
Abstract
Background:
Nectin-4 is a key therapeutic target of antibody–drug conjugates (ADCs) in advanced urothelial carcinoma (UC), but its expression patterns and underlying biology across anatomical sites remain poorly understood.
Objectives:
This study aimed to elucidate Nectin-4-related features in bladder (urinary bladder carcinoma, UBC) and upper urinary tract (upper tract urothelial carcinoma, UTUC) through a multi-layered approach, including primary tumor characterization, paired primary–metastatic analyses, and immune transcriptomic profiling.
Design:
A retrospective cohort study.
Methods:
We retrospectively analyzed primary tumors from 139 patients with advanced UC, including 56 with paired metastatic specimens and 75 with sufficient primary tumor tissue for immune profiling. Membranous Nectin-4 expression was assessed by immunohistochemistry and categorized as Nectin-4High (H-score 100–300) or Nectin-4Low (0–99). Immune profiling was performed using the nCounter® PanCancer Immune Profiling Panel (NanoString Technologies). External transcriptomic datasets (UBC: TCGA-BLCA; UTUC: GSE244957) were used to assess the consistency of immune profiling results.
Results:
Primary UBC tumors exhibited significantly higher Nectin-4 expression than UTUC tumors (median H-score 150.0 vs 95.0, p = 0.005; Nectin-4High 70.6% vs 50.0%, p = 0.018). Among paired specimens, 33.9% (19/56) showed primary–metastatic changes in Nectin-4 status, which occurred more frequently in UBC than in UTUC (52.2% vs 21.2%, p = 0.017). Immune profiling revealed a relatively immune-depleted pattern in Nectin-4High versus Nectin-4Low tumors in UBC, whereas this pattern was less evident in UTUC. These findings were consistent with those from external transcriptomic datasets.
Conclusion:
UBC and UTUC demonstrate distinct Nectin-4 expression patterns and associated immune contexture, highlighting the biological heterogeneity of Nectin-4 in advanced UC. Further prospective studies are warranted to validate these findings and clarify their clinical implications.
Plain language summary
Urothelial carcinoma is a type of cancer that can arise in different parts of the urinary system, most commonly in the bladder or the upper urinary tract (such as the kidney pelvis and ureter). Although these cancers are often grouped together, they may behave differently in terms of biology and response to treatment. In this study, we focused on a protein called Nectin-4, which is an important target for a newer class of cancer treatments called antibody–drug conjugates. We examined how Nectin-4 is expressed in tumor samples from patients with advanced urothelial carcinoma and compared differences between bladder and upper urinary tract cancers. We found that bladder cancers generally had higher levels of Nectin-4 than upper urinary tract cancers. We also observed that in some patients, Nectin-4 levels changed when comparing the original tumor to metastatic sites, and this change was more common in bladder cancer. In addition, we analyzed immune-related activity within the tumors. Tumors with high Nectin-4 levels tended to show a less active immune environment in bladder cancer, while this pattern was less clear in upper urinary tract cancer. These findings were consistent across independent external datasets. Overall, our results suggest that bladder and upper urinary tract urothelial cancers are biologically different in terms of Nectin-4 expression and immune features. These differences may be important for understanding how patients respond to Nectin-4–targeted treatments.
Keywords
Introduction
Urothelial carcinoma (UC) is a heterogeneous malignancy arising from distinct anatomical sites, most commonly the urinary bladder carcinoma (UBC) and the upper urinary tract (upper tract urothelial carcinoma, UTUC). Although they share histopathological features, evidence indicates that they differ in molecular characteristics, immune microenvironments, and clinical behavior.1–5 Such diversity raises important questions regarding whether emerging therapies can be uniformly applied across UC sites.
Nectin-4, a cell adhesion molecule involved in cancer growth, migration, and invasion, is frequently expressed in UC.6–9 It has become a clinically relevant therapeutic target with the development of Nectin-4-directed antibody–drug conjugates (ADCs), which have shown meaningful antitumor activity in advanced UC.10–14 Accordingly, characterization of Nectin-4-associated features has gained increasing relevance within the evolving UC treatment landscape.
