
Abstract
Introduction
Pinch strength is a widely used measurement of hand function, but digit position on the pinch gauge has not been described in the literature. The aim of this study was to assess for differences in tip, lateral, and three-jaw-chuck pinch force when the digits are placed on the groove or bridge of a Bernadette and Linda pinch gauge.
Methods
Thirty-six healthy volunteers each pinched six times in random order: one for each type of pinch force with the digits placed in each position.
Results
There were no significant differences in pinch strength measurements based on digit position, except for three-jaw-chuck pinch which was slightly higher on the groove. Equivalence was found within one pound for tip and lateral pinch but not for three-jaw-chuck.
Conclusion
Variations in finger position may result in similar pinch strength measurements for tip and lateral pinch. Clinicians may reliably assess lateral and tip pinch using either position; however, standardized positioning is still recommended.
Introduction
Pinch strength measurement is a key point of interest to a myriad of health professionals working in hand therapy. A direct relationship between pinch strength and function has been demonstrated and illustrates the importance of hand strength in clinical practice.1,2 Clinicians, especially those interested in preventing deformities and preserving functional performance, utilize pinch strength as an assessment tool and outcome measure. Specifically, pinch strength measurement using the “gold standard” Bernadette and Linda (B&L) pinch gauge has been found to be psychometrically sound with established reliability and validity.3,4 Clinicians and researchers utilize pinch strength to compare clients’ strength with normative data, characterize upper extremity impairment, document improvement in strength and overall function, determine goals, demonstrate industry research outcomes, and provide appropriate interventions.1–6
Position of the upper extremity during hand strength measurement has been a topic of discussion for decades. In 1981, the American Society of Hand Therapists (ASHT) suggested standardization of arm position during grip strength tests. 7 Fess and Moran recommended, “the patient should be seated with his shoulder adducted and neutrally rotated, the elbow flexed to 90˚, and the forearm and wrist in neutral position.” 7 However, while these recommendations may be valuable, they do not necessarily provide a standard testing position specific to pinch strength. A measurement protocol specific to pinch strength was not included in the most recent ASHT clinical assessment recommendations, nor has it been established in the literature thus far. Several studies have addressed the impact of certain factors on pinch strength as well as providing recommendations for standardizing pinch strength positioning independent of grip strength.8–11 However, positioning the finger on the bridge or the groove of the pinch gauge has not been carefully described. Therefore, additional normative studies specific to hand and forearm positioning are needed to establish a comprehensive standard measurement protocol for the assessment of pinch strength.
One study addressed the effect of various upper extremity positionings on pinch strength with 20 healthy male students aged 20 to 34 years. 8 Results indicated no effect of shoulder position on pinch strength measurements, but a large effect of elbow position on pinch strength measurements when the elbow was flexed 120° or more. Similarly, Halpern and Fernandez 8 examined forearm and wrist positions. This experiment included 27 combinations involving three different pinches (lateral, tip, and three-jaw-chuck), three forearm positions, and three wrist positions. Results of their study indicated that for all three types of pinch combined, maximum flexion and extension of the wrist resulted in decreased pinch strength measurements. The pronated forearm position also showed decreased pinch strength measurements (up to 7%), as compared with supinated and neutral forearm positions.
Stegink Jansen et al. 9 researched the effect of three forearm positions on lateral, tip, and three-jaw-chuck pinch measurements. 9 This study agreed with an earlier study by Woody and Mathiowetz, 10 which found that forearm position did not affect three-jaw-chuck pinch measurements. 9 However, unlike those researchers as well as Halpern and Fernandez, Stegink Jansen et al. found differences in lateral and tip pinch measurements between the different forearm positions.8–10 They found measurements of lateral pinch to be lowest in the supinated position, while tip pinch measurements were lowest when the forearm was pronated. Although these differences were noted, none of the differences were found to be statistically significant (largest effect size 0.144). The researchers used these findings to suggest that “standardization of forearm position is recommended when measuring pinch strength, but not required.” 9 They also indicate that the lack of standardization regarding finger placement on the bridge or groove of a B&L pinch gauge, could be a confounding factor when interpreting results of current, recent, and future studies.
