
Abstract
Introduction
In recent years, three-dimensional (3D) printing has emerged as a new manufacturing technique for orthoses, showing comparable stability and wearing comfort to traditional orthoses. However, the lengthy designing and printing process is assumed to take more time than the common practice of manufacturing low-temperature thermoplastic orthoses (LTTOs). The aim of this prospective cross-sectional study was to compare the production time of 3D-printed orthoses (3DPO) to LTTOs.
Methods
The active and passive time needed to manufacture the orthoses was measured in a clinical setting. 17 orthoses (8 3DPOs and 9 LTTOs) were included in the data analysis.
Results
The mean total production time of a 3DPO (12:14:50h total time; 0:44:35h active production time) was significantly longer than in LTTOs (0:14:14h; p < 0.001).
Discussion
The longer production time might be a hurdle regarding the implementation of 3DPOs in hand therapy. Although 3D-printing might become more cost- and time-efficient due to future developments in technology and growing experience, some practical advantages of LTTOs prevail, such as the fast and efficient provision of orthoses and the adaptability of the material if subsequent changes are needed. A combination of both manufacturing techniques may be a feasible solution to provide patient-centred orthosis provision in future hand therapy practice.
Introduction
The use of custom fabricated orthoses is common in the treatment of injuries and conditions of the upper extremity. Orthoses are traditionally made using different types of materials such as low-temperature thermoplastics (LTT), fiberglass, or plaster, depending on the condition or injury to be treated, the patient’s needs, and the experience or preference of the health care provider (HCP).1,2 The accurate fit of an orthosis is deemed of utmost importance to ensure the appropriate immobilisation and protection of the affected parts, while allowing the best possible hand function for the patients to carry out their everyday activities. 3 Good patient satisfaction regarding comfort, aesthetics and convenience of usage is believed to improve the patient’s adherence to the prescribed immobilisation regime, therefore leading to faster rehabilitation and fewer complications. 4
In recent years, three-dimensional (3D)-printing has emerged as a new manufacturing technique for patient-specific or custom fitted orthoses.1,5,6 Although the stability and wearing comfort has been established as comparable to conventional orthoses,7–9 the widespread implementation of 3D-printing in everyday hand therapy practice has not yet been achieved. 10 In a feasibility study evaluating the designing process of 3D-printed orthoses (3DPOs), the costs and practicability of 3D-printing have been identified as a significant concern of participating therapists. 11 The lengthy designing and printing process is assumed to take more time and to be less straightforward than the commonly used manufacturing of low-temperature thermoplastic orthoses (LTTOs). 11 However, only a few studies report the production time of 3DPOs in detail.12,13 Although the time issues are very dependent on the printing technique and materials used, more information is needed in order to provide the evidence base necessary to promote the integration of 3DPOs in hand therapy practice. 14
The aim of this study, therefore, was to analyse and compare the production time of the manufacturing process of 3-dimensionally printed wrist orthoses by Digital Light Processing (DLP) of unpolymerized photosensitive resin, compared to low-temperature thermoplastic wrist orthoses in a clinical setting, and to discuss practicability issues and their potential impacts on future hand therapy practice.
Methods
A prospective, cross-sectional analysis of the production time of 3DPOs compared to LTTOs was performed in a clinical setting, aiming to compare the expenditure of time needed for the manufacturing of the orthoses from a healthcare provider perspective.
Sample
A convenience sample of consecutively referred palmar wrist orthoses was collected, regardless of the underlying diagnosis and duration of wear, as the study focused solely on the manufacturing process of the orthosis itself, excluding all additional treatment (such as change of dressing, patient education, exercise therapy, etc.). Inclusion criteria were referral for palmar wrist orthoses fabricated either out of low-temperature thermoplastic material (Klarity KS 3.2 mm; Klarity Medical & Equipment Co. Ltd, Guangdong, China), or by 3D-printing (DLP-technique). Circular (dorso-volar) wrist orthoses, as well as orthoses fabricated for patients under the age of 18, were excluded to ensure comparability of the results.