Despite the growing use of Nectin-4-targeted ADCs, most studies have evaluated Nectin-4 expression in aggregated UC cohorts without systematically considering anatomical tumor sites. Prior evidence suggests that Nectin-4 expression may differ between UBC and UTUC 15 ; however, the biological significance remains unclear. In particular, how Nectin-4 expression in primary tumors relates to its changes during metastatic progression and to the surrounding immune milieu across UC sites has not been comprehensively elucidated, limiting the translational interpretation of site-specific effects on Nectin-4-directed ADCs.
In this study, we systematically analyzed membranous Nectin-4 expression in primary and metastatic specimens and characterized Nectin-4-associated features of the tumor immune microenvironment (TIME) in UBC and UTUC.
Patients and methods
Study design and patient cohorts
We retrospectively enrolled 139 patients with histologically confirmed advanced UC, including UBC and UTUC, treated at National Taiwan University Hospital (NTUH) or National Taiwan University Cancer Center between 2012 and 2024 (the overall cohort). Advanced UC was defined as metastatic disease or unresectable locally advanced disease not amenable to curative surgery. Patients with either de novo or recurrent metastatic disease were included. De novo metastatic disease was defined as metastatic disease present at initial diagnosis, whereas recurrent metastatic disease was defined as metastasis occurring after prior treatment for localized disease.
Eligible patients had (i) histologically confirmed and radiologically documented advanced UC; (ii) archival primary tumor specimens obtained prior to systemic treatment; and (iii) complete clinical and treatment data. Among them, 56 had matched metastatic tumor specimens for paired Nectin-4 analysis (the paired primary–metastatic cohort), and 75 had sufficient primary tumor tissue for immune profiling (the immune profiling cohort). The patient flow diagram is shown in Figure 1. Detailed procedures for tissue acquisition are provided in the Supplemental Data. The reporting of this study conforms to the STROBE statement for cohort studies (Table S1 in the Supplemental Data). 16

Patient flow diagram of the study cohorts.
Immunohistochemical analysis and assessment of Nectin-4 expression
Archival primary and metastatic tissues were cut into 5-μm-thick sections from formalin-fixed, paraffin-embedded (FFPE) blocks for immunohistochemical analysis. Nectin-4 staining was performed using a validated rabbit monoclonal antibody (clone EPR15613-68; Abcam, Cambridge, UK). 17 Slides were reviewed by a board-certified uropathologist (C.-C.W.), who was blinded to the clinical data.
Membranous Nectin-4 expression was quantified using the histochemical score (H-score; range, 0–300), which was calculated by multiplying staining intensity by the percentage of positive tumor cells. For categorical analyses, tumors were classified as Nectin-4High (H-score 100–300) or Nectin-4Low (H-score 0–99) using a prespecified cut-off applied consistently across primary and metastatic specimens. This threshold was selected in accordance with prior translational studies, in which higher membranous expression has been associated with the therapeutic activity of the Nectin-4-directed ADC enfortumab vedotin (EV).17,18
To minimize potential bias related to categorical classification, continuous H-scores were also analyzed in complementary analyses. Additional details of the staining protocol and scoring procedures are provided in the Supplemental Data.
Immune profiling
RNA was extracted from 10-μm FFPE tumor sections and hybridized in accordance with the manufacturer’s instructions. Gene expression profiling of the tumor immune contexture was performed using the nCounter® PanCancer Immune Profiling Panel (NanoString Technologies, Inc., Seattle, WA, USA). Raw data were processed with nSolver™ Analysis Software (version 4.0; NanoString Technologies, Inc., Seattle, WA, USA), and normalization was performed using the most stable housekeeping genes. Immune cell populations were estimated using the method described by Danaher et al. 19 The detailed RNA extraction procedures are provided in the Supplemental Data.
