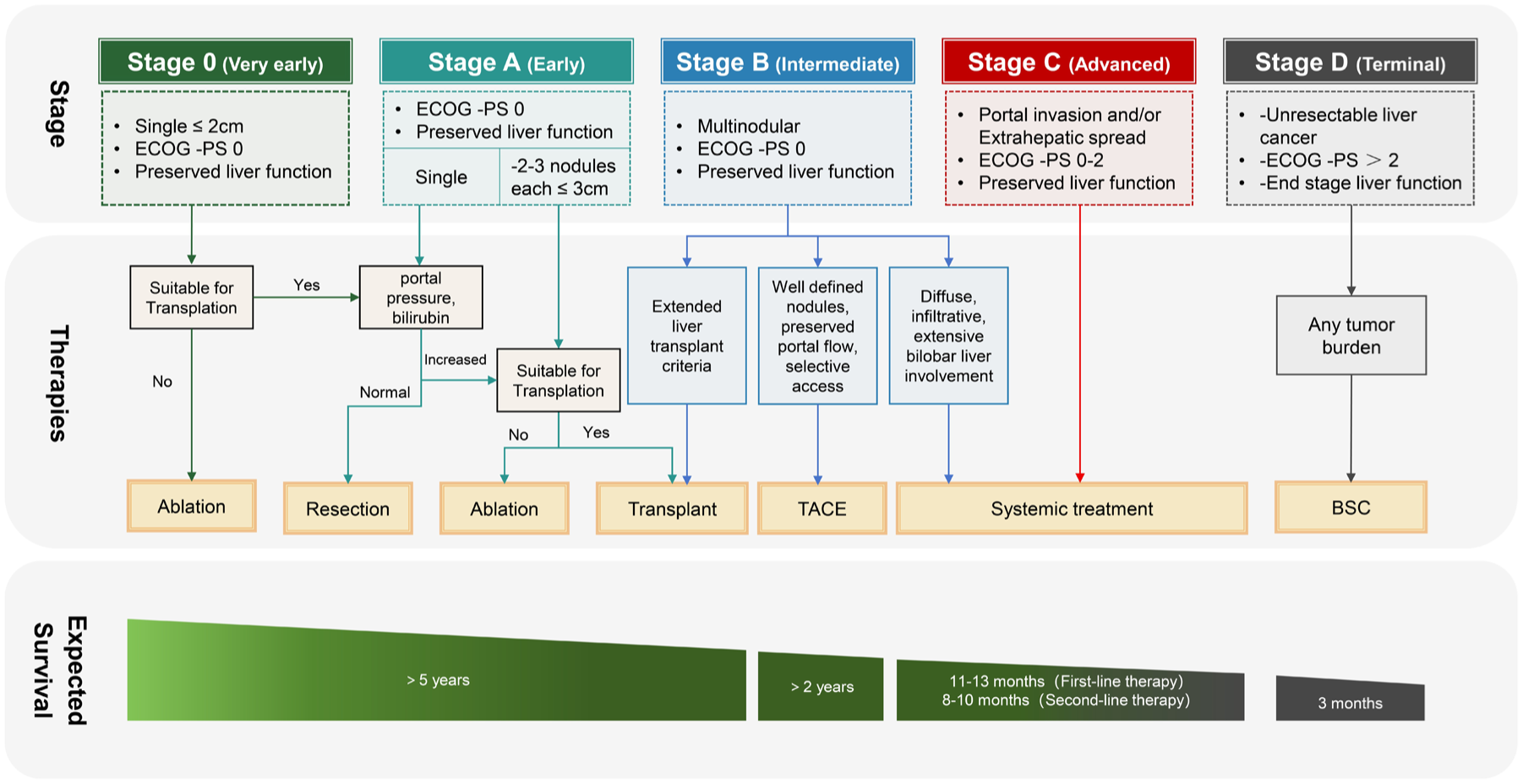
The BCLC staging system: therapeutic strategies and prognostic outcomes in HCC. In asymptomatic early-stage HCC (stages 0 and A), management predominantly involves ablation, surgical resection, or liver transplantation, with an anticipated overall survival exceeding 5 years. Intermediate-stage HCC (stage B) is generally addressed through transarterial chemoembolization, resulting in a median survival of over 2 years. Advanced HCC (stage C) is treated with systemic therapies, including targeted agents and immunotherapy, which provide a median survival ranging from 19 to 23 months. For end-stage disease (stage D), best supportive care is typically administered, with a median survival of approximately 3 months.
In recent years, cancer immunotherapy, particularly immune checkpoint inhibitors (ICIs) targeting programmed cell death-1 (PD-1)/programmed death-ligand 1 (PD-L1) and cytotoxic T-lymphocyte-associated-4 (CTLA-4), has catalyzed a transformative advancement in the therapeutic landscape of advanced HCC. ICI functions by reactivating antitumor immune responses through the inhibition of suppressive signaling pathways on T cells, thereby improving survival outcomes. Notably, in contrast to the era dominated by multi-kinase inhibitors, ICI-based immunotherapy has facilitated an overall survival (OS) exceeding 4 years in up to 25% of patients. 3 Based on the favorable outcomes of several pivotal randomized clinical trials, combination immunotherapy regimens—such as atezolizumab plus bevacizumab (the T+A regimen) and tremelimumab plus durvalumab (the dual ICI regimen)—have supplanted traditional targeted therapies as the new standard first-line treatment for advanced HCC, significantly extending OS. 4 Among these, the T+A regimen has emerged as a cornerstone of therapy, with the IMbrave150 study reporting a median OS of 19.2 months (24.0 months in the Asian subgroup) and an objective response rate (ORR) of approximately 30%. 5
In contrast to the notable success of immunotherapy in highly immunogenic tumors, such as melanoma and non-small cell lung cancer, its effectiveness in HCC remains limited. For example, in advanced melanoma, the combination of nivolumab and ipilimumab has resulted in a median OS of 72 months and an ORR of up to 58%, while pembrolizumab monotherapy has achieved a 5-year OS rate of 34%.6,7 Conversely, in HCC, even the most advanced combination regimens—such as T+A or dual ICI therapies—yield ORR of merely around 25%, with complete responses observed in fewer than 5% of patients. 4 This disparity is largely attributed to the inherently low immunogenicity of HCC, characterized by insufficient or absent tumor antigen expression, limited T-cell infiltration, and a profoundly immunosuppressive microenvironment. As a result, the majority of patients experience primary resistance or rapid disease progression following ICI treatment. 8
A thorough understanding of the mechanisms that constrain antitumor immune responses in HCC, alongside the investigation of strategies to enhance tumor immunogenicity, is crucial for addressing the limitations associated with immunotherapy for this malignancy. This review systematically delineates the intrinsic and extrinsic factors affecting HCC immunogenicity and concentrates on strategies, with the objective of providing a theoretical basis for the development of next-generation, efficacious combination immunotherapies for HCC, by incorporating the most recent advancements in the field.
