
Abstract
Therapeutic decision-making for older adults, operationally defined in this review as patients aged ⩾65 years, with extensive-stage small-cell lung cancer (ES-SCLC) remains clinically challenging, complicated by heterogeneous decline in physiological reserve, multiple comorbidities, and narrow therapeutic indices. Although chemoimmunotherapy has redefined the first-line standard of care, the selection bias inherent in pivotal registrational randomized controlled trials—which often exclude the oldest-old and frail patients—limits the generalizability of their efficacy and safety profiles within complex real-world populations. As the therapeutic armamentarium expands, emerging modalities such as small-molecule anti-angiogenic agents, hypofractionated or adaptive radiotherapy, and novel molecular therapies (e.g., lurbinectedin and delta-like ligand 3-targeting constructs) offer tailored therapeutic avenues for this demographic. However, a pronounced evidence gap persists regarding geriatric-specific toxicity and functional endpoints within the existing evidence hierarchy. Consequently, the integration of Comprehensive Geriatric Assessment (CGA) for functional status stratification is imperative to navigate current therapeutic bottlenecks. The objective of this narrative review is to summarize recent therapeutic advances in older adults with ES-SCLC, critically examine the limitations of current evidence, and propose a CGA-guided framework for risk-adapted clinical decision-making and holistic management.
Plain language summary
Small-cell lung cancer is an aggressive disease that commonly affects older adults. Unfortunately, most clinical trials test new treatments on younger, healthier people, excluding those who are very old or frail. This creates a significant “evidence gap,” leaving doctors unsure of how to safely treat elderly patients who often have other serious health conditions, such as heart or lung disease. This paper reviews the latest medical advances and proposes a new way to solve this problem. We argue that a patient’s birth age should not be the only factor doctors use to make treatment decisions. Instead, we recommend using a detailed health check called a “Comprehensive Geriatric Assessment.” This assessment evaluates a patient’s physical strength, memory, and ability to perform daily activities, giving a clearer picture of their overall health. Based on this assessment, we provide a framework to classify patients into three groups: “Fit,” “Vulnerable,” or “Frail.” Fit patients are strong enough to receive standard, full-dose treatments. Vulnerable patients may receive adjusted treatments, such as lower chemotherapy doses, to reduce dangerous side effects. Frail patients may benefit most from care focused on comfort and maintaining quality of life rather than aggressive treatment. This personalized approach aims to give older adults the best chance of survival while protecting them from treatments that might be too harsh for their bodies.
Keywords
Introduction
Small-cell lung cancer (SCLC) represents a highly aggressive neuroendocrine malignancy. Despite comprising approximately 15% of all lung cancer cases, it has long been associated with a dismal prognosis driven by a high proliferation index and early micrometastatic dissemination. 1 Approximately 70% of patients present with extensive-stage small-cell lung cancer (ES-SCLC) at diagnosis. While this subtype demonstrates a high initial response rate to cytotoxic therapy, rapid recurrence is inevitable. Consequently, the traditional standard regimen based on etoposide plus platinum (EP) has historically plateaued at a median overall survival (mOS) of approximately 10 months.2,3 Since 2018, the integration of immune checkpoint inhibitors (ICIs) with chemotherapy has established a new first-line standard of care, marking a new era of chemoimmunotherapy for SCLC. 4 However, this paradigm shift has also exposed important limitations in the applicability of current trial evidence: the median age at SCLC diagnosis is approximately 70 years 5 ; yet, pivotal registrational randomized controlled trials (RCTs)—constrained by stringent performance status (PS) criteria and comorbidity exclusions—have resulted in significant underrepresentation of older and frail patients.6,7 This ambiguity limits the generalizability of standard chemoimmunotherapy within real-world older cohorts, leaving the benefit-risk ratio without sufficient evidence-based substantiation.
To maintain consistency throughout this review, “older adults” are operationally defined as patients aged ⩾65 years, a cutoff commonly adopted in geriatric oncology research and clinical guideline frameworks. This age threshold is not intended to substitute for biological age or functional reserve; therefore, trial-specific age cutoffs such as ⩾70 or ⩾75 years are discussed separately when applicable. Notably, the median age at diagnosis for SCLC is approximately 70 years, indicating that older patients constitute a major population in ES-SCLC clinical practice. Older adults with ES-SCLC constitute not merely a demographic defined by advanced age, but a distinct cohort characterized by high clinical heterogeneity and physiological frailty. 8 Beyond the inherent aggressiveness of the tumor, the frequent asynchrony between chronological and biological age complicates therapeutic decision-making. The decline in organ reserve, the burden of complex comorbidities (e.g., chronic obstructive pulmonary disease (COPD), cardiovascular diseases), and polypharmacy significantly narrow the therapeutic index.8,9 Previous studies indicate that older patients are more susceptible to treatment-induced disruption of physiological homeostasis and impaired tissue repair capacity, thereby lowering the tolerance threshold for combined regimens. 10 Nevertheless, prospective, stratified research specifically targeting older adults with ES-SCLC remains scarce. Clinical decision-making relies predominantly on indirect inferences from RCT subgroup analyses or retrospective data, leaving clinicians in a constant dilemma of balancing therapeutic efficacy against potential toxicity risks. 11
Given these challenges, the clinical management of older adults with ES-SCLC urgently necessitates a paradigm shift from a “one-size-fits-all” standard approach to a precision decision-making framework grounded in multidimensional assessment, risk stratification, and holistic management. 11 The objective of this narrative review is to summarize the therapeutic evolution of ES-SCLC in older adults in the immunotherapy era, critically examine the limitations of applying current trial evidence to real-world older populations, and provide a clinically relevant framework for comprehensive geriatric assessment (CGA)-guided, risk-adapted decision-making and holistic management. The ultimate aim is to support more individualized and clinically applicable diagnostic and treatment pathways for this vulnerable population. The conceptual framework of therapeutic challenges and evolving strategies in older adults with ES-SCLC is illustrated in Figure 1.