External transcriptomic datasets for immune profiling
External transcriptomic datasets were used to assess the consistency of findings from the immune profiling cohort. Processed gene expression data for UBC were obtained from the TCGA-BLCA dataset via the UCSC Xena platform, 20 and data for UTUC were obtained from the Gene Expression Omnibus (accession number GSE244957). 2 Nectin-4 mRNA expression was categorized into tertiles, with the highest and lowest tertiles defined as Nectin-4 mRNAHigh and Nectin-4 mRNALow groups, respectively. In total, 286 UBC and 56 UTUC tumors were included in these analyses. Immune cell populations were estimated as previously described. 19
Statistical analyses
Descriptive statistics were used to summarize the clinical characteristics and distributions of biomarkers. Fisher’s exact test was used for comparison of categorical variables, and the Mann–Whitney U test for continuous variables. Linear regression analyses were performed to identify factors associated with Nectin-4 expression in primary tumors. Variables included in the multivariable model were selected based on clinical relevance (including variables with baseline imbalance) and statistical significance in univariable analyses (p < 0.05).
Paired differences in Nectin-4 H-scores were evaluated using the Wilcoxon signed-rank test. Changes in categorical Nectin-4 status (Nectin-4High vs Nectin-4Low) were assessed using McNemar’s test, and transitions were visualized using Sankey plots. For immune profiling and external transcriptomic analyses, p values were adjusted for multiple comparisons using the Benjamini–Hochberg false discovery rate method. All statistical tests were two-sided, and p values <0.05 were considered statistically significant. Statistical analyses were performed using GraphPad Prism version 10.4.1.
Results
Differential Nectin-4 expression in primary UBC and UTUC tumors
The baseline characteristics of the overall cohort (N = 139), as well as the UBC (n = 51) and UTUC (n = 88) subgroups, are summarized in Table 1. Clinical characteristics were generally similar between the two subgroups, with the exception of a higher proportion of de novo metastases in the UBC subgroup.
Baseline characteristics of the overall cohort.