The multidimensional determinants of immunogenicity in HCC
Immunogenicity refers to the capacity of the immune system to identify and respond to foreign or abnormal antigens. Within the field of oncology, tumor immunogenicity denotes the ability of tumor cells to be recognized and eradicated by the immune system. 9 Tumors with high immunogenicity effectively activate dendritic cells (DCs) and effector T cells, thereby demonstrating favorable responses to immunotherapy. Conversely, tumors with low immunogenicity are more likely to evade immune surveillance, leading to reduced therapeutic efficacy. 10 Across a range of malignancies, the degree of tumor immunogenicity is strongly correlated with the response rate to ICI. This correlation highlights the critical importance of immunogenicity in determining the success of immunotherapeutic interventions.
Tumor immunogenicity is not a static characteristic but is dynamically influenced by the intrinsic properties of tumor cells in conjunction with the extrinsic factors of the tumor microenvironment (TME).11,12 These intrinsic and extrinsic components constitute a complex regulatory network that collectively dictates the efficacy of immune-mediated tumor cell recognition and elimination. This review systematically examines the fundamental mechanisms that impair efficient immune recognition and elimination of tumor cells in HCC.
Intrinsic mechanisms in tumor cells
Deficient antigen expression
Tumor antigens constitute the molecular basis for initiating antitumor immune responses and can be categorized into two primary types based on their expression patterns: tumor-associated antigens (TAAs) and tumor-specific antigens (TSAs). TAAs are antigens that are expressed at low levels in certain normal tissues but are significantly upregulated in tumor cells. Conversely, TSAs result from somatic mutations or other genetic alterations that produce novel antigens uniquely present on tumor cells and absent from normal tissues. Because of their tumor-specific expression and strong immunogenicity, TSAs are considered ideal targets for cancer immunotherapy. 13 Tumor mutational burden (TMB) refers to the total number of somatic mutations—including point mutations and insertions/deletions—per megabase (Mb) of the tumor genome. Studies employing whole-exome sequencing have demonstrated that TMB directly influences the abundance of TSAs. For instance, tumors with high TMB, such as melanoma (⩾10 mutations/Mb), exhibit robust immunogenicity due to the generation of numerous TSAs. 14 In contrast, HCC typically exhibits a TMB of less than 5 mutations/Mb (median: 2.65–5 mutations/Mb), which is significantly lower than that of many other solid tumors, thereby limiting the response rate to ICI. 15
Tumor heterogeneity dilutes immunogenicity
Intratumoral heterogeneity (ITH) constitutes a significant factor that compromises tumor immunogenicity. According to Reading et al., 16 the immunogenic strength of a tumor is influenced not only by its total mutation burden but, more critically, by the proportion of clonal mutations within it. Clonal mutations originate during the early stages of tumorigenesis and are present in all cancer cells, capable of eliciting broad and sustained T-cell immune responses, thus correlating with clinical benefit from ICI. In contrast, subclonal mutations are confined to specific cellular subpopulations, and the resulting antigenic heterogeneity hinders the comprehensive recognition and elimination of tumor cells by T cells, thereby weakening immunogenicity. 17 The formation and evolution of ITH are driven by the intrinsic mechanism of immunoediting. 17 Under the selective pressure exerted by the immune system, tumor cells undergo further genetic and epigenetic modifications, which eliminate highly immunogenic clones while promoting the expansion of low-antigenicity subclones. 18 This process not only diminishes immune recognition but also fosters conditions that facilitate tumor recurrence and metastasis. Clinical studies have demonstrated a negative correlation between ITH and the response to immunotherapy; specifically, in melanoma, a higher proportion of nonclonal mutations is linked to reduced efficacy of ICI. 19 Similarly, in HCC, ITH is recognized as a critical mechanism underlying both the low initial response to ICI and the development of acquired resistance. 20 Consequently, elevated ITH is associated with reduced immunotherapy efficacy and may facilitate tumor adaptation under immune selective pressure, thereby promoting immune escape and resistance.
Antigen processing and presentation
The integrity of the antigen processing and presentation machinery (APM) is a crucial determinant of tumor immunogenicity. Tumor cells can evade immune detection by downregulating or losing major histocompatibility complex class I (MHC-I) molecules and by silencing genes involved in antigen processing, such as TAP1/2, LMP2/7, and β2-microglobulin. 21 Wang et al. 11 developed an APM scoring system using gene set variation analysis and demonstrated that tumors with high TMB can still exhibit low immunogenicity if APM gene expression is compromised, as neoantigens cannot be effectively processed and presented to immune cells. Numerous studies have corroborated that the downregulation of MHC-I expression is closely associated with insufficient intratumoral T-cell infiltration, an immunologically “cold” phenotype, and poor patient outcomes. 22 In HCC, the loss of MHC-I expression similarly correlates with adverse prognosis. 23 Beyond transcriptional and post-transcriptional regulation, the functionality of the MHC-I system is also determined by its underlying genetic architecture. MHC-I molecules are encoded by three classical human leukocyte antigen (HLA) genes, including HLA-A, HLA-B, and HLA-C, which represent some of the most polymorphic loci in the human genome. This high degree of genetic diversity enables individuals to present a diverse repertoire of neoantigens, thereby sustaining effective antitumor immune surveillance. 24 In recent years, HLA loss of heterozygosity (HLA LOH) has emerged as a structurally profound and relatively irreversible mechanism of immune evasion. HLA LOH markedly reduces the diversity of HLA alleles available for antigen presentation, thereby impairing neoantigen display and attenuating cytotoxic T-cell recognition.24,25 Immunogenomic analyses have revealed that HLA LOH is prevalent across multiple solid tumors and is also well documented in HCC, where it is associated with impaired antigen presentation, reduced infiltration of cytotoxic T cells, and signatures of immunoediting. 26 Furthermore, accumulating evidence suggests that HLA LOH contributes to resistance to ICI therapy, underscoring its role as a critical mechanism of immune escape. 25 Together, alterations in APM function, MHC-I expression, and HLA integrity limit effective antigen presentation in HCC.
Extrinsic regulation by the TME
In addition to intrinsic tumor cell characteristics, extrinsic factors within the TME critically shape antitumor immune responses in HCC. Through the coordinated action of multiple components, the TME establishes a formidable barrier that interferes with antigen presentation and impedes immune recognition. Table 1 summarizes the major immunosuppressive components of this barrier and their key mechanisms of action.
Key components of the TME that suppress HCC immunogenicity and their core mechanisms.
