
Abstract
Background:
The relationship between biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) and the incidence of interstitial lung disease (ILD) in patients with rheumatoid arthritis (RA) remains unclear.
Objective:
To investigate the influence of b/tsDMARDs on the development of ILD in patients with RA, particularly in Asian patients.
Design:
Retrospective cohort study.
Methods:
We examined data from patients with seropositive RA who had no prior ILD between January 1, 2010, and October 31, 2022, utilizing the Nationwide Korean Health Insurance Review and Assessment database. Cohort A consisted of individuals initiating b/tsDMARDs, while Cohort B included those starting conventional DMARDs, including individuals who subsequently began b/tsDMARDs. Patients were observed from the medication index date until the onset of ILD, death, or the conclusion of the study. In Cohort A, multivariate Cox proportional hazards analysis was conducted, followed by propensity score matching (PSM) analysis. In Cohort B, a time-dependent Cox proportional hazards analysis was performed, accounting for methotrexate (MTX) pretreatment period.
Results:
In Cohort A (13,908 patients), the crude incidence rate (IR) of ILD was 3.05 per 1000 person-years. After multivariable adjustment and PSM, no statistically significant differences in ILD development were observed among the biologics classes, with hazard ratios (HRs) ranging from 0.81 to 1.19 when compared to tumor necrosis factor (TNF) inhibitors as a reference. In Cohort B (75,013 patients), the overall IR was 2.8 per 1000 person-years. Time-dependent multivariable Cox analysis, adjusting for baseline characteristics and MTX pretreatment duration, showed no statistically significant differences between biologic users and MTX maintainers (adjusted HR range: 0.74–1.29, all p > 0.05).
Conclusion:
No specific b/tsDMARDs consistently showed significant differences in ILD incidence compared to other b/tsDMARDs. Biologics showed no significant increase in the risk of ILD compared to MTX maintainers. TNF inhibitors performed similarly to non-TNF biologics and Janus kinase inhibitors in terms of ILD incidence.
Plain language summary
Although biologic or targeted synthetic antirheumatic drug (b/tsDMARD) have improved the prognosis of RA, it is unclear which one class is specifically more helpful or harmful. Utilizing the extensive Nationwide Korean Health Insurance Review and Assessment (HIRA) database, which covers nearly the entire Korean population, this retrospective observational cohort study included two distinct cohorts: Cohort A, comprising patients initiating b/tsDMARD therapy after at least one year on cDMARDs, and Cohort B, consisting of patients starting cDMARDs with or without subsequent transition to b/tsDMARDs. Over a mean follow-up duration of approximately four years in both cohorts, multivariate Cox proportional analysis followed by propensity score matching analysis in Cohort A, and a time-dependent multivariate Cox analysis accounting for the methotrexate pretreatment period in Cohort B, did not show any specific class is better or worse in terms of the incidence of ILD.
Keywords
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease that affects extra-articular organs, such as the lungs. Recent advancements in biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) have markedly improved the prognosis of patients with RA, enhancing their quality of life and diminishing disability rates. 1 Despite these therapeutic advances, interstitial lung disease (ILD) remains a significant extra-articular manifestation of RA, with substantial morbidity and mortality and limited effective treatment or prevention options. 2
The incidence of ILD in patients with RA has been increasingly recognized because of its profound implications for patient outcomes. 3 The landscape of RA treatment has undergone a dramatic transformation since the introduction of bDMARDs in the early 2000s, prompting investigations into their possible effects on the occurrence of ILD. 4 Early case reports raised concerns about potential ILD exacerbation with tumor necrosis factor (TNF) inhibitors, leading to uncertainty about their safety profile in this context.
However, as the therapeutic options diversified to include various non-TNF bDMARDs and tsDMARDs in the 2010s, recent real-world data have provided more nuanced perspectives. For instance. A recent nationwide study observed that while the absolute number of RA-ILD cases may be increasing due to the aging population and extended survival of RA patients, the actual incidence and prevalence rates of ILD have remained stable. 4 Furthermore, a recent comprehensive meta-analysis demonstrated that the use of biologic agents may actually act as a protective factor against the development of RA-ILD.5,6
Historically, the use of methotrexate (MTX), the anchor drug for RA, was also heavily debated due to early fears of pulmonary toxicity. However, a recent paradigm shift supported by accumulating evidence suggests that MTX is not associated with an increased risk of chronic ILD and may even exert a protective effect. 7 Despite this changing perspective on conventional therapies and the encouraging population-level trends in the post-biologic era, comprehensive evaluation of the incidence of ILD across various classes of b/tsDMARDs in direct comparison with conventional agents, such as MTX, are still lacking. This is particularly relevant given that TNF is often the initial biological choice for patients with RA, and clinicians need evidence-based guidance on whether concerns about ILD should influence this therapeutic decision.
The investigation of the association between b/tsDMARDs and the incidence of ILD in Asians is also scarce, despite evidence suggesting a higher ILD incidence in Asian RA patients than in Caucasian populations.
Therefore, this study aimed to determine the frequency of ILD in Asian patients with RA who received various types of DMARDs, including b/tsDMARDs and conventional DMARDs (cDMARDs), and to identify which class of drugs reduces the risk of ILD.