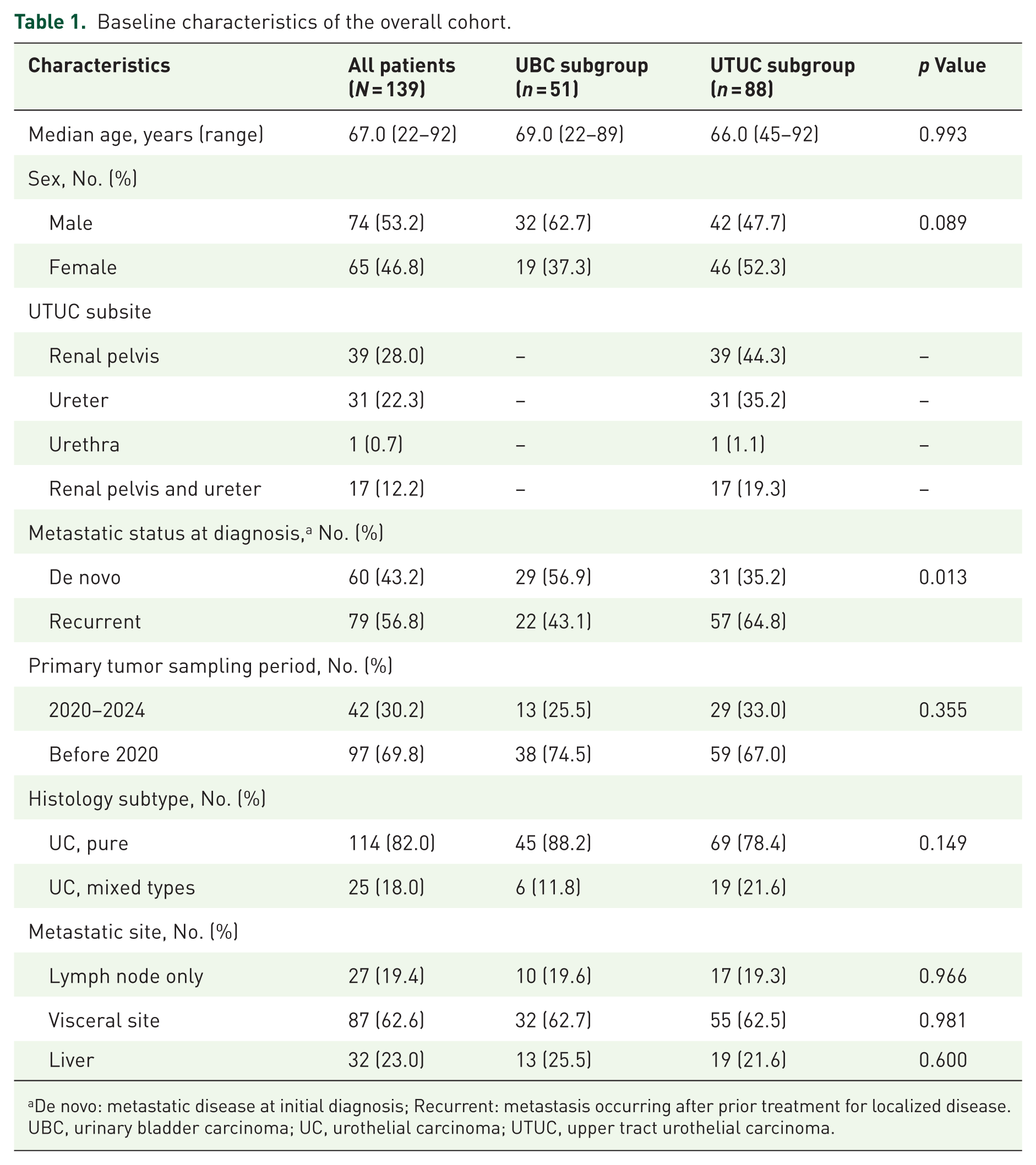
De novo: metastatic disease at initial diagnosis; Recurrent: metastasis occurring after prior treatment for localized disease.
UBC, urinary bladder carcinoma; UC, urothelial carcinoma; UTUC, upper tract urothelial carcinoma.
The median Nectin-4 H-scores were significantly higher in primary tumors of UBC than in UTUC (150.0 (interquartile range (IQR): 76.3–215.0) vs 95.0 (IQR: 10.0–155.0), p = 0.005; Figure 2(a)). In multivariable linear regression analysis adjusting for metastatic status at diagnosis, primary tumor sampling period, histology subtype, and lymph node-only metastasis, UBC remained independently associated with higher Nectin-4 H-scores (β: 39.3, 95% confidence interval (CI): 8.72–69.8, p = 0.012; Table S2 in the Supplemental Data). Similarly, the proportion of tumors classified as Nectin-4High was greater in UBC than in UTUC in unadjusted analyses (70.6% vs 50.0%; p = 0.018; Figure 2(b)).

Nectin-4 expression in primary UBC and UTUC tumors from the overall cohort. (a) H-scores assessed by IHC; median values were compared using the Mann–Whitney U test. (b) Categorical distribution (Nectin-4High vs Nectin-4Low); differences were assessed using Fisher’s exact test.
Paired comparison of Nectin-4 expression between primary and metastatic tumors
The baseline characteristics of the paired primary–metastatic cohort are shown in Table 2. Clinical characteristics were largely comparable between the UBC and UTUC subgroups, including variant histology distribution, metastatic sites, metastatic tumor sampling period, as well as the median interval between primary and metastatic tumor sampling, and systemic treatments received during this period, except for a higher proportion of de novo metastasis in the UBC subgroup. Exploratory analyses of metastatic lesions demonstrated variable Nectin-4 expression across metastatic sites, without statistically significant differences according to metastatic site or de novo versus recurrent metastatic status (Figure S1 in the Supplemental Data).
Baseline characteristics of the paired primary–metastatic cohort.

CI, confidence interval; ICIs, immune checkpoint inhibitors; PBC, platinum-based chemotherapy; UBC, urinary bladder carcinoma; UTUC, upper tract urothelial carcinoma.