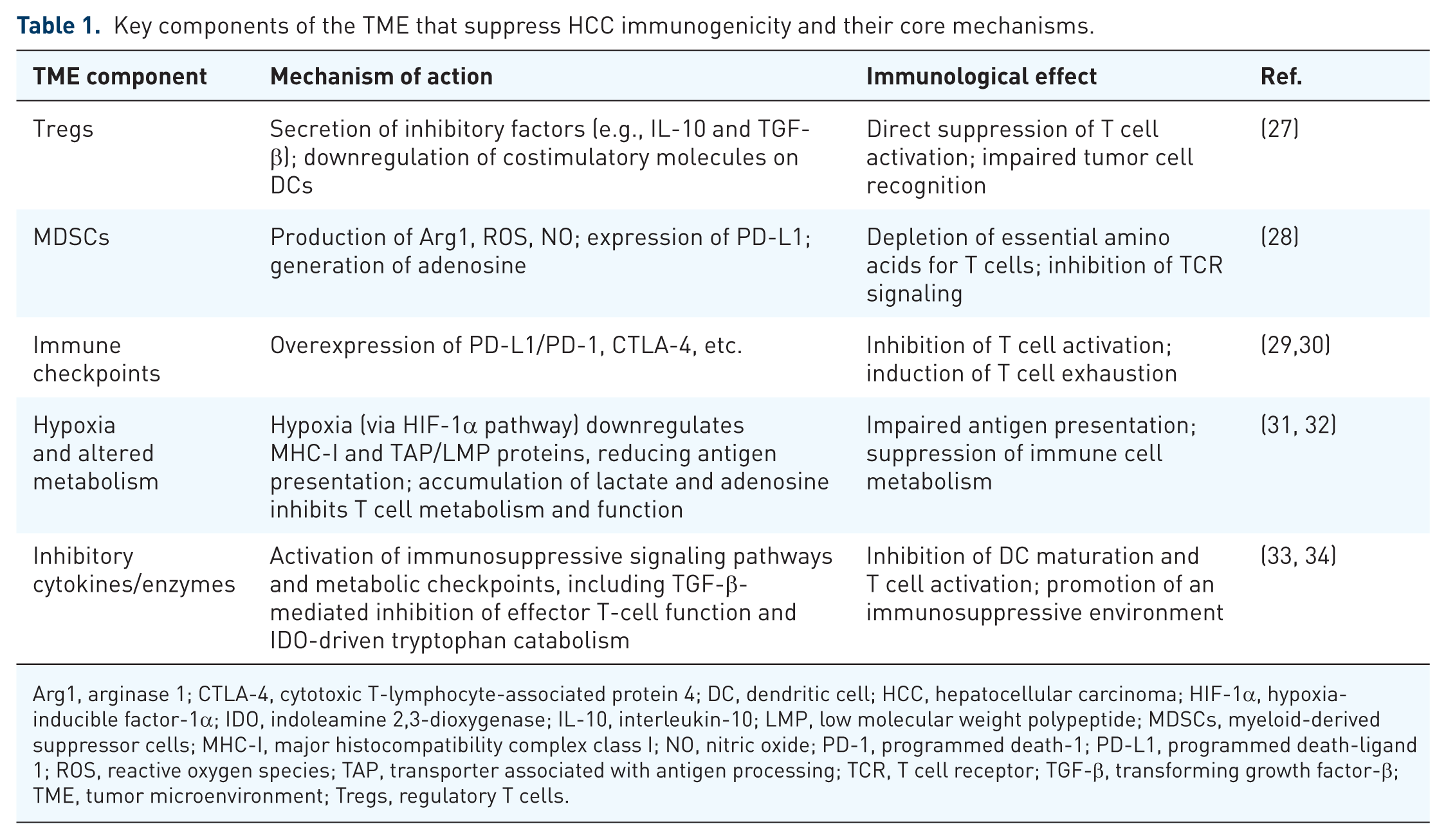
Arg1, arginase 1; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; DC, dendritic cell; HCC, hepatocellular carcinoma; HIF-1α, hypoxia-inducible factor-1α; IDO, indoleamine 2,3-dioxygenase; IL-10, interleukin-10; LMP, low molecular weight polypeptide; MDSCs, myeloid-derived suppressor cells; MHC-I, major histocompatibility complex class I; NO, nitric oxide; PD-1, programmed death-1; PD-L1, programmed death-ligand 1; ROS, reactive oxygen species; TAP, transporter associated with antigen processing; TCR, T cell receptor; TGF-β, transforming growth factor-β; TME, tumor microenvironment; Tregs, regulatory T cells.
At the cellular level, immunosuppressive cells, such as regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), inhibit effector T-cell function through the secretion of inhibitory factors or by depleting metabolic substrates. Simultaneously, hypoxia and elevated lactate levels within the TME further downregulate MHC-I and antigen-processing molecules, thereby exacerbating defects in antigen presentation. Moreover, immune checkpoint molecules are upregulated on both tumor cells and immunosuppressive cells, creating multiple layers of immune evasion. This internally coordinated, multicomponent inhibitory network establishes an immunosuppressive state and contributes to the limited efficacy of ICI monotherapy. Consequently, effectively enhancing the immunogenicity of HCC necessitates not only the correction of intrinsic tumor cell defects but also the alleviation of extrinsic suppression imposed by the TME.
In this immunosuppressive TME, DCs—as professional antigen-presenting cells (APCs) that serve as a critical link between innate and adaptive immunity—occupy a pivotal role, with their functional status directly influencing the immunogenicity of HCC. Medler et al. 12 have emphasized that the conventional subset cDC1 is the principal APC capable of effective cross-presentation and the initiation of CD8+ T-cell responses, with its infiltration into tumors and subsequent maturation playing a crucial role in the activation of antitumor immunity. However, in the context of HCC, immunosuppressive elements within the TME, such as transforming growth factor-β (TGF-β), interleukin-10 (IL-10), and lactate, hinder DC maturation, downregulate costimulatory molecules, and limit DC recruitment and migration, thereby attenuating the initiation of immune responses. 33 Importantly, both preclinical and clinical investigations have demonstrated that interventions, including the activation of the stimulator of interferon genes/type I interferon (STING/IFN-I) pathway or the administration of ex vivo-generated DC vaccines, can activate DCs and restore their functionality, thereby exhibiting potential to reconfigure antitumor immunity. 35 These findings underscore that targeting DCs and restoring their antigen-presenting capacity may represent a promising strategy to enhance antigen presentation and antitumor immune activation.
Strategies to enhance HCC immunogenicity
In HCC, the combination of anti-angiogenic therapy with ICI has become a central paradigm of current systemic treatment. Previous studies have indicated that dysregulated expression of pro-angiogenic factors, particularly vascular endothelial growth factor (VEGF), not only promotes aberrant angiogenesis but also facilitates immune evasion by upregulating PD-L1 expression and impairing DC function, thereby promoting immune escape of tumor cells. 36 In addition, VEGF-driven aberrant angiogenesis further shapes an immunosuppressive TME, impairs antigen presentation and effector T-cell infiltration, and ultimately diminishes tumor immunogenicity. 36 Clinically available anti-angiogenic agents include multi-target tyrosine kinase inhibitors, such as sorafenib and lenvatinib, and monoclonal antibodies targeting the VEGF ligand, represented by bevacizumab. 37 The clinical success of the T+A regimen may derive from its mechanistic synergy: ICI restores antitumor immunity by releasing inhibitory signals on T cells, whereas anti-angiogenic therapy induces vascular normalization, improves tumor perfusion, and alleviates hypoxia, thereby reducing microenvironment-mediated suppression of antigen processing and presentation and preserving antigen-processing machinery.36,37 Through these complementary effects, anti-angiogenic therapy does not directly generate new tumor antigens but enables more efficient presentation and recognition of pre-existing antigens, indirectly enhancing tumor immunogenicity. 36 Nevertheless, although microenvironmental remodeling is essential for effective immunotherapy, it remains insufficient to fully overcome the intrinsically low immunogenicity of HCC, underscoring the need for more proactive immunogenicity-enhancing strategies.
