
Abstract
Background:
Predicting difficult-to-manage (D2M) axSpA remains challenging, as both inflammatory and non-inflammatory factors contribute to treatment failure. Functional impairment captured by Health Assessment Questionnaire–Disability Index (HAQ-DI) and Multidimensional Health Assessment Questionnaire (MDHAQ) may provide additional predictive value, but are rarely evaluated in this context.
Objectives:
To assess the predictive value of HAQ-DI and MDHAQ for identifying patients at risk of D2M axSpA in real-world clinical practice.
Design:
Single-center retrospective observational study based on data from a clinical registry.
Methods:
The study included patients with axSpA initiating biologic or targeted synthetic disease-modifying antirheumatic drugs. Data included demographic, clinical, and laboratory parameters, as well as patient-reported outcomes. D2M status was defined according to the Assessment of SpondyloArthritis International Society (ASAS) criteria. Health status was evaluated using HAQ-DI and MDHAQ. Logistic regression identified predictors of D2M status at baseline, 24 and 48 weeks.
Results:
The cohort included 300 treatment courses in 217 patients (average age 45 years, 49% female, 83% HLA-B27 positive, 83% r-axSpA). At baseline, 11% patients met ASAS criteria for D2M axSpA, decreasing to 8.8% at week 48. D2M patients were older (p = 0.03), exercised less frequently (p = 0.04) and had higher disease activity. In multivariable models, baseline HAQ-DI independently predicted D2M status at baseline (OR 3.29, p = 0.008) and week 24 (OR 4.56, p = 0.005) and functional dimension of MDHAQ at week 24 (OR 3.47, p = 0.039).
Conclusion:
Functional impairment, reflected by higher HAQ-DI and MDHAQ scores, was the strongest predictor of D2M axSpA and may serve as a valuable tool for identifying these patients early and addressing nonpharmacological management strategies ahead.
Plain language summary
Axial spondyloarthritis (axSpA) is a long-term inflammatory rheumatic disease that mainly affects the spine and causes pain, stiffness, and reduced mobility. Some patients respond well to treatment, while others continue to experience troublesome symptoms even when receiving innovative drugs such as biologic or targeted synthetic. If two or more of such therapies fail, these patients are described as having difficult-to-manage (D2M) axSpA. Being able to identify such patients early may help doctors provide better care and distinguish between the true need of modification of pharmacotherapy or rather addressing other aspects of the disease, such as pain and functional decline due to causes not related to inflammation. In this study, we followed adults with axSpA who were receving biologic or targeted synthetic treatments. We collected clinical information, laboratory results, and patients’ own reports about how their symptoms affect daily activities. Two questionnaires “HAQ-DI” and “MDHAQ” were used to measure everyday functioning, such as the ability to dress, stand, walk, or complete routine tasks. We found that patients with D2M axSpA had worse functional limitations from the beginning and throughout treatment, even though inflammation markers in blood tests were similar to other patients. Higher HAQ-DI and MDHAQ scores strongly predicted which patients would continue to struggle during treatment. These findings suggest that assessing everyday functioning “not only inflammation” can help identify people who may need additional support. Early use of exercise programs, physical therapy, and personalized care strategies could improve outcomes for these patients.
Background
Prediction of difficult-to-manage axial spondyloarthritis (D2M axSpA) in clinical practice remains challenging due to the limited availability of longitudinal data addressing both inflammatory and non-inflammatory determinants. The definition of D2M axSpA, developed in 2025 by the Assessment of SpondyloArthritis International Society (ASAS), comprises three key elements: (1) treatment failure of ⩾2 biologic or targeted synthetic disease-modifying antirheumatic drugs (DMARDs) with different mechanisms of action; (2) suboptimal disease control; and (3) persistent or problematic signs or symptoms acknowledged by either the physician or the patient. 1 The multifactorial nature of D2M axSpA reflects the contribution of sociodemographic, inflammatory, and other factors not directly related to rheumatic disease activity, such as comorbidities and psychosocial factors.1 –3 Female sex, current smoking, fewer years of education, and having no paid work have been associated with a higher likelihood of D2M status.4,5 Among inflammatory factors, high baseline disease activity, peripheral musculoskeletal involvement (arthritis, enthesitis, or dactylitis), and coexisting psoriasis or inflammatory bowel disease (IBD) are recognized as major contributors to persistent disease activity.4 –7 Additionally, factors not directly related to rheumatic disease activity, including comorbidities (e.g., obesity, depression, fibromyalgia, hypertension), central pain sensitization, irreversible structural damage, along with reduced physical capacity secondary to long-standing disease, play a substantial role in sustaining residual symptoms and signs and treatment refractoriness.2,3,8,9 Together, these mechanisms may sustain residual symptoms despite adequate suppression of inflammation and increase the likelihood of fulfilling D2M criteria. 1
Recognizing and addressing this complex interaction is essential to differentiate between a true need for DMARD modification due to ongoing inflammation and the necessity of addressing non-inflammatory contributors that falsely amplify disease activity. However, implementing such a multifactorial assessment remains difficult in daily clinical practice, and longitudinal evidence on the predictive potential of these risk factors for D2M axSpA remains limited. Hence, there is a need to explore the prognostic value of clinical assessment measures, with special attention to non-inflammatory determinants. Among patient-reported outcome measures, the Health Assessment Questionnaire–Disability Index (HAQ-DI) is a widely used indicator of health status in inflammatory rheumatic diseases, reflecting functional limitation and perceived health. Another tool, the Multidimensional Health Assessment Questionnaire (MDHAQ) and its derivative, Routine Assessment of Patient Index Data 3 (RAPID 3), examines a functional component and adds psychological and general-health domains (e.g., patient global assessment, pain, fatigue/sleep/mood), yielding a more holistic picture of disease impact in routine care. 10 In axSpA cohorts, all three questionnaires align well with Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) or Bath Ankylosing Spondylitis Functional Index (BASFI) for overall symptom burden and can be applied in a busy clinic, while dedicated axSpA measures such as Axial Spondyloarthritis Disease Activity Score (ASDAS) indices still anchor disease activity evaluation.11 –13 In the setting of D2M axSpA, the ASAS expert consensus emphasizes that challenging management may persist despite controlled objective inflammation; as such, persistently high HAQ-DI or MDHAQ scores should prompt consideration of non-inflammatory drivers, such as structural damage or psychosocial distress.