Among the 56 patients with matched primary and metastatic tumors, the Nectin-4 H-score was numerically lower in metastatic lesions than in primary tumors (median 50.0 (IQR: 5.0–130.0) vs 100.0 (IQR: 10.0–160.0)) without reaching statistical significance (paired Wilcoxon signed-rank test, p = 0.058; Figure 3(a)). In subgroup analyses, a significantly lower H-score in metastatic lesions was observed in UBC (median 55.0 (IQR: 10.0–155.0) vs 140.0 (IQR: 85.0–231.8), n = 23, p = 0.032, paired test; Figure 3(b)). In contrast, H-scores were comparable between metastatic and primary tumors in UTUC (median 30.0 (IQR: 0–112.5) vs 40.0 (IQR: 5.0–121.3), n = 33, p = 0.540, paired test; Figure 3(c)).

Nectin-4 expression in the paired primary–metastatic cohort. (a) All patients. (b) UBC subgroup. (c) UTUC subgroup. Paired comparisons were performed using the Wilcoxon signed-rank test.
We next analyzed changes in Nectin-4 status (Nectin-4High vs Nectin-4Low) in patients with paired primary and metastatic specimens. Overall, 33.9% (19/56) of patients experienced a shift in Nectin-4 status from primary to metastatic tumors, with shifts more frequently in UBC than in UTUC (52.2% vs 21.2%; p = 0.017; Table 3). In UBC, among patients with primary Nectin-4High tumors, 64.7% shifted to metastatic Nectin-4Low, whereas among those with primary Nectin-4Low tumors,16.7% shifted to metastatic Nectin-4High; this directional change was significant by McNemar’s test (p = 0.006; Figure 4(a)). In contrast, no significant directional change was observed in UTUC (p = 0.453; Figure 4(b)).
Distribution of Nectin-4 status in the paired primary–metastatic cohort.

Percentages are calculated within each primary tumor Nectin-4 category (PRIHigh or PRILow).
Patients with changes were defined as a status shift from PRIHigh to METLow or from PRILow to METHigh.
Patients without changes were defined as concordant status between primary and metastatic tumors.
METHigh, high Nectin-4 expression in metastatic tumors; METLow, low Nectin-4 expression in metastatic tumors; PRIHigh, high Nectin-4 expression in primary tumors; PRILow, low Nectin-4 expression in primary tumors; UBC, urinary bladder carcinoma; UTUC, upper tract urothelial carcinoma.

Categorical distribution of Nectin-4 expression in the paired primary–metastatic cohort. (a) UBC subgroup. (b) UTUC subgroup. Directional shifts were assessed using McNemar’s test.
Association of Nectin-4 expression with the immune contexture
We examined the association between Nectin-4 expression and the TIME in 75 primary tumors from the immune profiling cohort (UBC, n = 27; UTUC, n = 48). The clinicopathologic characteristics of this cohort are summarized in Table 4. Baseline features were generally comparable between UBC and UTUC, with a higher proportion of de novo metastases in UBC.
Baseline characteristics of the immune profiling cohort.

UBC, urinary bladder carcinoma; UTUC, upper tract urothelial carcinoma.
After false discovery rate adjustment, UBC Nectin-4High tumors (n = 20) tended to show lower immune-related signatures across most evaluated immune cell populations compared with Nectin-4Low tumors (n = 7; Figure 5(a)), consistent with a relatively immune-depleted pattern. In contrast, UTUC showed an opposite directional trend, in which most immune-related signatures tended to be higher in Nectin-4High tumors (n = 17) than in Nectin-4Low tumors (n = 31; Figure 5(b)).

Association of Nectin-4 expression with the tumor immune microenvironment in the immune profiling cohort. Immune cell enrichment in Nectin-4High versus Nectin-4Low primary tumors in (a) UBC subgroup (n = 27) and (b) UTUC subgroup (n = 48). Each dot represents an immune cell population. The horizontal dashed line indicates the significance threshold corresponding to adjusted p = 0.05. Blue dots indicate significantly lower signatures in Nectin-4High tumors, whereas gray dots indicate non-significant differences.
