
Abstract
Primary prostatic seminoma (PPS) is an exceptionally rare extragonadal germ cell tumor, with only isolated cases reported in the literature. Owing to its anatomical location, PPS may clinically and radiologically mimic prostate adenocarcinoma or other bulky pelvic malignancies, creating a risk of inappropriate local treatment. We report the case of a 34-year-old man presenting with a large prostatic mass and discordance between substantial tumor burden and only mildly elevated serum prostate-specific antigen (PSA; 3.43 µg/L). Serum lactate dehydrogenase (LDH) was markedly elevated (11.50 µkat/L), beta-human chorionic gonadotropin (beta-hCG) was mildly increased (5.3 IU/L), and alpha-fetoprotein remained within the normal range. Multiparametric magnetic resonance imaging and [18F]FDG positron emission tomography/computed tomography demonstrated a bulky, metabolically active prostatic tumor, but histopathological verification was essential for diagnosis. Immunohistochemistry showed strong positivity for SALL4 and c-KIT/CD117 with focal placental alkaline phosphatase expression, and negativity for prostatic, lymphoid, and non-seminomatous germ cell tumor markers, confirming seminoma. The patient was classified as good-risk according to the International Germ Cell Cancer Collaborative Group classification and achieved sustained complete remission following cisplatin-based chemotherapy. A structured literature review following PRISMA reporting principles identified 12 modern cases reported between 1990 and 2026. A recurrent observation was biochemical discordance between extensive tumor burden and low or only mildly elevated serum PSA levels. Germ cell markers, including LDH and beta-hCG, were variably elevated but lacked sufficient sensitivity and specificity to establish or exclude the diagnosis. Most patients were treated with cisplatin-based chemotherapy and/or radiotherapy, with a high rate of complete remission. PPS is a rare but highly curable malignancy. In young patients with atypical bulky prostatic masses and PSA levels disproportionate to tumor burden, early biopsy with germ cell-specific immunohistochemistry is essential. Functional imaging may support staging and response assessment, but systemic cisplatin-based chemotherapy remains the cornerstone of curative treatment.
Plain language summary
Primary prostatic seminoma is an extremely rare type of cancer that starts in the prostate but behaves like a germ cell tumor, a group of cancers more commonly found in the testicle. Because it grows in the prostate, it can be mistaken for the usual type of prostate cancer. This distinction is important because the treatment is different. We describe the case of a 34-year-old man with a large tumor in the prostate. His prostate-specific antigen (PSA), a blood test often used in prostate cancer, was only mildly increased despite the large tumor size. Imaging scans showed the extent of the tumor, but the final diagnosis required a biopsy and special laboratory tests on the tumor tissue. These tests confirmed that the tumor was a seminoma. The patient was treated with cisplatin-based chemotherapy and achieved complete remission. We also reviewed previously published cases of this very rare disease from the modern treatment era. Most patients responded well to chemotherapy and/or radiotherapy. This case shows that young patients with a large prostate tumor and unexpectedly low PSA should be carefully evaluated for rare diagnoses. Early biopsy and correct tumor testing are essential, because recognizing this rare but highly treatable cancer can help patients avoid unnecessary extensive surgery and receive the most appropriate treatment.
Keywords
Introduction
Primary extragonadal germ cell tumors (EGCTs) are uncommon malignancies that account for only about 5% of all germ cell tumors. According to epidemiological data published by Stang et al., 1 the total incidence varies from 1.8 to 3.4 per 1 million persons. Seminomas account for 30%–40% of these tumors, while non-seminomatous germ cell tumors (NS-GCTs) comprise the remaining 60%–70%. EGCTs typically arise along the midline of the body, such as the mediastinum (50%–70%), retroperitoneum (30%–40%), the pineal gland (5%), and the sacrococcygeal area (less than 5%). 2
Primary prostatic involvement is exceedingly rare among EGCTs. The first case was described by Miyake in 1935, and only isolated cases have been reported thereafter.3,4 To focus on contemporary diagnostic and therapeutic standards, our structured review was restricted to the modern era and identified 12 clinically documented cases, including the present case, reported between 1990 and 2026. Because of its anatomic location and clinical presentation, primary prostatic seminoma (PPS) frequently mimics high-grade prostate adenocarcinoma or benign prostatic hyperplasia, often leading to diagnostic delays or inappropriate primary surgical interventions.
The histogenesis of PPS remains a subject of ongoing discussion. The most widely accepted theory suggests that these tumors arise from the neoplastic transformation of primordial germ cells that were displaced during their midline migration from the yolk sac to the urogenital ridge. These cells are hypothesized to remain dormant within the prostatic utricle, a midline remnant of the Müllerian duct, until malignant transformation occurs. 5 Unlike the more common prostate adenocarcinoma, PPS typically affects younger patients and demonstrates exquisite sensitivity to platinum-based chemotherapy, highlighting the importance of early and accurate histological differentiation.
A major clinical challenge in identifying PPS is the frequent discordance between extensive tumor volume and relatively low or normal serum prostate-specific antigen (PSA) levels. This biochemical discordance may represent a useful clinical clue for non-epithelial prostatic malignancies. In such scenarios, the integration of germ cell-specific markers, including LDH, beta-human chorionic gonadotropin (beta-hCG), and alpha-fetoprotein (AFP) is important for both suggesting a germ cell origin and differentiating between seminomatous and non-seminomatous components. Along with these biochemical markers, functional imaging modalities such as multiparametric MRI (mpMRI) and [18F]FDG positron emission tomography/computed tomography (PET/CT) provide valuable information for staging, assessment of tumor extent, and modern response evaluation, although histopathological confirmation remains the gold standard for diagnosis. 6
In this report, we present a case of a 34-year-old male with a bulky PPS successfully managed with bleomycin, etoposide, cisplatin (BEP) chemotherapy. Furthermore, we provide a comprehensive structured literature review of the modern cohort of cases (1990–2026) to define key diagnostic features and optimize therapeutic strategies for this rare clinical entity.
Case presentation
A 34-year-old man with no significant medical history was referred to our department due to progressive clinical deterioration. His symptoms originated in February 2024 as a suspected urinary tract infection. Despite initial conservative management, his condition worsened by July 2024, manifesting as progressive lower urinary tract symptoms (LUTS), persistent pelvic pain, and eventually acute urinary retention. This necessitated the placement of a suprapubic epicystostomy in October 2024. Physical examination via digital rectal examination revealed a markedly enlarged, fixed, and “stony-hard” mass occupying the prostatic region.
