
Abstract
Introduction
Previous research concerning the conservative management of mallet finger has focused on splint application, with limited representation of supplementary rehabilitation and best practice. This research sought to investigate the practice and opinions of members of the British Association of Hand Therapists regarding their current treatment and to determine whether any specific exercise prescription or rehabilitation protocols are followed.
Methods
British Association of Hand Therapists members were contacted via e-mail and requested to complete an online survey. Thirty-five responses (5.7% response rate), 30 (4.8% response rate) of which were fully completed were obtained over the eight-week data collection period. The questionnaire consisted of 30 questions (20 quantitative and 10 qualitative) concerning therapists’ roles and condition management. Responses were analysed in terms of response frequencies, percentages and thematic text analysis.
Results
The results demonstrated current clinical practices in line with available best-evidenced practice. Conservative therapeutic management is diverse and varied. Therapists believe their role to be significant in optimising outcome success.
Discussion
Exercises and other interventions supplementary to splinting are commonly utilised in the therapeutic management of acute, closed mallet finger. This research found hand therapists implement a diverse range of clinical skills in order to optimise outcome success. Recommendations for best practice and further research are presented.
Introduction
Mallet finger commonly occurs following an axial load onto a flexed distal interphalangeal joint (DIPJ), resulting in a tendinous or bony avulsion of the terminal extensor tendon. 1 The term describes the subsequent unopposed flexed joint position caused by loss of active DIPJ extension. Frequently seen in Emergency Departments, the condition is associated with sporting injuries, but also occurs through innocuous activities such as pulling up socks and bed-making. 2 Acute closed mallet finger refers to the presentation time and mechanism of injury and excludes cases that are attributed to surgery, open injury, lacerations, co-existing trauma and rheumatoid or osteoarthritic conditions and those where presentation is delayed beyond two months. 3 Conservative management is widely considered appropriate for all acute injuries, excluding those that are open or involve over one-third of the DIPJ articular surface.4–6 However, it is also endorsed in more complex cases, such as those involving greater joint involvement and fracture displacement.5,7,8 This is mainly due to reported long-term complications associated with surgical intervention such as infection, joint incongruency and nail deformities.9,10 Despite favourable outcomes with recent advancements in surgical techniques,11,12 conservative management continues to be widely advocated and debated. Long-term outcomes are successful with regards to patient satisfaction and correction of DIPJ extension lag.13–17 Inferior outcomes are associated with delayed presentation 9 and poor patient compliance. 18
Previous literature reviews and professional guidance3,19,20 demonstrate limited research evidence and offer no clear conclusion for the most effective splint type or joint position in ensuring treatment success. Continuous splinting is advocated for approximately six weeks, but there is no indication of post-splinting management, despite recognition of common treatment impediments and complications. 20 Therapist-led clinics have produced successful outcomes with this population21,22 but information about treatment content, supplementary to splinting, is dated and limited. Deficiencies in literature were felt to justify investigation into the role of the hand therapist in the management of this condition and as to whether current therapeutic practices are meeting the goals of equality, value for money, efficacy and quality pursued by health care standards.23,24
Literature review
Terms and sources searched for the literature reviewed between April and August 2014.
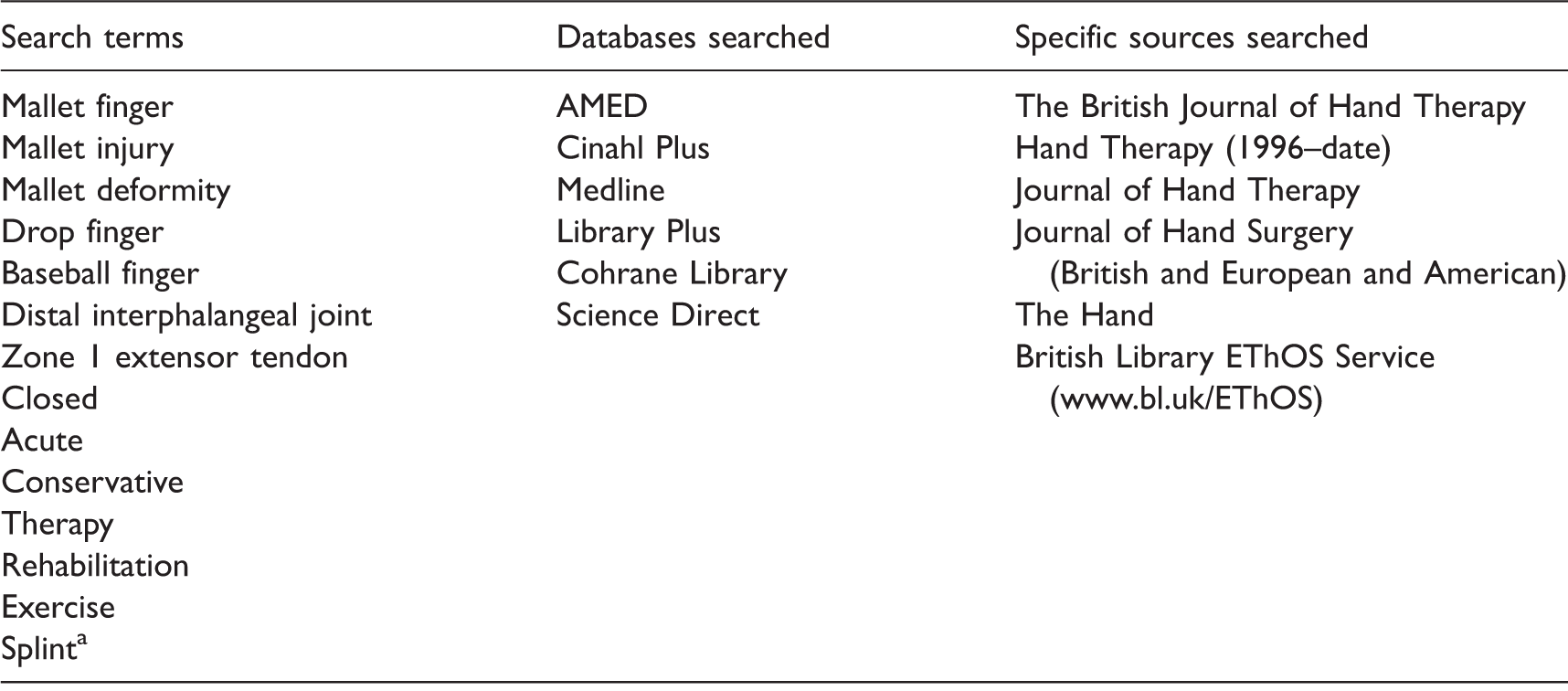
Indicates truncation of all possible word endings.