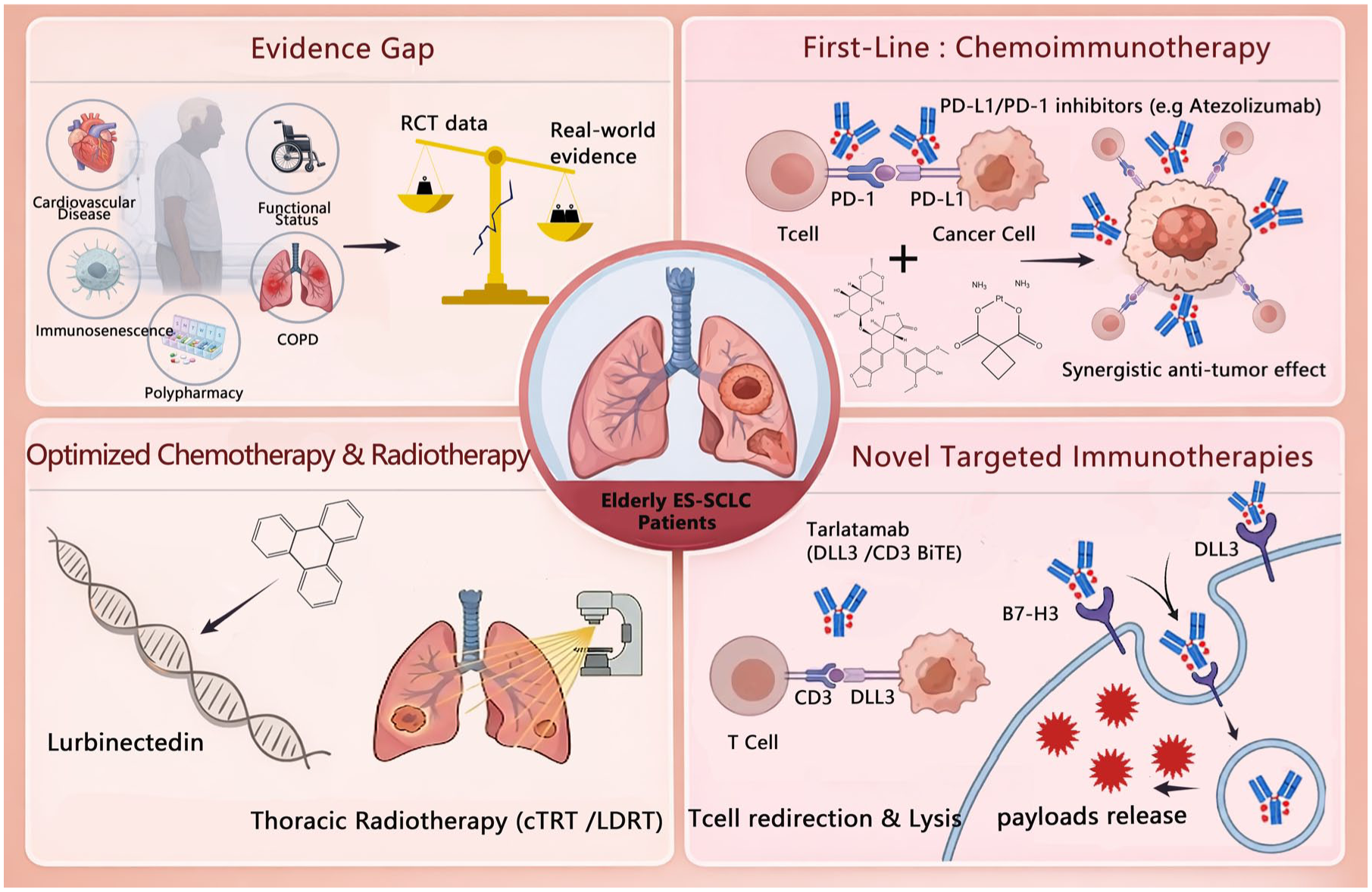
Overview of the therapeutic landscape and evolving management strategies for elderly ES-SCLC. The figure illustrates the paradigm shift from evidence gaps to precision medicine. (Top left) The evidence gap: Elderly patients are characterized by high heterogeneity, including cardiovascular disease, immunosenescence, polypharmacy, and functional decline (e.g., COPD). A significant disparity exists between RCT data and real-world evidence due to strict exclusion criteria. (Top right) First-line standard: Chemoimmunotherapy (platinum/etoposide + PD-L1/PD-1 inhibitors like atezolizumab) is the established standard, leveraging the synergistic effect of cytotoxic killing and immune activation against cancer cells. (Bottom left) Optimization strategies: For specific subgroups, novel transcriptional inhibitors (lurbinectedin) and thoracic radiotherapy (cTRT/LDRT) offer optimized therapeutic indices. (Bottom right) Future horizons: Novel targeted immunotherapies, including DLL3-targeting BiTEs (e.g., tarlatamab) and B7-H3 ADCs, mediate MHC-independent T-cell redirection and precise payload delivery, respectively, reshaping the landscape for relapsed/refractory patients.
Clinical heterogeneity and therapeutic implications in elderly ES-SCLC
The representation gap in evidence-based medicine
In current oncological practice, a unified definition of the “elderly” population remains elusive. 12 Although clinical trials frequently utilize chronological age cutoffs of 65 or 70 years, there is a consensus that chronological age is a poor surrogate for a patient’s functional reserve and biological frailty. 13 This reliance on arbitrary age thresholds has perpetuated a consistent underrepresentation of the elderly within RCTs. 14 Data indicate that while patients aged ⩾65 years constitute 66.6% of the real-world SCLC population, they account for merely 42.9% in pivotal RCTs. This “evidence gap” is particularly pronounced in the oldest-old, with a staggering disparity between real-world and trial proportions for those aged ⩾75 years (27.5% vs 8.5%). Such exclusionary criteria severely compromise the external validity of RCT data, implying that the efficacy and safety of standard first-line regimens (e.g., immunotherapy plus EP) in elderly ES-SCLC lack generalizable evidentiary support. 15 Given the scarcity of high-quality prospective data, clinical decision-making is reduced to navigating a precarious balance between potential benefits and toxicity risks, where slight deviations can lead to either undertreatment or treatment-related morbidity.6,14,16
Multidimensional physiological heterogeneity and therapeutic tolerance
Elderly ES-SCLC patients exhibit unique physiological heterogeneity, where therapeutic complexity arises from the interplay of multidimensional pathophysiological factors rather than chronological aging alone. Foremost, comorbidity burden and polypharmacy create a complex pharmacological landscape. 17 Epidemiological data suggest that approximately 66% of elderly SCLC patients present with at least one chronic condition 8 ; long-term smoking history induces systemic vascular endothelial injury and chronic inflammation, fundamentally compromising the body’s physiological reserve.18,19 Concurrently, drug-drug interactions driven by polypharmacy may significantly alter the pharmacokinetics of antineoplastic agents. 20
Furthermore, functional decline and sarcopenia serve as core predictors of treatment tolerance. 21 Although the Eastern Cooperative Oncology Group performance status (ECOG PS) score is a classic prognostic factor, approximately 60% of elderly patients present with a PS ⩾2 at diagnosis, and PS alone often underestimates occult frailty—a functional limitation resulting from the synergistic effects of cancer cachexia and age-related sarcopenia.22–24 Physiologically, elderly patients are often characterized by reduced hepatic and renal blood perfusion and diminished bone marrow hematopoietic reserve. 25 These changes precipitate decreased clearance and prolonged half-life of cytotoxic drugs (e.g., etoposide), which significantly narrows the therapeutic index for myelosuppression and mucosal toxicity.20,26 Therefore, the development of treatment regimens for geriatric patients necessitates a paradigm shift from standardized dosing models to individualized dose adjustments based on organ function. For etoposide, dose modification should be quantitatively guided, with renal function serving as the central metric. For patients with creatinine clearance of 15–50 mL/min, an initial 25% dose reduction, corresponding to 75% of the planned dose, is generally recommended. 27 In Vulnerable patients without overt renal impairment but with impaired Instrumental Activities of Daily Living (IADL), sarcopenia, borderline marrow reserve, hypoalbuminemia, or prior grade ⩾3 hematologic toxicity, a pragmatic initial etoposide reduction of approximately 20%–25% may be considered, followed by cycle-by-cycle titration according to hematologic recovery and non-hematologic toxicity. 28 Furthermore, in patients with markedly deteriorated renal function, recurrent severe toxicity, or those classified as Frail by CGA, more substantial dose reduction up to 50% or extension of the dosing interval should be considered.28,29 It should be emphasized that dose attenuation in Vulnerable patients is not intended as a universal dose-reduction strategy, but rather as an initial risk-adapted approach for patients with impaired functional reserve, borderline organ function, or high predicted chemotherapy toxicity; subsequent dose escalation may be considered if cycle-1 tolerance is favorable.
Consequently, treatment planning for older adults with ES-SCLC must transcend chronological age thresholds and shift toward individualized decision-making based on functional status, comorbidity burden, and pharmacokinetic vulnerability.
Immunosenescence and remodeling of the tumor microenvironment
The efficacy of ICIs is contingent upon the integrity of the host immune system; however, immunosenescence may significantly alter the benefit-risk profile in elderly ES-SCLC patients. 21 Mechanistically, thymic involution precipitates a decline in naïve T-cell output and restriction of T-cell receptor diversity, thereby impairing the capacity for neoantigen recognition and clonal expansion. 30 Concurrently, age-related “inflammaging”—characterized by chronic low-grade systemic inflammation—facilitates the recruitment of immunosuppressive populations such as myeloid-derived suppressor cells and regulatory T cells (Tregs), fostering an immunosuppressive tumor microenvironment (TME).21,31 These biological alterations may predispose certain elderly cohorts to primary resistance against programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) blockade.
Importantly, immunosenescence does not preclude immunotherapy; rather, it underscores the complexity of clinical phenotypes. Immune-related adverse events (irAEs) in this population are often clinically subtle, exhibit protracted recovery, and may mimic underlying comorbidities.32,33 Therefore, this biological context mandates a strategic shift from “reactive management” to “proactive surveillance,” leveraging intensified baseline immune and frailty assessments to identify potential beneficiaries and optimize risk stratification.34,35
Chemoimmunotherapy: Paradigm shift and real-world challenges
Following a decades-long therapeutic plateau defined by the EP regimen, the introduction of ICIs has redefined the first-line treatment landscape for ES-SCLC. 4 Although older adults were underrepresented in early pivotal registrational RCTs, subgroup analyses from multiple landmark studies have supported the use of chemoimmunotherapy in selected older adults with preserved functional status. The key phase III trials and available elderly subgroup data are summarized in Table 1, illustrating the evolution of first-line treatment strategies from PD-L1 inhibitor-based combinations to emerging PD-1 inhibitor-based regimens. However, these findings should not be directly extrapolated to frail, multimorbid, or oldest-old patients without CGA-based risk stratification.