To date, various methodologies have been explored to enhance HCC immunogenicity, including epigenetic drugs, ablation therapies, radiotherapy and chemotherapy, oncolytic viruses (OVs), phototherapies, and cancer vaccines (Figure 2(a)). These strategies often employ multifaceted mechanisms: epigenetic drugs, OVs, and radiochemotherapy not only facilitate the exposure of tumor antigens but also reverse immunosuppression within the TME, whereas vaccine-based approaches deliver precise antigenic signals and modulate the TME. Based on the mechanisms underlying low HCC immunogenicity, these strategies can be categorized into two primary directions: first, enhancing the exposure of endogenous tumor antigens; and second, actively providing exogenous immunogenic signals to the immune system. The former seeks to “awaken” and exploit the tumor’s intrinsic antigen repertoire, while the latter externally equips the immune system with a precise “navigation map,” thereby circumventing the limitations imposed by deficient antigen expression and ITH.
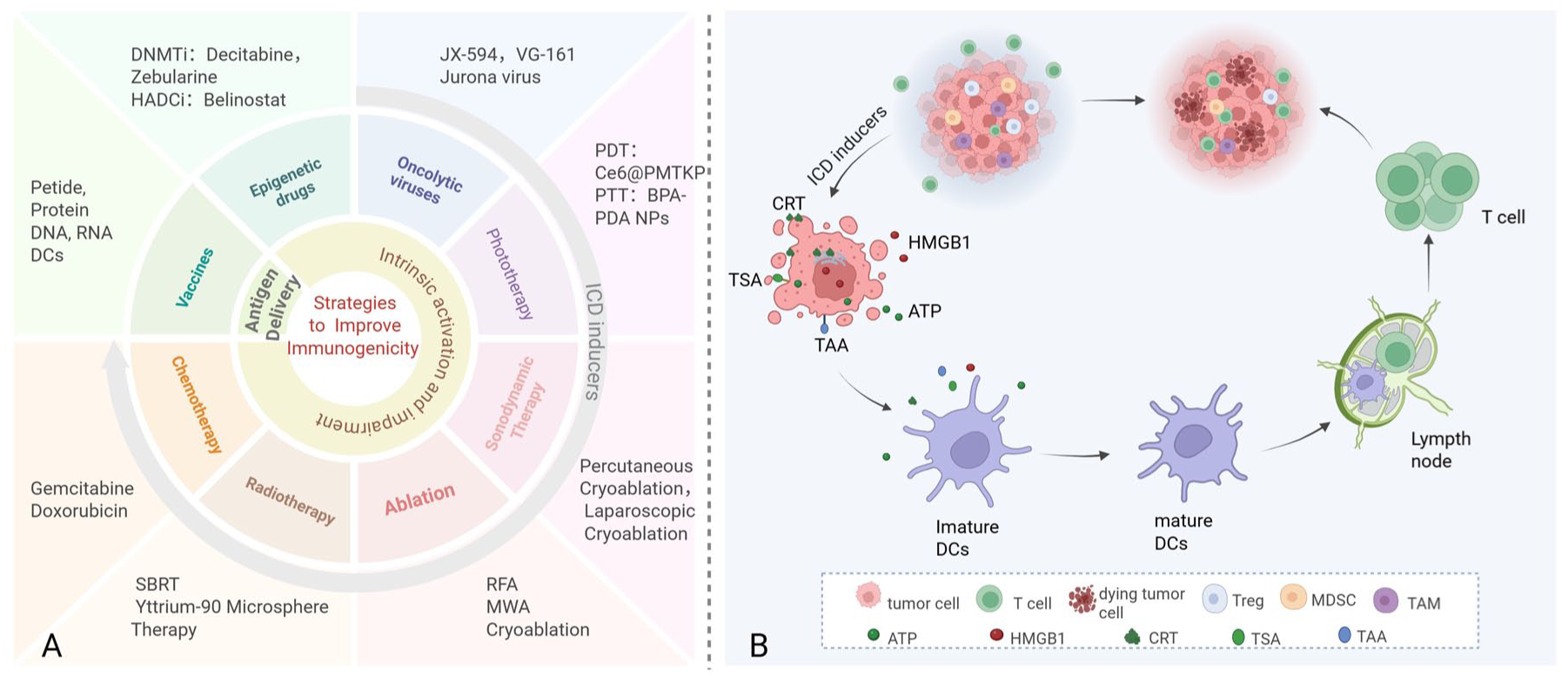
(a) Strategies for enhancing the immunogenicity of HCC. Two principal strategies are employed to enhance HCC immunogenicity: (1) increasing the exposure of endogenous tumor antigens and (2) introducing exogenous immunogenic antigens. The first strategy includes oncolytic virotherapy, phototherapy, sonodynamic therapy, ablation, and radiochemotherapy, all of which can induce ICD in tumor cells and thereby enhance tumor immunogenicity. (b) Mechanism of ICD in tumor cells. ICD inducers trigger tumor cell death accompanied by the exposure of neoantigens or tumor-associated antigens on the cell surface and the release of DAMPs, including HMGB1, ATP, and CRT. ATP acts as a “find-me” signal that recruits DCs into the tumor microenvironment. HMGB1 promotes DC maturation and enhances antigen processing and presentation. CRT exposure on the cell surface serves as an “eat-me” signal that facilitates phagocytosis of tumor cells by DCs. Collectively, these DAMPs orchestrate antitumor immune responses by promoting DC recruitment, maturation, and antigen presentation, enabling activated DCs to migrate to draining lymph nodes. There, DCs prime naïve T cells, ultimately leading to cytotoxic T-cell activation and the elimination of primary and distant tumor lesions.