Research aims and objectives
This research aimed to investigate the practice and opinions of hand therapists based in the UK, with regards to the extent of their treatment of acute, closed mallet finger. Particular interest was given to the post-immobilisation period and factors influencing clinical decision making. It was proposed that the therapist’s role is undervalued and extends beyond that of splint provider. The objectives of the research were:
To determine the extent of the hand therapist’s role in the management of acute closed mallet finger. To establish what current interventions are used, supplementary to splinting, in the management of this condition. To determine hand therapists’ views on the relevance and efficacy of their role in the management of acute closed mallet finger.
Methods
Study design
A cross-sectional, non-experimental study design was undertaken, through use of a self-completed online questionnaire. Although the validity of results relies upon the honesty of respondents, 38 the anonymity and lack of researcher bias were proposed to positively influence data validity. 39 Prior web-based surveys of therapists’ views have obtained response rates ranging from 3% 40 to 31% 41 and demonstrated the additional benefits of being a quick and effective data collection method for a wide geographical area.
Data collection
Lack of pre-existing validated or published measure necessitated the construction of an original questionnaire. 42 This contained a combination of 30 closed and open-ended questions that obtained demographic data, details of clinical practice and therapists’ opinions. Questions were based on salient themes, which emerged from the literature review and prior study. 31 Topics covered splint type and position, duration of wear, the application of any splint weaning phase, supplementary rehabilitation and specific exercise prescription and/or avoidance. A participant information sheet was also provided, assuring anonymity, confidentiality and rights to withdrawal in accordance with ethical requirements.
Sample
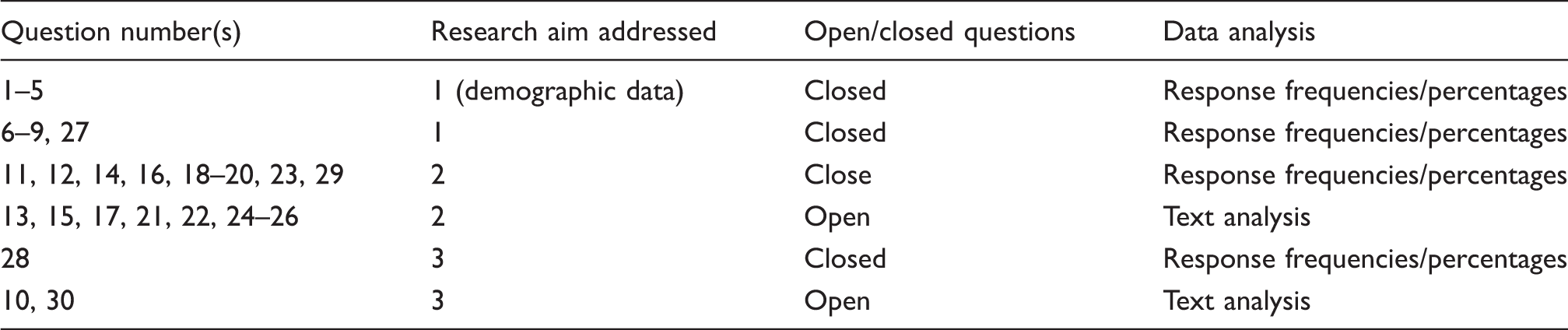
Summary and aims of questions included in final questionnaire.
Data analysis
Responses were grouped into emerging themes and summarised as response frequencies and percentages.
Results
Summary of demographic data.
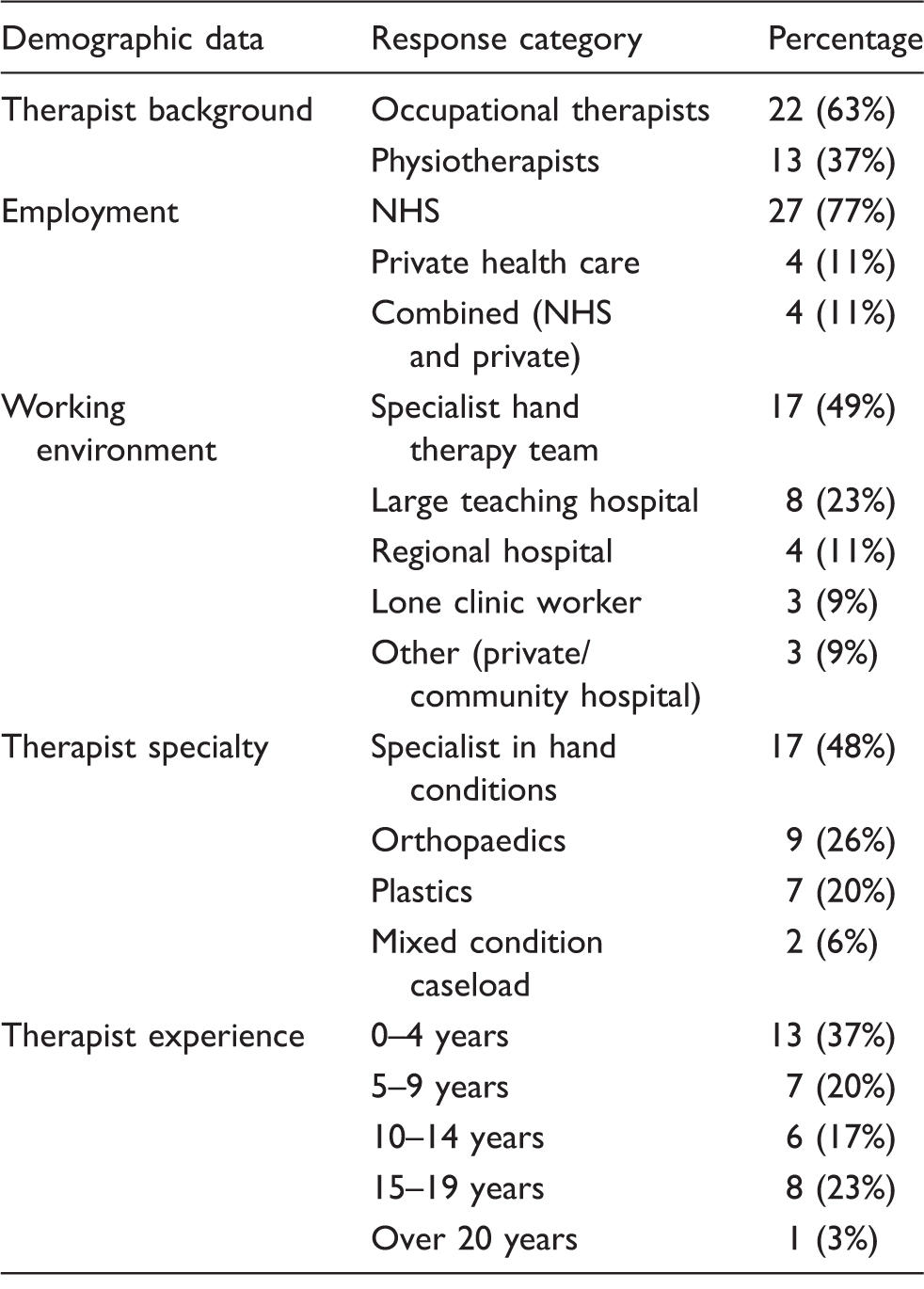
NHS, National Health Service
Current management and treatment interventions
Ninety-seven percent (34 of 35) of therapists worked within set protocols for the management of the condition. Most frequently reported protocol elements were the provision of guidance on splinting duration, splint type, DIPJ position and post-splinting exercise (Figure 1).
Aspects included within protocols for the management of acute, closed mallet finger.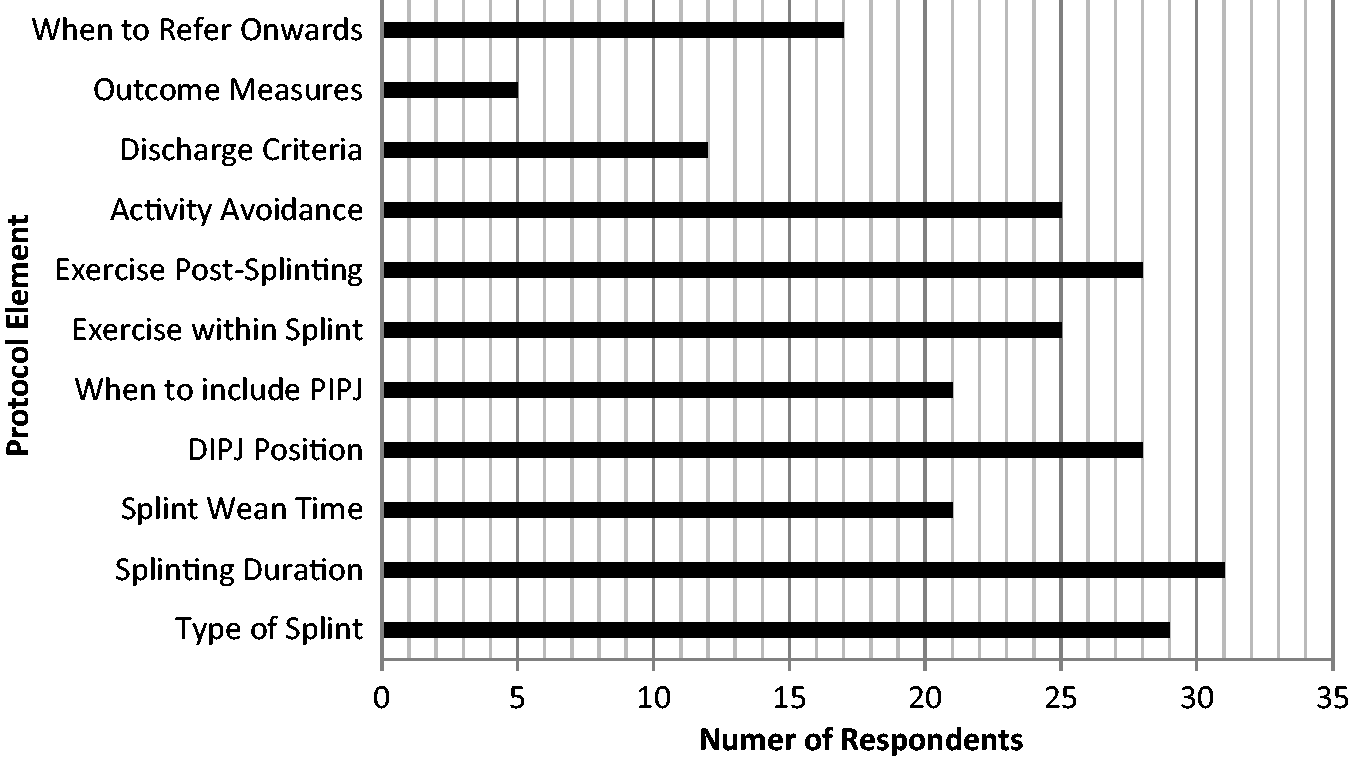
Therapists most frequently reported the provision of custom splinting, post-splinting follow-up, outcome assessment and discharge to constitute their role in mallet finger management. Provision of exercises during treatment, regular patient monitoring and determination of appropriate splint removal time were also reported elements of therapist intervention. Seventy-eight percent provided thermoplastic custom-made splints (Figure 2).