Overview of key phase III clinical trials of first-line immunotherapy combinations in ES-SCLC with elderly subgroup analysis.
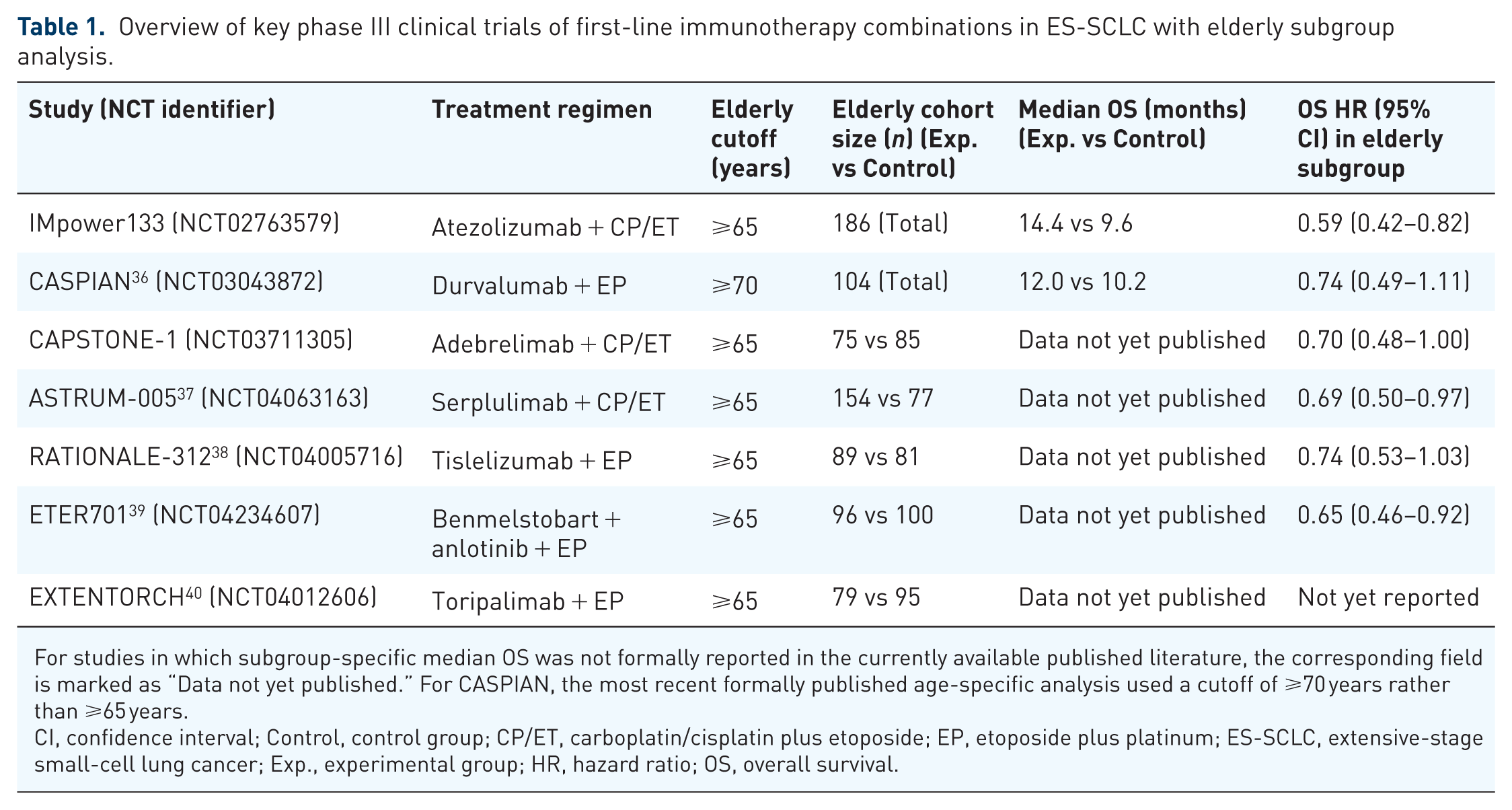
For studies in which subgroup-specific median OS was not formally reported in the currently available published literature, the corresponding field is marked as “Data not yet published.” For CASPIAN, the most recent formally published age-specific analysis used a cutoff of ⩾70 years rather than ⩾65 years.
CI, confidence interval; Control, control group; CP/ET, carboplatin/cisplatin plus etoposide; EP, etoposide plus platinum; ES-SCLC, extensive-stage small-cell lung cancer; Exp., experimental group; HR, hazard ratio; OS, overall survival.
PD-L1 inhibitors combined with chemotherapy: Validation of the first-line standard
The IMpower133 trial, the pioneering phase III study to demonstrate a survival benefit with chemoimmunotherapy, established atezolizumab plus etoposide-carboplatin as a standard of care. Long-term follow-up data revealed that in the subgroup aged ⩾65 years, the atezolizumab arm exhibited superior survival benefits (median OS 14.4 vs 9.6 months); notably, the magnitude of benefit (hazard ratio (HR) = 0.59) was numerically superior to that of the younger subgroup, with no unexpected geriatric-specific toxicity observed. This preliminarily supports the feasibility of this modality in the geriatric population.4,15
Subsequent analyses from CASPIAN further supported the benefit of durvalumab combined with etoposide plus cisplatin/carboplatin in older patients. In the most recent formally published age-specific analysis, which used a cutoff of ⩾70 years, mOS was 12.0 versus 10.2 months, with an OS HR of 0.74 (95% confidence interval (CI) 0.49–1.11), indicating that the survival benefit remained directionally consistent in selected older patients.41,42 Furthermore, the CAPSTONE-1 study, conducted in a Chinese cohort to evaluate adebrelimab, also suggested a survival benefit in older patients, although subgroup-specific mOS data have not yet been formally published. 43 Together, these findings support the broader clinical relevance of PD-L1 inhibitor-based chemoimmunotherapy in older adults with ES-SCLC, while also underscoring the need for more complete age-specific outcome reporting.
Expansion of PD-1 inhibitors and statistical interpretation of subgroup data
As the therapeutic landscape evolves, PD-1 inhibitors combined with chemotherapy offer additional therapeutic options for older adults with ES-SCLC, but interpretation of age-specific subgroup findings remains challenging. In ASTRUM-005, serplulimab plus chemotherapy established a strong OS signal in the overall population, and the ⩾65 subgroup showed prolonged progression-free survival (PFS), supporting meaningful disease control in older patients.38,44 However, subgroup-specific mOS data for older patients have not yet been formally reported. A similar issue applies to other recent phase III studies. In RATIONALE-312, although the overall population derived clear benefit, the HR for the ⩾65 subgroup (HR = 0.74, 95% CI: 0.53–1.03) crossed unity, which may reflect limited statistical power rather than true absence of benefit. 45 Likewise, the EXTENTORCH study confirmed overall efficacy, but more granular age-specific survival reporting remains limited. 40 Therefore, for several recent first-line phase III trials, available elderly subgroup HRs should be interpreted cautiously in the absence of formally published subgroup-specific mOS data.
