
Abstract
Background:
Fibromyalgia (FM) is a chronic pain syndrome characterized by widespread musculoskeletal pain, fatigue, sleep disturbance, and cognitive dysfunction. Alexithymia—difficulty identifying and describing emotions—has been reported in up to 48% of FM patients and is associated with increased psychological distress and pain intensity, yet its specific contribution to FM remains unclear.
Objectives:
This study aimed to assess the interplay among alexithymia, self-compassion, pain catastrophizing, and hope to inform future integrated and emotion-focused treatment strategies for FM.
Design:
We conducted a cross-sectional investigation, consecutively recruiting 112 Caucasian women meeting the 2016 American College of Rheumatology criteria for FM between October 2023 and June 2024.
Methods:
Socio-demographic, clinical, and psychometric data were collected at baseline. Disease burden was evaluated using the Widespread Pain Index, Symptom Severity Scale (SSS), Polysymptomatic Distress Scale, modified Fibromyalgia Assessment Scale, and revised Fibromyalgia Impact Questionnaire (FIQ-R). Psychological constructs were assessed using the Toronto Alexithymia Scale (TAS-20), Adult Hope Scale, Hospital Anxiety and Depression Scale (HADS), Pain Catastrophizing Scale (PCS), and Self-Compassion Scale (SCS). Participants were stratified into non-alexithymic, borderline, and alexithymic groups according to TAS-20 thresholds. Group differences were analyzed through χ2 or Kruskal–Wallis tests, and associations were examined using univariable and multivariable linear regression models (α = 0.05).
Results:
Alexithymic traits were identified in 51.8% of patients. Individuals with alexithymia exhibited significantly higher anxiety, depression, and total HADS scores (all p < 0.01), greater pain catastrophizing (p = 0.003), and lower levels of hope (p < 0.05). Two self-compassion components, self-judgment and overidentification, were also significantly impaired (p = 0.012). Univariable analyses showed that alexithymia was positively associated with FM severity indices (SSS, FIQ-R) and psychological distress and negatively associated with hope and several self-compassion domains (all p < 0.001). In multivariable models, SSS (p < 0.001), PCS-Helplessness (p = 0.005), and SCS-Overidentification (p = 0.020) emerged as significant independent associated variables.
Conclusion:
Alexithymia represents a prominent marker of emotional vulnerability in FM, closely linked to symptom severity, maladaptive pain coping, and reduced hope and self-compassion. Integrating these constructs into FM assessment and management may support more comprehensive, emotion-focused therapeutic approaches.
Plain language summary
Fibromyalgia (FM) is a long-lasting condition that causes widespread pain, fatigue, sleep problems, and other symptoms that strongly affect daily life. Many people with FM also struggle to recognize, understand, or express their emotions. This difficulty, known as alexithymia, may make it harder to cope with pain and stress, but its specific impact in FM is still not fully understood. In this study, we evaluated 112 Caucasian women diagnosed with FM to explore how alexithymia relates to disease burden and key psychological factors: hope, self-compassion, and pain catastrophizing (a pattern of negative thoughts about pain). All participants completed questionnaires measuring symptom severity and emotional well-being. Over half of the women in the study showed signs of alexithymia. Compared to those without alexithymia, these patients reported higher levels of anxiety and depression, more catastrophic thinking about pain, and lower levels of hope and self-compassion. They also tended to experience more severe fibromyalgia symptoms, particularly fatigue, sleep problems, and overall distress. When we analysed the data in detail, three factors were strongly linked to higher levels of alexithymia:
1. Greater symptom severity,
2. A stronger sense of helplessness toward pain, and
3. A tendency to become overwhelmed by negative experiences, reflected by low scores in the self-compassion domain of overidentification.
These findings suggest that emotional difficulties are deeply intertwined with the experience of fibromyalgia. Addressing alexithymia and related psychological factors may help clinicians better understand patient needs and deliver more personalized care. Treatments that support emotional awareness, coping strategies, and self-compassion—such as mindfulness-based approaches—may be particularly helpful for individuals who struggle with these aspects. Overall, our results highlight that managing FM effectively requires attention not only to physical symptoms.
Keywords
Introduction
Fibromyalgia (FM) syndrome is a chronic and multifaceted condition characterized by widespread musculoskeletal pain, associated with a constellation of extra-articular symptoms such as fatigue, anxiety, depression, and sleep disturbances, which may be simultaneously present. 1 Diagnosing FM remains challenging, as no specific clinical or laboratory tests are currently available to confirm or exclude this condition.2,3 Although its etiopathogenesis is not yet fully elucidated, substantial evidence supports the primary role of central sensitization, a dysfunction in the neural circuits responsible for the perception, modulation, and processing of nociceptive inputs. 4 In recent years, additional factors have been suggested in FM pathogenesis, including low-grade inflammation, neuroimmune dysregulation, endocrine alterations, genetic predispositions, as well as psychosocial stressors.5,6
FM is largely considered a biopsychosocial disorder, wherein biological, psychological, and social dimensions interact dynamically to influence symptom expression and disease course. 4 Within this context, alexithymia, a personality construct denoting impaired emotional awareness and expression, has garnered considerable attention due to its potential role in shaping both psychological vulnerability and somatic symptom burden in FM.7,8 Originally described by Sifneos in 1972, alexithymia (from the Greek “a” = lack, “lexis” = word, “thymos” = emotion) refers to a cluster of traits including: difficulty identifying and describing feelings, confusion between emotions and bodily sensations, and a cognitive style characterized by externally-oriented thinking with diminished capacity for introspection and imaginative processes.9,10 Several studies showed a heightened prevalence of alexithymic traits across a range of chronic pain conditions, including chronic low back pain, myofascial pain syndrome, chronic migraine, and notably, FM.7,8,11,12 In individuals with FM, alexithymia has been reported in up to 48% of patients, significantly more than in healthy controls and those with other chronic inflammatory diseases such as rheumatoid arthritis. 13 Moreover, alexithymia in FM is positively correlated with greater psychological distress, particularly symptoms of anxiety and depression, as well as increased pain intensity.7,14 These findings underscore the clinical relevance of addressing emotional processing deficits as part of a comprehensive approach to FM management. Indeed, interventions targeting emotional awareness, regulation, and interpersonal functioning may hold therapeutic potential in this patient population.13,14
Drawing on previous research showing elevated rates of alexithymia in FM populations, 13 but acknowledging the limited understanding of its relationship with specific psychological constructs, the aim of the present study is to assess the interplay among alexithymia, self-compassion, pain catastrophizing, and hope, to develop future integrated and emotion-focused treatment strategies for this disease.