Types of immobilisation splint provided.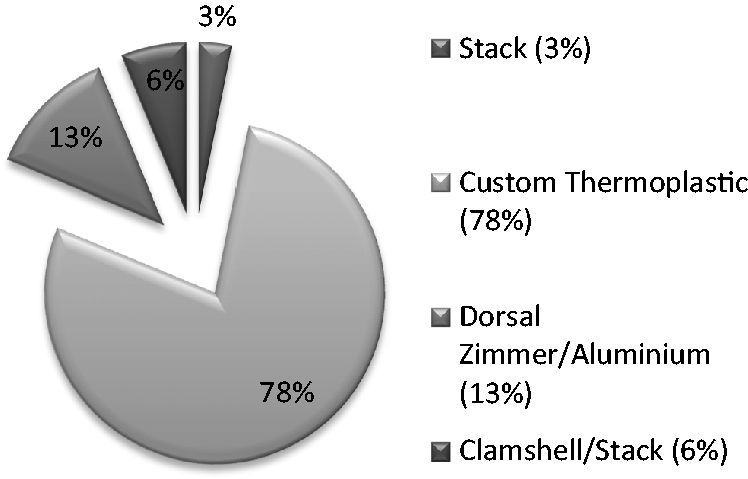
Twenty-six respondents (81%) advised continuous splinting for six to eight weeks (Figure 3).
Recommended DIPJ immobilisation period.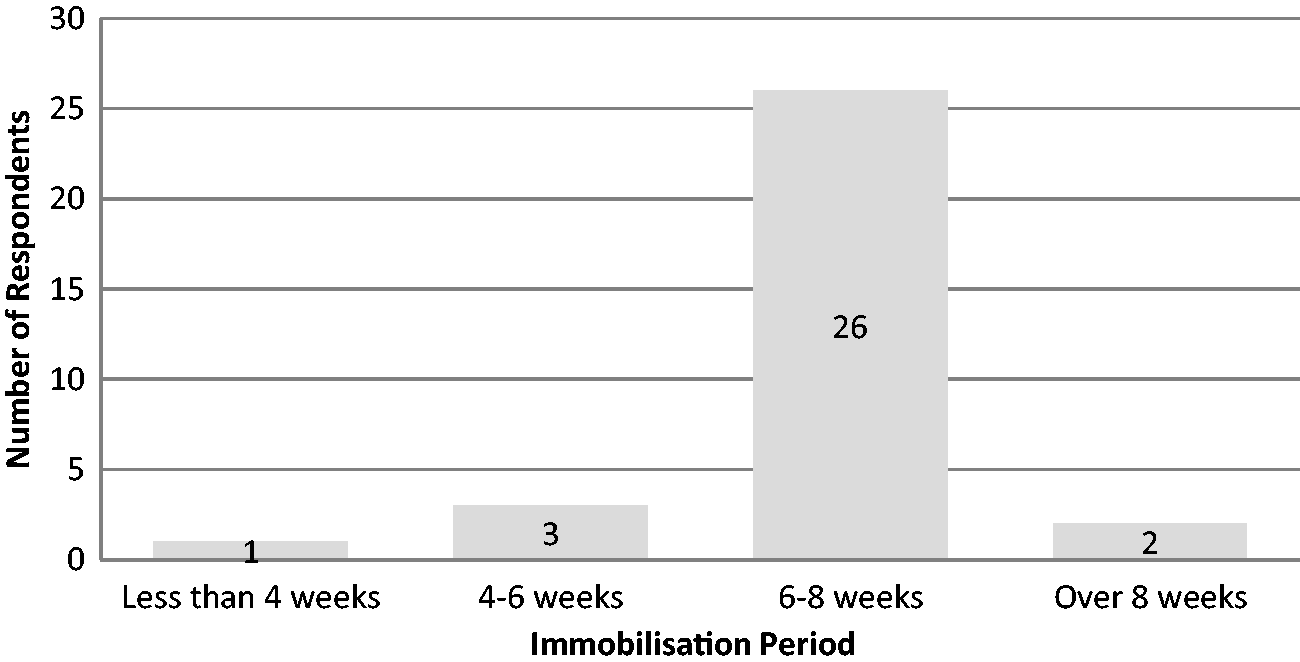
Eighty-four percent (27) reported extended splinting times for tendinous injuries. Splint weaning periods ranged from none to 12 weeks, although the majority (81%) recommended up to four weeks. Respondents reported basing this on individual patient lifestyle, tendon strength and DIPJ lag on initial splint removal. Proximal IPJ (PIPJ) immobilisation was not favoured with initial splinting, yet all respondents amended their management upon development of a swan-neck deformity. In such cases, therapists favoured dorsal splinting to include the PIPJ in between 15° and 40° of flexion. Oval-8® splints (3-Point Products, MD, USA) or Murphy® ring splints (North Coast Medical, CA, USA) were also widely used and a neoprene finger-tube was another suggested alternative. Careful weaning and specific advice were also considered appropriate in addressing swan-neck deformity, whilst regular active PIPJ flexion and early attention to mild PIPJ hypermobility at splinting onset were considered preventative measures. Although all respondents offered advice as part of their management, only 80% (24) provided this in written form.
Exercise provision
Identified exercise themes during DIPJ immobilisation.