Real-world evidence: Bridging the gap in poor PS
While RCTs have confirmed benefits in strictly selected elderly subgroups, a vast number of elderly patients with poor PS (ECOG PS ⩾2) in real-world settings are often excluded from the evidence base due to “enrollment bias,” resulting in a clinical evidence gap. 6 A retrospective real-world study from the Mayo Clinic has partially bridged this gap by including elderly patients with PS 2–3 who are typically ineligible for RCTs. The results indicated that following chemoimmunotherapy, the median OS of the PS 2–3 subgroup (9.3 months) showed no statistically significant difference from that of the PS 0–1 subgroup (10.6 months; p = 0.2718). 46 This finding challenges the conventional paradigm of making treatment decisions based solely on PS scores, suggesting that select elderly patients with compromised PS may still derive benefit from immunotherapy. Nevertheless, given the inherent selection bias and sample size limitations of retrospective studies, and the high burden of complex comorbidities in this population, future prospective, real-world studies targeting the “old and frail” cohort are imperative to precisely delineate the therapeutic index of immunotherapy.6,47
Exploration of novel immunotherapy combinations: From mechanistic synergy to strategic stratification
While chemoimmunotherapy has established the first-line standard, achieving a new equilibrium between therapeutic efficacy and toxicity tolerance remains a pressing clinical challenge for elderly patients with limited physiological reserve. 48 To address current therapeutic bottlenecks, research is focusing on novel combinations based on mechanistic complementarity, evolving along two primary strategic pathways: “intensification” aimed at synergistic efficacy, and “de-escalation” aimed at optimizing tolerability.49,50
Vascular normalization and remodeling of the immune microenvironment
Aberrant activation of the vascular endothelial growth factor (VEGF) pathway not only drives tumor angiogenesis but also fosters a highly suppressive immune microenvironment by inhibiting dendritic cell maturation and promoting the infiltration of Tregs.51,52 Consequently, blocking the VEGF pathway facilitates vascular normalization and enhances intratumoral immune cell infiltration, theoretically generating synergistic antitumor effects with ICIs. 39
The ETER701 study, utilizing a “four-drug combination” of benmelstobart, anlotinib, and EP chemotherapy, significantly extended mOS to 19.3 months (HR = 0.61), setting a new survival benchmark. However, caution is warranted regarding generalizability to the elderly: the median age of participants was only 62 years, and the incidence of Grade ⩾3 treatment-related adverse events (TRAEs) reached 93.1%. Given that elderly patients prevalently exhibit age-related vascular stiffness and impaired hemodynamic regulation, the risks of hypertension and hemorrhage induced by small-molecule tyrosine kinase inhibitors (TKIs) may be significantly exacerbated when superimposed with chemotherapy toxicity. 39 Therefore, when considering such “full-dose intensification” regimens in the geriatric population, cardiovascular reserve must be prioritized as a core screening metric rather than solely focusing on survival extension.53,54
Conversely, a “chemo-free” maintenance strategy may offer a superior therapeutic index for frail elderly patients. Retrospective data indicate that for patients achieving stable disease after first-line chemotherapy, adopting anlotinib combined with PD-1/PD-L1 inhibitors for maintenance can yield a median PFS of 6 months with a manageable safety profile. 55 This suggests that for elderly patients intolerant to the cumulative toxicity of long-term chemotherapy, a sequential maintenance strategy of immunotherapy plus anti-angiogenesis provides a viable, low-toxicity alternative pathway.56,57
Radio-immunotherapy synergy: From cytotoxic control to immunomodulation
With chemoimmunotherapy established as the first-line standard, the role of radiotherapy is undergoing a paradigm shift from purely local control to systemic immunomodulation. Its core mechanism lies in inducing immunogenic cell death to release tumor-associated antigens, thereby priming a systemic antitumor immune response (i.e., the abscopal effect).57,58 Consequently, the safety and efficacy of sequential thoracic consolidative radiotherapy (cTRT) in the immunotherapy era have emerged as a critical area of investigation.
Retrospective data indicate that ES-SCLC patients receiving sequential cTRT after induction chemoimmunotherapy can achieve a median PFS of 12.8 months; furthermore, under strict constraints on normal lung dosimetry (e.g., Lung V20), no prohibitive toxicities were observed, confirming feasibility. 59 However, elderly patients frequently present with comorbidities such as COPD and pulmonary fibrosis, and their diminished pulmonary reserve renders them extremely sensitive to radiation-induced injury. 60 Clinicians must exercise heightened vigilance regarding the overlapping toxicity of radiation pneumonitis and checkpoint inhibitor pneumonitis; once Grade ⩾2 pneumonitis occurs, the complexity of management and mortality risk increase significantly in the elderly.61,62 Therefore, the implementation of cTRT must adhere to principles of “adaptive dosing” and “precision targeting.”
Concurrently, low-dose radiotherapy (LDRT) is gaining attention as an emerging immunomodulatory strategy. Distinct from traditional high-dose cytotoxic radiation, LDRT aims to remodel the stromal microenvironment and promote the infiltration of effector T cells into the tumor parenchyma. 63 For elderly ES-SCLC patients with poor PS who cannot tolerate radical radiation doses, LDRT may provide a “toxicity-sparing” microenvironmental sensitizing approach, although its optimal dose-fractionation regimen warrants further validation through prospective studies.64–66
Novel therapeutic strategies for elderly relapsed and refractory ES-SCLC: The evolution toward chemotherapy-free and precision immunotherapy
For elderly patients progressing after first-line chemoimmunotherapy, traditional second-line regimens, exemplified by topotecan, present a significant clinical challenge characterized by limited efficacy (objective response rate (ORR) <20%) and severe cumulative myelotoxicity. This often leads to dose interruptions or discontinuation rather than therapeutic benefit.67,68 In recent years, driven by breakthroughs in transcriptional inhibition technology and bispecific antibody engineering, the therapeutic paradigm for relapsed/refractory ES-SCLC is undergoing a profound transformation from “broad-spectrum cytotoxicity” to “precision targeting and immune redirection.” Key emerging agents and their specific geriatric management considerations are summarized in Table 2.
Emerging therapeutic agents for relapsed/refractory ES-SCLC and specific management considerations for the geriatric population.
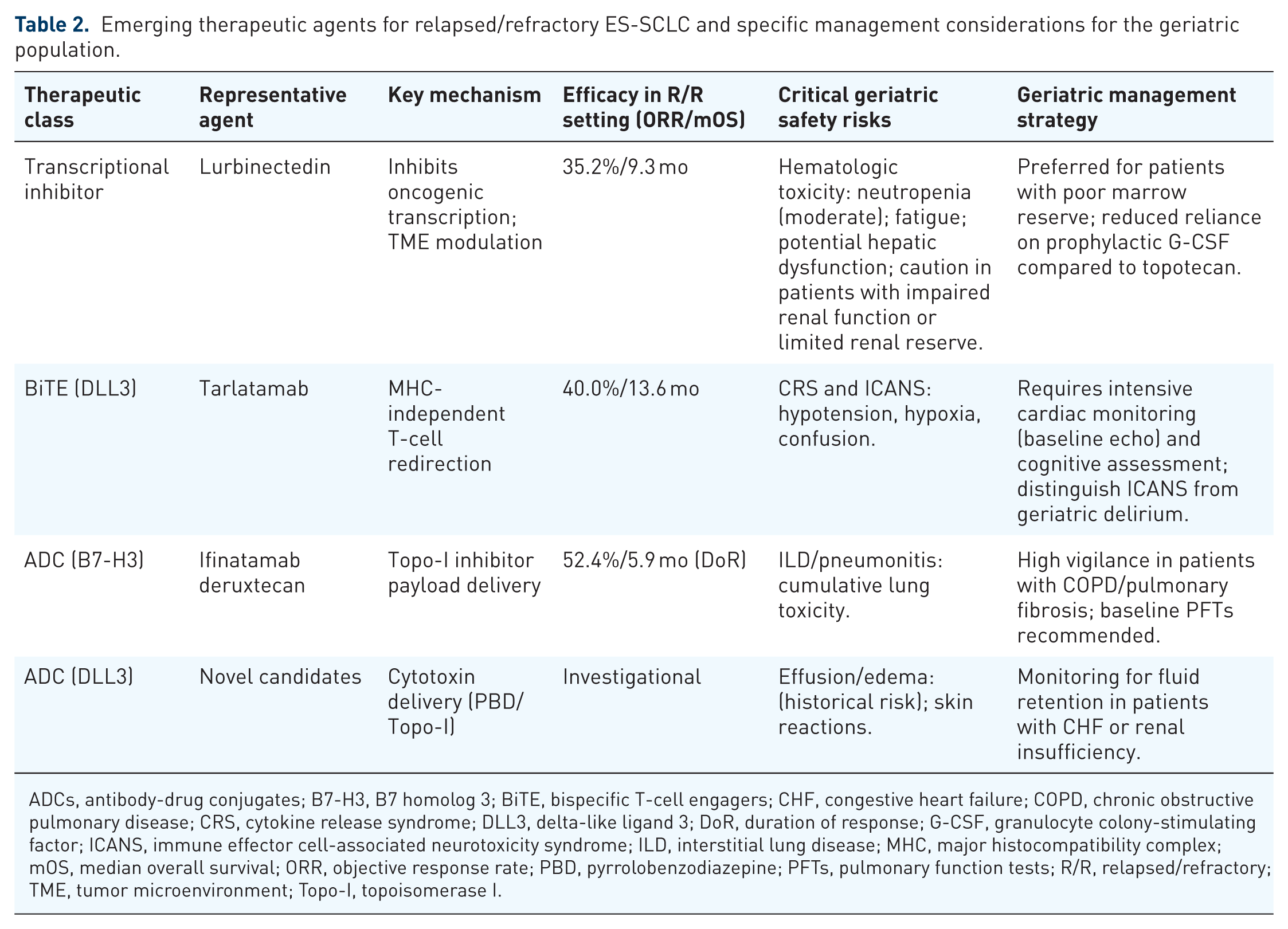
ADCs, antibody-drug conjugates; B7-H3, B7 homolog 3; BiTE, bispecific T-cell engagers; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CRS, cytokine release syndrome; DLL3, delta-like ligand 3; DoR, duration of response; G-CSF, granulocyte colony-stimulating factor; ICANS, immune effector cell-associated neurotoxicity syndrome; ILD, interstitial lung disease; MHC, major histocompatibility complex; mOS, median overall survival; ORR, objective response rate; PBD, pyrrolobenzodiazepine; PFTs, pulmonary function tests; R/R, relapsed/refractory; TME, tumor microenvironment; Topo-I, topoisomerase I.