Methods
Participants’ inclusion/exclusion criteria
A cross-sectional observational study was conducted on Caucasian female participants attending the Arthritis Center, Rheumatology Clinic of the Fondazione Policlinico Campus Bio-Medico of Rome. A consecutive sampling strategy was employed. All eligible Caucasian women attending the clinic between October 2023 and June 2024 were screened, and 112 consecutive patients meeting the inclusion criteria were enrolled.
This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15 The completed STROBE checklist is provided as Supplemental File 1. Figure 1 shows a STROBE-compliant participant flow diagram summarizing screening, exclusion criteria, and final inclusion.
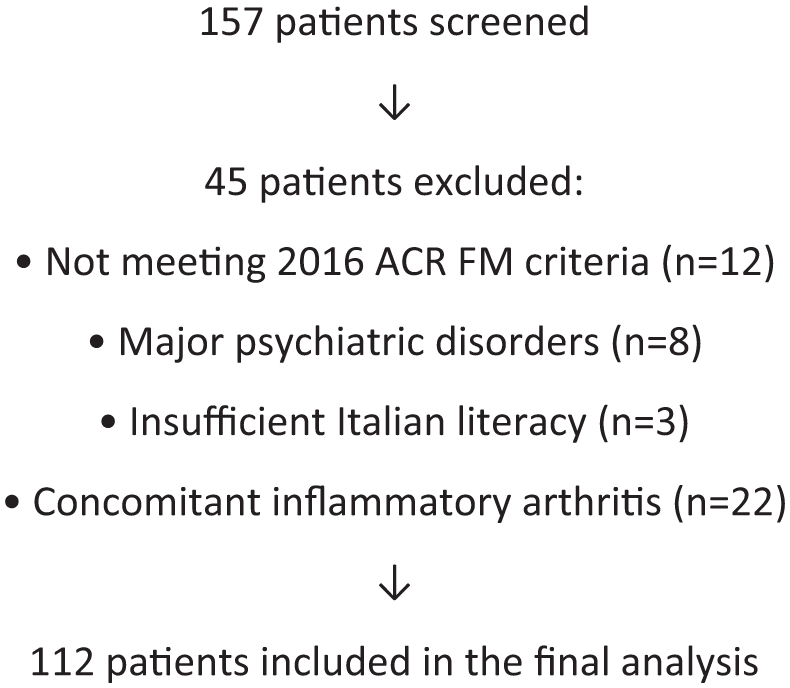
Participant flow diagram.
Participants were eligible if they met the following criteria: (i) a diagnosis of FM according to the 2016 American College of Rheumatology (ACR) revised criteria for FM 16 ; (ii) provision of written informed consent; (iii) age between 18 and 65 years; (iv) female sex; and (v) Caucasian ethnicity.
Exclusion criteria were: (i) <18 years old; (ii) low educational level (<5 years); (iii) presence of major psychiatric disorders according to the Diagnostic and Statistical Manual of Mental Disorders 5th Edition 17 ; (iv) insufficient knowledge of the Italian language that would prevent filling out the questionnaires; and (v) having concomitant FM complicating chronic inflammatory diseases. 18
Ethics
The study was approved by the Ethics committee of the University Campus Bio-Medico of Rome and conducted in conformity with the Declaration of Helsinki and its later amendments (approval number 13.23, May 2023).
Materials
At baseline, socio-demographic, clinical, and psychometric data have been collected. FM disease measures included the Widespread Pain Index (WPI), Symptom Severity Scale (SSS), Polysymptomatic Distress Scale (PDS), modified Fibromyalgia Assessment Scale (FAS-mod), and revised Fibromyalgia Impact Questionnaire (FIQ-R). Psychometric measures included 20-item Toronto Alexithymia Scale (TAS-20), Adult Hope Scale (AHS), Hospital Anxiety and Depression Scale (HADS), Pain Catastrophizing Scale (PCS), and Self Compassion Scale (SCS). All psychometric and clinical questionnaires were fully completed by all participants, with no item-level or scale-level missingness. As a result, no completion thresholds were required, and no imputation procedures were performed; all analyses were conducted on complete cases.