Although little research has been done on the effect of finger position on pinch strength measurements, two studies have addressed factors specific to the hand. In one study, McCoy and Dekerlegand 11 addressed the lack of standardization for positioning of the ulnar three digits during tip pinch with 76 healthy volunteers. They found that pinch was stronger when the fingers were flexed, which agreed with findings by Hook and Stanley. 12 These researchers suggested that lack of standardization could greatly impact pinch strength measurements because the values are small, and hence even small differences could largely impact pinch measurement scores. In another study, Apfel 13 sought to determine if thumb interphalangeal (IP) joint position, flexed or extended, affects lateral pinch measurements. This study examined two IP joint positions, flexed or extended. Findings included significant differences in pinch strength measurements depending on IP joint position when all ASHT positioning standards were followed. For females and males, IP joint flexion showed an increase in strength by 28–30% and 36–38%, respectively, as compared to IP joint extension measurements.
Currently, no studies in the literature have focused how finger and thumb positioning on the pinch gauge impacts pinch strength. The potential problem may be due to how clinicians guide clients to place fingers and the thumb on the pinch gauge versus calibration standards of the pinch gauge. B&L Engineering pinch gauges are calibrated with a digital force gauge by placing the pinch gauge into the force gauge at the groove. Therefore, the owner of B&L, Lee Barnes, recommends that clients place fingers on the groove of the pinch gauge (Figure 1) when taking pinch measurements (L Barnes, personal communication, 17 October 2012). This is in contrast to the position of the ASHT Clinical Assessment Recommendations which state: “the fingertips must stop at the groove.” 14 There were no studies found specifying the area of contact between the tip of the finger and thumb, but authors who presented illustrations of the test position showed that subjects pressed the bridge (Figure 2) of the pinch meter rather than the groove. 9 The current study sought to determine if this discrepancy is clinically relevant and whether there is a need to introduce finger positioning recommendations.
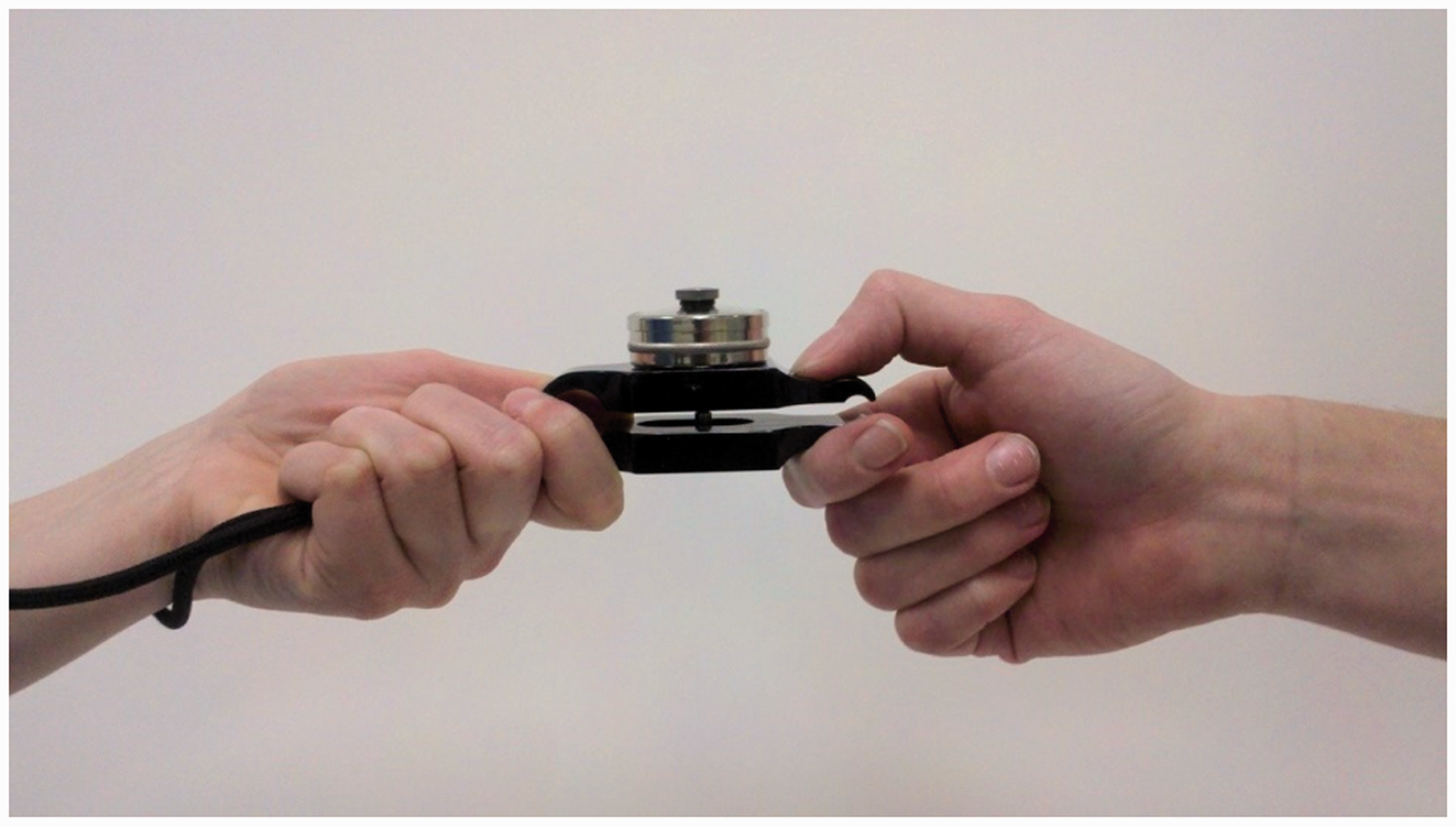
Lateral pinch on the groove of a B&L Engineering pinch gauge.
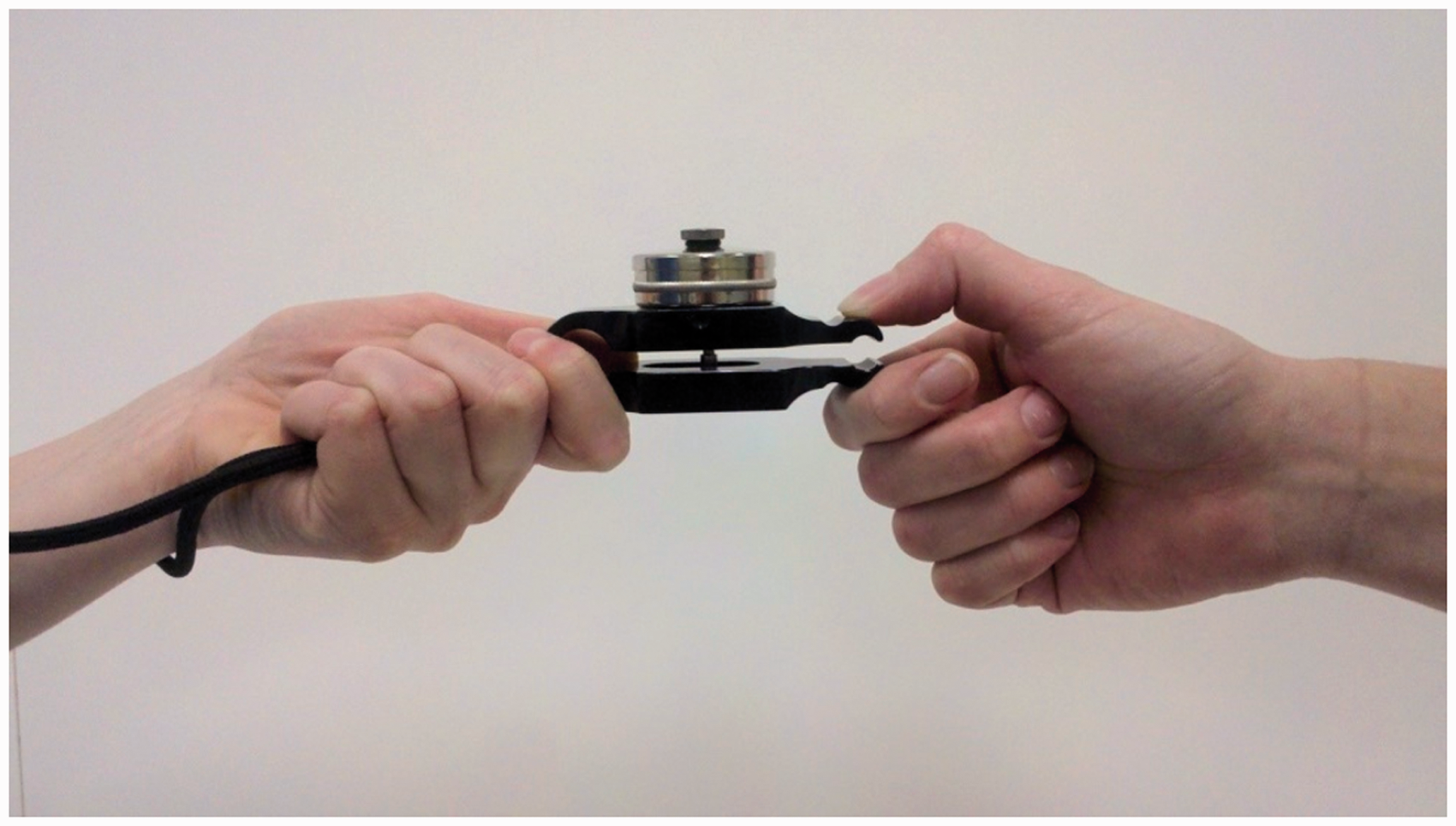
Lateral pinch on the bridge of a B&L Engineering pinch gauge.