Transcriptional regulators: The safety advantage of lurbinectedin
Lurbinectedin, a novel selective oncogenic transcription inhibitor, possesses a dual mechanism of action: it induces tumor cell apoptosis by inhibiting active transcription while simultaneously modulating the stimulator of interferon genes (STING)-interferon (IFN) pathway within the TME to reactivate antitumor immunity.69,70 This unique profile positions it as the first novel agent approved by the U.S. Food and Drug Administration for SCLC since the era of topotecan. Key basket trials have validated its second-line efficacy: at a dose of 3.2 mg/m2, it achieved an ORR of 35.2% and extended mOS to 9.3 months. 58 More critically, recent data from phase III clinical trials (e.g., the IMforte study) demonstrated that lurbinectedin combined with atezolizumab as maintenance therapy significantly outperformed single-agent controls in both median PFS and OS, with no unexpected safety signals observed. For elderly ES-SCLC patients, the core advantage of lurbinectedin lies in its favorable hematologic safety profile. 71
Real-world data indicate that even in the subgroup aged ⩾65 years, efficacy remains comparable to the overall population, while the incidence of Grade 3–4 febrile neutropenia is significantly lower than that of topotecan, substantially reducing reliance on prophylactic granulocyte colony-stimulating factor. 72 This “hematologic-sparing” profile renders it an optimal choice for elderly patients with marginal PS or intolerance to high-intensity chemotherapy. 73 Furthermore, studies such as LUPER are exploring its combination with ICIs; preliminary results suggest it holds promise for overcoming first-line immune resistance via remodeling of the TME, offering a new strategy of “chemo-immune resensitization” for later-line therapy. 74
Delta-like ligand 3-targeting BiTE: Therapeutic potential and geriatric management challenges
Delta-like ligand 3 (DLL3), an inhibitory ligand of the Notch signaling pathway, exhibits aberrant high expression on the surface of approximately 85% of SCLC cells while remaining minimally expressed in normal adult tissues.75,76 This exceptional tumor-specificity renders it a compelling target for precision immunotherapy. Tarlatamab, a first-in-class half-life extended BiTE, functions by bridging T cells and tumor cells to form a lytic synapse, thereby directly mediating the specific lysis of DLL3-positive tumor cells in a major histocompatibility complex (MHC)-independent manner. 77
The DeLLphi series of studies have redefined treatment standards for second-line and later-line settings. The phase II DeLLphi-301 study confirmed durable responses in heavily pretreated patients. 78 Subsequently, the confirmatory phase III DeLLphi-304 study demonstrated that, compared to standard second-line chemotherapy, tarlatamab significantly extended mOS to 13.6 months (vs 8.3 months), corresponding to a 40% reduction in the risk of death. Subgroup analyses revealed consistent survival benefits regardless of platinum sensitivity or prior immunotherapy exposure. 79 Such broad efficacy is clinically significant for elderly patients with relapsed disease who otherwise face a paucity of effective options.
However, the application of BiTE therapy in the elderly population entails unique safety challenges, necessitating vigilance against the interplay between cytokine release syndrome (CRS) and age-related physiological decline. Primarily, transient hypotension or hypoxemia induced by CRS can precipitate severe hemodynamic decompensation in elderly patients with comorbid coronary artery disease or heart failure. 80 Secondly, increased blood-brain barrier permeability and diminished baseline cognitive reserve in the elderly may lead to earlier and more severe manifestations of immune effector cell-associated neurotoxicity syndrome (ICANS); these symptoms can be easily confounded with geriatric delirium, leading to delayed diagnosis. 81 Therefore, while tarlatamab spares patients from severe myelosuppression, clinical practice mandates a risk-adapted monitoring strategy: this includes intensive cardiac monitoring during the initial dosing period, early differentiation of neurotoxicity from delirium, and a lower threshold for corticosteroid intervention, ensuring that survival benefits are balanced against the preservation of the elderly patient’s functional reserve.79,82
Antibody-drug conjugates: Precision payload delivery and investigational development
Antibody-drug conjugates (ADCs) combine a tumor-directed monoclonal antibody, a chemical linker, and a cytotoxic payload to enable antigen-directed drug delivery.83,84 This design provides a mechanistic rationale for increasing intratumoral payload exposure while reducing nonspecific systemic exposure compared with conventional chemotherapy; however, whether this strategy translates into a consistently wider therapeutic index in ES-SCLC, particularly in older adults, remains unproven.83,84 At present, the clinical evidence supporting ADCs in ES-SCLC is derived mainly from early-phase studies, and no ADC has yet been approved for ES-SCLC at the time of this revision.85,86 Among current ADC candidates, the B7 homolog 3 (B7-H3)-directed DXd ADC ifinatamab deruxtecan (I-DXd) has generated the most clinically advanced evidence in previously treated ES-SCLC, with encouraging antitumor activity reported in the phase II IDeate-Lung01 trial. 86 Nevertheless, ADCs should not be regarded as inherently toxicity-sparing. Hematologic adverse events and interstitial lung disease (ILD)/pneumonitis remain clinically relevant safety concerns, and these risks may be amplified in older patients with limited marrow reserve, impaired pulmonary function, or comorbid chronic lung disease.86,87 Therefore, in older adults with ES-SCLC, ADCs should be presented as emerging investigational treatment candidates whose efficacy, tolerability, and functional impact require further validation in prospective studies, rather than as established strategies that widen the therapeutic index.
B7 homolog 3
B7 homolog 3/(CD276), an immune checkpoint molecule, is aberrantly upregulated in SCLC and significantly correlates with tumor invasion, metastasis, and poor prognosis.88,89 Given its differential expression profile, B7-H3 has become a focal point for SCLC ADC development. I-DXd is a frontrunner in this domain, utilizing a topoisomerase I inhibitor payload conjugated via a cleavable linker. Data from the phase II IDeate-Lung01 study demonstrated encouraging antitumor activity (ORR 52.4%, median duration of response 5.9 months) in ES-SCLC patients refractory to multiple lines of therapy. 86 Notably, this agent also exhibited significant central nervous system activity, which holds profound clinical significance for elderly SCLC patients frequently burdened with brain metastases.