These findings were further evaluated in external transcriptomic datasets to assess consistency with the immune profiling cohort. In UBC, Nectin-4 mRNAHigh tumors were associated with significantly reduced immune-related signatures across most immune cell populations, suggesting an immune-depleted phenotype (TCGA-BLCA, n = 286; Figure 6(a)). In contrast, no significant associations between Nectin-4 mRNA expression status and immune-related signatures were observed in UTUC (GSE244957, n = 56; Figure 6(b)).

Association of Nectin-4 expression with the tumor immune microenvironment in external transcriptomic datasets. Immune cell enrichment in Nectin-4 mRNAHigh versus Nectin-4 mRNALow tumors in (a) UBC dataset (TCGA-BLCA, n = 286) and (b) UTUC dataset (GSE244957, n = 56). Blue and red dots indicate significantly lower and higher immune signatures in Nectin-4 mRNAHigh tumors, respectively, whereas gray dots indicate non-significant differences.
Discussion
In this study, we evaluated Nectin-4 expression in primary and metastatic tumors of UBC and UTUC and its association with the TIME. Nectin-4 expression in primary tumors was significantly higher in UBC than in UTUC. Among patients with matched specimens, Nectin-4 status changed from primary to metastatic tumors in 33.9% of patients, with alterations occurring more frequently in UBC. High Nectin-4 expression in UBC was associated with a relatively immune-depleted pattern, which was not evident in UTUC.
A previous systematic review by Crupi et al. 15 suggested that Nectin-4 positivity is more frequent in UBC than in UTUC. However, cross-study comparisons were limited by heterogeneity in primary antibodies, staining protocols, interpretation criteria (membranous only vs membranous plus cytoplasmic), H-score cut-offs, and inconsistent reporting of specimen origin. Our study addressed these limitations by using a standardized immunohistochemical protocol with a single validated antibody, restricting scoring to membranous expression, and applying a prespecified cut-off. Using this approach, we confirmed higher Nectin-4 expression in primary UBC than in UTUC after adjustment for relevant clinical factors.
From a therapeutic perspective, these baseline differences in target expression may be relevant to therapeutic considerations. Nectin-4 expression has been reported to be associated with sensitivity to Nectin-4-targeted ADCs,17,21–23 suggesting that intrinsic variability in target expression may contribute to differences in treatment response across disease settings. Tumors with low Nectin-4 expression may therefore warrant consideration of alternative strategies to enhance target expression or overcome target-related resistance, several of which are currently under investigation.24,25
Beyond baseline expression, dynamic changes in Nectin-4 during metastasis represent another important consideration for biomarker-guided therapy. Klümper et al. 17 previously reported a significant decrease in membranous Nectin-4 expression during metastatic progression in UBC (median H-score: metastatic 40 vs primary 110; p < 0.001). Consistent with these findings, our paired analysis demonstrated a significant reduction in Nectin-4 H-scores in UBC metastases, whereas UTUC metastases showed no significant change. Moreover, McNemar’s test revealed a significant directional transition from Nectin-4High primary tumors to Nectin-4Low metastatic tumors in UBC, while no significant directional change was observed in UTUC, supporting site-specific differences in Nectin-4 dynamics during metastatic progression. Notably, compared with primary tumor expression, Nectin-4 expression in metastatic tumors has been reported to better correlate with EV response. 18 These findings suggest the potential role of metastatic biopsies prior to initiating Nectin-4-targeted ADC therapy, particularly in UBC, where substantial loss of membranous Nectin-4 may affect therapeutic efficacy.