Therefore, while HAQ-DI and MDHAQ provide valuable insight into the multidimensional burden of disease in axSpA, data on their predictive value in difficult-to-manage axSpA patients remains limited. The aim of our study was to address this gap, by evaluating the predictive value of these patient-reported measures and D2M status in a real-world cohort of patients.
Methods
This study was designed as a retrospective analysis of real-world data, with a longitudinal analytical approach. The ASAS definition of difficult-to-manage axial spondyloarthritis (D2M axSpA) was applied retrospectively to the already collected clinical data of patients initiating biological or targeted synthetic disease-modifying antirheumatic drugs (bDMARDs or tsDMARDs), with follow-up assessments at 24 and 48 weeks as part of routine clinical care. These time points were selected because they correspond to mandatory evaluations required for patients receiving b/tsDMARDs under the national guidelines. Real-world data were collected during routine clinical assessments and recorded using standardized clinical software (GoTreatIt Rheuma). 14 Patient-reported outcome measures were completed electronically by patients using tablet devices in the outpatient clinic prior to the clinical consultation. Patients who initiated their first or concurrent b/tsDMARD therapy between January 1, 2021, and October 1, 2025, were recruited at a single-center in an outpatient setting.
Eligible participants had a clinical diagnosis of axSpA made by a qualified rheumatologist and fulfilled the Assessment of Spondyloarthritis (ASAS) classification criteria. 15 Other inclusion criteria comprised the ability to provide informed consent, complete self-reported questionnaires, and initiation of treatment with a bDMARD or tsDMARD. Patients with unavailable baseline data (e.g., treatment initiated before the data collection period) were excluded. No additional exclusion criteria were applied, as the study was designed to reflect real-world clinical practice.
Data extraction was performed on October 6, 2025, and included anonymized variables relevant to the analysis. All clinical assessments were conducted by physicians trained in rheumatology or internal medicine. Patient-reported outcome questionnaires were completed electronically on-site during scheduled visits. The study protocol was approved by the Institutional Review Board. All participants provided written informed consent prior to participation, with assurance that their responses would be used exclusively for research purposes.
Baseline demographic and clinical variables collected for analysis included age (years), sex (male/female), and body mass index (BMI), calculated from patient-reported weight and height (kg/m2). Additional variables included self-reported cigarette smoking (yes/no), current employment status (employed/unemployed), years of education, physical exercise at least once per week (yes/no), and baseline HLA-B27 status (positive/negative).
Comorbidities were initially self-reported by patients through electronic entry on tablet devices as part of the standardized assessment in GoTreatIt Rheuma. Subsequently, the treating physician reviewed and verified the reported comorbidities during the clinical visit using available electronic medical records, prior documentation, and relevant clinical information. Cardiovascular comorbidities included hypertension, arrhythmia, hypercholesterolemia, ischemic heart disease, and peripheral artery disease. Gastrointestinal comorbidities included peptic ulcer disease, gastroesophageal reflux disease, IBD, and liver disease. Endocrine comorbidities included thyroid disorders and diabetes mellitus. Dermatological comorbidities were also recorded. Other comorbidities were not included in the analysis due to their absence or low prevalence in the study cohort; however, these data are available upon reasonable request.
Regarding treatment, the current line of bDMARD or tsDMARD therapy was recorded, and proportions were calculated. Information on prior bDMARD or tsDMARD treatment was also collected, including TNF inhibitors (adalimumab, golimumab, infliximab, certolizumab, etanercept), IL-17 inhibitors (bimekizumab, ixekizumab, secukinumab), and targeted synthetic DMARDs (upadacitinib, tofacitinib). Currently initiated treatment, including the above medications, was also reported. Treatments comprised both original formulations and generic medications, as determined by the national healthcare fund system.
Clinical and disease activity variables included laboratory results, specifically erythrocyte sedimentation rate (ESR, mm/h) and serum C-reactive protein (CRP, mg/L) concentration. The Axial Spondyloarthritis Disease Activity Score using CRP (ASDAS-CRP) was calculated as a composite measure of disease activity. Investigator global assessment (IGA, 0–100) and patient-reported outcome measures, including patient global assessment (PGA, 0–100) and the BASDAI (0–10), were recorded. Additionally, patients reported their current global pain, back pain, and fatigue on 0–100 visual analog scales.