Initial laboratory investigations confirmed a significant biochemical discordance: the serum PSA was only mildly elevated (3.43 µg/L, normal range <2.5 µg/L) despite the massive tumor burden. However, systemic germ cell markers showed a markedly elevated LDH of 11.50 µkat/L (normal range 2.25–3.75 µkat/L) and a marginally increased beta-hCG of 5.3 IU/L (normal range <2.6 IU/L), while AFP remained within normal limits (6.0 µg/L, normal range <7.0 µg/L).
mpMRI performed in September 2024 revealed a significantly enlarged prostate measuring 87 × 61 × 73 mm (volume approx. 200 mL). The imaging demonstrated a large, heterogeneous mass originating from the transition zone, causing marked apical compression of the relatively spared peripheral zone. The lesion showed overall low signal intensity on T2-weighted images, but the signal was noticeably higher than is typically present in conventional prostate adenocarcinoma. The mass showed diffusion restriction on ADC mapping (values 750–900 mm2/s) and marked contrast enhancement with central non-enhancing areas suggestive of necrosis. Extensive infiltration of the prostate base was noted, with bilateral involvement of the seminal vesicles and ductus deferentes, consistent with extraprostatic extension. A formal PI-RADS category was not assigned, as the lesion was considered atypical for conventional prostate adenocarcinoma and histopathological verification was prioritized. These baseline and post-treatment mpMRI findings are shown in Figure 1.
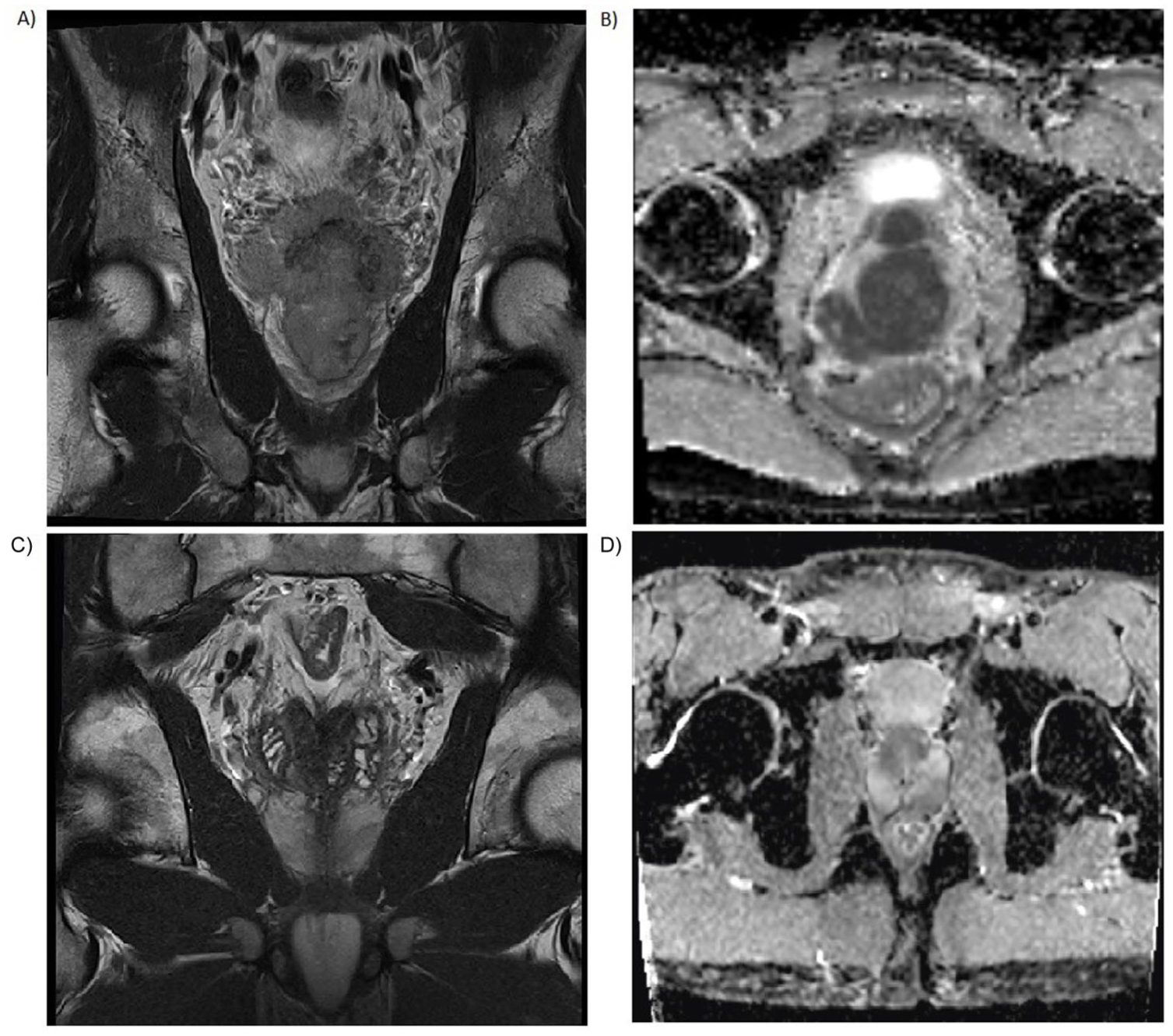
Multiparametric MRI of primary prostatic seminoma. Upper panel (Pre-treatment): (a) Coronal T2-weighted image showing a large, poorly demarcated hypointense mass involving the entire prostate gland. (b) Axial ADC map demonstrating marked diffusion restriction within the tumor. Lower panel (Post-treatment): (c) Coronal T2-weighted image and (d) Axial ADC map following 4× BEP chemotherapy, documenting complete structural and functional remission with restitution of normal prostatic volume.
Subsequent [18F]FDG PET/CT (October 2024) confirmed a massive, metabolically hyperactive prostatic lesion (73 × 95 × 75 mm) with an intense SUVmax of 15.14 (liver SUVavg 2.26). Notably, the staging scan showed no evidence of regional lymphadenopathy or distant metastatic spread, and scrotal ultrasonography excluded a primary testicular malignancy. Baseline and follow-up [18F]FDG PET/CT findings are shown in Figure 2.