However, the risk of ADC-associated ILD/pneumonitis warrants heightened vigilance, particularly in the elderly population with comorbid chronic pulmonary diseases (e.g., COPD, pulmonary fibrosis). 87 Future research must further define the optimal dosage and toxicity management algorithms within elderly subgroups to prevent the compounding toxicity of drug-induced pneumonitis superimposed on underlying pulmonary pathology.
Delta-like ligand 3
DLL3, acting as an inhibitory ligand of the Notch signaling pathway, specifically aggregates on the surface of approximately 85% of SCLC cells, making it an ideal target for precision therapy. 90 Rovalpituzumab Tesirine (Rova-T), the first-in-class ADC targeting DLL3, initially showed promise but ultimately failed in pivotal phase III trials (TAHOE and MERU) due to severe toxicities (e.g., pleural effusions, photosensitivity) stemming from linker instability and a lack of survival benefit.91,92 Although the development of Rova-T was terminated, it validated DLL3 as a therapeutic target.
Next-generation DLL3-ADCs are achieving technical optimization by utilizing more stable linkers and novel high-potency payloads (such as pyrrolobenzodiazepine dimers or topoisomerase inhibitors). 93 Crucially, compared to bispecific antibodies that rely on the patient’s endogenous T-cell function, the mechanism of ADCs—directly delivering cytotoxins—is theoretically independent of host immune competence. 94 This characteristic makes ADCs potentially more suitable for elderly patients suffering from immunosenescence. Future development should focus on minimizing off-target toxicity to achieve efficient tumor killing that is uncoupled from the host’s declining immune system.
Chimeric antigen receptor T-cell therapy
While chimeric antigen receptor T-cell (CAR-T) therapy has transformed the landscape of hematologic malignancies, its translation to solid tumors like SCLC faces significant biological and clinical barriers.95,96 Despite the attractive target profile of DLL3 in SCLC, the application of CAR-T in elderly patients is impeded by unique physiological and technical challenges.
First, immunosenescence constitutes a fundamental bottleneck: the senescent phenotype and diminished diversity of peripheral T cells in elderly patients compromise the efficacy of leukapheresis, ex vivo expansion potential, and in vivo persistence post-infusion. 21 Second, the toxicity of lymphodepleting conditioning regimens presents a major hurdle. Standard CAR-T protocols require fludarabine/cyclophosphamide-based pretreatment to suppress host immune rejection; this poses prohibitive risks to elderly patients with diminished hematopoietic reserve, potentially precipitating prolonged pancytopenia and severe infections. 96
Finally, regarding safety signals, elderly patients often present with limited cardiopulmonary reserve, rendering them vulnerable to the hemodynamic instability associated with CRS and the neurological sequelae of ICANS. 97 Consequently, excluding the development of “off-the-shelf” allogeneic CAR-T products or toxicity-sparing strategies, this modality remains largely investigational rather than a viable standard of care for the geriatric SCLC population in the near term. 98
Holistic management and strategic optimization for elderly ES-SCLC patients
From single scores to multidimensional assessment: Establishing a CGA-based stratified decision system
At present, in the management pathway of elderly patients with ES-SCLC, the establishment of a decision-making framework centered on CGA constitutes the cornerstone for maximizing therapeutic efficacy while minimizing TRAEs. 99 Clinical practice should abandon the traditional model that relies solely on PS scoring. 100 In practical implementation, a standardized CGA should encompass at least the following core domains, and the use of internationally recognized assessment instruments is recommended to ensure homogeneity and comparability of evaluations: (1) Functional status: assessed using the Katz Index of Activities of Daily Living (ADL) and the Lawton–Brody IADL scale101–103; (2) Comorbidities: quantified using the Charlson Comorbidity Index (CCI) or the Cumulative Illness Rating Scale for Geriatrics (CIRS-G)101,102; (3) Cognitive function: screened using the Mini-Mental State Examination or the Montreal Cognitive Assessment (MoCA)104,105; (4) Nutritional status: identified using the Mini Nutritional Assessment–Short Form (MNA-SF)106–108; (5) Psychological status: evaluated using the 15-item Geriatric Depression Scale. 109 Polypharmacy and medication appropriateness should also be routinely reviewed as part of CGA, particularly in older patients with multimorbidity. In routine practice, CGA may be performed at baseline before treatment initiation and repeated at key treatment milestones to guide dynamic adjustment of therapeutic intensity and supportive interventions.
Based on the integrated findings of the CGA, patients should be precisely stratified into three categories—Fit, Vulnerable, and Frail (Figure 2, Table 3)—to determine the appropriate gradation of treatment intensity. 100 For Fit patients who are independent in ADL/IADL, have limited comorbidities, and demonstrate preserved cognitive function, physiological reserve is considered adequate, and standard-intensity immunotherapy combined with platinum-based doublet chemotherapy may be considered in pursuit of maximal therapeutic benefit. 110 For Vulnerable patients with potentially reversible impairments in one to two CGA domains, priority should be given to dose-adjusted chemotherapy regimens, sequential or maintenance immunotherapy strategies, accompanied by proactive prevention of treatment-related toxicities.111–113 In contrast, for Frail patients with severe multidimensional impairments (e.g., marked dependence in ADL and a high burden of comorbidities), the therapeutic objective should be shifted toward best supportive care or symptom-directed management, with emphasis on improving quality of life.100,113
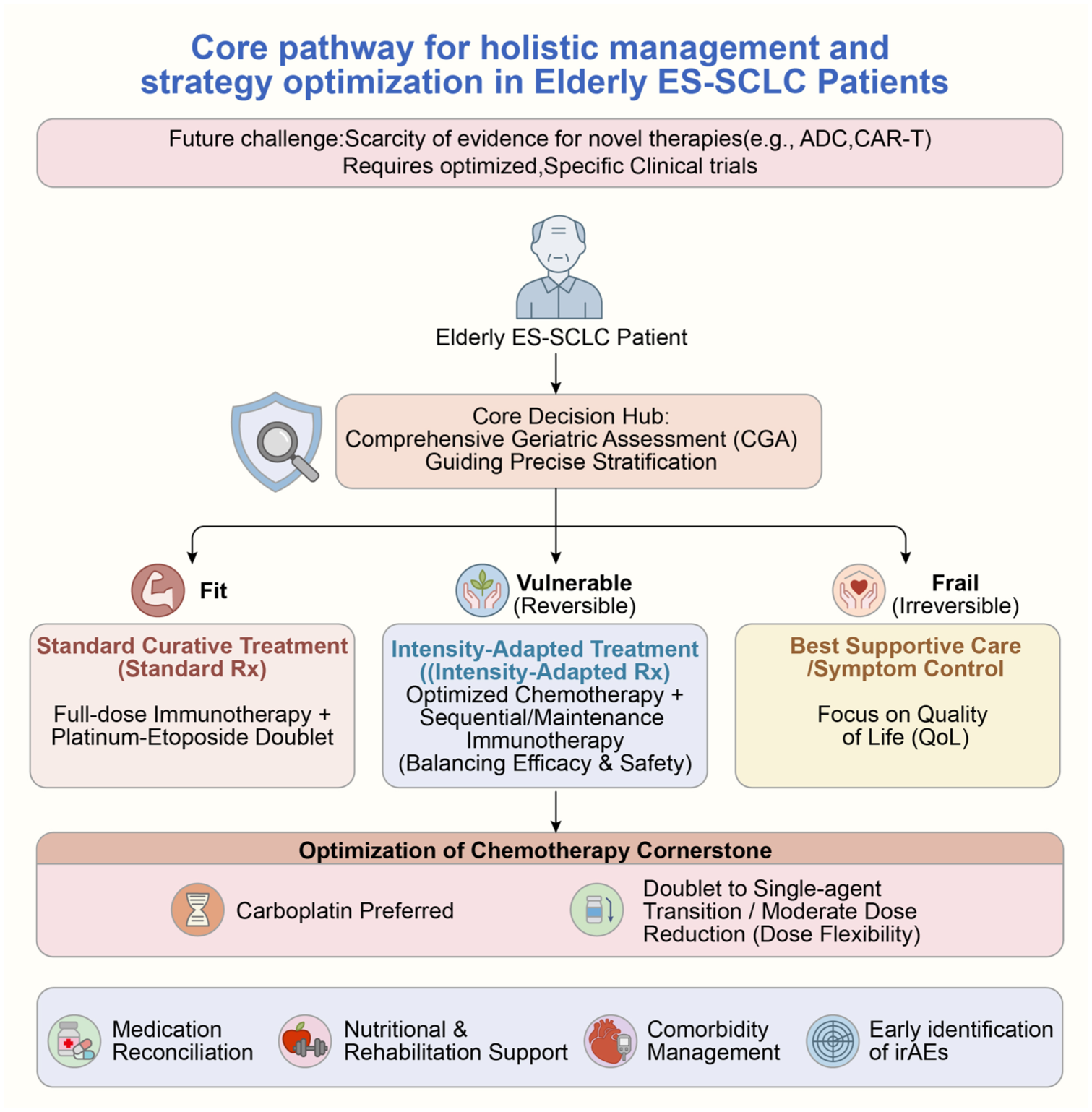
Proposed algorithm for CGA-guided holistic management and stratified treatment in elderly ES-SCLC. The flowchart illustrates the core decision-making pathway centered on CGA. Step 1: Patients undergo CGA to determine functional reserve. Step 2 (Stratification): Patients are categorized into “Fit,” “Vulnerable,” or “Frail” subgroups. Step 3 (Intervention):
Proposed framework for CGA-based stratified management in elderly ES-SCLC.