In the first category of strategies, epigenetic drugs enhance the expression of tumor antigens by reversing the silencing of immune-related genes. Techniques such as ablation therapies, radiotherapy, chemotherapy, OVs, phototherapy, and sonodynamic therapy (SDT) primarily augment the immunogenicity of HCC by inducing immunogenic cell death (ICD). Unlike conventional cell death, ICD not only releases tumor antigens but also emits a specific array of damage-associated molecular patterns (DAMPs), including high-mobility group box 1 (HMGB1), adenosine triphosphate (ATP), and calreticulin (CRT). 38 ATP facilitates the recruitment of DCs; CRT serves as an “eat-me” signal recognized by DCs, enhancing their antigen-presenting capabilities; and HMGB1 interacts with Toll-like receptors 2 and 4 on DCs to promote their maturation. Through these mechanisms, mature DCs effectively cross-present tumor antigens, thereby activating antigen-specific T-cell responses and initiating antitumor immunity 39 (Figure 2(b)). During this process, tumor immunogenicity is enhanced, characterized by upregulated MHC-I expression on tumor cells, increased secretion of proinflammatory cytokines such as IFN-γ and IL-12, and reduced infiltration of immunosuppressive cells. Collectively, these changes enhance the surveillance and clearance of tumor cells. 40
The second strategy focuses on the exogenous delivery of tumor antigens to directly prime and shape specific immune responses. Tumor vaccines serve as a prime example of this approach, delivering selected tumor antigens in the form of peptides, nucleic acids, or cellular carriers to furnish the immune system with defined antigenic targets. By supplying defined antigenic cues independent of endogenous antigen expression, this strategy may overcome antigen loss and heterogeneous antigen distribution caused by ITH.
Epigenetic drugs
Epigenetic dysregulation is a key driver of diminished immunogenicity in HCC. During immunoediting, tumor cells undergo epigenetic alterations that downregulate the expression of TAAs or TSAs, thereby facilitating immune evasion.
DNA methyltransferase inhibitors
DNA methyltransferase inhibitors (DNMTis) have the potential to reverse the hypermethylated state of tumor cells, thereby reactivating tumor antigens that have been silenced through epigenetic mechanisms. Preclinical investigations have shown that decitabine increases the expression of TAAs such as glypican-3 (GPC-3) and alpha-fetoprotein (AFP), thereby enhancing the vulnerability of tumor cells to T-cell-mediated cytotoxicity. 41 A phase I/II clinical trial preliminarily demonstrated that in patients with advanced HCC treated with low-dose decitabine, downregulation of DNMT1 expression and genome-wide DNA hypomethylation were detected in peripheral blood mononuclear cells, suggesting potential antitumor activity mediated through epigenetic modulation and immune response induction. 42 Nevertheless, the clinical application of decitabine is constrained by its dose-dependent myelosuppression and systemic toxicity, which limit its broader use in solid tumors. By contrast, next-generation DNMTis, such as zebularine, have exhibited improved safety profiles and immunostimulatory effects in animal models; however, large-scale clinical validation of these findings remains insufficient. 41
Histone deacetylase inhibitors
Histone deacetylase inhibitors (HDACis) enhance histone acetylation, altering the antigen repertoire of HCC cells by increasing the surface expression of TAAs and upregulating MHC-I and costimulatory molecules, which together enhance tumor immunogenic features. 43 Preclinical studies have shown that micellar nanoparticles co-delivering an HDACi and PD-L1 siRNA, designed by Zhao et al., induce enhanced CD8+ T cell-mediated antitumor immune responses. In HCC animal models, this combination regimen exhibited superior tumor growth suppression and survival benefits compared to monotherapies. 44 Similarly, Llopiz et al. 45 showed that combining the HDACi belinostat with anti-PD-1 therapy reduced tumor volume by 72% and extended median survival to 56 days in HCC models, compared with 21 days in controls. 45 Although HDACis exhibit limited efficacy as monotherapy in solid tumors, they show potential in augmenting the immunogenicity of HCC. Nevertheless, the mechanisms underlying these synergistic effects, as well as optimal dosing schedules and clinical applicability, require further investigation.
Physical ablation
Radiofrequency ablation
Radiofrequency ablation (RFA) is a well-established local therapy for early-stage HCC that also enhances tumor immunogenicity and elicits antitumor immune responses. This is accomplished through the release of tumor antigens, activation of DCs, and modulation of circulating immune cells, thereby fostering an “immune-sensitive” microenvironment that is favorable for subsequent immunotherapeutic interventions.46–48
In clinical practice, RFA is a standard treatment for BCLC stage 0 and selected stage A unresectable HCC, owing to its minimally invasive nature, repeatability, and favorable safety profile, particularly for lesions ⩽3 cm. Although RFA has demonstrated significant potential to activate antitumor immunity, challenges persist, including incomplete ablation leading to local recurrence and hypoxia-induced immunosuppression in the periablation zone. 49 Residual tumor cells may upregulate PD-L1 expression, which interacts with PD-1 on activated T cells, resulting in T-cell exhaustion and enhanced immune evasion. 50 This mechanism underscores the rationale for combining RFA with ICI. Early-phase clinical studies have shown promising efficacy and safety; however, vigilant monitoring is essential to address potential liver function deterioration and recurrence because of incomplete ablation. 51
Microwave ablation
In comparison to RFA, microwave ablation (MWA) results in more extensive tumor necrosis, releases a greater quantity of TAAs, and alters the cytokine environment to facilitate immune activation. 52 A prospective cohort study indicated that 30% of patients with HCC developed specific immune responses following MWA, which was associated with an extended progression-free survival (27.5 months compared to 10.0 months). 53 Further research demonstrated that among patients undergoing MWA combined with surgical resection, those with high levels of tumor-infiltrating T cells experienced a disease-free survival of 37.4 months, significantly longer than the 13.1 months observed in the low-infiltration group, suggesting the sustained immunologic effects of MWA. 53 Due to its shorter procedure times, larger ablation zones, and reduced susceptibility to heat-sink effects, MWA is increasingly replacing RFA and shows potential in enhancing immunogenicity, positioning it as a promising candidate for combination immunotherapy. 52
Cryoablation
In comparison to RFA and MWA, cryoablation exhibits enhanced local control in the treatment of HCC and induces adaptive immune responses characterized by relative safety and efficacy. 54 Mechanistically, cryoablation differs from RFA and MWA by destroying tumor cells through extreme cold, which results in the release of immunogenic native antigens, as opposed to the denatured antigens produced by RFA and MWA. This process establishes an in situ antigen reservoir within the tumor, which may trigger a “cryoimmunologic response.” 55 Preclinical studies have demonstrated that cryoablation in conjunction with CpG or CpG plus PD-1 inhibitors enhances the infiltration of cytotoxic T lymphocytes. 56 A randomized controlled trial has shown that, for HCC lesions measuring more than 3 cm, cryoablation achieves better local control compared to RFA, with a local progression rate of 7.7% versus 18.2%, while maintaining comparable safety profiles. 54 Currently, clinical evidence supporting the combination of cryoablation with immunotherapy remains limited, and several ongoing trials are assessing its long-term efficacy (Table 2).
Completed or ongoing clinical trials of cryoablation combined with immunotherapy.