Functional disability was assessed using the Health Assessment Questionnaire (HAQ), Multidimensional Health Assessment Questionnaire (MDHAQ) and the Routine Assessment of Patient Index Data 3 (RAPID3), a validated patient-reported instrument evaluating difficulty in performing activities of daily living. The HAQ-DI comprises eight domains (dressing, arising, eating, walking, hygiene, reach, grip, and usual activities), each scored from 0 to 3, where 0 indicates no difficulty and 3 indicates inability to perform the activity. The total score is calculated as the mean of the domain scores, with higher values reflecting greater functional impairment. MDHAQ assesses both functional and psychological aspects of health–the functional component evaluates difficulties in performing daily activities such as dressing, walking, or gripping, while the psychological component captures aspects of emotional well-being, including fatigue, anxiety, and depression. Each item is scored on a 0–3 scale, with higher scores indicating greater impairment or symptom severity. RAPID3 can be derived directly from the MDHAQ. It combines three patient-reported domains: (1) physical function score from the MDHAQ (0–10), (2) pain (0–10), and (3) PGA (0–10). These components are summed to produce a total RAPID3 score ranging from 0 to 30, with higher scores reflecting greater disease activity and worse patient-reported outcomes. The BASFI is a patient-reported measure assessing functional ability in individuals with ankylosing spondylitis and axial spondyloarthritis. It comprises 10 questions on daily activities and physical function, each scored on a 0–10 numeric rating scale, with higher scores indicating greater functional impairment. The Bath Ankylosing Spondylitis Global Score (BAS-G) is a patient-reported measure evaluating overall well-being and disease impact in axial spondyloarthritis. It includes two visual analog scales assessing the patient’s perception of disease over the past week and the past 6 months, with scores ranging from 0 (best) to 10 (worst).
Patients were categorized as D2M across baseline and follow-up assessments using the following criteria: failure of at least two bDMARDs or tsDMARDs with different mechanisms of action, PGA or IGA score ⩾50 indicating issues with therapy from the patient’s or physician’s perspective, and high disease activity as indicated by an ASDAS-CRP >2.1. The proportion of patients classified as D2M at baseline referred to the entire cohort of patients initiating a b/tsDMARD, including both first-line and later-line initiators. While patients starting first-line therapy were not eligible to meet D2M criteria at baseline, they were intentionally retained in the denominator to reflect the real-world prevalence of D2M among all patients initiating b/tsDMARD therapy. As such, the baseline analysis was cross-sectional and reflects prevalent D2M cases. At weeks 24 and 48, the analysis was longitudinal and allowed identification of incident D2M cases—patients who newly fulfilled the criteria during follow-up after failing additional therapies or had persistent D2M status. These follow-up estimates reflect the combined effects of persistent prevalent cases and incident cases emerging during the observation period.
Potential sources of bias related to the observational real-world design were considered, including selection bias from single-center recruitment and information bias from self-reported patient outcomes. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 16
Statistical analysis
Since this is a real-world study, no formal sample size calculation or power analysis was performed. The sample size was determined by the data available from the observational sources. Results are presented as mean (standard deviation, SD) or number (percentage, %) depending on the variable type. The distribution of continuous variables was assessed using the Shapiro–Wilk test and visually using histograms. Due to the presence of non-normally distributed data, non-parametric tests were applied. Categorical variables were compared using the chi-square test or Fisher’s exact test, and numerical variables were compared using the Kruskal–Wallis test. To assess baseline factors potentially influencing D2M status at the 24- and 48-week follow-up, logistic regression models were used with D2M status as the dependent variable. Models were adjusted for relevant demographic and clinical variables, including age, sex, HLA-B27 status, HAQ, BMI, and CRP, based on investigator selection. The main method was the enter procedure, while the backward elimination method was additionally performed as a sensitivity analysis to confirm the robustness of the findings. A p-value <0.05 was considered statistically significant, and all p-values were two-sided. Analyses were conducted using IBM SPSS Statistics version 29.0.0.0, IBM Corp., Armonk, MY, USA. Due to the real-world nature of the study, some variables contained missing data; analyses were therefore performed using available case analysis without imputation.
Results
Characteristics of study population
Baseline characteristics of the study population are presented in Table 1. A total of 300 therapy cases from 217 patients with axial spondyloarthritis were included in the analysis. The cohort had an average age of 45 years, with 49% females and 83% testing positive for HLA-B27. Of the participants, 182 patients (84%) had radiographic axSpA, while 35 patients (16%) had non-radiographic axSpA. The occurrence of comorbidities was relatively rare, with cardiovascular, gastrointestinal and endocrine disorders being the most frequently seen. TNF inhibitors were the most used agents across all time points, followed by IL-17 inhibitors and, to a lesser extent, JAK inhibitors.
Baseline demographic, comorbidity, and treatment characteristics of the examined axial spondyloarthritis cohort, dichotomized by D2M status.