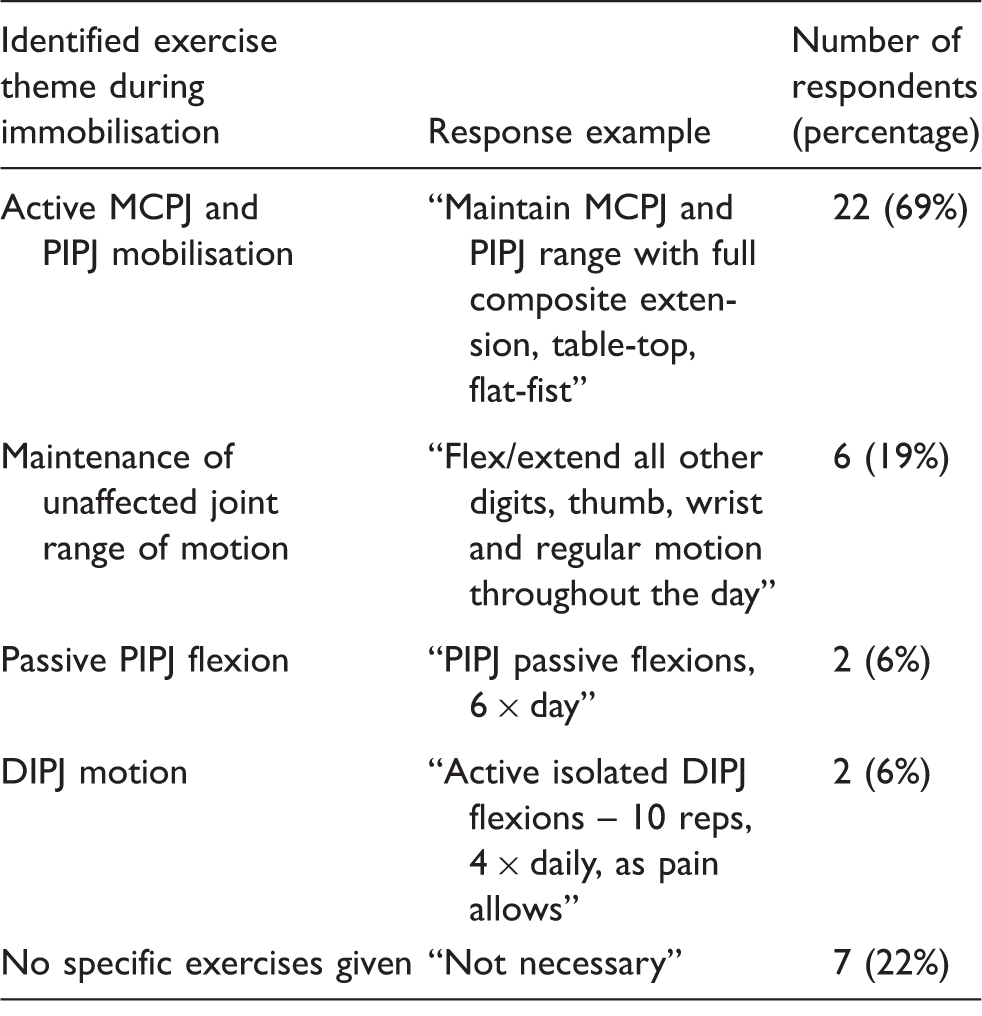
MCPJ, metacarpophalangeal joint; DIPJ, distal interphalangeal joint; PIPJ, proximal interphalangeal joint.
Themes and exercises reported on splint cessation.

DIPJ, distal interphalangeal joint; PIPJ, proximal interphalangeal joint.
Respondents declined to give exercises in cases with good active movement or a residual DIPJ extension lag. Ninety percent (28) offered advice on avoiding certain exercises and activities upon splint cessation. This included sport, housework and task specific activities where the digit is vulnerable, i.e. opening jars, carrying bags, twisting objects and ‘tucking in’. Twenty-three percent (7) avoided passive DIPJ flexion at any stage of management. In general, DIPJ flexion exercises were seen as unnecessary, other than to address joint stiffness and movement restriction. Thirty-seven percent (11) initiated passive DIPJ flexion no sooner than 10 weeks post injury. Forty-three percent (13) did not routinely assess nor address strength and grip as part of their management. Of those who did, 71% (12) introduced gripping activities no earlier than eight weeks post injury. Therapists’ management also included initial assessment and monitoring, hygiene checks and specific patient and carer teaching sessions for splint removal and reapplication.
Therapists’ views on outcome success and job role
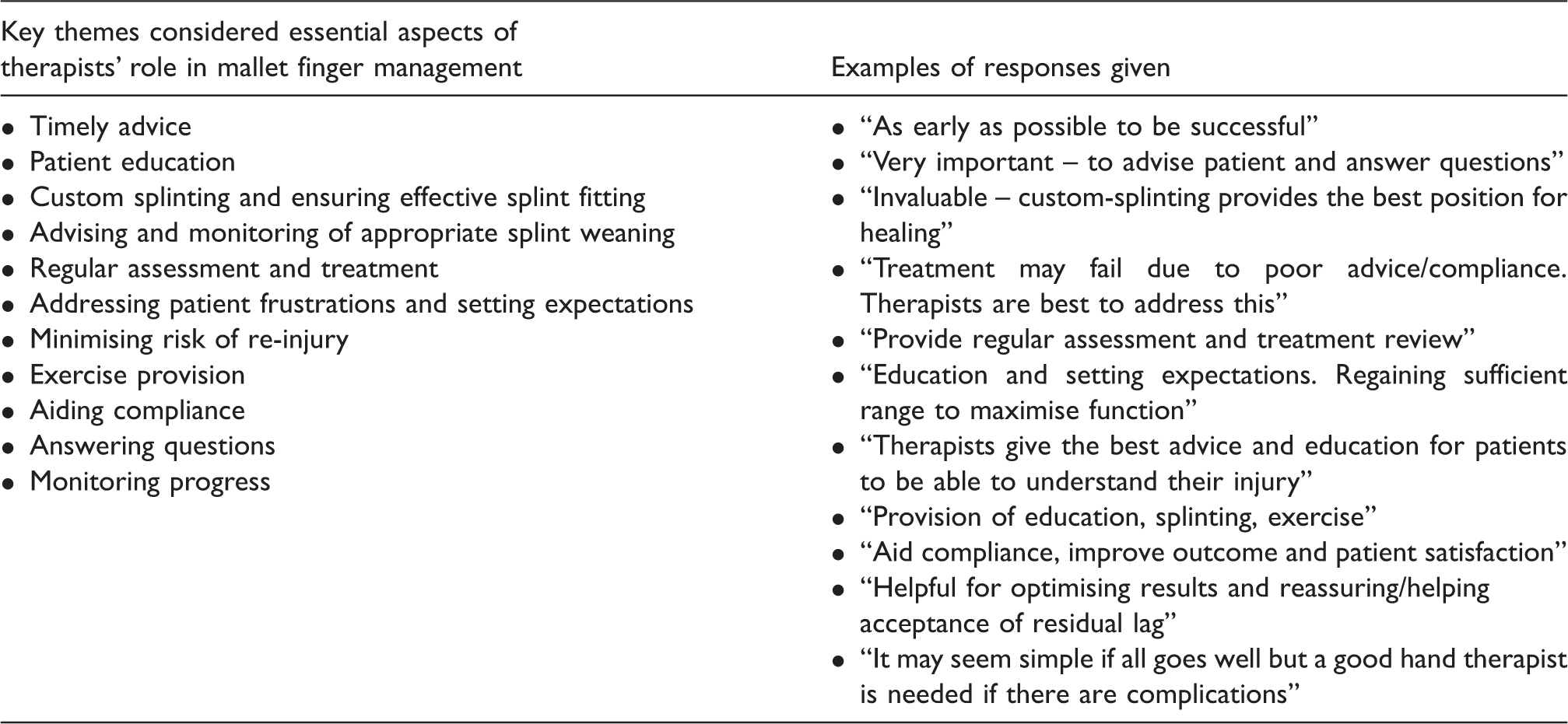
Respondents ranked seven various determinants of outcome success in terms of their importance (Figure 4) with 1 being the least and 7 the most important. Sixty percent (18) determined functional ability as the most important, whilst 63% felt passive range of motion was the least important measure of outcome success. In light of an unsuccessful period of initial splinting, 77% (23) recommended further splinting. No respondents identified that they would discharge the patient without further discussion or advice. Text analysis of open questions determined that therapists felt their role in mallet finger management to be significant in optimising outcome success, ensuring effective splint fitting, monitoring compliance and offering appropriate advice. Prior experience was felt to influence and justify clinical decision making (Table 6).