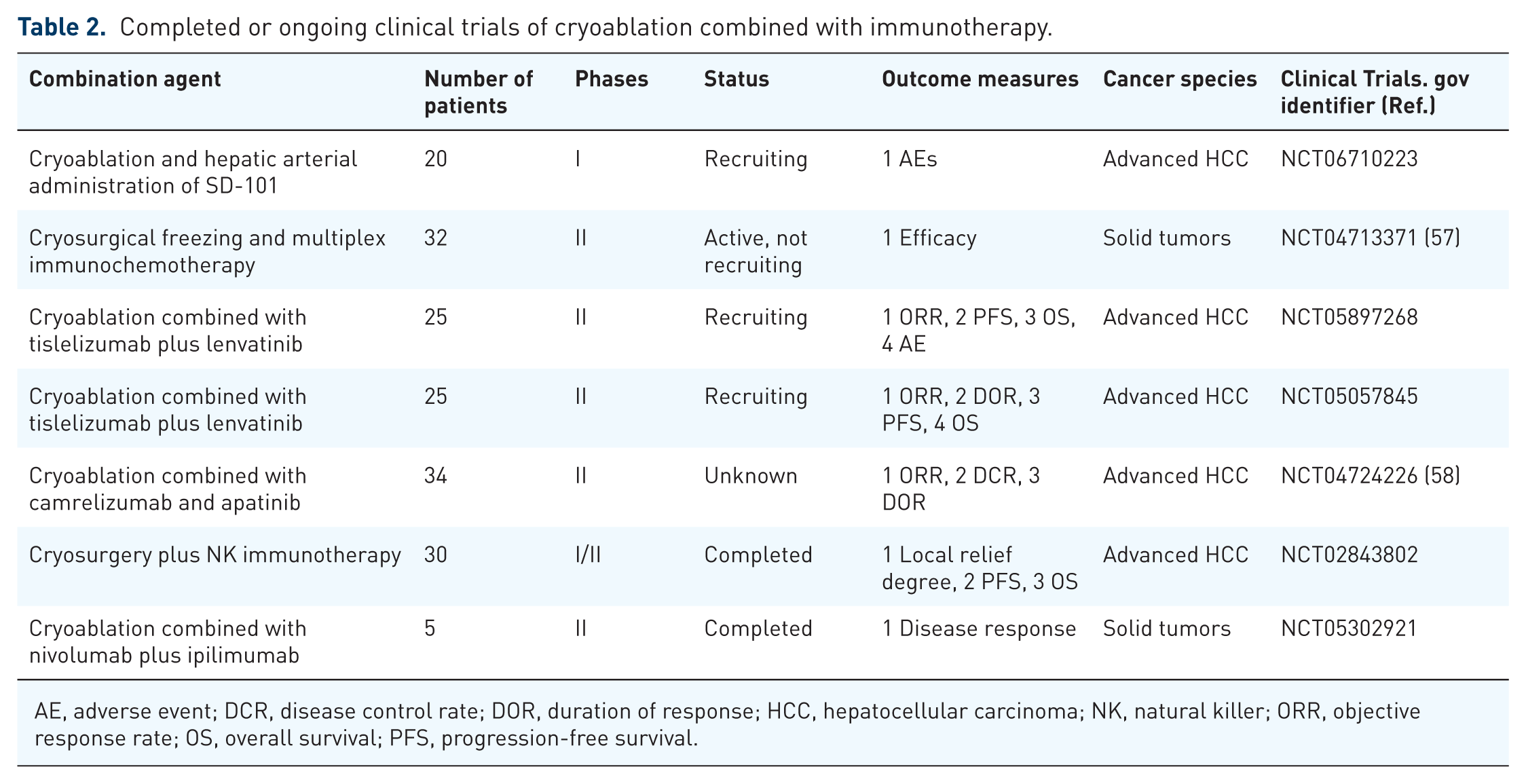
AE, adverse event; DCR, disease control rate; DOR, duration of response; HCC, hepatocellular carcinoma; NK, natural killer; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
Radiotherapy
Radiotherapy enhances tumor immunogenicity through the induction of DNA damage, which subsequently triggers genomic instability and upregulates the expression of TSAs and MHC-I molecules. 59 Furthermore, radiotherapy induces reactive oxygen species (ROS) stress, which can trigger ICD, thereby amplifying antitumor immune responses. Yttrium-90 radioembolization (Y90-RE) significantly increases the proportion of tumor-infiltrating CD8+ T cells, reduces Treg levels, and enhances APC function. 60 Radiotherapy not only augments immunogenicity within the irradiated field but has been reported to induce an “abscopal effect,” wherein distant, non-irradiated lesions regress due to systemic immune activation. 61 The preclinical study has suggested that the combination of radiotherapy with PD-L1 inhibitors more effectively induces abscopal effects compared to monotherapy. 62 A pooled analysis by Theelen et al. 63 of the PEMBRO-RT and MDACC trials demonstrated that the group receiving radiotherapy plus pembrolizumab achieved higher out-of-field response rates (41.7% vs 19.7%) and longer median OS (19.2 vs 8.7 months) compared to those receiving pembrolizumab alone.
Chemotherapeutic agents
Traditionally, chemotherapeutic agents have been extensively utilized for their direct cytotoxic effects on tumor cells. However, recent research has demonstrated that these drugs also impact tumor immunogenicity. Chemotherapy can enhance T-cell-mediated recognition and cytotoxicity by inducing and promoting tumor antigen release, upregulating MHC-I and B7-1 molecules through inflammatory signals such as IFN-γ and TNF-α. 64 Certain agents, such as cyclophosphamide and taxanes, can selectively deplete Tregs and MDSCs, thereby reducing the secretion of immunosuppressive factors, such as IL-10 and TGF-β. 64
Clinical evidence further supports the synergistic effects of chemotherapy combined with immunotherapy. For instance, in microsatellite-stable (MSS) colorectal cancer (CRC), the METIMMOX study (NCT03388190) reported that oxaliplatin combined with nivolumab achieved complete responses in 16% of patients, whereas oxaliplatin monotherapy produced none. 65 This suggests that short-course oxaliplatin-based treatment may convert MSS CRC into an immunogenic state, thereby enhancing ICI responsiveness. In HCC, a phase Ib/II trial (NCT03092895) showed that camrelizumab combined with the FOLFOX4 regimen yielded an ORR of 29.4% and a disease control rate (DCR) of 79.4% in advanced HCC patients. 66 More encouragingly, a retrospective study indicates that hepatic arterial infusion chemotherapy combined with ICI and targeted therapy further increased ORR and DCR to 70.4% and 88.9%, respectively. 67 These findings indicate that chemotherapy may enhance tumor immunogenicity, providing a critical window for synergistic immunotherapy.
Oncolytic viruses
OVs, either naturally occurring or genetically engineered, are specialized viruses that preferentially target and lyse tumor cells while sparing normal tissues. These viruses enhance the immunogenicity of HCC through several mechanisms: OVs selectively replicate within tumor cells, leading to cell lysis and the release of abundant TAAs. In addition, they can induce ICD, thereby promoting the release of immunostimulatory signals and activation of antitumor immune responses, as described above (Figure 3). 68 Advances in genetic engineering have further augmented the therapeutic value of OVs.