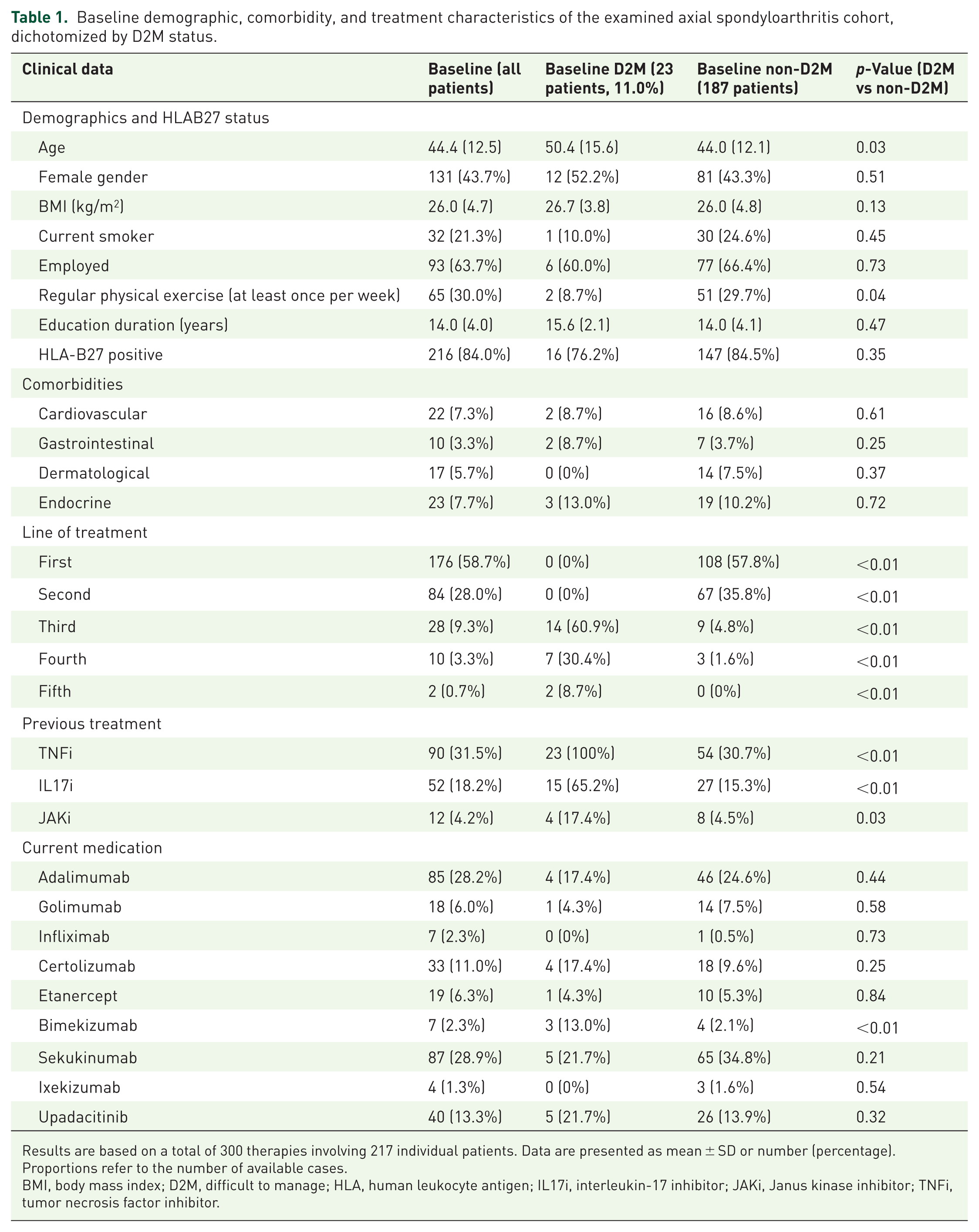
Results are based on a total of 300 therapies involving 217 individual patients. Data are presented as mean ± SD or number (percentage). Proportions refer to the number of available cases.
BMI, body mass index; D2M, difficult to manage; HLA, human leukocyte antigen; IL17i, interleukin-17 inhibitor; JAKi, Janus kinase inhibitor; TNFi, tumor necrosis factor inhibitor.
Occurrence of difficult-to-manage axSpA in the study cohort
At baseline (defined as initiation of any bDMARD or tsDMARD), 11% of patients met the ASAS criteria for D2M axSpA. During follow-up, the overall proportion of patients classified as D2M was 10.4% at week 24 and 8.8% at week 48 (Table 2). Nearly all D2M patients had prior exposure to TNF inhibitors, and more than half were receiving third-line or later biologic therapies, most commonly targeting the IL-17 pathway (Table 1).
Clinical variables, patient-reported outcome measures, and composite scores at baseline and follow-ups, dichotomized by D2M status.

Results are based on a total of 300 therapies involving 217 individual patients. Data are presented as mean ± SD or number (percentage). Proportions refer to the number of available cases. p-Values refers to results of comparison at specific time point.
ASDAS-CRP, Ankylosing Spondylitis Disease Activity Score calculated with C-reactive protein; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BAS-G, Bath Ankylosing Spondylitis Global Score; CRP, C-reactive protein; D2M, difficult to manage; ESR, Erythrocyte Sedimentation Rate; HAQ-DI, Health Assessment Questionnaire Disability Index; IGA, Investigator Global Assessment; MDHAQ-Fn, Multidimensional Health Assessment Questionnaire, Functional; MDHAQ-Ps, Multidimensional Health Assessment Questionnaire, Psychological; PGA, Patient Global Assessment; RAPID3, Routine Assessment of Patient Index Data 3; VAS, visual analog scale.