Clinical evaluation
The WPI and SSS are integral components of the ACR 2010/2011 and revised 2016 diagnostic criteria for FM.16,19,20 The WPI quantifies the distribution of pain by assessing 19 specific anatomical regions; patients indicate whether they have experienced pain in each area over the past week, yielding a score ranging from 0 to 19. The SSS evaluates the severity of three core symptoms—fatigue, unrefreshing sleep, and cognitive disturbances—each rated on a scale from 0 (no problem) to 3 (severe). Additionally, it includes an assessment of the extent of somatic symptoms (headache, abdominal pain, and depression), also scored from 0 to 3, resulting in a total score ranging from 0 to 12.16,19,20
PDS is calculated as the sum of the WPI (range: 0–19) and the SSS (range: 0–12), yielding a total score ranging from 0 to 31.19–21
The FIQ-R is the most widely used and validated instrument for evaluating the severity and overall impact of fibromyalgia. 22 The FIQ-R comprises 21 numerical rating scale items (ranging from 0 to 10, with 10 representing the most severe level for each item), and assesses three core health domains: physical function, overall impact, and symptom severity. All items refer to the patient’s experiences over the previous 7 days. The total FIQ-R score ranges from 0 to 100, with higher scores indicating greater disease severity.22,23
The FAS-mod is a modified version of the original Fibromyalgia Assessment Status (FAS) questionnaire, developed in 2019. It consists of two components designed to assess symptoms experienced over the previous 7 days. The first component includes two 11-point numerical rating scales that evaluate fatigue and non-restorative sleep. The second component is a body manikin (anterior and posterior views) representing 19 distinct anatomical regions, used to assess the presence of widespread pain. The total FAS-mod score ranges from 0 to 39 and is calculated as the sum of the scores from the fatigue and sleep scales, along with the number of painful body areas indicated on the manikin.22,24,25
Psychometric evaluation
The TAS-20 is a self-report scale designed to measure the degree of alexithymia, which consists of 20 items. We used the Italian translation of the revised TAS-20.10,26,27 Although alexithymia is a dimensional construct, a cutoff score of 61 has been recommended to distinguish patients with and without alexithymia. 26 We classified patients based on alexithymia as a categorical variable: those with a TAS-20 score of 61 or higher were considered alexithymic, while those with a score below 61 were classified as non-alexithymic.9,10
The AHS, developed by Snyder in 1991, assesses an individual’s level of dispositional hope, a construct closely associated with psychological well-being and mental health. The scale is based on two interrelated components: pathways and agency. The pathways component reflects an individual’s perceived ability to generate effective strategies to achieve goals. In contrast, the agency component represents the motivational drive and self-belief in one’s capacity to initiate and sustain goal-directed behavior. The condensed version of the AHS consists of eight items—four measuring agency and four assessing pathways. Each item is rated on a 4-point Likert scale, where 1 corresponds to definitely false, 2 to mostly false, 3 to mostly true, and 4 to definitely true. Higher total scores indicate greater levels of hope, which may play a significant role in chronic conditions such as FM by influencing emotional resilience and adaptive coping strategies.28–30
The HADS is used to assess levels of anxiety and depression in a clinical setting. It consists of two subscales: one for anxiety and one for depression, each containing seven items. Each subscale score ranges from 0 to 21, and a score of 8 or more suggests a clinically relevant level of depression or anxiety symptoms. The overall score helps determine the severity of these two emotional states.31,32
The PCS measures the extent to which an individual experiences catastrophic thoughts about pain. It includes 13 items assessing rumination, magnification, and helplessness related to pain. High PCS scores correlate with greater pain perception and emotional distress.33,34
The SCS assesses the construct of self-compassion. Conceptualized by Neff,35,36 this psychological construct is defined as a healthy, nonjudgmental attitude toward oneself in times of failure, suffering, or personal inadequacy. SCS is a valid and reliable 26-item measure of self-compassion with excellent internal consistency.36–38 It includes subscales representing the three positive components of self-compassion (self-kindness, common humanity, mindfulness) and three negative corresponding components (self-judgment, isolation, overidentification). Participants are required to rate each item on a 5-point scale (1 “almost never” to 5 “almost always”).
Among the SCS subscales, the three negative components are reverse-scored. To compute the total self-compassion score (SCS-total), the items belonging to the negative subscales, self-judgment, isolation, and over-identification, should be first reverse-coded. Subsequently, the mean score for each subscale is calculated, and the overall self-compassion score is obtained by averaging the six subscale means. In this paper, the negative subscales are presented in all tables already in their reverse-coded form. Therefore, lower scores indicate higher levels of the original negative components (self-judgment, isolation, and over-identification) and reflect a reduced overall level of self-compassion. Self-compassion may be categorized as low (score range: 1.0–2.49), moderate (score range: 2.5–3.5), or high (score range: 3.51–5.0).
Statistical analysis
Normality of continuous variables was assessed using the Shapiro–Wilk test, and these were described using medians (25th–75th percentiles); categorical variables were presented as percentages (%). χ2 tests were used for analyzing contingency tables, while Mann–Whitney was used for rank comparisons of continuous variables. To address multiplicity across psychometric subscales, Holm’s step-down correction was applied to all p-values. Univariable and multivariable linear regression were employed to assess variables associated with alexithymia levels in FM patients.
A multivariable linear regression analysis was conducted to identify variables independently associated with alexithymia (TAS-20 score). Covariates were selected through a stepwise selection approach. For analytical planning, an ANOVA-based screening across TAS-20 categories using PCS scores was performed, with sample size considerations based on an expected medium effect size (f = 0.40), α = 0.05, β = 0.20 (power = 0.80), 3 groups, and a minimum required sample of 66 participants. The final sample (n = 112) exceeded this threshold. Covariates entered into the final model included Age, body mass index (BMI), SSS, PCS-Helplessness, and SCS-Overidentification.
Model assumptions were evaluated through standard diagnostics. Linearity and homoscedasticity were examined visually and tested using the studentized Breusch–Pagan test (BP = 0.88, p = 0.97). Residual normality was confirmed by the Shapiro–Wilk test (W = 0.991, p = 0.659). Collinearity was minimal, with all Variance Inflation Factor (VIF) values below 1.5 (Age = 1.04; BMI = 1.07; SSS = 1.19; PCS-Helplessness = 1.43; SCS-Overidentification = 1.29). As all assumptions were satisfied, no robust or penalized models were required. The final model accounted for 37% of the variance in alexithymia (adjusted R2 = 0.37). All statistical analyses were performed using R Studio (version 4.5.0), with p-values <0.05 considered “statistically significant.”