Fabrication process of the orthoses
Following the routine treatment pathway, both LTTOs and 3DPOs were provided by the therapists of the hand therapy department after referral from the attending hand surgeon. The type of orthosis to be manufactured by the therapists was discussed and determined depending on the individual’s needs and preferences. Factors influencing the decision included the duration of wear or the patient’s activities. For example, in a long-term chronic illness, a 3DPO might be chosen over a LTTO due to the easy file storage and reproducibility of the orthosis, especially if the patient was using the orthosis for activities including water contact and risk of soiling. Conversely, in an acute injury, a LTTO might be preferred due to the easier subsequent adaptations to changes in swelling or wound dressings.
The manufacturing of both orthosis types was done by graduated occupational therapists and/or certified hand therapists, with experience in the manufacturing of LTTOs varying between 2 and 14 years, and approximately 6 months experience in the fabrication of 3DPOs since its implementation in the hand therapy department.
3D-printing
To manufacture a 3DPO, the patient’s affected limb was scanned during a first therapy appointment using an optical structure sensor (Mark I Structure Sensor®, Occipital Inc. TM, Boulder, Colorado, USA) rigged on a tablet (Apple iPad® 6th generation Apple Inc. TM, Cupertino, California, USA) (Figure 1(a)). In absence of the patient, the scan was then uploaded to a purpose-built and European Conformity (CE)-marked application (Spentys© Point-of-Care Solution®, Spentys SA/NVTM, Brussels, Belgium), and the orthosis was designed on the tablet using semi-automated modelling (“Autoformat”), allowing to automatically fit the chosen orthosis design onto the scanned model (Figure 1(b)). After converting the orthosis model into a Stereolithography Tesselation Language (STL)-file, it was exported into the 3D-printer’s software (atum3D®, atum3DTM, Gouda, The Netherlands) and the printing settings (material, printing speed, position of model on printing platform) were defined. The orthosis was then printed using a DLP technique with unpolymerized photosensitive resin (BASF Ultracur3D, ST45 B, black) on a local printer (atum3D DLP Station 5-405; atum3D, Gouda, The Netherlands) (Figure 1(c)). Manufacturing of a 3D-printed orthosis: (a) Scanning of the arm, (b) designing, (c) 3D-printing, and (d) fitting.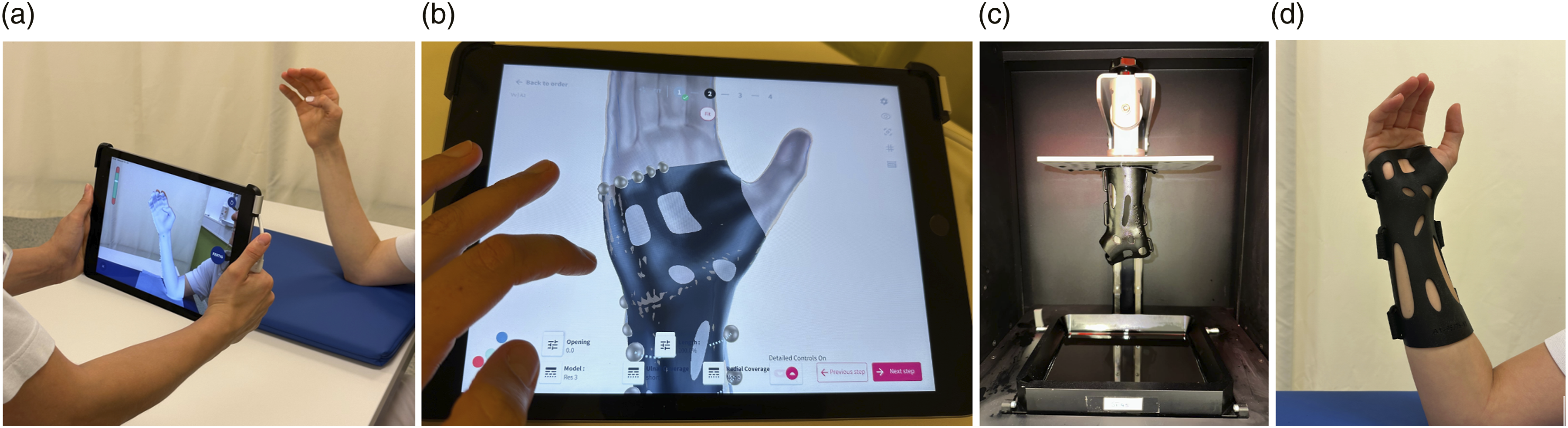
Once the orthosis was printed, it was manually wiped clean with ethanol, and then cured in a curing station using UV-light and vacuum (atum3D Curing Station; atum3D, Gouda, The Netherlands). After the structural supports were removed and the edges smoothed with sandpaper, the orthosis was fitted to the patient during a second appointment, adding the Velcro straps (Figure 1(d)).