Mechanisms of OVs in antitumor therapy. (a) Selective tumor targeting and lysis. OVs exhibit preferential tropism toward tumor cells and selectively replicate within them, leading to direct tumor cell lysis and immunogenic cell death. (b) Immunogenic cell death and immune activation. Virus-mediated oncolysis induces the release of tumor-associated antigens, DAMPs, and PAMPs, which promote DC activation and CTL infiltration. In parallel, viral infection stimulates interferon and chemokine production, enhancing MHC-I-mediated antigen presentation, recruiting tumor-specific CD8+T cells, and triggering systemic antitumor immune responses. (c) Genetic engineering for enhanced therapeutic efficacy. Genetic modification of OVs improves tumor selectivity and therapeutic potency while reducing off-target cytotoxicity toward normal tissues, thereby enhancing overall safety and efficacy.
Building upon these mechanisms, OVs have been investigated as an approach to enhance antitumor immunity in HCC. For instance, the oncolytic vaccinia virus JX-594 (Pexa-Vec) has demonstrated the ability to activate systemic immune responses in early-phase clinical trials, showing manageable safety and modest efficacy even in cases of advanced HCC resistant to sorafenib, thereby indicating its potential as an immune-sensitizing agent.69,70 Nevertheless, the phase III PHOCUS trial of JX-594 did not achieve its survival endpoint, underscoring the limitations of its application as a monotherapy. 71 Recent research has increasingly concentrated on the combination of genetically engineered OVs with ICI. For example, a multicenter phase I study demonstrated that treatment with VG161, an engineered OV, enhanced the efficacy of ICI and achieved ORR of 18.92% and a median OS of 12.4 months in patients with refractory HCC. 72 Similarly, Tesfay et al. 73 developed a novel OV, the Jurona virus, which, when used in conjunction with anti-PD-L1 antibodies in HCC mouse models, reduced tumor volume, prolonged survival, increased CD8+ T-cell infiltration, and decreased Tregs proportion. Despite these promising findings, most studies on OV–ICI combinations remain at the preclinical stage, and further clinical validation is required.
Phototherapy
Photodynamic therapy
Photodynamic therapy (PDT) utilizes photosensitizers that, upon activation by specific wavelengths of light, generate ROS. This oxidative stress induces ICD, thereby enhancing antigen-presenting function. 74
Extensive preclinical investigations have demonstrated that PDT can enhance the efficacy of PD-1/PD-L1 inhibitors, mitigate distant metastases, and induce immunological memory. 75 Modifications based on nanotechnology have been shown to improve the tumor-targeting capabilities of PDT and enhance its effectiveness under hypoxic conditions. 76 For instance, the Ce6@PMTKP nanoplatform, developed by Gao et al., integrates PDT with chemotherapy, thereby not only augmenting tumor clearance but also remodeling the tumor immune microenvironment. When combined with ICI, this platform successfully eradicated primary tumors and inhibited the growth of metastatic lesions. 77 Currently, the clinical application of PDT is predominantly confined to superficial tumors, such as basal cell carcinoma, because of its limited efficacy in deep-seated tumors, which is constrained by the restricted tissue penetration of light. 78 Consequently, high-level clinical evidence in HCC remains scarce, and PDT has not yet demonstrated sufficient impact to alter standard first-line treatment paradigms.
Photothermal therapy
Photothermal therapy (PTT) induces localized hyperthermia within tumors through selective photothermal conversion, leading to tumor cell death and the exposure of tumor antigens, thereby enhancing tumor immunogenicity. A notable advantage of PTT is its oxygen-independent mechanism, which permits the induction of ICD even in hypoxic TMEs. 79 Research has demonstrated that PTT upregulates intracellular heat shock protein 70 in tumor cells, which acts as an immunoadjuvant-like molecule, facilitating immune activation and enhancing CD8+ T-cell responses. 80 Further investigations have revealed that engineered nanomaterials can augment both the therapeutic efficacy and immunostimulatory effects of PTT. In the context of HCC, boronated phenylalanine-modified polydopamine nanoparticles have been developed to selectively accumulate via the highly expressed L-type amino acid transporter 1. 81 These nanoparticles enable concurrent execution of PTT-mediated tumor ablation and sorafenib delivery, thereby not only enhancing tumor cell cytotoxicity but also suppressing Tregs and MDSCs to counteract immunosuppression. When combined with anti-PD-L1 inhibitors, this approach achieved a 50% complete response rate in HCC-bearing mice, with a 1-year tumor recurrence rate of only 20%, markedly lower than the 60% observed in the PTT monotherapy group. 81
Sonodynamic therapy
SDT utilizes ultrasound to activate sonosensitizers, resulting in the concurrent production of ROS and cavitation effects, which collectively induce dual-mode damage to tumor cells. 82 In comparison to PTT and PDT, SDT offers superior tissue penetration, is noninvasive, and does not depend on light sources, rendering it particularly advantageous for the treatment of deeply located HCC lesions. 83 A preclinical study has shown that SDT facilitates the release of DAMPs and reduces immunosuppressive cell populations within the TME. 84 Recent investigations have highlighted that SDT can act as an “in situ vaccine,” augmenting tumor immunogenicity and activating anti-tumor immune responses, thereby suggesting its potential role as an immune therapy “initiator” or “amplifier.”85,86 Xu et al. 86 reviewed the recent advances in SDT-based cancer treatment, highlighting that the combination of SDT with multiple therapeutic modalities, including ICI and chemotherapy, can synergistically enhance antitumor efficacy, while emphasizing that further research is needed to facilitate the clinical translation of this combined strategy. Although some studies have investigated the use of SDT in refractory breast cancer, there is currently a paucity of clinical evidence supporting its efficacy in HCC. 84 Furthermore, the pharmacokinetics and long-term safety of sonosensitizers in the liver remain incompletely understood, and the frequent occurrence of compromised hepatic reserve in HCC patients may further constrain the safety and broader application of SDT.
Tumor antigen vaccines
Tumor vaccines, a prototypical exogenous delivery strategy, can be primarily categorized into peptide vaccines, nucleic acid vaccines, and DC-based vaccines (Figure 4). The subsequent sections will provide a comprehensive analysis of the mechanisms of action and current research advancements for each vaccine type.

Vaccine-mediated enhancement of tumor immunogenicity. Peptide and nucleic acid vaccines rely on host APCs for antigen processing and subsequent T-cell activation. In contrast, DC-based vaccines adopt an ex vivo strategy, in which DCs are loaded with tumor antigens via tumor cell fusion, antigen pulsing, or genetic transfection before reinfusion into patients. With adjuvant support, these engineered DCs efficiently migrate to draining lymph nodes, where they enhance antigen presentation and promote robust T-cell activation, thereby amplifying antitumor immune responses.