Results
The median age of the participants was 51 years (46.25–59.25). Regarding marital status, 20 patients (17.9%) were single, 25 (22.3%) were cohabiting, 34 (30.4%) were married, 20 (17.9%) were divorced, and 13 (11.6%) were widowed. Forty-six participants (41.1%) had a FIQ-R score >70, indicating a higher level of disease severity. 23 Data on the socio-demographic and clinical variables are presented in Table 1.
Demographic, clinical, and psychometric characteristics of study population.
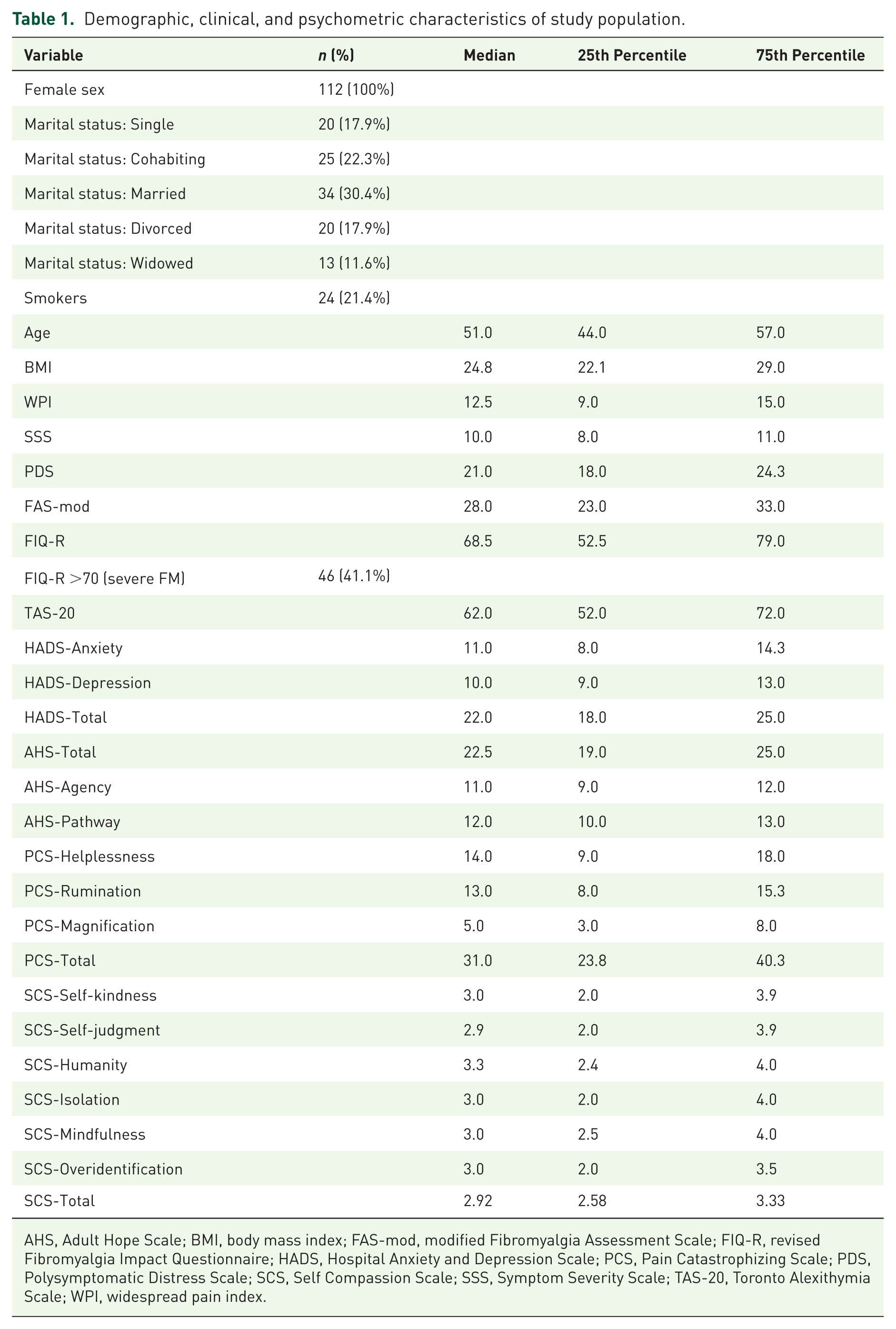
AHS, Adult Hope Scale; BMI, body mass index; FAS-mod, modified Fibromyalgia Assessment Scale; FIQ-R, revised Fibromyalgia Impact Questionnaire; HADS, Hospital Anxiety and Depression Scale; PCS, Pain Catastrophizing Scale; PDS, Polysymptomatic Distress Scale; SCS, Self Compassion Scale; SSS, Symptom Severity Scale; TAS-20, Toronto Alexithymia Scale; WPI, widespread pain index.
Participants were stratified into three groups based on TAS-20 scores: no alexithymia (⩽51; n = 26, 24.2%), borderline alexithymia (52–60; n = 28, 25%), and alexithymia (⩾61; n = 58, 51.8%). A comprehensive comparison of demographic, clinical, and psychometric characteristics was conducted across these groups. There were no statistically significant differences among the groups in terms of age (p = 0.428) or BMI (p = 0.201). Clinical pain measures such as the WPI and SSS did not differ significantly (p = 0.122 and p = 0.260, respectively). However, a trend toward higher levels of PDS and FIQ-R was observed in patients with alexithymia, although significance was not reached (p = 0.308 and p = 0.060, respectively).
In contrast, patients with alexithymia showed elevated symptoms of anxiety (HADS-Anxiety: 13 (9.25–15.75), p = 0.001), depression (HADS-Depression: 11.5 (9–14), p = 0.001), and total psychological distress (HADS-Total: 23.5 (20–28), p = 0.001).