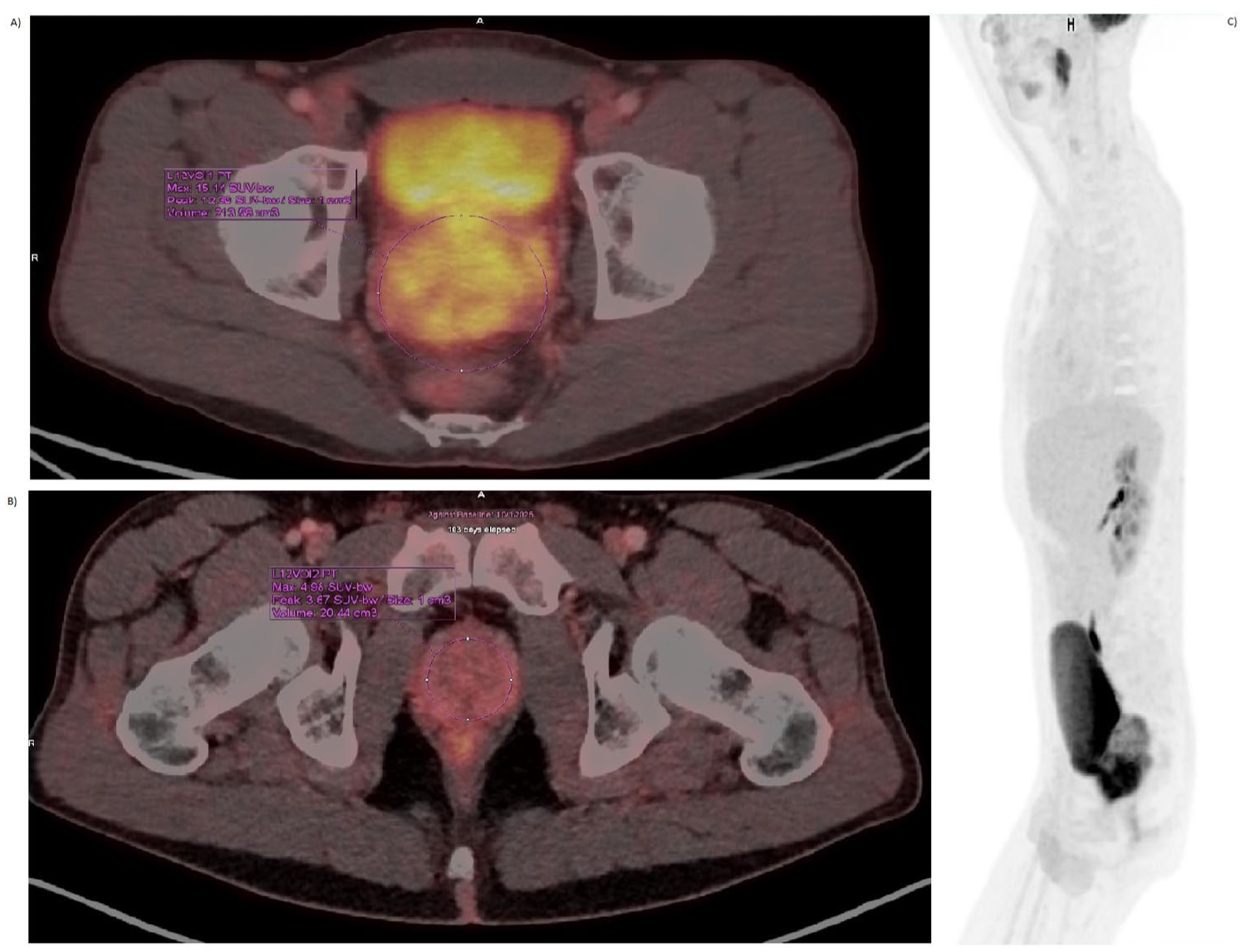
Functional imaging (baseline and response assessment). (a) Baseline axial [18F]FDG PET/CT demonstrating a massive, hypermetabolic mass in the prostatic region (SUVmax 15.14). (b) Follow-up axial [18F]FDG PET/CT following four cycles of BEP, confirming complete metabolic remission (residual SUVmax 2.5). (c) Sagittal PET MIP showing the localized nature of the primary tumor at baseline.
A TRUS-guided core needle biopsy was performed. Histological examination revealed a solid-growing high-grade malignant infiltrate composed of cells with rounded nuclei, dense chromatin, and indistinct amphophilic cytoplasm. High mitotic and apoptotic activity was observed, alongside focal necrosis and characteristic lymphocytic infiltration. Representative histopathological findings are shown in Figure 3.