Low-temperature thermoplastics
An LTTO was fitted during a single therapy session. First, a pattern of the orthosis based on the patient’s arm was drawn on a piece of plastic, foil or paper (Figure 2(a)) and transferred on a thermoplastic sheet (Klarity KS 3.2 mm, Klarity Medical & Equipment Co. Ltd, Guangdong, China). The thermoplastic material was heated and softened for a few minutes in a water bath (WDB 6-100/4; Heuser Apparatebau GmbH, Haan, Germany) at a temperature of 70°C and adjusted to the patient’s arm (Figure 2(b)). Once the material was sufficiently cooled and hardened, the orthosis was removed, overlaps cut down, and small corrections done using a heat gun (HL 1920 E, Steinel GmbH, Herzebrock-Clarholz, Germany). The straps were fitted using adhesive Velcro hook on the orthosis and Velcro loop on the dorsal side of the arm during the final fitting of the orthosis (Figure 2(c)). Manufacturing of a thermoplastic orthosis: (a) Pattern drawing, (b) modelling, and (c) fitting.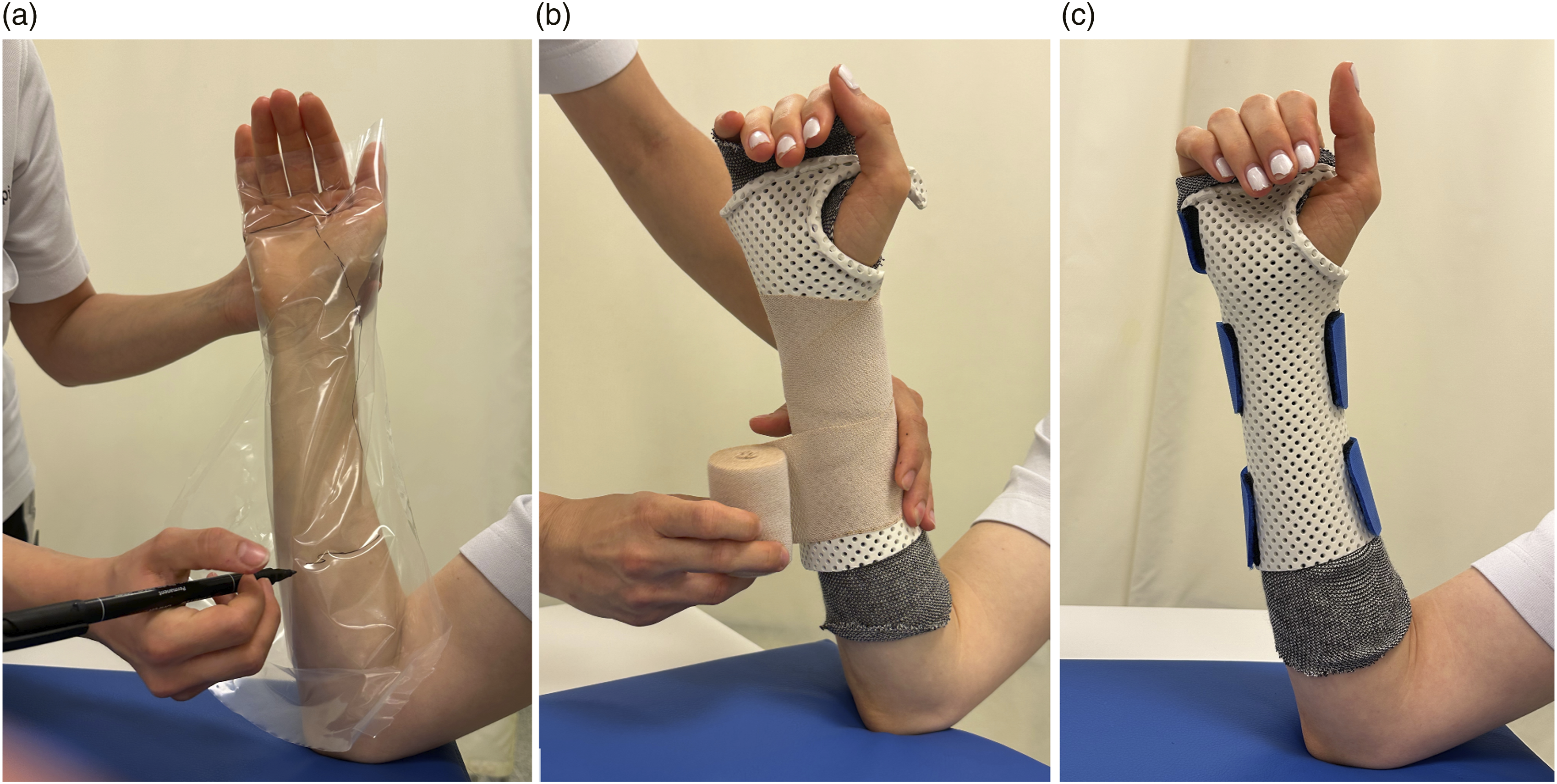
Data collection