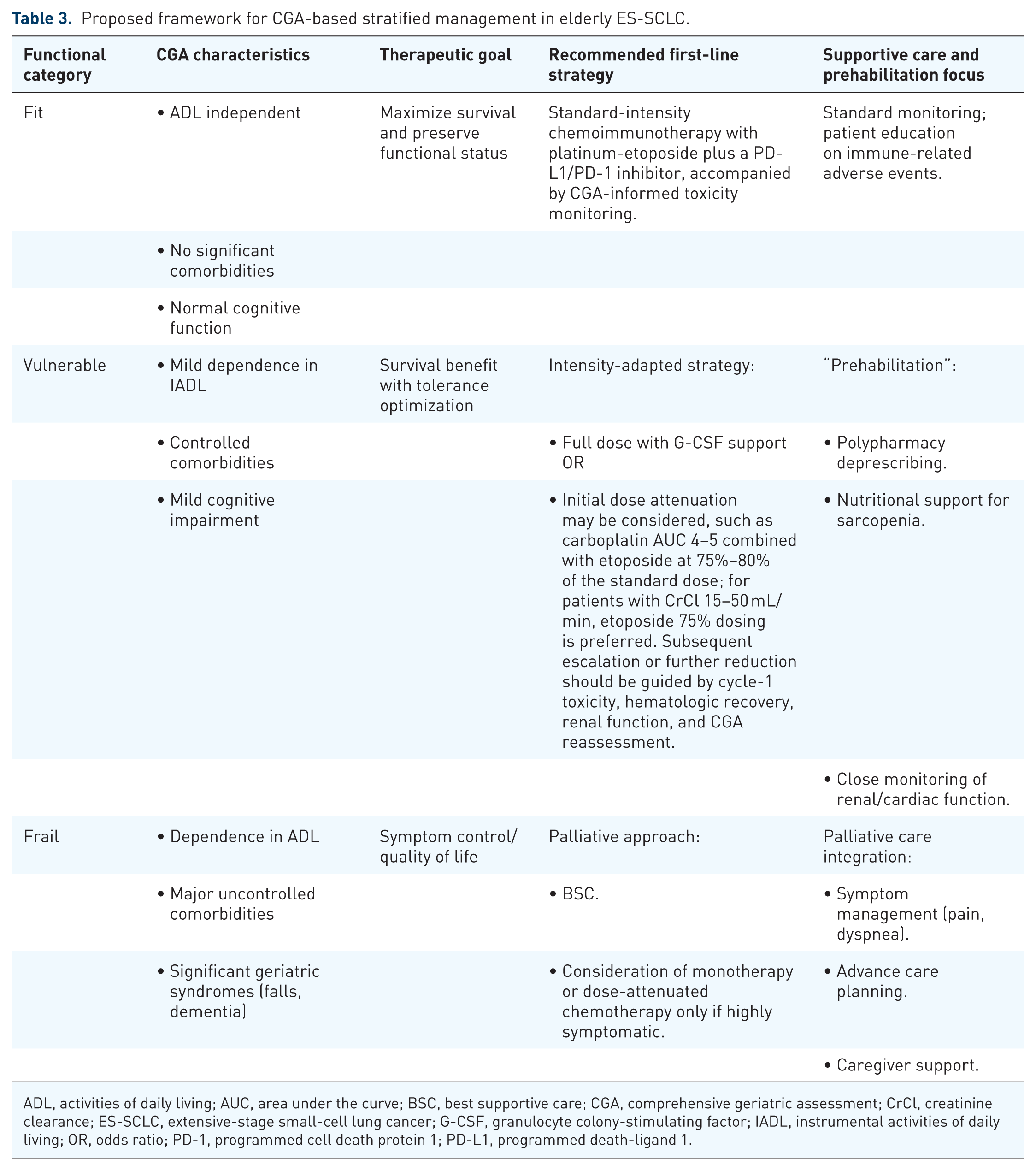
ADL, activities of daily living; AUC, area under the curve; BSC, best supportive care; CGA, comprehensive geriatric assessment; CrCl, creatinine clearance; ES-SCLC, extensive-stage small-cell lung cancer; G-CSF, granulocyte colony-stimulating factor; IADL, instrumental activities of daily living; OR, odds ratio; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1.
Concurrently, longitudinal management requires clinicians to implement precise interventions throughout the entire treatment continuum, including rigorous medication reconciliation and deprescribing in accordance with the Beers Criteria 114 ; enhancement of muscle reserve and physical performance through nutritional support and exercise-based rehabilitation for patients in whom deficits are identified by MNA-SF or ADL/IADL assessments 115 ; timely management of cardiovascular and metabolic comorbidities based on CCI or CIRS-G evaluation results; and early recognition and prompt management of irAEs, which may present more insidiously in elderly patients.116,117
Optimization of the chemotherapy backbone: Balancing platinum selection and dose intensity
Although chemoimmunotherapy has established its first-line status, cytotoxic chemotherapy remains an essential backbone of systemic treatment for ES-SCLC. Given the physiological characteristics of elderly patients, such as declined glomerular filtration rate and increased susceptibility to ototoxicity and neurotoxicity, the formulation of chemotherapy regimens must strike a balance between “dose intensity” and “organ protection.” 13 Existing evidence strongly supports carboplatin as the preferred platinum agent for elderly ES-SCLC. A meta-analysis comprising 663 SCLC patients indicated that carboplatin is non-inferior to cisplatin regarding OS benefits but exhibits a significantly superior safety profile 118 ; real-world evidence from the SEER database further corroborates that the carboplatin-etoposide regimen significantly reduces treatment-related renal and neurological toxicities without compromising OS.119,120 Consequently, the use of cisplatin should be restricted to a highly select minority of “Fit” elderly patients with intact organ function. 118 Furthermore, dosing flexibility is a critical clinical strategy. A retrospective study suggests that a “toxicity-guided” dose adjustment strategy—dynamically adjusting doses or extending cycle intervals based on patient tolerance—may compromise short-term ORRs but significantly lowers treatment-related mortality, ultimately improving OS by preserving treatment continuity. 121 This implies that in the geriatric population, maintaining the integrity of treatment cycles is more critical than adhering to peak dose intensity.
Bridging the evidence gap: Translation of novel therapies and pragmatic trials
Novel immunotherapeutic combinations, such as ADCs and bispecific antibodies, bring therapeutic potential to ES-SCLC, yet the “evidence gap” remains the primary bottleneck restricting their precise implementation in the elderly. 6 Due to the prevalence of physiological aging, multiple comorbidities, and declined organ reserve, the pharmacokinetic parameters and maximum tolerated dose established in younger populations often cannot be directly extrapolated to the elderly. 122 Therefore, filling this void is an urgent priority, and future research paradigms must undergo fundamental transformation. First, traditional RCTs should mandate the incorporation of CGA-based stratification factors and actively recruit “Vulnerable” and “Frail” subgroups to comprehensively assess safety boundaries under real physiological conditions. 122 Second, “Pragmatic Clinical Trials (PCTs)” and adaptive designs should be prioritized, relaxing comorbidity restrictions to better mirror real-world clinical scenarios. 123 Finally, a geriatric-specific pharmacovigilance system should be constructed utilizing real-world data, focusing on monitoring occult risks such as ADC-induced pulmonary toxicity and immunotherapy-related myocarditis.124,125 By constructing a closed-loop evidence system of “RCT confirmation + RWE supplementation,” the field can ultimately achieve the precise, safety-optimized, and individualized application of novel antitumor therapies in elderly ES-SCLC patients.