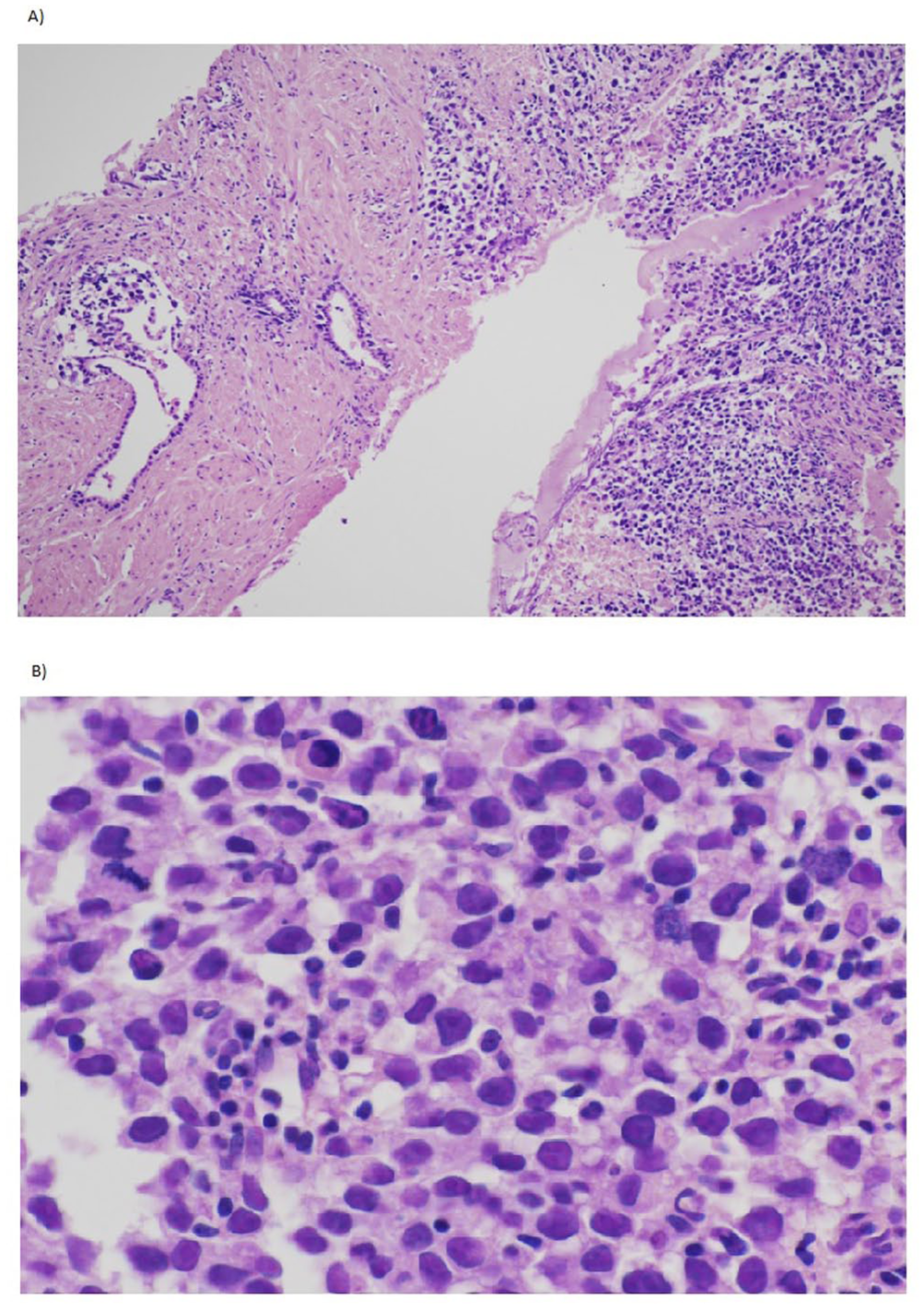
Representative histopathology (H&E staining). (a) Low-power magnification (100×) showing normal prostatic acini (left) being infiltrated by the malignant neoplasm (right). (b) High-power view (600×) demonstrating large neoplastic cells with prominent nucleoli and a characteristic background of small, mature lymphocytes.
Immunohistochemical (IHC) profiling was pivotal for the diagnosis. The tumor cells were positive for SALL4, c-KIT (CD117), and focally for placental alkaline phosphatase. Crucially, markers for other lineages, including PSA, Nkx3.1, ERG (prostatic), CD30, hCG, glypican-3 (non-seminomatous), and LCA (lymphoma)—were all negative. In particular, LCA staining was negative in tumor cells (Figure 4(c)). Based on the morphology and IHC profile, the diagnosis of PPS was confirmed.
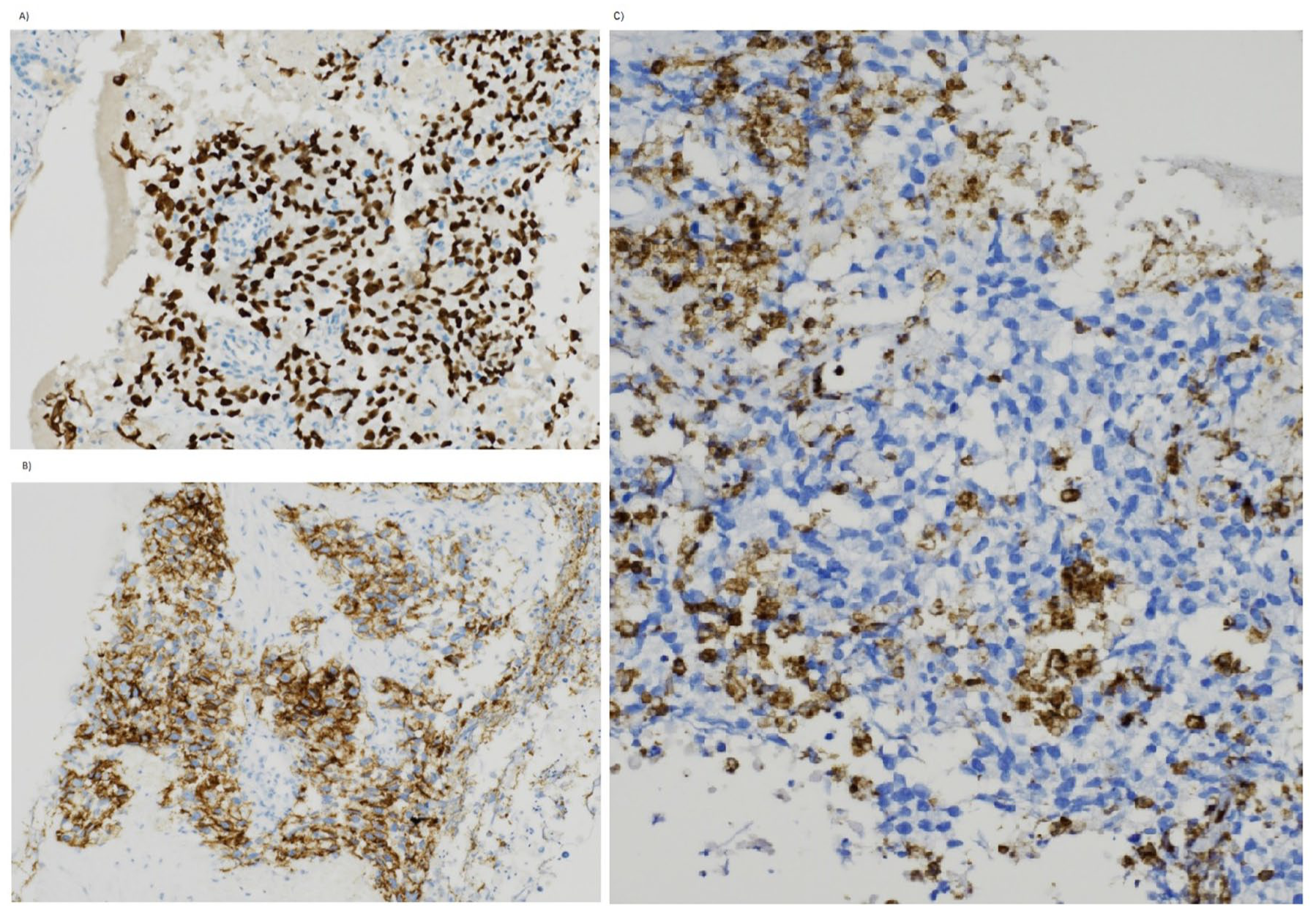
Immunohistochemical profiling and differential diagnosis. The tumor cells demonstrate strong, diffuse nuclear positivity for (a) SALL4 (200×) and strong membranous staining for (b) c-KIT/CD117 (200×), confirming the diagnosis of seminoma. Staining for (c) LCA (200×) is negative in the large malignant cells, while the small intratumoral lymphocytes serve as an internal positive control, effectively excluding primary prostatic lymphoma.