During a 12-week period between March and June 2023, the time needed in the fabrication process of referred wrist orthoses was recorded by the therapists of the hand therapy department manufacturing the orthoses. The therapists participating in the evaluation were briefed beforehand on the measurements to be taken, based on the provided data collection sheet. The time needed for each step of the manufacturing process was measured using an electronic time clock. At the beginning of each step, the therapist started the time clock, and wrote down the time needed after its completion. The different steps are detailed in Figure 3. Orthosis manufacturing steps: The patient needs to be present for the highlighted steps. LTTO = Low-Temperature Thermoplastic Orthosis; 3DPO = 3D-Printed Orthosis.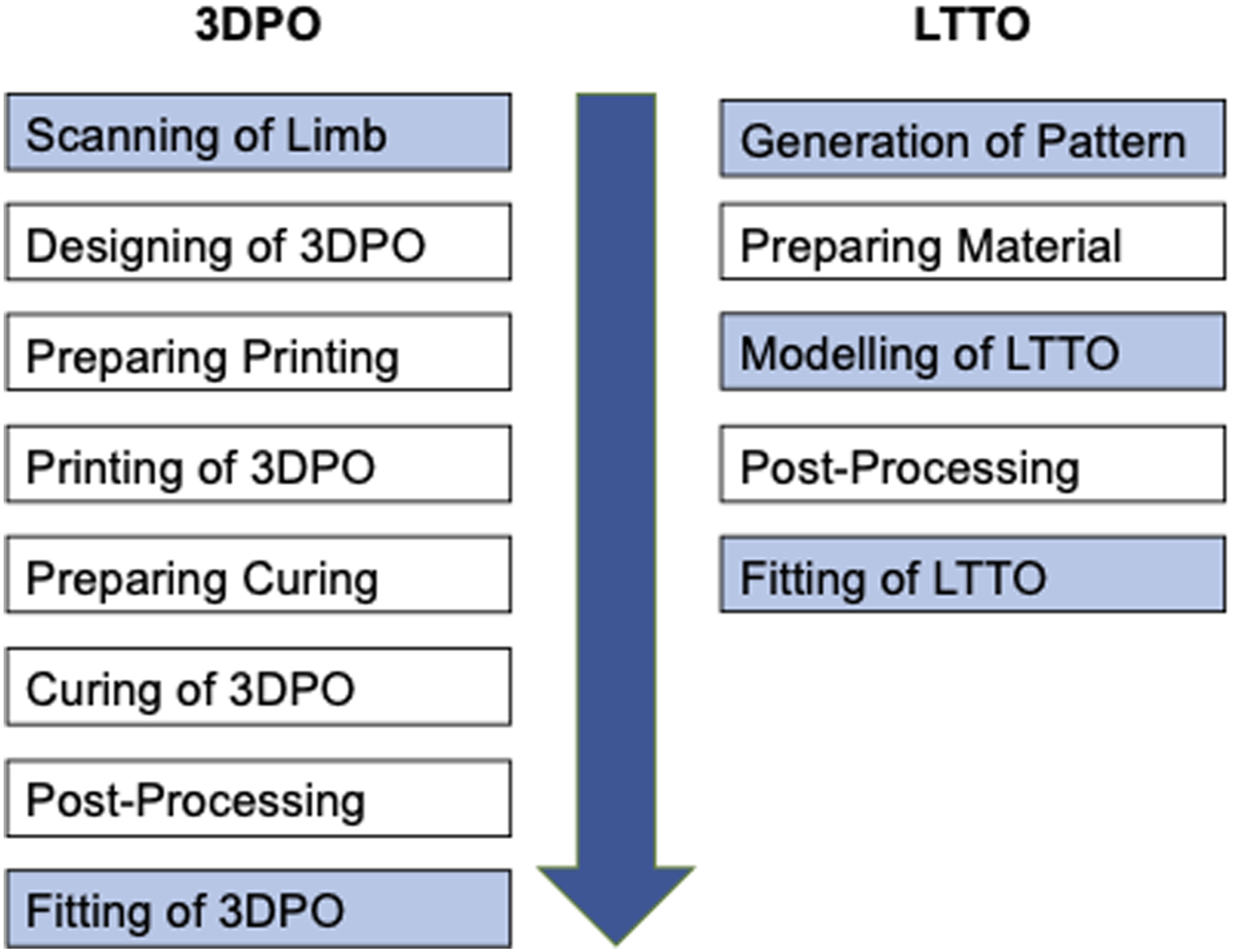
Statistical analysis
For the testing of the null hypothesis, stating that there is no difference in the time needed for manufacturing of 3DPOs and LTTOs, the fabrication time was summarised with descriptive statistics for numerical data. Due to the non-parametric distribution (as confirmed by Shapiro-Wilk test (0.707); p < 0.01), the Mann-Whitney U test was applied for the comparison of the means of two independent groups. 15 The statistical analyses were performed using SPSS statistics for Mac, version 27 (IBM Corp., Armonk, NY, USA).
Results
During the 12 weeks of data collection, 21 palmar wrist orthoses were referred to the hand therapy department, of which 17 were included in the data analysis. Reasons for dropout were incomplete data collection in 3 cases, and one patient below the minimum age criteria. Therefore, the data of 8 3DPOs and 9 LTTOs were analysed.
The mean total production time of a 3DPO (12:14:50h) was statistically significantly longer than for an LTTO (0:14:14h; p < 0.001). When looking at the active production time only (excluding the printing and curing times), the LTTOs still took significantly less time (0:14:14 h) than the 3DPOs (0:44:35 h; p < 0.001).
Average time needed for fabrication steps (in h:min:sec).