Discussion
Although chemoimmunotherapy has been endorsed by major guidelines as the first-line standard for ES-SCLC, its applicability to real-world older adults remains limited. Milestone trials such as IMpower133, CASPIAN, and ASTRUM-005 demonstrated survival benefits in elderly subgroups15,41,54; however, these subgroups largely consisted of relatively fit older patients with preserved organ function and limited comorbidity burden. As a result, the available trial evidence does not adequately capture the clinical complexity of older adults with multimorbidity, frailty, or poor baseline PS. This limitation is particularly relevant for patients aged ⩾75 years or those with baseline PS ⩾2, for whom randomized evidence remains sparse and real-world studies suggest a less favorable benefit-risk balance.126,127 Therefore, the key challenge is not simply the absence of data, but the limited external validity of current evidence for heterogeneous geriatric populations.
In the dimension of safety, the trend toward long-term administration of immunotherapy poses a substantial challenge to the homeostatic resilience of elderly patients. 128 The management of irAEs often necessitates high-dose and prolonged courses of glucocorticoids. For the elderly, this represents not merely an anti-inflammatory intervention but a potential “cumulative iatrogenic burden” that precipitates the exacerbation of sarcopenia, acceleration of osteoporosis, and susceptibility to secondary infections, thereby increasing the risk of non-tumorigenic mortality.129,130 Furthermore, the lack of validated predictive biomarkers remains a major barrier to precision immunotherapy in ES-SCLC. 131 Unlike non-SCLC, in which PD-L1 immunohistochemistry can inform the use of ICIs in several clinical settings, PD-L1 expression has not demonstrated sufficient predictive value in SCLC. 131 Tumor cell PD-L1 expression in SCLC is generally low, varies across assays and specimen types, and exhibits substantial spatial and temporal heterogeneity. More importantly, subgroup analyses from first-line chemoimmunotherapy trials, including IMpower133, suggest that survival benefit can be observed irrespective of PD-L1 status, indicating that PD-L1 should not be used as a stand-alone biomarker for selecting ES-SCLC patients for immunotherapy.15,132 Therefore, PD-L1 expression should not be used as a biomarker in otherwise eligible older adults with ES-SCLC; instead, treatment selection should rely on a composite assessment integrating tumor biology, clinical fitness, comorbidity burden, organ reserve, and CGA-derived vulnerabilities. In this context, tumor biology refers to clinically relevant disease and tumor features, including molecular subtype, disease burden, metastatic pattern, pace of progression, brain or liver involvement, platinum sensitivity or treatment-free interval, and target antigen expression when targeted agents are considered. Clinical fitness refers to the patient’s overall treatment tolerance, including ECOG PS, ADL/IADL independence, nutritional status, cognitive function, comorbidity burden, and renal, hepatic, cardiac, and pulmonary reserve. CGA-derived vulnerabilities refer to deficits identified through CGA, including frailty or sarcopenia, functional dependence, malnutrition, cognitive impairment, depression, polypharmacy, fall risk, and limited social support. Therefore, future biomarker development in elderly patients with ES-SCLC should move beyond single-marker approaches and integrate tumor-intrinsic features, immune microenvironmental signatures, inflammatory status, and CGA-derived host factors. Specifically, tumor-intrinsic features may include molecular subtype, genomic alterations, transcriptional programs, tumor burden, metastatic pattern, and therapeutic target expression. Immune microenvironmental signatures may include T-cell infiltration, antigen-presentation capacity, IFN-related signaling, and enrichment of immunosuppressive myeloid cells or regulatory T cells. Inflammatory status may be reflected by systemic markers such as the neutrophil-to-lymphocyte ratio, C-reactive protein level, lymphocyte count, and cytokine-related inflammatory activity. CGA-derived host factors include frailty, functional dependence, malnutrition, cognitive impairment, comorbidity burden, organ reserve, polypharmacy, and limited social support.
Regarding the optimization of combination strategies, while combining anti-angiogenic agents with chemoimmunotherapy possesses biological plausibility for microenvironmental normalization, the narrow therapeutic window in elderly patients cannot be overlooked. 39 Due to the decline in baseline vascular compliance associated with vascular aging, elderly patients are significantly more sensitive to hypertension, hemorrhage, and thrombotic events induced by TKIs. 55 Once superimposed with cardiac or renal insufficiency, toxicity risks may be markedly exacerbated. 133 Therefore, caution must be exercised regarding such “intensification” regimens, necessitating the establishment of dynamic cardiovascular risk monitoring mechanisms. Similarly, while thoracic radiotherapy can enhance local control, the “overlapping pneumonitis risk” (radiation-induced plus immune-mediated) constitutes a major barrier against a background of pre-existing pulmonary fibrosis.134,135 Future directions should focus on adaptive radiotherapy strategies, shifting target delineation from “broad coverage” to “precision sparing” to achieve an optimal balance between tumor control and pulmonary functional preservation. 136
Targeting therapeutic breakthroughs for relapsed and refractory patients, the application of novel agents must be grounded in a profound understanding of geriatric physiological characteristics. Lurbinectedin, with its non-cumulative myelotoxicity profile, offers a “hematologic-sparing” alternative superior to topotecan for elderly patients with diminished marrow reserve; however, the responsiveness of its immunomodulatory mechanism against a backdrop of immunosenescence remains to be validated. 137 More aggressive BiTE agents (e.g., tarlatamab), while capable of overcoming elderly antigen presentation defects via non-MHC-dependent mechanisms, face their greatest geriatric application barrier in the form of CRS and neurotoxicity (ICANS).82,138 Given the decline in cardiopulmonary reserve and alterations in blood-brain barrier permeability in the elderly, even low-grade CRS or mild neurotoxicity can trigger severe physiological decompensation (e.g., hemodynamic shock or delirium). 137 Consequently, ADCs require vigilance regarding the compounding of ILD on underlying pulmonary conditions, while CAR-T therapy still requires evaluation in carefully selected clinical settings; the current priority must be the establishment of a graded early warning and early intervention system tailored to geriatric physiology.139,140
Summary
The therapeutic landscape of elderly ES-SCLC is undergoing a paradigm shift, transitioning from empirical regimens to precision-guided holistic management. Although chemoimmunotherapy has established a new first-line standard and emerging agents—such as BiTEs, ADCs, and novel small molecules—have expanded the later-line therapeutic armamentarium, persistent selection bias regarding elderly subgroups in clinical trials has resulted in a significant evidentiary gap.
Given the multidimensional physiological decline and narrow therapeutic indices characteristic of this population, reliance on chronological age as the sole determinant for treatment selection is now obsolete. Future clinical practice must therefore integrate CGA as a foundational tool for decision-making, implementing stratified treatment and holistic toxicity management to achieve a precise equilibrium between tumor control and physiological tolerance. By prioritizing PCTs to bridge these data gaps, the field can advance toward true individualized precision medicine—one that not only extends survival but also maximally preserves the functional status and quality of life for this vulnerable population. Nevertheless, important limitations remain. For several emerging therapies, elderly-specific efficacy and safety data are still insufficient, and the proposed CGA-based stratification framework still requires further refinement through integration with clinically relevant biomarkers. Future research should prioritize prospective elderly-focused studies and biomarker-informed risk stratification to improve the precision and applicability of treatment decision-making in this population.
Footnotes
Acknowledgements
None.
Declarations
Artificial intelligence disclosure
No generative artificial intelligence tools were used to generate scientific content, analyze data, or produce references in this study. The authors take full responsibility for the accuracy, originality, and integrity of the manuscript.