Respondents’ median ranking of importance for determinants of outcome success. Key themes identified in therapists’ opinions on their role significance.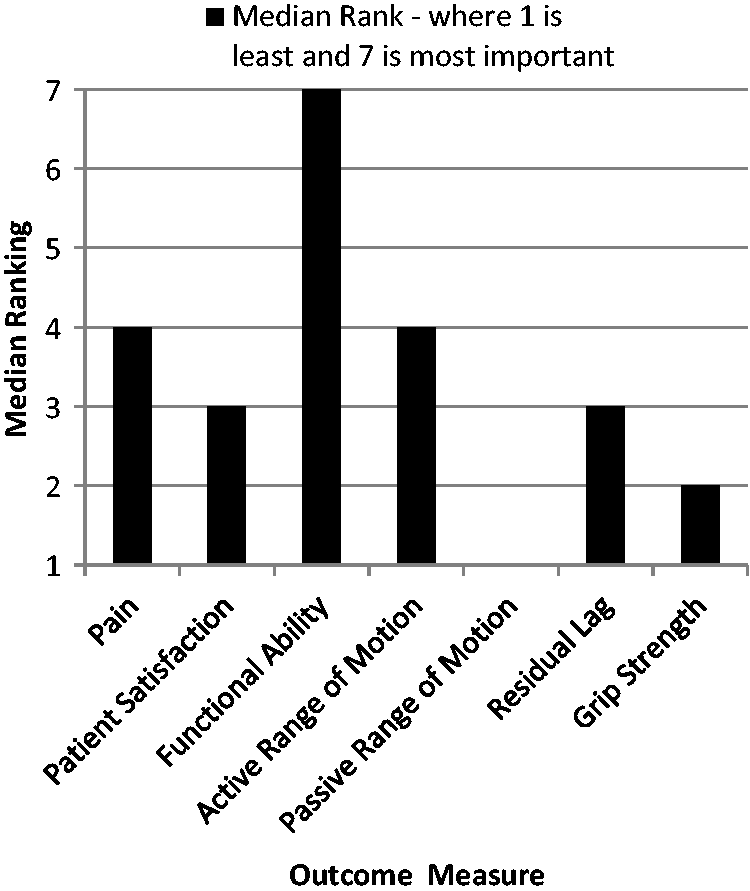
Discussion
Despite the limited generalisability afforded by the low response rate, the survey yielded relevant information concerning current therapeutic intervention in the conservative management of acute, closed mallet finger. The sample demographic data highlighted the diverse experience and working environments in which hand therapists are employed and compared favourably to that of current BAHT members in terms of occupational therapists and physiotherapist ratios. However, purposive sampling through the use of a web-based survey to BAHT members relied heavily on specific and willing participants and therefore has limitations regarding the generalisability of findings to other BAHT and non-BAHT therapists. Improved validity would be afforded by investigation of a larger sample that ensures the inclusion of multiple treatment centres, more evenly distributed therapist demographics and non-BAHT members. A more detailed review of therapists’ clinical decision-making processes may highlight areas for care quality improvement and standardise current practice.
Research aim 1: Determining the extent of hand therapists’ role in the management of acute, closed mallet finger
Prior investigation into early mallet finger management within Emergency Departments27–29 may explain the limited representation of specific therapy; yet, research within specialist orthopaedic and hand centres2,25,26 has also under-represented hand therapists’ interventions and role significance. Therapist-led mallet finger clinics have demonstrated the clinical importance and autonomy of practitioners 22 and survey results reflected such practice. All except one respondent reported working within a set treatment protocol. This therapist was lone-working within a small private health care clinic; yet, their responses reflected the same autonomous and responsive management of those working within standardised treatment practice in specific hand centres. Specific protocols appeared to provide guidelines for appropriate triage and treatment progression, requiring sound clinical reasoning in patient-specific care (Figure 1). Hand therapists play a varied role in mallet finger management, often reliant upon appropriateness and timing of referrals. More extensive research into the extent and timing of therapist involvement and subsequent outcome success across a variety of treatment centres would be of further clinical interest.
Research aim 2: Establishing current interventions in condition management
Splint provision and joint involvement
Previous literature has failed to demonstrate consensus on the most effective splint design.3,19 However, custom splinting has been shown to permit a more appropriate and comfortable fit and potentially fewer skin complications2,25–27 and was the favoured splinting option by respondents (Figure 2). Clinical and biomechanical literature proposes PIPJ exclusion during immobilisation2,26–29,31,43–45 and findings of this research confirm this practice. Furthermore, therapists reported their ability to tailor splint design and exercise in order to prevent and manage subsequent complications.