Regarding cognitive-emotional variables, alexithymic participants showed a significantly lower total hope score (AHS-Total: 21 (17–24), p = 0.024), with no statistical significance regarding the two subscales Agency and Pathways, (p = 0.068, respectively). Pain catastrophizing was markedly higher in the alexithymia group, with a significant increase in the levels of Helplessness (p < 0.001), Rumination (p < 0.001), Magnification (p < 0.001), and PCS-Total (median: 35.5 (28.75–42.5), p = 0.003) scores.
Alexithymia was associated with significantly higher levels of self-judgment (p = 0.012) as well as significant increased levels of overidentification (p = 0.012). The SCS-Total was slightly lower in alexithymic individuals (median: 2.85 (2.5–3.25)) but did not reach statistical significance (p = 0.120). Data on alexithymia group comparisons are presented in Table 2.
Alexithymia group comparison.
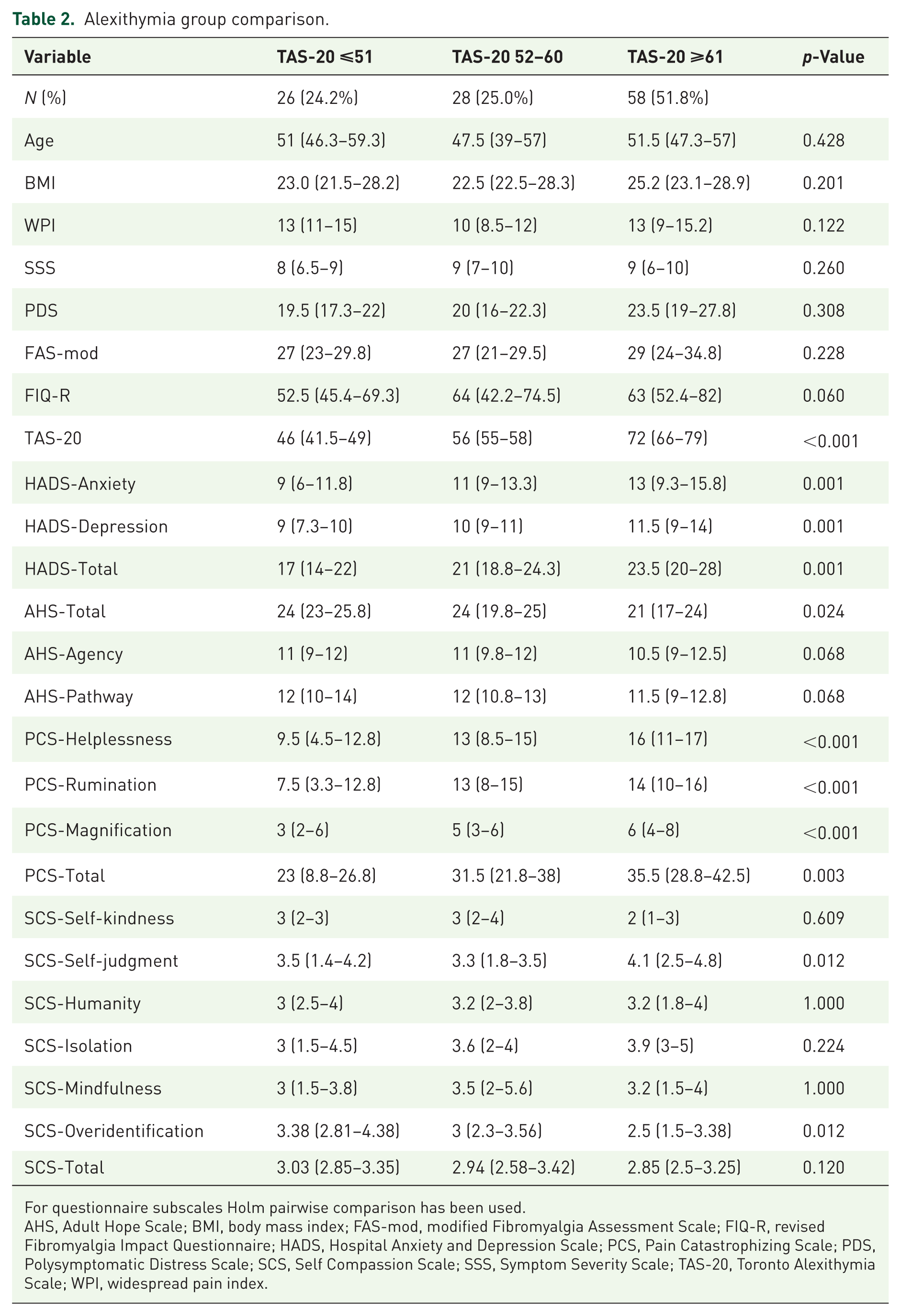
For questionnaire subscales Holm pairwise comparison has been used.
AHS, Adult Hope Scale; BMI, body mass index; FAS-mod, modified Fibromyalgia Assessment Scale; FIQ-R, revised Fibromyalgia Impact Questionnaire; HADS, Hospital Anxiety and Depression Scale; PCS, Pain Catastrophizing Scale; PDS, Polysymptomatic Distress Scale; SCS, Self Compassion Scale; SSS, Symptom Severity Scale; TAS-20, Toronto Alexithymia Scale; WPI, widespread pain index.