The aim of the present study was to demonstrate whether finger position impacts three common pinch strengths using a B&L Engineering pinch gauge. Further, it was intended that this research adds to the existing literature of normative studies demonstrating the need for industry standardization of positioning with a pinch gauge during assessment. The hypothesis was that there is no significant difference in lateral, tip, and three-jaw-chuck pinch strength when measured with fingers placed on the bridge or groove of a B&L Engineering pinch gauge.
Methods
Study design
This study utilized a crossover design with randomization of exposure to bridge versus groove positioning. The researchers sought to determine how this finger positioning on the pinch gauge affected the participants’ tip, lateral, and three-jaw-chuck pinch strength.
Participants
A power analysis was conducted using G*Power 3.1.9.2 based on a two-tailed paired t-test. To detect a moderate effect at a 5% significance level with 80% power, it was determined that a sample size of at least 34 would be needed. 15 Thirty-six participants were recruited to better correspond to the order randomization scheme described below. Study participants were volunteers recruited from Grand Valley State University University’s (GVSU) student body, faculty, and guests using posters and faculty’s verbal announcements. The study included 36 healthy adults (9 males, 27 females), aged 19–49. Of these participants, 33 were right hand dominant and three were left hand dominant. Exclusion criteria included neurological or other disorders of one or both upper extremities, a history of upper extremity surgery or impairment within the last 12 months, and inability to follow English commands.
Equipment
The 0–30 pound B&L Engineering pinch gauge with one pound increments was utilized in this study. This instrument was chosen because it has high test–retest reliability, very high inter-rater reliability, demonstrated validity, and is known as the “gold standard” for pinch strength assessment. 5 The one B&L pinch gauge that was used in this study was newly purchased, calibrated by the manufacturer, and not used prior to data collection.
Procedures
This study was submitted to the GVSU Human Research Review Committee. After approval, this study was performed at the Cook DeVos Center for Health Sciences (CHS) in Grand Rapids, Michigan. On the day of testing, the researchers verbally explained the research procedures and written information detailing potential risks and benefits was given to each participant. The participants were blinded to the research hypothesis. The order of pinch was randomly assigned among participants with each order combination being represented equally. This was done to eliminate any potential order or fatigue effects. Prior to data collection, the researchers listed order combinations on demographic forms. Order combinations included pinch type (tip, lateral, and three-jaw-chuck) and starting finger position (bridge or groove). Thus, there were 12 possible order combinations, and since there were 36 participants, each pinch combination was written on 36 different demographic forms. After equally distributing orders onto the demographic forms, the forms were physically shuffled for randomization, so that on the day of testing, each participant was simply given the next demographic form in the pile. Each participant pinched the gauge a total of six times; once on the bridge and once on the groove for each type of pinch. Using one trial as the outcome score was selected to limit fatigue because research has shown no significant difference in pinch strength measurements when the mean of three trials, best of three trials, and one trial have been used to collect data.3,9,16
Patients were instructed to be seated with shoulder adducted and neutrally rotated, elbow flexed at 90°, and the forearm and wrist in neutral position, according to the guidelines by ASHT. 7 Literature also suggests no significant difference in pinch strength when the wrist is extended up to 30° and hence slight variations in wrist position up to 30° extension were permissible. 