Splint immobilisation and weaning period
Eighty-four percent (27) of respondents observed a longer immobilisation period for tendinous injuries. Although 81% (26) respondents reported a six- to eight-week splinting period (Figure 3), only 72% (23) defined this to be six weeks for bony mallets and eight weeks for tendinous injury. Previous research2,19,25,26,31 suggests continuous six- to eight-week splinting, with night splinting until 12 weeks post presentation; whether tendinous or with bony involvement. Support of a splint weaning period post-immobilisation is lacking within high-level clinical evidence,2,26,46 yet all respondents indicated this to be their standard practice, with 81% recommending a period of up to four weeks. Further investigation is warranted into the efficacy, implications and timescales of splint weaning and to provide more robust evidence for its undertaking.
Exercise and supplementary intervention
Exercise provision during and post splint removal was advocated by 81% (25) and 90% (28) respondents, respectively. Suggested activities included flat and composite fist, digital extension, isolated/blocked PIPJ flexion and extension (Flexor Digitorum Superficialis [FDS] glides) and proximal joint and uninjured digit exercises (Table 5). These offer the benefits of active motion and address intrinsic and ligamentous tightness 47 and extensor tendon glide. 48 Passive PIPJ flexion was suggested to maintain range and prevent swan-neck deformity. Two respondents (6%) advised active DIPJ exercise during initial immobilisation, although biomechanical evidence contests this.49–54 Tendon lengthening of one millimetre may produce an extensor lag of 25°, 43 but can be prevented through DIPJ extension immobilisation.55,56 Stress application and tendon glide with proximal joint motion limit adhesion formation and maintain strength.52,57 However, this is unnecessary at the extensor terminus, where insertion stability is essential and tendon excursion is negligible.58–61 Maintaining PIPJ flexion was highlighted by 92% (23) respondents and considered significant in preventing swan-neck deformity. Biomechanical evidence supports this suggesting it to discourage proximal migration of the dorsal mechanism in the presence of terminal tendon deficiency.57,61,62
Ninety-four percent of respondents recommended exercises on completion of continuous splinting (Table 6). The number and frequency of exercises ranged from 5 repetitions undertaken hourly to 5 to 10 repetitions performed three to four times daily. One to three sets of 6 to 12 repetitions of resistance exercise on alternate days have been advocated for strength improvements. 63 Stretches for up to 60 seconds, repeated two to four times, are recommended at least two to three times weekly in order to increase range of movement and tissue flexibility. 63 There are no specific guidelines for exercise load, frequency or duration following mallet finger injury. Avoiding undue stresses is recommended with immature and healing tissue.49–54 Immobilisation has been shown to reduce tensile strength, inhibit tendon glide and increase adhesion formation. 64 Active exercise maintains motion and prevents adhesions65,66 and early application is favoured in recent advancements in extensor tendon rehabilitation.67,68 Despite this, the immobilisation of terminal extensor injuries is justified by the need for stability and limited tendon excursion.43,59–61 In one case, guide splints were advocated to gradually increase DIPJ flexion over a four-week period. A similar undertaking has been previously reported in an unpublished small-scale Irish study. 33 The authors questioned whether the non-significant but marginal improvement in DIPJ extensor lag was offset by the necessary cost and time implications of increased therapy input. Further clinical research is required into the timing and intensity of active motion within this population. The optimum type, frequency and duration of such exercises also require further exploration in order to guide best practice.
Commonly cited outcome scores define anything between a 15° and 25° lag as poor or failed treatment.69,70 A lag of up to 10° may be deemed a successful outcome, yet high patient outcome satisfaction has been found with a residual extensor lag of up to 30°. 4 More recently as much as a 40° flexion deformity is suggested to have minimal impact on patient concern and functional performance. 71 Survey results suggested that, in terms of outcome success, therapists grant equal priority to patient satisfaction and residual lag, but attribute greater significance to functional ability (Figure 2). This implies that a good functional outcome may not necessarily indicate high patient satisfaction, or full correction of DIPJ extension lag. Investigation into how therapists evaluate functional outcome success would be of further clinical value. Assisting patients to comply with treatment and cope with an unfavourable outcome were also identified as important therapist attributes. Ninety-two percent advocated further splinting in light of a failed initial period. Other literature supports splinting chronic cases of mallet finger 35 and those with delayed presentation 72 ; although surgical intervention may subsequently be required. 73 Responses demonstrated therapists to be instrumental in educating patients about these procedures, which can assist in their future decision making.
The majority of respondents (93%) reported the provision of specific one-to-one management. Effective understanding of splinting requirements is essential to ensure compliance and optimise treatment success.2,18,27 However, this can be poor despite regular follow-up and education.2,26 Patient-specific care can address individual unhealthy behaviours and beliefs and promote self-efficacy;74–76 thus, further maximising rehabilitation potential. Therapists use clinical judgement to adapt splinting timescales and weaning periods, grade exercises and functional exposure. Further input may involve offering advice on sports return and activity avoidance and assisting adaptation in light of an unsuccessful outcome. Therapists might consider the provision of written information in order to substantiate their verbal advice. This is suggested in light of only 80% respondents reporting this as current practice.
Research aim 3: Determine hand therapists’ views on the significance of their role in condition management
Respondents believed appropriate and timely intervention to be essential for achieving outcome success (Table 6). However, nurse practitioners and Emergency Department staff were identified as being equally capable of providing appropriate advice and splinting. Furthermore, a recent UK one-year service audit 77 found a self-care mallet finger protocol to produce acceptable functional results and patient satisfaction.
Therapists considered their intervention necessary in optimising treatment success through the provision of tailored and well-fitting splints, advice and exercise and ensuring patients to be well informed and compliant. They also identified the more significant role they have in addressing complications through their advanced clinical reasoning and diverse practical skills. However, the cost-efficacy of early and continued therapeutic intervention requires further research. Delegation of uncomplicated cases of acute, closed mallet finger to a therapist-led clinic is effective and provides hand surgeons with more time for complex injuries. 22 Furthermore, prevention of complications through timely and appropriate management may minimise the subsequent costs and time demands of further surgical and therapeutic intervention.