A univariable linear regression analysis was performed to examine the association between a wide range of demographic, clinical, and psychological variables and the level of alexithymia. Among demographic variables, no significant associations were found between age (β = 0.15; 95% confidence interval (CI): −0.09 to 0.39; p = 0.213), BMI (β = 0.34; 95% CI: −0.16 to 0.83; p = 0.177), smoking status (β = 1.83; 95% CI: −4.50 to 8.15; p = 0.568), and marital status (β = 1.52; 95% CI: −1.43 to 4.47; p = 0.310). Regarding clinical measures, the following variables showed statistically significant positive associations with alexithymia: SSS (β = 3.22; 95% CI: 2.14–4.30; p < 0.001), PDS (β = 0.86; 95% CI: 0.39–1.32; p < 0.001), FAS-mod (β = 0.54; 95% CI: 0.15–0.93; p = 0.007), and FIQ-R (β = 0.34; 95% CI: 0.22–0.47; p < 0.001).
In the emotional and psychological domain, significant associations were found for: HADS-Anxiety (β = 1.12; 95% CI: 0.51–1.72; p < 0.001), HADS-Depression (β = 1.75; 95% CI: 1.03–2.47; p < 0.001), HADS-Total (β = 0.91; 95% CI: 0.54–1.28; p < 0.001). Conversely, hope-related constructs were negatively associated with alexithymia: AHS-Total (β = −1.00; 95% CI: −1.46 to −0.54; p < 0.001), AHS-Agency (β = −2.02; 95% CI: −2.92 to −1.11; p < 0.001), AHS-Pathway (β = −1.69; 95% CI: −2.50 to −0.88; p < 0.001). Regarding pain catastrophizing, all subdomains and total scores were significantly and positively associated with TAS-20: Helplessness (β = 1.08; 95% CI: 0.69–1.46; p < 0.001), Rumination (β = 1.15; 95% CI: 0.69–1.61; p < 0.001), Magnification (β = 1.62; 95% CI: 0.85–2.39; p < 0.001), PCS-Total (β = 0.53; 95% CI: 0.35–0.71; p < 0.001). Within the domain of self-compassion, multiple components were significantly negatively associated with alexithymia, in particular Self-judgment (β = −3.09; 95% CI: −5.15 to −1.02; p = 0.004) and Overidentification (β = −4.35; 95% CI: −6.44 to −2.27; p < 0.001). As Self-judgment and Overidentification are reverse-scored, lower scores indicate greater levels of these negative components, making negative β coefficients directionally consistent. Other components, such as Self-kindness, Common Humanity, and Mindfulness, did not show significant associations (all p > 0.05). These data are presented in Table 3.
Univariable linear regression analysis, TAS-20 as dependent variable.
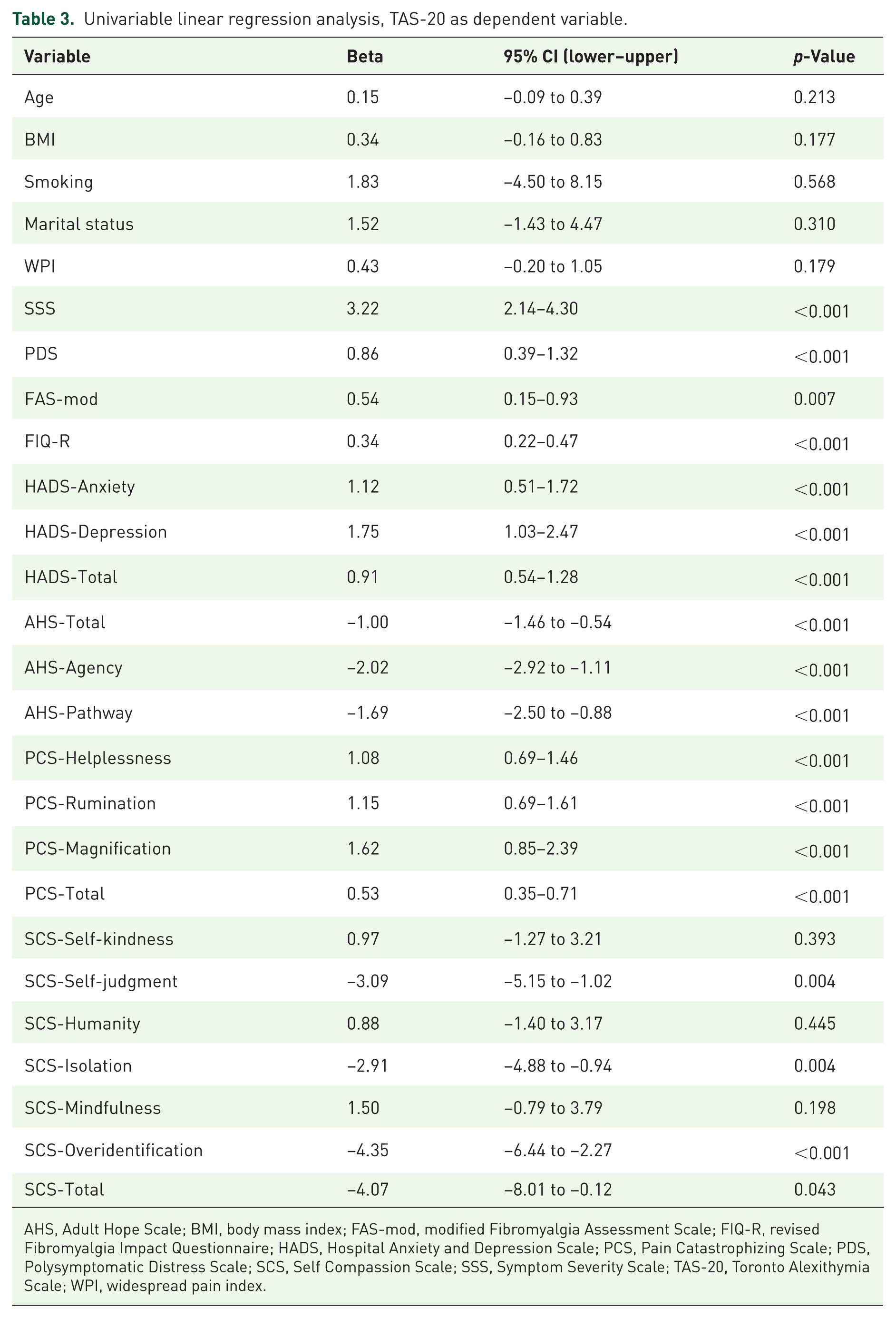
AHS, Adult Hope Scale; BMI, body mass index; FAS-mod, modified Fibromyalgia Assessment Scale; FIQ-R, revised Fibromyalgia Impact Questionnaire; HADS, Hospital Anxiety and Depression Scale; PCS, Pain Catastrophizing Scale; PDS, Polysymptomatic Distress Scale; SCS, Self Compassion Scale; SSS, Symptom Severity Scale; TAS-20, Toronto Alexithymia Scale; WPI, widespread pain index.