Factors associated with difficult-to-manage axSpA
In the cross-sectional comparison, patients with D2M axSpA were significantly older than those without D2M (mean age 50.4 ± 15.6 vs 44.0 ± 12.1 years; p = 0.03). The proportion of females (52.2% vs 43.3%; p = 0.51) and HLA-B27 positivity (76.2% vs 84.5%; p = 0.35) did not differ significantly between groups. The average symptom duration in the entire cohort was 15.3 ± 8.8 years, while the average disease duration was 8.3 ± 7.6 years, resulting in a mean diagnostic delay of 6.8 ± 6.5 years. Patients classified as D2M at baseline had a significantly longer symptom duration compared to non-D2M patients (18.4 ± 6.9 vs 15.4 ± 9.0 years; p = 0.04) and a longer disease duration (13.2 ± 7.8 vs 8.4 ± 7.4 years; p < 0.01). In contrast, diagnostic delay did not differ significantly between the groups (5.4 ± 4.0 vs 7.0 ± 6.9 years; p = 0.76).
Regular physical exercise (⩾ once per week) was significantly less common in D2M patients (8.7% vs 29.7%; p = 0.04). Other baseline variables, such as BMI, current smoking status, employment, years of education, and the presence of comorbidities, did not differ significantly between the D2M and non-D2M groups.
At baseline, patients with D2M axial spondyloarthritis presented with significantly higher disease activity and patient-reported outcome scores compared with non-D2M patients, including PGA, BASDAI, ASDAS-CRP, HAQ-DI, MDHAQ functional and psychological components, RAPID3, BASFI, and BAS-G (all p < 0.05). Higher global pain was also observed in the D2M group (p = 0.03). In contrast, IGA, ESR and CRP values did not differ significantly between groups at baseline, and differences in back pain and fatigue did not reach statistical significance.
At 24 and 48 weeks, D2M patients continued to demonstrate higher disease activity and disability scores across almost all measures, whereas CRP remained comparable between groups in week 48. Detailed results are presented in Table 2.
Predictive factors of difficult-to-manage axial spondyloarthritis: Longitudinal analysis
In the multivariable logistic regression model including age, sex, HLA-B27 status, BMI, and CRP, baseline HAQ-DI was the only variable significantly and independently associated with D2M status at baseline and at 24-week follow-up (Table 3).
Predictive factors for D2M at baseline, 24-week, and 48-week follow-up: logistic regression outcomes adjusted for HAQ and other clinically relevant variables.
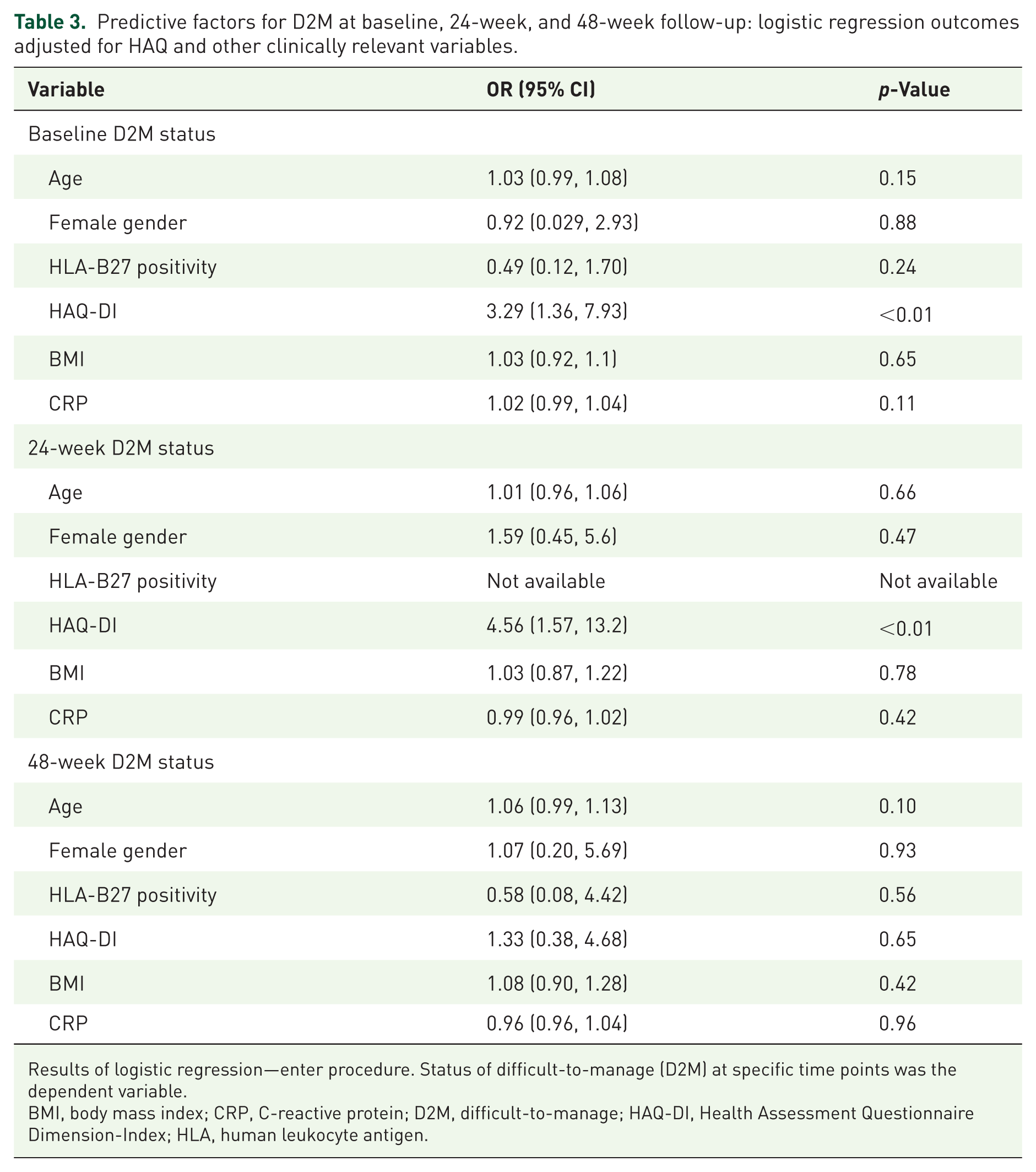
Results of logistic regression—enter procedure. Status of difficult-to-manage (D2M) at specific time points was the dependent variable.