Based on the absence of non-pulmonary visceral metastases and the primary extragonadal site, the patient was classified as good-risk according to the International Germ Cell Cancer Collaborative Group (IGCCCG) criteria. Systemic therapy was initiated in November 2024. While three cycles of BEP or four cycles of EP are the standard for good-risk patients per NCCN and ESMO guidelines, a total of four cycles of the BEP regimen were administered in this case due to the massive local tumor burden and the exceptional rarity of the primary site. The patient demonstrated a dramatic clinical and biochemical response immediately after the initiation of the protocol.
The serum markers showed a rapid and profound decline. Following the first cycle (assessed on November 9, 2024), LDH levels plummeted from a baseline of 11.50 to 2.08 µkat/L, while beta-hCG levels normalized to <0.2 IU/L. This biochemical remission correlated with significant clinical improvement; the patient regained spontaneous voiding function, which allowed for the removal of the epicystostomy prior to the second cycle (December 3, 2024). After the third cycle, which commenced on December 30, 2024, laboratory evaluations remained stable, with LDH at 1.90 µkat/L and beta-hCG remaining undetectable.
The treatment course was characterized by manageable hematological toxicity, specifically grade 4 neutropenia and grade 2 thrombocytopenia (CTCAE v5.0). Non-hematological toxicity was minimal, limited to grade 1 nausea. The patient required standard supportive care with granulocyte colony-stimulating factors but successfully completed the planned therapeutic protocol without the need for dose reductions or treatment delays.
Following the completion of four cycles of BEP chemotherapy in January 2025, the patient underwent comprehensive restaging in March 2025 to assess the therapeutic response.
A follow-up [18F]FDG PET/CT (March 26, 2025) demonstrated complete metabolic remission. The previously massive hypermetabolic prostatic lesion showed a marked reduction in both size and glucose uptake, with the SUVmax decreasing from 16.18 to 2.5, a value consistent with physiological urethral activity. Metabolic activity in the seminal vesicles and pelvic region normalized. A mildly hypermetabolic focus (SUVmax 3.8) in the anterior mediastinum was interpreted as thymic rebound, a benign reactive phenomenon commonly observed in young adults following intensive chemotherapy.
Follow-up mpMRI (March 27, 2025) corroborated the clinical response and confirmed dramatic structural regression. The prostate volume significantly decreased to 40 mL. The previously extensive 90-mm lesion was no longer present and was replaced by small, residual T2-hypointense areas within the peripheral zone (9 mm on the right, 25 mm on the left). Crucially, the ADC values in these regions increased to 1100–1150 mm2/s, suggesting the absence of restricted diffusion. These findings were interpreted as post-therapeutic fibrotic changes or normal glandular tissue corresponding to the patient’s age rather than residual viable tumor. No pathologically enlarged pelvic lymph nodes were detected.
Biochemical markers remained stable during follow-up, with LDH at 1.90 µkat/L and undetectable beta-hCG levels. The serum PSA was 3.43 µg/L (PSA density 0.08), further supporting the hypothesis that PSA reflected residual benign prostatic tissue rather than malignant activity.
Clinically, the patient achieved full functional recovery. Following the removal of the suprapubic catheter, he maintained normal spontaneous voiding without obstructive symptoms or pelvic pain. At the most recent follow-up in January 2026, the patient remained in complete clinical, biochemical, and radiologic remission. A schematic overview of the diagnostic workup, treatment course, and follow-up is provided in Figure 5.
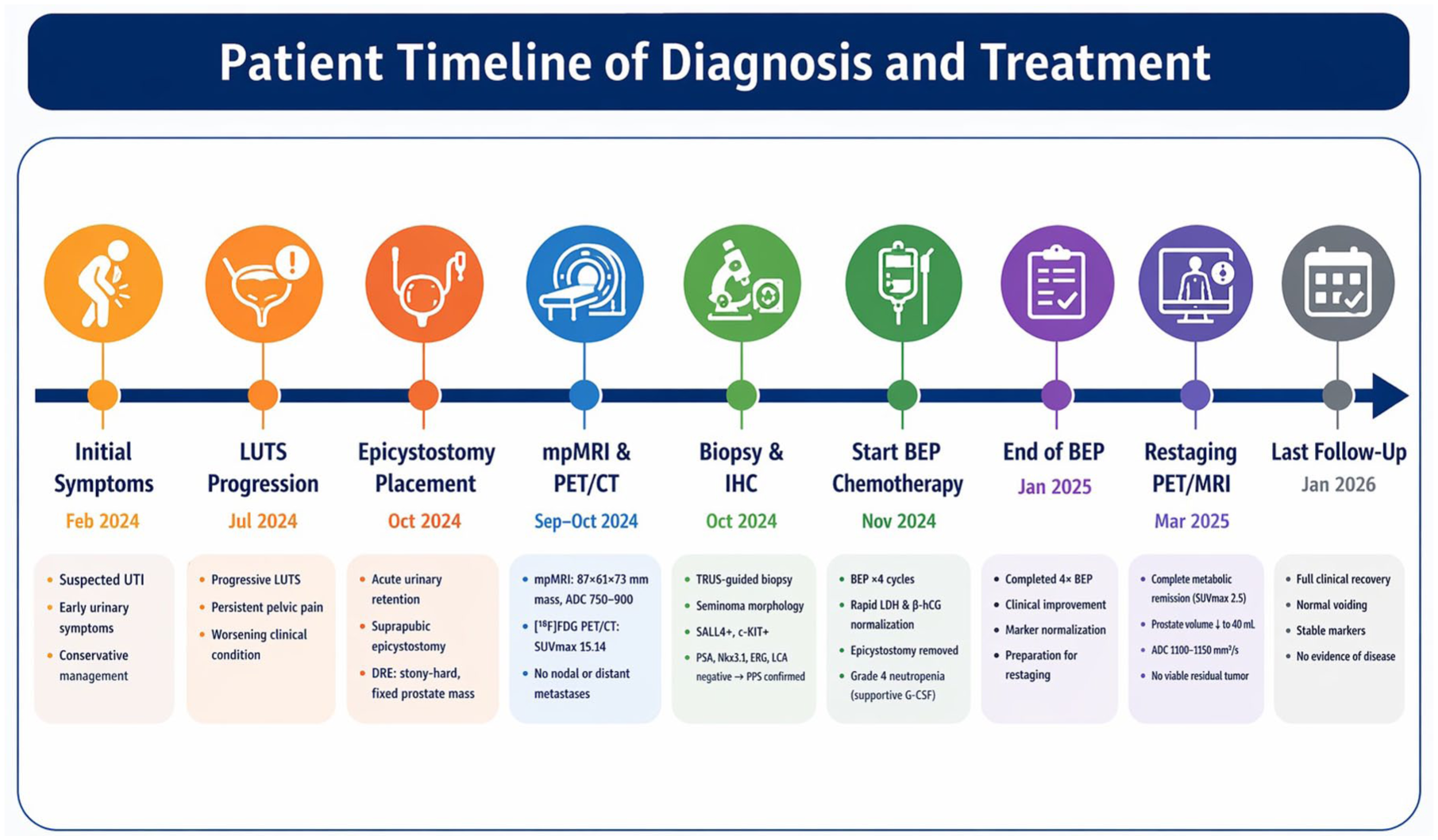
Clinical timeline of the patient’s diagnostic workup, treatment, and follow-up.