Peptide vaccines
Peptide vaccines targeting TAAs such as GPC-3 and AFP have shown favorable safety profiles in HCC and can elicit antigen-specific immune responses. Previous studies have found that GPC-3 peptide vaccines induce antigen-specific immunity, 87 while AFP vaccines, which have been optimized through epitope engineering and delivered via lentiviral vectors, enhance antigen immunogenicity and activate CD8+ T-cell responses. 88 Building on the theoretical advantages of TSAs discussed above, personalized neoantigen vaccines have emerged as a promising peptide vaccine strategy in HCC, particularly when combined with ICI. For example, a phase I/II clinical trial (NCT04251117) demonstrated that a personalized neoantigen vaccine combined with pembrolizumab achieved ORR of 30.6% in advanced HCC, which surpasses the 16.9% ORR previously reported for pembrolizumab monotherapy. 89 Furthermore, the use of nanoparticle carriers and adjuvant technologies can enhance the delivery to lymph nodes and the immunogenicity of peptide vaccines. 90 It is important to acknowledge that vaccines based on TAAs are vulnerable to suppression by the TME and may result in selective immune evasion. In contrast, vaccines based on TSAs face challenges in clinical translation due to the technical and temporal demands associated with neoantigen prediction and production.
Nucleic acid vaccines
Nucleic acid vaccines enhance the immunogenicity of HCC by delivering exogenous nucleic acids that encode TAAs or TSAs, thereby facilitating the in vivo expression of target antigens. DNA vaccines, which utilize plasmid vectors, offer the advantage of prolonged antigen expression in vivo; however, their efficacy is constrained by low delivery efficiency and potential risks associated with genomic integration. Conversely, mRNA vaccines do not require nuclear entry, allowing for direct cytoplasmic translation of antigens and mitigating the risks of genomic integration.91,92 Furthermore, the production of mRNA is more straightforward and scalable, positioning it as a focal point in contemporary nucleic acid vaccine research. 91 Preliminary clinical trials targeting gastrointestinal cancers (NCT03480152) have shown that mRNA vaccines can effectively induce neoantigen-specific T cell responses in patients, thereby providing evidence of immune activation within solid tumors. 93
Circular RNA (circRNA), as an emerging RNA vaccine platform, features a covalently closed loop structure, which confers resistance to nuclease degradation, thereby addressing the short half-life limitation of conventional linear RNA and facilitating more sustained antigen expression in vivo. Preclinical studies have shown that circRNA-based vaccines improve neoantigen stability and inhibit tumor growth while promoting T-cell infiltration and tumor cell apoptosis. 94 This study suggests that circRNA may serve as a stable platform for sustained antigen expression.
DC-based vaccines
DC-based vaccines, recognized for their exceptional antigen-presenting capabilities, are regarded as an optimal platform for augmenting HCC immunogenicity. By loading DCs with tumor lysates or transfecting them with plasmid DNA or mRNA, a comprehensive antigen repertoire can be delivered, facilitating broad-spectrum immune activation. This characteristic is particularly beneficial for addressing the pronounced heterogeneity that is characteristic of HCC. 95
Clinical investigations have indicated that DC vaccines possess favorable safety profiles and demonstrate potential efficacy in HCC. An initial phase II trial utilizing HepG2 lysate-pulsed DC vaccines in patients with advanced HCC reported an absence of severe toxicities, with a subset of patients experiencing tumor regression, disease stabilization, and reductions in AFP levels. 96 Another phase II trial involving personalized neoantigen-loaded DC vaccines in conjunction with T cell therapy revealed that 70% of patients developed antigen-specific T cell responses, and 71.4% maintained recurrence-free survival at 2 years. 97 A randomized controlled trial (NCT03674073) demonstrated that the neoantigen-loaded DC vaccine (LK101) elicits broad neoantigen-specific T-cell responses and promotes the expansion of CD4+ and CD8+ effector memory T cells. HCC patients who received LK101 in combination with ablation therapy exhibited no mortality and a low recurrence rate during the study follow-up. 98 Preclinical studies further indicate that DC vaccines combined with ICI have exhibited synergistic effects; in sorafenib-refractory advanced HCC, the combination of DC vaccines and pembrolizumab achieved ORR of 33.3%. 99 These findings support the use of DC vaccines in HCC, although their long-term efficacy and safety require validation in larger clinical trials.
Conclusion and perspectives
The advent of ICI has revolutionized cancer therapy; however, the limitations in antigen presentation and immune activation remain major barriers to therapeutic efficacy. Existing reviews have primarily focused on immune escape mechanisms or clinical efficacy, prioritizing treatment outcomes over tumor immunogenicity as the fundamental driver of immunotherapy response. In this review, we conceptualize HCC immunogenicity as a dynamic and therapeutically remodelable property. By integrating intrinsic tumor characteristics with extrinsic microenvironmental regulation, we propose an immunogenicity-centered framework in which diverse therapeutic modalities, including epigenetic therapies, locoregional interventions, radiotherapy, chemotherapy, OVs, and tumor vaccines, are unified under the common objective of enhancing tumor immunogenicity. This framework provides a coherent explanation for heterogeneous clinical responses and resistance patterns observed in HCC immunotherapy and offers a mechanism-guided alternative to empirically assembled combination strategies, thereby supporting the development of more precise and patient-tailored therapeutic regimens.
Despite the conceptual advances in immunogenicity remodeling, achieving consistent clinical benefit for patients with HCC remains challenging. First, the lack of robust predictive biomarkers limits the precise application of immunotherapy. Current indicators used to identify potential beneficiaries and predict therapeutic outcomes are still insufficiently developed, and candidate biomarkers such as TMB, immune-related gene signatures, and the integrity of antigen presentation pathways require further validation in prospective clinical studies. Second, patient selection is highly complex. HCC exhibits marked etiological heterogeneity, variability in tumor biology, and differing levels of hepatic functional reserve, all of which significantly influence immune responsiveness and treatment tolerance. Third, toxicity and safety require continued careful consideration, particularly in the context of underlying liver disease. Immune-related hepatitis and the cumulative toxicities associated with multimodal combination therapies require careful evaluation and management.
Technological innovation offers new opportunities for improving HCC immunogenicity. In particular, artificial intelligence-based neoantigen prediction tools provide a feasible approach for neoantigen identification. In clinical practice, multi-omics profiling of tumor tissue and blood samples can be performed and combined with computational algorithms to integrate mutational data, antigen presentation capacity, and expression levels to screen and prioritize potential neoantigens. This approach may improve antigen recognition, even in the context of low TMB and provide more clinically meaningful targets for personalized vaccines. At the same time, such tools may also assist in therapeutic response prediction, resistance mechanism analysis, and the design of combination treatment strategies, and can ultimately be incorporated into multidisciplinary decision-making in a standardized manner. Although challenges remain in terms of assay standardization, turnaround time, and clinical validation, these technologies already demonstrate the feasibility of gradual integration into clinical workflows and may support the implementation of precision immunotherapy. In summary, overcoming HCC immune tolerance is unlikely with single treatments. A comprehensive approach that integrates “antigen release—enhanced presentation—immunosuppression reversal,” backed by technological innovations for personalized combination therapies, may provide a rational framework for reshaping tumor immunogenicity and improving long-term clinical outcomes.