BMI, body mass index; CRP, C-reactive protein; D2M, difficult-to-manage; HAQ-DI, Health Assessment Questionnaire Dimension-Index; HLA, human leukocyte antigen.
At baseline, higher HAQ-DI values were independently associated with an increased likelihood of meeting the ASAS D2M criteria (B = 1.189, p = 0.008; OR = 3.29, 95% CI 1.36–7.93). Similarly, at week 24, HAQ-DI remained a significant predictor of D2M status (B = 1.517, p = 0.005; OR = 4.56, 95% CI 1.57–13.23). No other demographic or clinical variables, including age, sex, HLA-B27 status, BMI, or CRP, showed a statistically significant association at either time point. At week 48, none of the included variables reached statistical significance. Although HAQ-DI and CRP showed numerical trends, neither met the threshold for statistical significance (p > 0.05).
In another model, including age, sex, HLA-B27 status, BMI, CRP, and baseline MDHAQ functional and psychological scores, only the MDHAQ functional score (MDHAQ-Fn) was identified as a significant independent predictor of D2M status at week 24 (B = 1.244, p = 0.039, OR = 3.47). None of the other variables—including age, sex, HLA-B27, BMI, CRP, or MDHAQ psychological (MDHAQ-Ps) showed a statistically significant association with D2M status (all p > 0.05). No additional predictors were found at other time points (Table 4).
Predictive factors for D2M at baseline, 24-week, and 48-week follow-up: logistic regression outcomes adjusted for MDHAQ-Fn, MDHAQ-Ps and other clinically relevant variables.
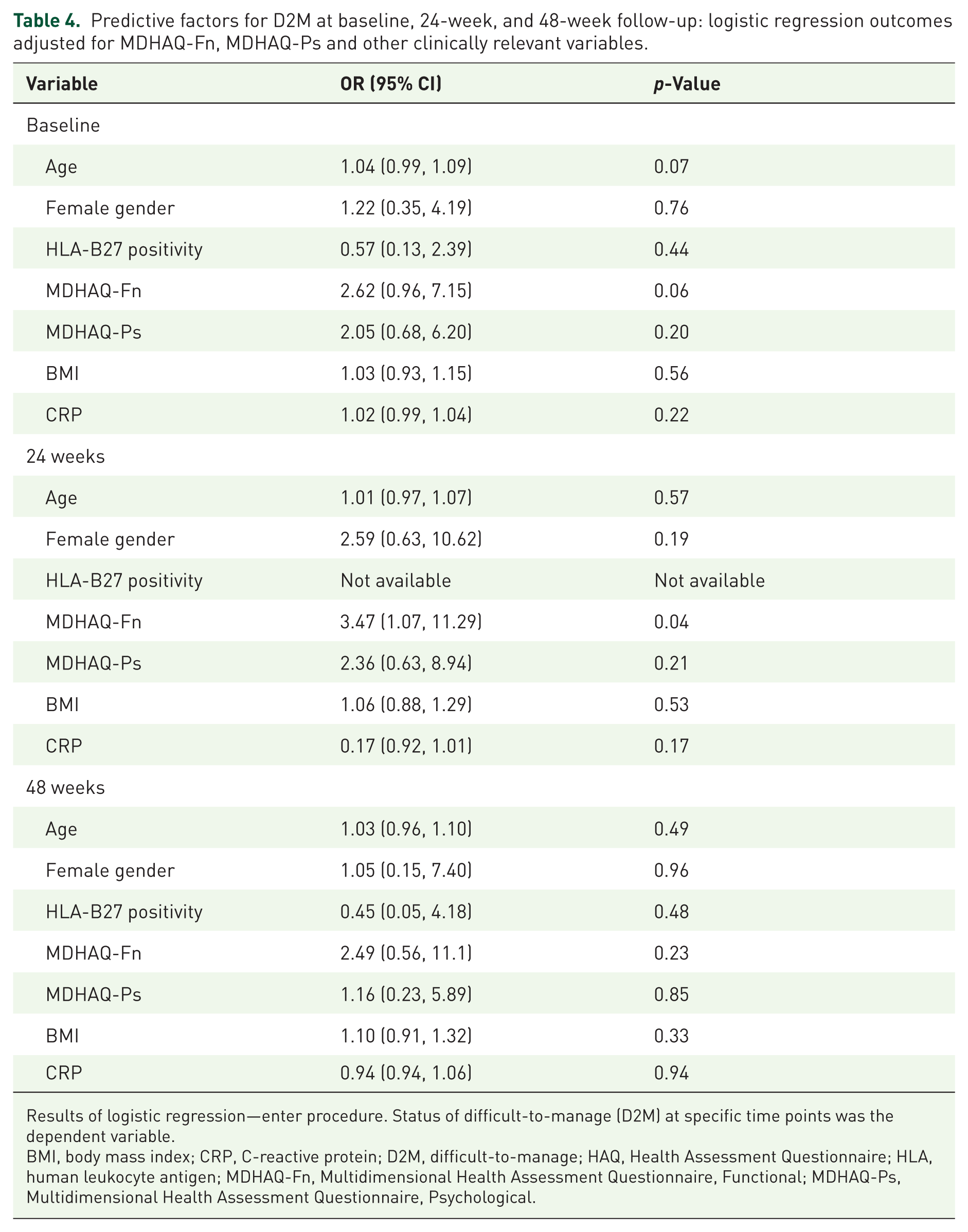
Results of logistic regression—enter procedure. Status of difficult-to-manage (D2M) at specific time points was the dependent variable.
BMI, body mass index; CRP, C-reactive protein; D2M, difficult-to-manage; HAQ, Health Assessment Questionnaire; HLA, human leukocyte antigen; MDHAQ-Fn, Multidimensional Health Assessment Questionnaire, Functional; MDHAQ-Ps, Multidimensional Health Assessment Questionnaire, Psychological.
In a combined model including HAQ-DI alongside BASFI, HAQ-DI lost statistical significance, and no functional variable reached significance. Despite this, model fit (adjusted R2) remained essentially unchanged.
Discussion
The present study provides novel real-world evidence on factors predicting the difficult-to-manage phenotype in axSpA. Overall, we found that functional impairment, as reflected by higher HAQ-DI or MDHAQ functional scores, was the main independent correlate of D2M status at both baseline and follow-up, while, surprisingly, no consistent effects were observed for demographic or inflammatory parameters. Notably, older age was linked to D2M status at baseline but did not independently predict incident D2M during follow-up. This suggests that age likely reflects accumulated disease burden, longer disease duration, previous treatment exposure, and comorbidity load at study entry rather