A multivariable linear regression was conducted to identify independent variables associated with alexithymia levels. After adjusting for relevant covariates (age and BMI), SSS, PCS-Helplessness, and SCS-Overidentification emerged as significant independent associated variables. Specifically, SSS was strongly associated with higher alexithymia scores (β = 2.25; 95% CI: 1.18–3.33; p < 0.001), indicating that increased symptom severity is independently associated to the emotional dysregulation captured by the TAS-20. Helplessness was also an independent significant positive associated variable (β = 0.59; 95% CI: 0.18–1.00; p = 0.005), supporting the relevance of maladaptive pain coping in alexithymic traits. SCS-Overidentification showed a significant inverse association with alexithymia (β = −2.40; 95% CI: −4.41 to −0.39; p = 0.020), consistent with its reverse scoring, whereby lower scores reflect greater levels of this negative component. Data are presented in Table 4.
Multivariable regression analysis, TAS-20 as dependent variable, model adjusted for age, BMI, SSS, PCS-Helplessness, and SCS-Overidentification.
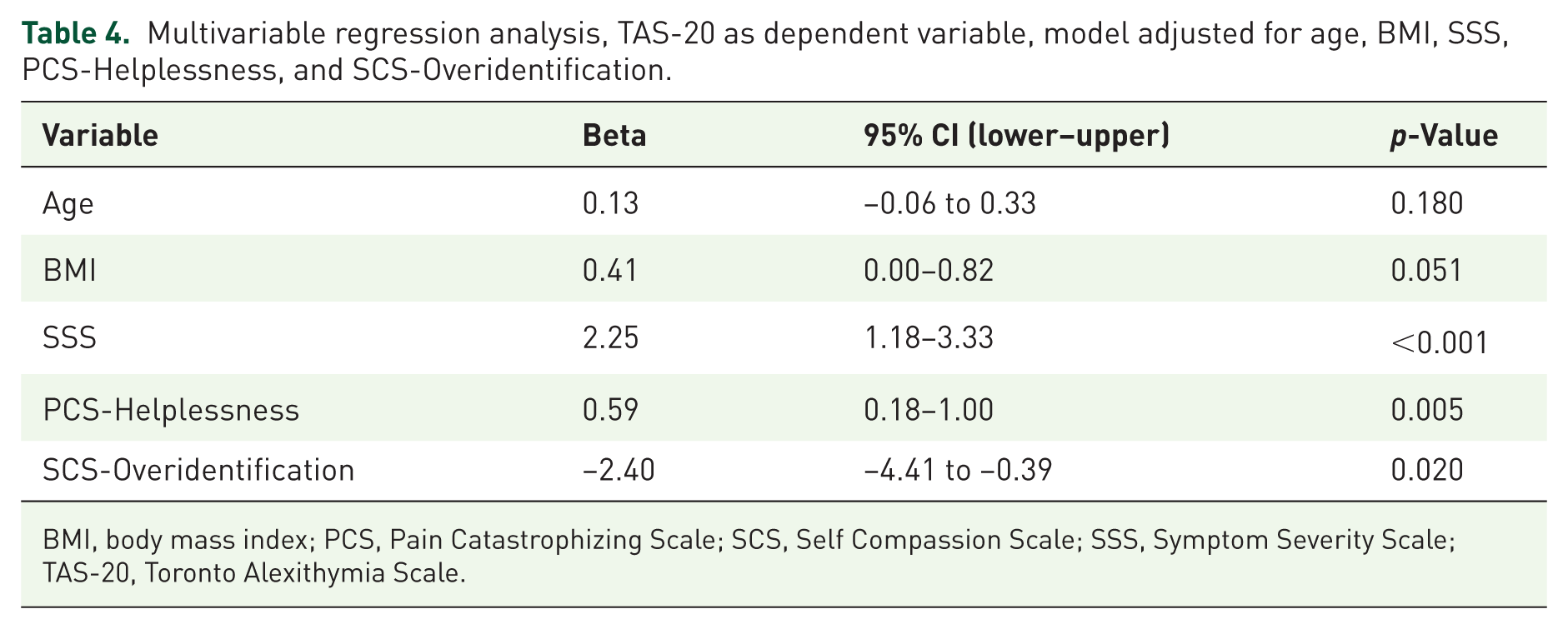
BMI, body mass index; PCS, Pain Catastrophizing Scale; SCS, Self Compassion Scale; SSS, Symptom Severity Scale; TAS-20, Toronto Alexithymia Scale.