Conclusions
A summary of best practice relating to the findings of this study and available literature is presented in Figure 5. Custom thermoplastic splinting was considered the preferential means of DIPJ immobilisation. The practice of six to eight weeks continuous immobilisation was observed; six weeks for bony and eight weeks for tendinous injury (72% respondents), as is consistent with other survey evidence
31
and appropriate healing times.49–54 Despite the questionable efficacy of a splint weaning period,
46
it was often seen as clinically necessary by respondents and influenced by individual presentation and functional demand. The majority (81%) advocated such practice for up to four weeks; splinting intermittently in the day for protection as well as at night. Range of motion exercises for unaffected and proximal joints may be appropriate during the DIPJ immobilisation period; subsequently incorporating graded exposure to increasing DIPJ flexion and extensor resilience upon splint removal. Functional ability was considered the most significant indicator of successful outcome, whilst passive DIPJ flexion and grip strength tended to be initially avoided and considered of low significance. Supplementary intervention may include advice and education on condition, compliance and prognosis, reinforced with written material. Regular and patient-specific therapeutic intervention, although costly, may be justified by the consequences of ineffectual initial management. Therapists considered their role to be significant in the effective management of acute, closed mallet finger with results demonstrating the varied interventions often undertaken. However, the limited representation of hand therapist management within existing literature2,25–29 undervalues their clinical skills by failing to demonstrate this.
Flow chart summarising current management and best-evidenced practice.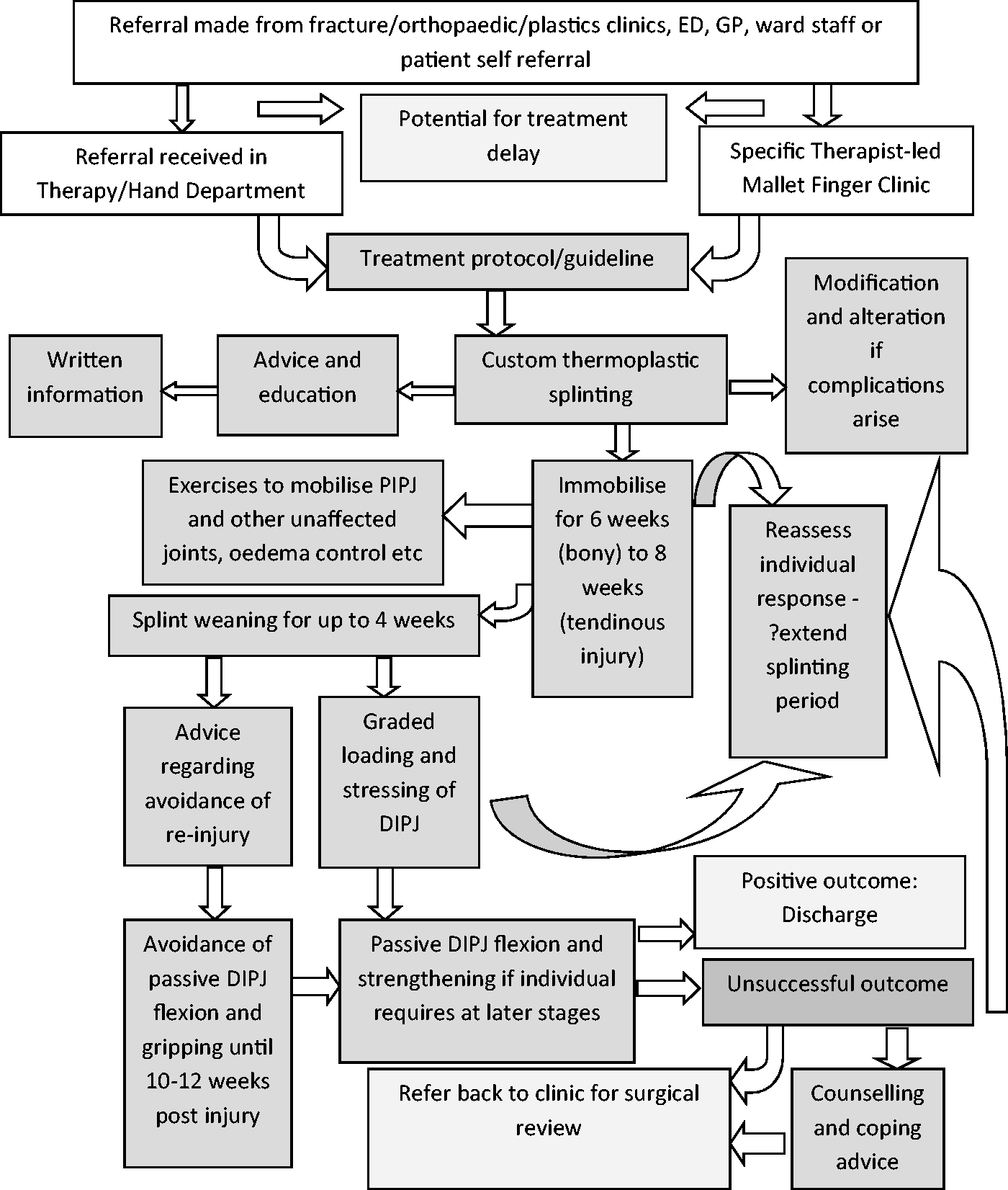
Footnotes
Acknowledgements
SC wishes to thank Leanne Miller, Eve Dunn, Katy Mitchell and the BAHT Clinical Evidence Committee and those BAHT members who kindly responded to the research questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
An on-line information sheet was provided for all participants and consent was implied with questionnaire completion and submission.
Ethical approval
Ethical approval for this study was obtained from the College of Health and Social Care Research Ethics Committee, University of Derby (14.07.14).
Guarantor
SC.
Contributorship
SC undertook this research towards an MSc in Hand Therapy from the University of Derby. SC conceived and implemented the research, literature review and its documentation. Permissible supervision, guidance and corrections were provided by ND and SW. ND also assisted with preparation for publication and proof read and amended the final manuscript.