In addition to distinct expression characteristics, Nectin-4 may play a role in modulating the TIME. Nectin-4 has been identified as a ligand for TIGIT, 26 an inhibitory receptor upregulated on tumor-infiltrating lymphocytes that contributes to an immunosuppressive microenvironment by impairing T-cell and natural killer cell function.27,28 Chu et al. 21 further reported that NECTIN-4 expression is enriched in luminal bladder cancer subtypes, which are characterized by an immune-cold phenotype driven by PPARG activation.29,30 These biological features may partially explain the relatively immune-depleted pattern observed in Nectin-4High UBC tumors. In contrast, this pattern was not observed in Nectin-4High UTUC tumors, suggesting distinct Nectin-4-associated immune biology between the two primary tumor sites. External transcriptomic datasets further supported these observations, demonstrating consistent Nectin-4-associated immune signature patterns across independent cohorts. Such site-specific differences may be relevant to the development of combination strategies incorporating immune checkpoint blockade.
This study has several limitations. The retrospective design and the two-center cohort may limit the generalizability of our findings. The sample size for matched primary–metastatic tumor analyses and immune profiling was modest, potentially limiting statistical power for certain subgroup comparisons. In addition, interpretation based on a prespecified H-score cut-off may be influenced by the dichotomization of a continuous variable. To address this concern, complementary analyses using continuous H-scores were performed, which yielded consistent patterns and supported the robustness of our findings. From an analytical perspective, external transcriptomic analyses were based on mRNA expression data with cohort-specific stratification and, therefore, are not directly comparable to the immunohistochemistry-based H-score system used in the study cohort, which may limit cross-platform interpretation. Finally, this study did not include treatment-response data related to Nectin-4-targeted ADCs; therefore, potential associations with therapeutic response and biomarker-guided clinical implications remain hypothesis-generating. Larger prospective studies are warranted for validation.
Conclusion
In summary, our findings demonstrate distinct patterns of Nectin-4 expression, its metastatic dynamics, and the associated immune contexture between UBC and UTUC, providing biological insights into Nectin-4 heterogeneity across different anatomic sites. Further prospective studies are warranted to validate these observations and clarify their clinical implications.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261463147 – Supplemental material for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs
Supplemental material, sj-docx-1-tam-10.1177_17588359261463147 for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs by Fu-Jen Hsueh, Chung-Chieh Wang, Chia-Lang Hsu, Shu-Cheng Wu, Jhe-Cyuan Guo, Chien-Huai Chuang, Shih-Chieh Chueh and Yu-Chieh Tsai in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261463147 – Supplemental material for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs
Supplemental material, sj-docx-2-tam-10.1177_17588359261463147 for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs by Fu-Jen Hsueh, Chung-Chieh Wang, Chia-Lang Hsu, Shu-Cheng Wu, Jhe-Cyuan Guo, Chien-Huai Chuang, Shih-Chieh Chueh and Yu-Chieh Tsai in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359261463147 – Supplemental material for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs
Supplemental material, sj-docx-3-tam-10.1177_17588359261463147 for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs by Fu-Jen Hsueh, Chung-Chieh Wang, Chia-Lang Hsu, Shu-Cheng Wu, Jhe-Cyuan Guo, Chien-Huai Chuang, Shih-Chieh Chueh and Yu-Chieh Tsai in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-4-tam-10.1177_17588359261463147 – Supplemental material for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs
Supplemental material, sj-docx-4-tam-10.1177_17588359261463147 for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs by Fu-Jen Hsueh, Chung-Chieh Wang, Chia-Lang Hsu, Shu-Cheng Wu, Jhe-Cyuan Guo, Chien-Huai Chuang, Shih-Chieh Chueh and Yu-Chieh Tsai in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261463147 – Supplemental material for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs
Supplemental material, sj-pdf-1-tam-10.1177_17588359261463147 for Site-specific differences in Nectin-4 expression and associated immune contexture in advanced urothelial carcinoma: implications for Nectin-4-targeted ADCs by Fu-Jen Hsueh, Chung-Chieh Wang, Chia-Lang Hsu, Shu-Cheng Wu, Jhe-Cyuan Guo, Chien-Huai Chuang, Shih-Chieh Chueh and Yu-Chieh Tsai in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.