Discussion
Our findings underscore the central role of emotional dysregulation and maladaptive cognitive-affective processes in FM patients who exhibit alexithymic traits. Alexithymia is considered a prototypical example of emotion dysregulation characterized by impairments across multiple stages of emotional processing, both at the psychological and physiological levels. 9 Although it is well established in the literature that patients with chronic pain, especially those with FM, show higher levels of pain catastrophizing, 39 elevated psychological distress,14,40 and reduced self-compassion, 41 this study is the first to combine these different psychological constructs into one framework. In our cohort, a substantial proportion of FM patients exhibited clinically significant alexithymic traits (51.8%), mirroring prior reports of rates up to 48% in FM, higher than those observed in other chronic pain conditions (e.g., low back pain, chronic migraine) and rheumatic diseases such as rheumatoid arthritis and systemic lupus erythematosus.7,11,13,42 This increased frequency may reflect both primary alexithymia, a stable personality disposition characterized by lifelong deficits in emotional awareness, and secondary alexithymia, which may emerge as an adaptive response to chronic nociceptive input and the stress of living with persistent pain. 43
In our study, several psychological and symptom-related variables seem to be key contributors to alexithymic profiles. Consistent with our hypotheses, alexithymic FM patients showed higher levels of anxiety and depression, reduced self-compassion, lower dispositional hope, and heightened pain catastrophizing compared to their non-alexithymic counterparts. Specifically, they showed higher isolation, and overidentification on the SCS, reported lower agency and pathways thinking on the AHS, and indicated greater magnification, rumination, and helplessness on the PCS. These patterns, further confirmed in the univariable analysis, suggest that alexithymia in FM is not an isolated deficit in emotion identification but is embedded within a broader profile of maladaptive cognitive–affective coping, predisposing to global suffering.
Moreover, the univariable analysis revealed significant positive associations between alexithymia and clinical indicators of disease severity, such as SSS, PDS, FIQ-R, and FAS-mod. Interestingly, only WPI was not associated with alexithymia, even though it contributes to both the PDS and the FAS-mod score. This finding suggests that alexithymia may be a more complex construct, encompassing not only pain but also other somatic issues, such as fatigue and sleep disturbances, which collectively have a greater impact on quality of life. Alternatively, differently from previous studies linking pain and alexithymia, we assessed pain distribution using the WPI scale rather than Visual Analogue Scale (VAS)-pain or other pain-related questionnaires.13,40,44
The multivariable regression model further refined these findings, identifying SSS, PCS-Helplessness, and SCS-Overidentification as strong, independent variables associated with alexithymia, providing insights into the multifaceted network dynamics that support alexithymia in FM patients.
These findings may have some clinical implications. First, the assessment of alexithymia and related psychological constructs should be integrated into the comprehensive evaluation of FM patients. Second, evaluating emotional status alongside traditional measures may facilitate the internal stratification of patients and guide the development of tailored psychoeducational interventions aimed to improve the quality of life. Interventions targeting emotional awareness and regulation, such as mindfulness and mindful self-compassion training,35,45–49 may be particularly beneficial for those patients exhibiting high levels of alexithymia. Further studies may help to clarify the bidirectional link between emotional dysregulation and somatic distress amplification and providing evidence that managing alexithymia may improve psychological well-being as well as support adaptive coping strategies.
Limitations
We are aware that our study has some limitations. First, the relatively small sample size warrants caution in interpreting and generalizing the findings. Moreover, as this was an exploratory observational study, no a priori sample size calculation or power analysis was performed. Second, because our cohort consisted exclusively of Caucasian women recruited from a single center, the findings may not be representative of male FM populations or individuals from diverse ethnic backgrounds. Third, we are unable to distinguish between primary and secondary alexithymia. 43
In addition, the absence of a clinical control group limits our ability to distinguish FM-specific patterns from those associated with other chronic pain conditions. All psychometric variables (e.g., TAS-20, HADS, PCS, SCS) were based on patient self-report, introducing the possibility of response bias, social desirability effects, or inaccuracies.
Although fatigue represents a core symptom of FM, no stand-alone fatigue instrument was administered; however, fatigue was partially assessed through selected items within the SSS and FIQ-R. Moreover, structured data on medication use and menopausal status were not collected, despite their potential influence on symptom severity and psychological parameters. Their absence prevented us from exploring possible moderating or interacting effects, underscoring the importance of including these variables in future research.
Finally, the cross-sectional design does not allow for causal inference or the assessment of temporal relationships among variables, highlighting the need for longitudinal studies to better clarify directionality and underlying mechanisms.
Conclusion
To the best of our knowledge, this study is the first to demonstrate that alexithymia is associated with overall symptom severity, pain catastrophizing, and reduced levels of hope and self-compassion, psychological constructs whose relationships with alexithymia had not previously been assessed collectively. Furthermore, our results suggest that incorporating alexithymia, catastrophic thinking, and self-related constructs into a unified clinical framework may be helpful for diagnosing, monitoring, and managing FM. Longitudinal and interventional studies are now needed to evaluate whether targeted reduction of alexithymic traits can produce durable improvements in patient-centered outcomes.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261421707 – Supplemental material for Mapping emotional function in fibromyalgia: integrating alexithymia, pain catastrophizing, and self-compassion
Supplemental material, sj-docx-1-tab-10.1177_1759720X261421707 for Mapping emotional function in fibromyalgia: integrating alexithymia, pain catastrophizing, and self-compassion by Francesca Trunfio, Onorina Berardicurti, Rosa Bruni, Damiano Currado, Barbara Biticchi, Erika Corberi, Francesca Saracino, Lyubomyra Kun, Annalisa Marino, Ludovica Lamberti, Leonardo Frascà, Antonio Orlando, Andrea Pilato, Sebastiano Lorusso, Francesco Cimino, Alessandra Pia Crocitta, Dario Nejat, Lorenzo Fusco, Gianmarco Coluccia, Swathy Jayakrishnan, Irene Genovali, Marta Gatti, Marta Vomero, Vasiliki Liakouli, Roberto Giacomelli and Luca Navarini in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.