17 Additionally, the ulnar fingers and the IP joint of the thumb were flexed during the pinch measurement because research suggests these positions result in greater pinch force.11,13 This testing position was visually estimated, and then maintained throughout the testing process with verbal feedback from the researchers. One trained rater performed the pinch strength testing and verbally verified the measurement. A second researcher provided the information sheet to participants, and a third researcher monitored the testing position as well as recorded the data. Each participant then was given one submaximal pinch warm-up in the first pinch position that was randomly assigned because this type of warm-up has been found to result in increased strength measurements. 18 Participants were given 15-s rest breaks between position changes, which was determined to be adequate by Trossman and Li. 19 Pinch measurements were taken with the dominant hand only because research has found a correlation between ability to complete activities of daily living and pinch strength for the dominant hand only. 20 The rater encouraged the participant to squeeze as hard as possible during each trial by saying “go, go, go, stop,” as the use of consistent instructions is important for standardization of the test protocol. 21 This contraction time was no more than 3 seconds, which is supported by Smith and Lukens. 22
Data analysis
Pounds of force used during maximum pinch were gathered from the B&L Engineering pinch gauge. Data provided from all 36 participants were analyzed. Researchers entered data into Statistical Package for the Social Sciences version 20 and utilized the parametric paired t-test or the non-parametric Wilcoxon signed ranks test to analyze the data for each pinch type. The Shapiro-Wilk test of normality was used along with histograms and boxplots to determine the appropriate test. The parametric paired t-test was deemed appropriate to apply to the lateral and tip pinch data. For three-jaw-chuck pinch, all assumptions for the parametric paired t-test were not met. Since both the skewness (2.34) and kurtosis (1.97) coefficients were not between −1.96 and 1.96, the normality assumption was questioned, and the Wilcoxon signed ranks test was completed. An alpha level of 0.05 was used to determine significance. Additionally, equivalence intervals were used to demonstrate a lack of substantial difference between measurements taken on the bridge or groove. A substantial difference was defined as one-unit (one pound) difference between measurements taken on the groove or bridge, giving an equivalence interval of (−1,1). One pound was chosen because it is the smallest unit of measurement that can be read on the pinch gauge.
Results
Table 1 depicts mean strengths and standard deviations for each type of pinch and finger position on the gauge and the results of statistical analysis. There was no significant effect of finger position (p = 0.51) for lateral pinch. The 95% confidence interval for the difference in mean pinch strength between bridge and groove was (−0.90, 0.46); therefore, equivalence was found within one pound for lateral pinch. There was no significant effect of finger position (p = 0.059) for three-jaw-chuck pinch, which was observed to be slightly higher on average with fingers on the groove. The 95% confidence interval for the difference in mean pinch strength between bridge and groove was (−1.57, 0.12), which does not demonstrate equivalence for three-jaw-chuck pinch. There was no significant effect of finger position (p = 0.656) for tip pinch. The 95% confidence interval for the difference in mean pinch strength between bridge and groove was (−0.59, 0.92); therefore, equivalence was found within one pound for tip pinch.
Mean pinch strength and p-values of statistical analysis.

Note: Measurements in pounds.
TJC: three-jaw-chuck; WSR: Wilcoxon Signed Ranks.
The researchers considered the possible effects of hand dominance and gender on pinch strength in this study. Results were not found to be statistically significant (p = 0.703, p = 0.507, and p = 0.110, respectively) for tip, lateral, and three-jaw chuck pinches based on hand dominance. In addition to hand dominance, the researchers addressed differences of finger position based on gender. Results of paired t-tests comparing bridge and groove measurements from only male participants did not prove to be significant for tip, lateral, or three-jaw-chuck pinches (p = 0.165, p = 0.154, and p = 0.360, respectively). P-values for tip (0.473), lateral (1.00), and three-jaw-chuck pinches (0.159) were also not significant at the alpha level (<0.05) when data from only females were used to determine differences in bridge and groove measurements.