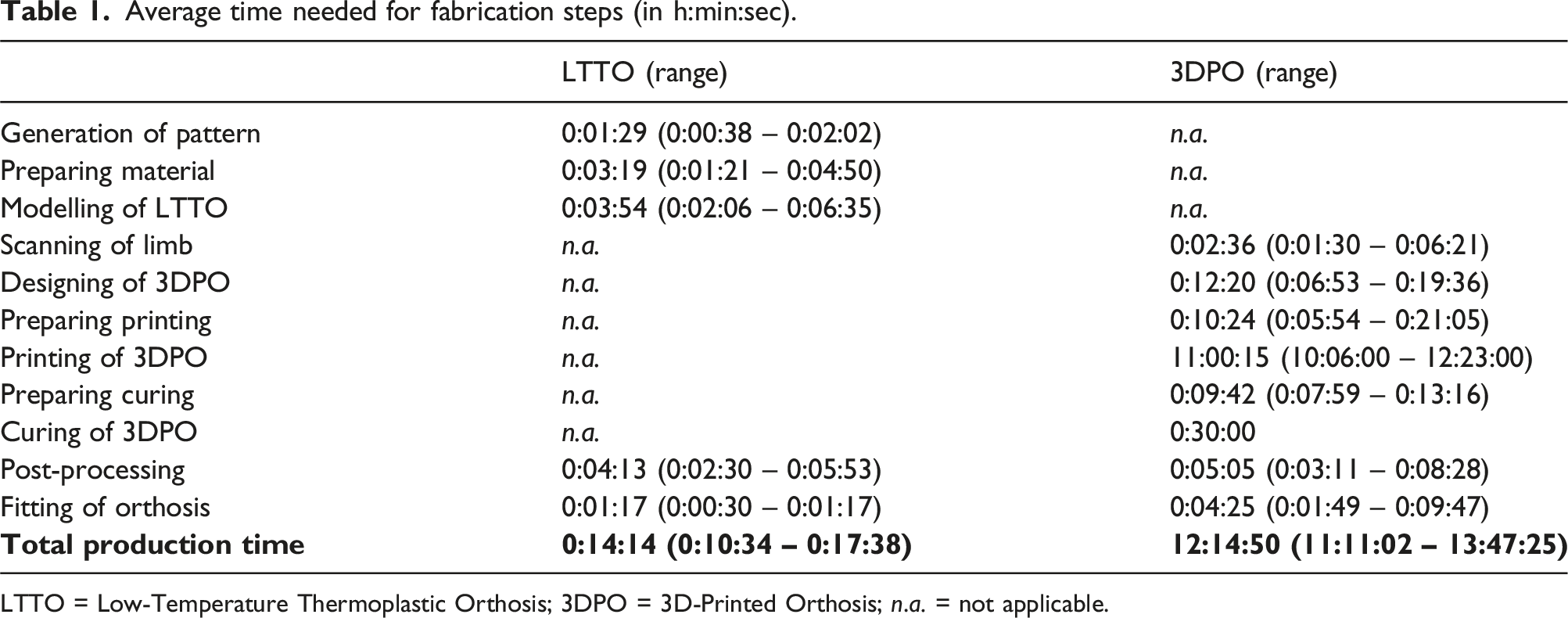
LTTO = Low-Temperature Thermoplastic Orthosis; 3DPO = 3D-Printed Orthosis; n.a. = not applicable.
Discussion
Printing technique
The results of this study show that while an LTTO could be manufactured within one therapy session, taking approximately 15 min, the total production time of a 3DPO took over 12 h, thus requiring two separate appointments. However, the printing technique and material used highly influences the time needed for the manufacturing of a 3DPO, especially the passive production time (comprising all steps during which the therapist does not take an active role, namely the printing and curing time of the 3DPO). In DLP, the printing time is dependent on the size of the orthosis, as the resin is hardened layer by layer, thus the length defines the duration of printing. The width of the orthosis, in contrast, is irrelevant, as all points of one layer are polymerised at once. Therefore, multiple orthoses could be fitted on the same building platform without prolonging the printing time, which might be one way to increase the productivity of the printer and reduce costs. 16 This represents one advantage of the DLP compared to other techniques such as Fused Deposition Modelling (FDM), where only one object can be printed at a time, or rather the printing time is increased according to the number of objects.