Methods
A structured literature review was performed in January 2026 to identify all reported cases of PPS. The search was conducted across PubMed (MEDLINE), Scopus, and Web of Science following PRISMA reporting principles. The initial search yielded 68 records (PubMed: 24, Scopus: 22, Web of Science: 22). After removing 27 duplicates, 41 records were screened by title and abstract.
The search strategy utilized the following Boolean string: ((“primary prostatic seminoma”) OR ((“seminoma” OR “germ cell tumor”) AND (“prostate” OR “prostatic”))). No initial date restrictions were applied to capture all historical records. However, to ensure relevance to contemporary imaging and chemotherapy standards, the final synthesis focused on the “modern era” (1990–2026). Inclusion was restricted to peer-reviewed articles published in English or those with available English translations.
The structured literature review was prepared in accordance with the PRISMA 2020 statement, and the reporting of this case report conforms to the CARE guideline.7,8 The completed PRISMA and CARE checklists are provided as Supplemental Material.
The selection process was conducted by the lead author (T.P.) and cross-checked by a second author (R.L.) to ensure the highest level of data accuracy. A total of 18 full-text articles were assessed for eligibility based on predefined inclusion criteria. Inclusion criteria required histologically confirmed pure primary seminoma originating within the prostate gland. Exclusion criteria were secondary prostatic involvement from testicular primaries, NS-GCTs, and cases with insufficient clinical data or unverified citations. The complete study selection process is detailed in the PRISMA flow diagram (Supplemental Figure 1).
For the synthesis of contemporary trends, we extracted data on patient age, clinical presentation, biochemical profile (PSA, LDH, beta-hCG), imaging findings (mpMRI with ADC mapping and [18F]FDG PET/CT), treatment modalities, and oncologic outcomes. The synthesized data were summarized in Table 1.
Reported cases of primary prostatic seminoma in the modern era (1990–2026), including clinical presentation, tumor markers, initial diagnostic suspicion, treatment, and outcomes.
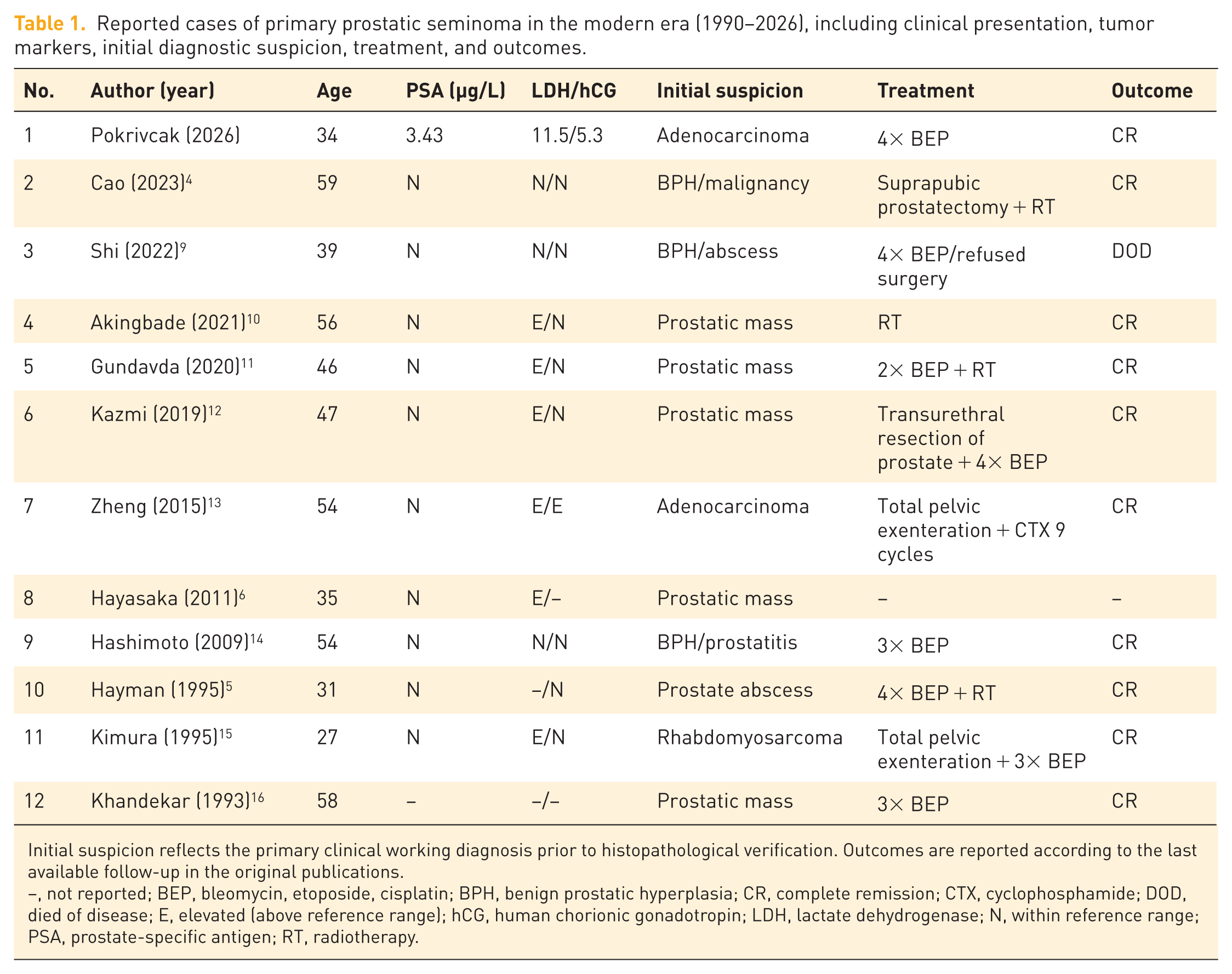
Initial suspicion reflects the primary clinical working diagnosis prior to histopathological verification. Outcomes are reported according to the last available follow-up in the original publications.