Discussion
No statistically significant differences in mean pinch strength were found between bridge and groove digit placement for any of the three pinch types. Additionally, equivalence was found within one pound for tip and lateral pinch, but not for three-jaw-chuck. Distinct from wrist position, forearm position, thumb IP position, and ulnar finger position, pinching on the bridge or groove may result in a similar tip pinch strength measurement on a B&L Engineering pinch gauge for tip and lateral pinch.8,9,11,13
The present study results are influential because they reveal that the discrepancy between calibration measurement and clinical measurement is not significant, implying that inter-rater reliability is not compromised. Practitioners may reliably assess lateral and tip pinch using either finger position. Clinicians may have increased confidence that measurements will be accurate regardless of whether they, or other healthcare personnel, guide clients to place fingers on the bridge or groove of the pinch gauge. Such information informs clinical practice by indicating that B&L Engineering’s recommendation to use a conversion factor of 0.9 may not be necessary when using the bridge instead of the groove. 9 Because finger position does not appear to impact pinch strength, perhaps the standard positioning on the bridge or groove could be determined by additional factors such as ease of positioning or patients’ preference for comfort. For instance, supporting the finding that positioning on the bridge is found to be easier to accomplish clinically, this study's participants informally reported that positioning on the bridge was also more comfortable. 9 A recommendation of the study is that results should guide clinicians to adopt their own standardized approach to pinch strength assessment, using either a pinch bridge or groove protocol consistently.
There were several limitations to this study. A small convenience sample of predominantly female volunteers from Grand Rapids, Michigan compromises generalizability and statistical power of findings. The three-jaw-chuck measurements did not satisfy the normality assumption for a paired t-test, and hence the Wilcoxon signed ranks test was used, which typically has less statistical power. A larger sample size could have also impacted on statistical significance. The research hypothesis was that we would not find a significant difference in lateral, tip, and three-jaw-chuck pinch strength between measurements with fingers placed on the bridge or groove of the gauge. Because of this, it would have been desirable to perform the power analysis based on a small, as opposed to moderate, effect size. Unfortunately, the necessary sample size for detecting a small effect (n = 199) was not feasible within the time and budget constraints of the study. It is also noted that the participant sample included more women than men. While the researchers would have preferred to collect data on a balanced sample of men and women, this was not available the day of testing. Despite this discrepancy, women did not exhibit significantly different pinch strengths between bridge and groove than men did. The rater was also not blinded to the research hypothesis, which could have consciously or unconsciously resulted in biased outcomes or reporting of outcomes. Although the researchers utilized the same new B&L pinch gauge for the study, the researchers did not verify the calibration of this pinch gauge directly prior to data collection. According to Fess, this can result in more than acceptable measurement error, and the researchers caution that results may not generalize to pinch gauges other than the B&L. 23 Additionally, we chose to visually estimate upper extremity positioning during the procedure rather than to record goniometric measurements or provide stabilization.
Future research should address the limitations of this study and focus on conducting similar normative studies using varied populations and a larger sample size balanced of men and women. Other pertinent populations include those with hand impairment or disability as well as older adults. These populations are relevant based on the findings in the literature which suggest that the relationship between hand strength and functional activities changes with these variables.24–27 In future studies, a qualitative component involving the participants’ perceptions of pinching on the bridge or groove may aid in understanding the effect of this variable on pinch strength measurements or lack thereof.
Conclusions
Although standardization of finger position is ideal and recommended, variations in finger position between the bridge and groove of the B&L Engineering pinch gauge may result in similar pinch strength measurements. We do recommend a standardized test position be established and that all research and clinical documentation include a description of the testing position. Further research on this topic is needed to support the findings from this study, especially with regard to the impact of finger position on three-jaw-chuck pinch strength since equivalence was not established.
Footnotes
Acknowledgements
The researchers would like to thank Barb Hoogenboom, PT, Ed.D, ATC, SCS, for overseeing the study at each phase and sharing her expertise regarding inter-rater reliability. Additionally, the researchers would like to extend a special thanks to Claudia Leiras-Laubach, PhD, for her assistance in creating an informational sheet for the participants of the study, and Lee Barnes, for providing us with valuable information concerning the calibration of the B&L Engineering pinch gauge.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from all subjects before the study.
Ethical approval
Ethical approval for this study was obtained from Grand Valley State University Human Research Review Committee.
Guarantor
KW.
Contributorship
KW, JP, RB, and JB researched literature, conceived the study, gained ethical approval, developed protocol, and drafted the first draft. KA was instrumental in data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.