The black resin used in this study takes significantly more time to polymerise than lighter colours, as the light is absorbed more readily, thus doesn’t transmit through the material as quickly. 17 For instance, in the randomised controlled trial by Gübeli et al., 16 the printing of a three-quarter circumferential wrist orthosis using the same DLP-printer, but using a light green resin, took only 60-90 min, thus reducing the printing time by approximately 85%. However, the experience before the start of the study showed that a majority of patients wished for a darker colour, leading to the routine use of black resin in the hand therapy department, as aesthetics are considered an important factor for the adherence of patients to an orthosis wearing regime. 4 The colour of the resin was therefore not changed for the purpose of this study, as the aim was to represent the routine pathway in place, without any changes to practice.
Designing of the orthosis
In the current study, all patients in both groups were able to actively maintain the requested position during the manufacturing of the orthosis (LTTOs) or scanning of the affected limb (3DPOs). However, if this had not been possible, in LTTOs, the position of the limb can be corrected during the modelling by applying some targeted pressure where needed, and by holding the patient’s arm while the material hardens. Nevertheless, caution is required in order not to cause sores and skin irritation through misplaced or excessive pressure. 2 Conversely, when scanning a limb for a 3DPO, a support structure or someone holding the hand could interfere with the 3D-model. 18 The generation of a 3D-model of the patient’s limb is a crucial part of the manufacturing of 3DPOs, as the design and fitting of the orthosis are based on its accuracy.1,11 This is especially challenging when an orthosis is provided to correct a deformity, as might be the case in subluxated joints (e.g. first carpo-metacarpal joint osteoarthritis) or spasticity. One possibility to overcome this problem is to scan the healthy contralateral limb, and to invert the 3D-model before designing the orthosis.8,19 Some designing software include this option in their application, enabling to save time in the scanning and designing process. However, this is only feasible if the volume of both limbs is comparable (e.g. absence of swelling or atrophy), and the contralateral limb can be controlled willfully.
Similarly, in case of patients experiencing severe hypersensitivity or allodynia, one further advantage of 3DPOs is the possibility to fabricate the orthosis without touching the patient, which might avoid additional pain provocation.5,20
The recording and analysis of the reasoning and the decision-making process regarding the provision of LTTOs versus 3DPOs has not been recorded in this study, however it might have given further insight in perceived advantages and disadvantages of the different types of orthoses and should therefore be considered in future research.
The designing and preparing of the printing-file of the 3DPO was the most time-demanding, amounting to 51% of the total active production time, which is in line with the results of the feasibility study by Waldburger et al., 21 where the 3DPO designing accounted for 55% in their comparison of thermoplastic and 3D-printed orthoses. The semi-automated design process used in the current study facilitates the designing process, as the orthosis model can be selected on the design-application and is automatically fitted around the previously scanned limb. The therapist then only needs to adjust the openings, trim the edges if necessary, and add the required fastening solution. This significantly speeds up the process compared to manually designing the orthosis using a CAD-software (computer aided design), as was done in other studies.13,20,22
Training of therapists
One factor influencing the time needed for designing an orthosis is the training and experience of the therapist, including the knowledge about anatomical landmarks and typical sensitive areas. 1 Nevertheless, while manual skills are needed in the traditional fabrication of orthoses, which is a part of the basic training of a hand therapists, the provision of 3DPOs demands very different skills, which are computer-related, and include the operating of the scanner, digital drawing and CAD utilisation skills, as well as knowledge and understanding regarding 3D-printing technology.13,23 Many of these skills are not (yet) part of a hand therapist’s training. Still, in a study comparing the satisfaction of occupational therapy students manufacturing 3D-printed versus LTT finger orthoses, a higher satisfaction regarding the fit, aesthetics and manufacturing process was reported in 3D-printed orthoses. 12 Therefore, the cutback of manual steps when printing an orthosis reduces the dependency on the abilities of the manufacturer, 22 while still producing precise and well-fitting orthoses. 24 It would even be possible to outsource the designing of the orthosis to a professional designer by sending on the scan of the affected limb,10,16 which might be timesaving and effective in settings where hand therapists are not always available.