than serving as a true long-term predictor of D2M development. Consistently, patients with D2M axSpA had significantly longer symptom and disease durations at baseline, supporting the idea that cumulative disease burden contributes to the appearance of a D2M phenotype. This finding aligns with previous real-world studies showing that longer disease duration and increased treatment exposure may raise the risk of D2M axSpA.4,5,8 In contrast, diagnostic delay was not associated with D2M status in our cohort, indicating that after starting targeted therapy, the long-term disease course may be more influenced by cumulative disease burden and treatment response than by the timing of the initial diagnosis.
The estimated prevalence of D2M axSpA in our cohort was 11% at baseline (cross-sectional assessment at treatment initiation). During follow-up, when D2M status was evaluated longitudinally as a dynamic outcome, the overall proportion of patients classified as D2M was 10.4% at week 24 and 8.8% at week 48, reflecting both persistent prevalent cases and incident cases emerging over time. These estimates were comparable to previously reported rates, which range between 9% and 23%, although fall at the lower end of this spectrum, potentially reflecting our setting in a highly specialized center with timely access to multiple biologic and targeted therapies, enabling earlier treatment optimization and switching.7,8,17 The declining frequency of D2M status over time may suggest management optimization or improved disease control, but may also be influenced by potential missing data during follow-up, which could affect the ability to meet the complete ASAS D2M definition.
To the best of our knowledge, studies specifically evaluating the predictive value of MDHAQ or HAQ-DI in D2M axSpA are currently lacking. To date, some cross-sectional data indicate that poorer health status is associated with D2M axSpA,4,8 although causal or temporal relationships remain uncertain. A recent real-world study from the Reuma-Check cohort did not identify HAQ-DI as a significant baseline predictor of ASAS-defined D2M. In fact, HAQ-DI did not significantly differ between D2M and non-D2M patients in that population, and ultrasound abnormalities emerged as the only independent predictor. 7 This discrepancy may reflect differences in case mix, disease characteristics, and methodological approach, including the systematic use of ultrasound to capture imaging-defined inflammatory burden, which may more directly reflect structural or inflammatory drivers of D2M. In contrast, in our cohort, functional impairment—captured by HAQ-DI and the MDHAQ functional score—was the strongest and most consistent correlate of D2M at baseline and early follow-up, suggesting that poor health reported by patients signals a difficult-to-manage trajectory even when inflammatory markers are not discriminatory.