–, not reported; BEP, bleomycin, etoposide, cisplatin; BPH, benign prostatic hyperplasia; CR, complete remission; CTX, cyclophosphamide; DOD, died of disease; E, elevated (above reference range); hCG, human chorionic gonadotropin; LDH, lactate dehydrogenase; N, within reference range; PSA, prostate-specific antigen; RT, radiotherapy.
Structured literature review results
Our systematic search identified 11 eligible studies, which, together with the present case, resulted in a total of 12 documented cases of PPS reported between 1990 and 2026 (Table 1). The median age at diagnosis was 46.5 years (range 27–59). Clinical presentation was predominantly characterized by obstructive LUTS or marked prostatic enlargement. A consistent finding across the reviewed cases was the biochemical discordance between PSA and tumor burden, defined by serum PSA levels remaining low or within the normal range despite significant tumor burden. In contrast, serum LDH levels were frequently elevated, while beta-hCG remained within normal limits in the majority of cases. This pattern may raise suspicion for a non-epithelial malignancy, but histopathological confirmation remains essential for diagnosis. Overall, 10 out of 12 patients (83.3%, including the present case) achieved complete remission following cisplatin-based chemotherapy, radiotherapy, or a combination of both.
Discussion
Primary EGCTs are uncommon malignancies that typically arise in midline structures such as the mediastinum, retroperitoneum, or pineal gland. 17 Primary seminoma of the prostate represents an exceptionally rare entity, with only a limited number of cases reported since its initial description in the early 20th century. 4 Our structured literature review identified 12 cases reported since 1990 (Table 1), underscoring the diagnostic challenges associated with this atypical localization. The pathogenesis remains debated but is most commonly attributed to the aberrant migration of primordial germ cells during embryogenesis, with subsequent sequestration within the prostatic utricle.
Epidemiologically, the mediastinum is the most frequent primary site for EGCTs in adults (50%–70%), followed by the retroperitoneum (30%–40%). 1 While the clinical presentation varies significantly based on the anatomic compartment, the treatment response is largely dictated by histology. Extragonadal seminomas exhibit a high degree of sensitivity to cisplatin-based chemotherapy, regardless of primary location, mirroring the excellent outcomes observed in gonadal seminomas. In the IGCCCG “good-risk” category, to which our patient belonged, 5-year survival rates for extragonadal seminomas typically exceed 90%. 2 This stands in stark contrast to extragonadal NS-GCTs, particularly those of mediastinal origin, which are associated with a significantly poorer prognosis and lower rates of complete response to standard regimens. The sustained complete remission achieved in our case reinforces the observation that PPS follows the same favorable therapeutic trajectory as other seminomatous EGCTs when managed with standard platinum-based chemotherapy.
A key observation in our case is the marked discrepancy between the extensive local tumor burden and the disproportionately low serum PSA levels. In our patient, a tumor exceeding 90 mm in diameter was associated with a PSA level of only 3.43 µg/L, illustrating the marked discordance between tumor burden and serum PSA levels. This presentation represents a significant clinical pitfall and may lead to delayed diagnosis or misinterpretation as inflammatory or atypical prostatic disease. As demonstrated in our structured literature review, LDH and, to a lesser extent, beta-hCG may support diagnostic suspicion, but neither marker is sensitive nor specific for seminoma. In young symptomatic patients presenting with significant prostatic enlargement and low PSA, incorporation of a germ cell marker panel (LDH, hCG, AFP) into the initial diagnostic workup, alongside early biopsy, should be strongly considered to avoid diagnostic delay. The diagnostic approach to PPS has evolved with the integration of mpMRI and functional imaging. While mpMRI is highly effective for assessing local tumor extent, it lacks the specificity to reliably differentiate primary seminoma from other aggressive prostatic malignancies, such as poorly differentiated adenocarcinoma, sarcoma, or lymphoma. In this context, [18F]FDG PET/CT was used for staging and response assessment in our case. The high baseline metabolic activity provided a quantitative reference for treatment monitoring and helped confirm complete metabolic remission following chemotherapy. This is particularly relevant when residual structural abnormalities persist on conventional imaging, as functional techniques allow distinction between viable tumor tissue and post-therapeutic fibrosis. It is important to highlight the high negative predictive value of PET/CT in the post-treatment setting for seminoma. A negative scan significantly reduces the likelihood of viable residual disease, allowing for a surveillance-based approach rather than aggressive post-chemotherapy surgical intervention. Regarding therapeutic management, our findings further support that PPS retains the high chemosensitivity characteristic of gonadal seminoma. Importantly, in seminoma, prognosis is primarily determined by IGCCCG risk classification rather than the site of origin, and extragonadal location does not appear to adversely affect outcomes compared to gonadal disease. The rapid clinical and biochemical response observed after initiation of the BEP regimen underscores the efficacy of platinum-based systemic therapy. Although historical reports describe the use of surgery and radiotherapy, contemporary evidence increasingly supports cisplatin-based chemotherapy as the primary curative modality for extragonadal seminomas.
The differential diagnosis of a bulky prostatic mass with low PSA is broad and includes other non-epithelial malignancies. A structured overview of the principal differential diagnoses is provided in Table 2.
Principal differential diagnosis of bulky prostatic masses with low or mildly elevated PSA.