Practicability
The fabrication of 3DPO is dependent on the availability of the infrastructure (e.g. scanner and printer), software, material, and the corresponding knowledge of HCPs. 6 This might have impeded the use of this technology in daily practice so far, as the investment needed to implement 3D-printing is considerable. 10
While the “coolness factor” of 3DPOs seems to have the potential to increase patient adherence to the wearing regime of orthoses,3–5 which might lead to faster and better rehabilitation outcomes, the advantages of LTTOs should not be discarded. The quick and immediate modelling of orthoses and the adjustability of the material are a key factor in acute hand therapy settings. 1 Even if the printing time of 3DPOs could be considerably accelerated through the use of different materials or the evolution of technology, the limited possibility of adaptation to the changing volume of the limb (e.g. through swelling or dressings) is a major detriment of the 3D-printing so far,1,5,21 especially in the provision of orthoses in an acute setting. In the provision of orthoses for extended use and chronic conditions, however, 3D-printing might be a valid option due to the storage of the printing file leading to easy reproducibility of the orthoses. 23
Limitations
Some limitations of the present study need to be taken into consideration.
Firstly, a convenience sample was used, including all diagnoses and wearing regimes, as they were assumed not to directly influence the manufacturing process of the orthosis. However, the time needed to model a LTTO on a patient with a very painful wrist or not understanding instructions might take longer than in a pain-free, accommodating patient. Nevertheless, the inclusion criteria were consciously not narrowed down, as these occurrences are an accurate reflection of daily practice.
Secondly, although all therapists were trained at the same time with equal opportunities to provide patients with 3DPOs, some did assemble more experience due to the allocation of patients, and possibly greater curiosity and interest in the new technology. This might account for the variances in the total production time of 3DPOs. As stated by Waldburger et al., 21 the learning curve in the designing of 3DPOs is steep, and a longer experience in the manufacturing of 3DPOs might accelerate the active production process. Nevertheless, these differences reflect the reality of hand therapy practice, and allow for the transferability of the results into other settings.
Thirdly, the use of black resin, which takes significantly longer to print than a lighter colour, influences the total production time of the 3DPOs. Yet, the active production time, which is a main factor for therapists in the clinical setting and in relation to the HCP perspective used in this study, is not affected by the choice of colour.
Lastly, some risk of measurement bias is present, as the data collection was performed by the treating therapists. The fact that the time was measured during the manufacturing of an orthosis might have influenced the working speed of the therapist. However, as this was the case in both groups, the validity and transferability of the results is likely not be affected.
Conclusion and impact on future practice
The production time of 3DPOs manufactured by DLP is significantly longer than that of LTTOs. As the 3D-printing technologies are diverse, cost-effectiveness analyses of different printing methods might lead to new insights.
Both manufacturing techniques of 3DPOs and LTTOs show some practical assets and drawbacks, however, further research is needed to evaluate the advantages of 3DPOs and LTTOs in hand therapy practice, with both an economic and clinical focus. In particular, the views and experiences of hand therapists as experts in the manufacturing of upper extremity orthoses need to be taken into consideration.10,11
In the field of hand therapy, 3D-printing is emerging not only in the manufacturing of orthoses, but also in the printing and individual production and adaptation of auxiliary equipments. 25 The inclusion of these techniques in the future education of hand therapists therefore seems likely and sensible.
The factors influencing the performance and success of an orthosis application are numerous, including the wearing comfort, the aesthetics, the patient’s acceptance, the convenience of usage, the durability of the material, and side effects such as sweating or pressure sores.4,26 The possibility to offer both 3DPOs and LTTOs in the hand therapy department has the potential to enrich hand therapy practice and allows for a new level of patient-centred orthosis provision.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MvH.
Contributorship
MvH researched literature and conceived and conducted the study, including data analysis, and wrote the first draft of the manuscript. LC was involved in protocol development. All authors reviewed and edited the manuscript and approved the final version of the manuscript.