Poor self-assessment of health status may reflect the cumulative consequences of structural damage, central pain sensitization, or physical deconditioning, rather than active inflammation alone; however, this remains a hypothesis that warrants further investigation in studies specifically designed to disentangle inflammatory and non-inflammatory contributors to D2M status. Surprisingly, psychological parameters derived from the MDHAQ did not show a significant or consistent association with D2M status. This may partly be explained by the relatively short observation period or the limited ability of the MDHAQ psychological component to accurately capture specific constructs such as depression or anxiety, and it is possible that functional limitation itself mediates much of the psychological burden, making direct effects of mood or stress less apparent in multivariable models.
From a clinical perspective, our findings highlight the importance of interpreting poor health status scores within a broader, multidimensional framework. A persistently unfavorable functional scores should prompt clinicians to consider non-inflammatory contributors to a difficult-to-manage state, allowing earlier intervention with physical therapy, pain education, or psychological support in addition to pharmacologic treatment. Such a muldimodal, patient-centered approach may prevent unnecessary escalation of targeted therapy in the absence of active inflammation, while improving long-term outcomes and patient satisfaction. Future research should focus on validating these findings in larger, multicenter cohorts across various healthcare settings. Developing integrated prediction models that combine functional measures, clinical indices, and imaging parameters may enhance early detection of patients at risk of D2M status. Additionally, prospective interventional studies are necessary to assess whether early strategies targeting functional impairment and patient-reported health status can change the course of the disease.
Limitations
Our study has several limitations. First, we were not able to assess some tools specifically developed for axial spondyloarthritis, such as the ASAS Health Index (ASAS-HI), 18 which is not yet routinely available in our daily clinical practice. However, HAQ-DI and MDHAQ remain commonly used tools for evaluating patient-reported outcomes across rheumatic diseases; therefore, our findings still provide valuable additional insight into health status in patients with axSpA. In our primary analyses, HAQ-DI and the functional dimension of MDHAQ were selected as measures of functional impairment because they capture both axial and peripheral limitations, as well as broader daily-life functional burden, which may be particularly relevant in a real-world cohort with mixed manifestations. In sensitivity analyses that included BASFI alongside HAQ-DI, the latter lost statistical significance, and no functional variable remained significant. This likely reflects collinearity between BASFI and HAQ-DI, as both instruments capture overlapping aspects of axial function. Despite this, model fit (adjusted R2) remained essentially unchanged, indicating that inclusion of BASFI does not materially improve the explanatory power of the model. Importantly, HAQ-DI and MDHAQ are routinely collected in our registry and provide a broader, patient-centered assessment of functional impairment, whereas BASFI was not consistently available for all patients. Therefore, we believe that HAQ-DI and MDHAQ remain the most practical and interpretable functional predictors for identifying patients at risk of D2M axSpA in this real-world cohort.
Another limitation concerns the retrospective application of the recently proposed ASAS definition of D2M axSpA to previously collected real-world data. Although all key components of the definition were available, the study was not originally designed to evaluate the D2M construct; therefore, some elements—particularly treatment failure and management difficulties perceived by physicians or patients—may not have been documented with the same level of detail as in studies specifically designed to assess D2M axSpA. In this analysis, the unit of analysis was the treatment course rather than the individual patient, since the goal was to identify predictors of D2M axSpA at the start of specific therapies. Due to the exploratory nature of the study and the relatively small sample size, standard logistic regression models assuming independence of treatment courses were used, although within-patient correlation cannot be completely ruled out. Additionally, the observed reduction in the proportion of patients classified as D2M axSpA at later time points may reflect clinical improvement but could also be partly influenced by missing data and attrition during follow-up, potentially leading to an underestimation of D2M cases at weeks 24 and 48. Nonetheless, the primary analyses focused on baseline predictors, and the association between functional impairment and D2M axSpA remained consistent across different time points, supporting the robustness of the main findings.
Another limitation is that treatment-refractory axSpA could not be formally evaluated because detailed data on why treatments were discontinued or switched were not systematically recorded in the registry. As a result, we could not determine whether the observed D2M phenotype truly indicated treatment refractoriness or was influenced by treatment changes caused by poor overall health, comorbidities, or other factors unrelated to efficacy. This restricts a more precise understanding of the mechanisms underlying D2M axSpA. A larger sample size, particularly at follow-up, as well as a larger D2M cohort, would allow for more reliable analyses and results.
Conclusion
In summary, our study is the first to demonstrate that functional impairment, reflected by higher HAQ-DI and MDHAQ scores, is the strongest predictor of D2M axSpA and may therefore serve as a valuable clinical tool for the early identification of these patients and the timely initiation of targeted nonpharmacological management strategies aimed at improving long-term outcomes.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261450527 – Supplemental material for Patients with poorer health status are more likely to have difficult-to-manage axial spondyloarthritis: insights from a real-world cohort
Supplemental material, sj-docx-1-tab-10.1177_1759720X261450527 for Patients with poorer health status are more likely to have difficult-to-manage axial spondyloarthritis: insights from a real-world cohort by Zofia Guła, Mateusz Wilk, Piotr Kuszmiersz, Magdalena Strach and Mariusz Korkosz in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors thank the staff of the Department of Rheumatology and Immunology at Jagiellonian University Medical College for their assistance with patient care and data collection. They also express their gratitude to all patients who took part in this study. This study was financially supported by the Dean’s funds of Faculty of Medicine, Jagiellonian College.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.