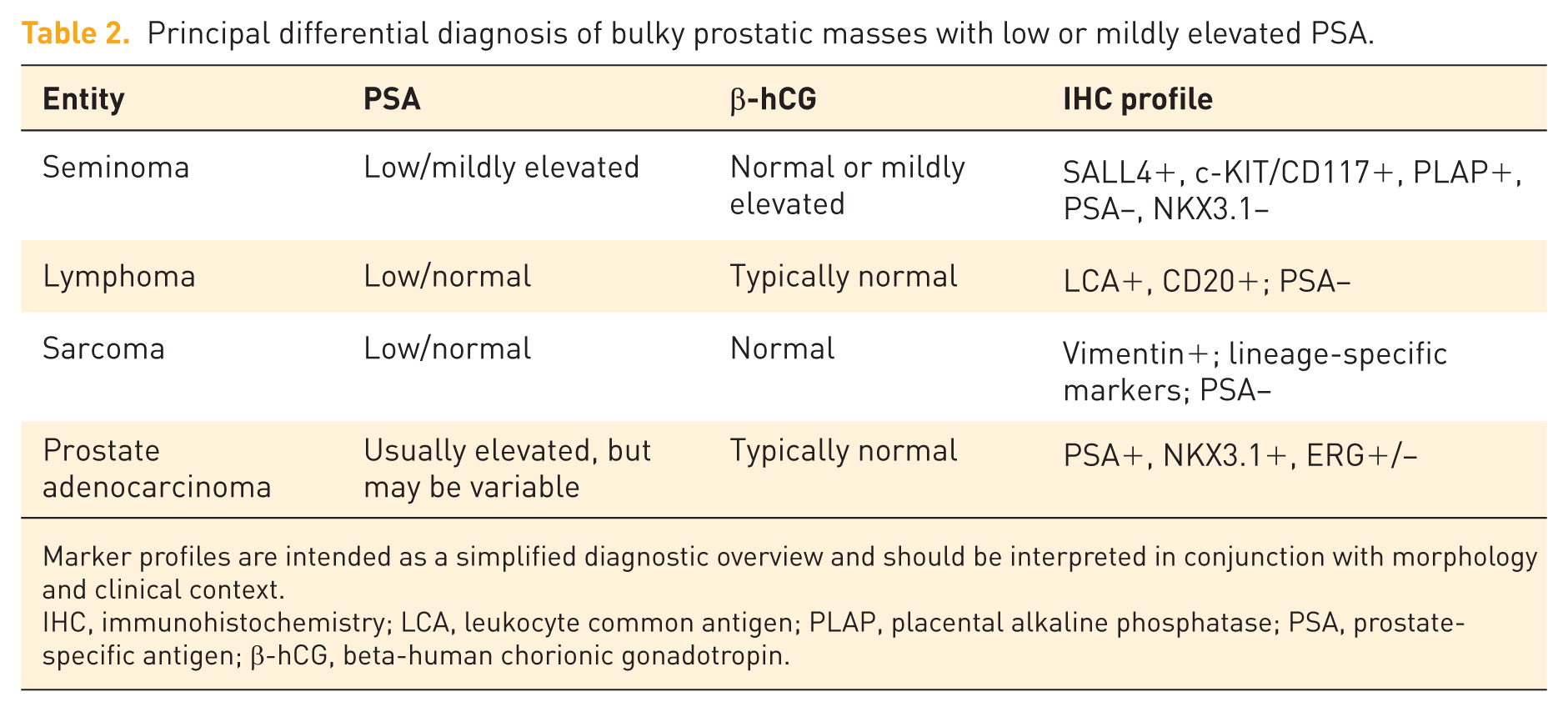
Marker profiles are intended as a simplified diagnostic overview and should be interpreted in conjunction with morphology and clinical context.
IHC, immunohistochemistry; LCA, leukocyte common antigen; PLAP, placental alkaline phosphatase; PSA, prostate-specific antigen; β-hCG, beta-human chorionic gonadotropin.
Primary prostatic lymphoma, although also rare, can present with similar clinical features. Prostatic sarcomas, such as leiomyosarcoma or rhabdomyosarcoma, must also be considered, as they typically present as aggressive, large-volume masses that do not produce PSA. Given these mimics, early TRUS-guided biopsy is the only definitive method to distinguish these entities and prevent inappropriate surgical or medical management. While radical surgical resection is considered for primary bulky prostatic malignancies, seminomas exhibit exquisite sensitivity to platinum-based chemotherapy. Our case, along with the reviewed literature, demonstrates that achieving a complete clinical response is possible through systemic treatment alone. Preserving the bladder and rectum not only maintains the patient’s quality of life but also avoids the high morbidity associated with pelvic exenteration in cases where a non-surgical curative option is available. Therefore, early histological confirmation via biopsy is paramount to prevent “over-treatment” by radical surgery.
Conclusion
Our case, in conjunction with the present structured literature review, suggests that biochemical discordance may represent a useful clinical clue in PPS. Clinicians should maintain a high index of suspicion in young patients presenting with atypical prostatic masses and low PSA levels, where the assessment of LDH and germ cell-specific markers may provide supportive diagnostic information. However, histological verification remains essential regardless of marker status. Prompt recognition and initiation of cisplatin-based chemotherapy offer a high likelihood of durable remission and favorable long-term outcomes in this rare but highly chemosensitive malignancy.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261465811 – Supplemental material for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance
Supplemental material, sj-docx-1-tam-10.1177_17588359261465811 for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance by Tomas Pokrivcak, Alexandr Poprach, Radek Lakomy, Pavel Fabian, Jiri Vasina, Michal Standara, Michal Stanik and Igor Kiss in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261465811 – Supplemental material for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance
Supplemental material, sj-docx-2-tam-10.1177_17588359261465811 for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance by Tomas Pokrivcak, Alexandr Poprach, Radek Lakomy, Pavel Fabian, Jiri Vasina, Michal Standara, Michal Stanik and Igor Kiss in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261465811 – Supplemental material for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance
Supplemental material, sj-pdf-1-tam-10.1177_17588359261465811 for Primary prostatic seminoma: a rare case report and structured literature review highlighting tumor marker discordance by Tomas Pokrivcak, Alexandr Poprach, Radek Lakomy, Pavel Fabian, Jiri Vasina, Michal Standara, Michal Stanik and Igor Kiss in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.