Methods
Data source
This retrospective cohort study utilized the Health Insurance Review and Assessment Service (HIRA) database in South Korea, which covers approximately 97% of the population and includes comprehensive information on treatment, diagnosis, and related tests of patients. The Korean health insurance system incorporates a special payment scheme for chronic, intractable, and rare diseases. Once registered, hospital costs are co-paid by the government to reduce the economic burden on affected individuals. Since 2009, patients with RA, particularly seropositive RA, who had either rheumatoid factor or anti-cyclic citrullinated peptide antibody and were diagnosed according to the 1997 American College of Rheumatology (ACR) criteria or the 2010 criteria of the ACR/EULAR, 8 have been included in this framework. This national registration improved diagnostic accuracy and ensured homogeneity of the disease cohort by mitigating the inclusion of patients with ambiguous diagnoses. Data were accessed and analyzed through the cooperation of the Korean HIRA with the project name HIRA research data (M20230602001). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 9 (Supplemental Checklist).
Eligibility criteria
The study population comprised patients with seropositive RA aged 19 years and older who transitioned from cDMARDs to bDMARDs or tsDMARDs between January 1, 2010, and October 31, 2022 (Cohort A; Figure 1). Eligible patients were treated with cDMARDs for a minimum of 1 year before initiating b/tsDMARD therapy. Patients with ILD confirmed before or within 28 days of starting the study drug were excluded to prevent counting ILD cases that occurred before study participation. In this study, only the incidence of ILD after index drug initiation was considered.
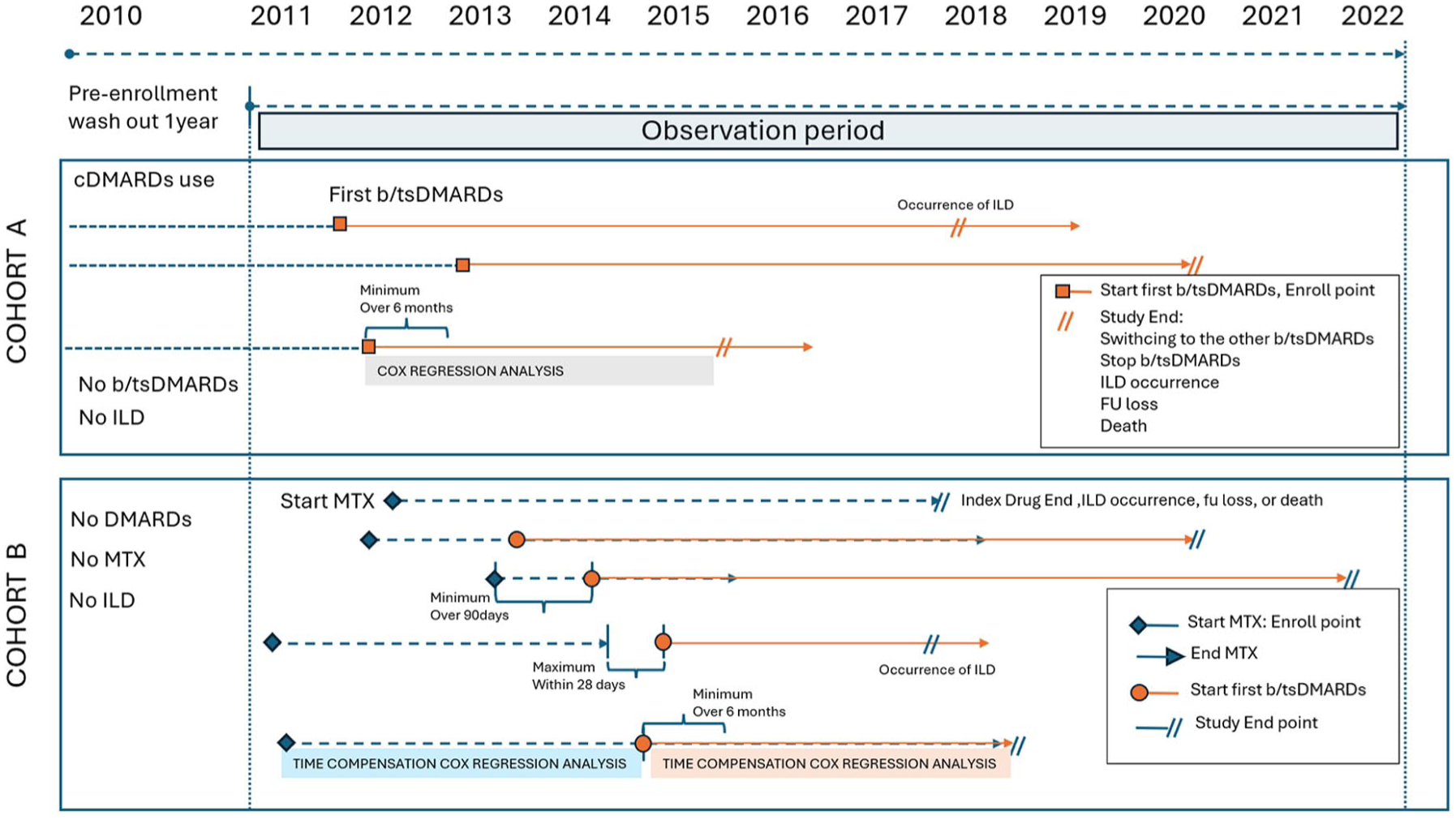
Study design diagram. For a comprehensive understanding of the inclusion criteria, please refer to the “Methods” section and Supplemental Materials.
b/tsDMARDs were classified into five categories: TNF inhibitors, Janus kinase inhibitors (JAK), B-cell inhibitors (rituximab, RIT), interleukin-6 inhibitors (tocilizumab, TOC), and T-cell inhibitors (abatacept, ABA). The study followed patients from the initiation of the new drug to the earliest occurrence of the following events: ILD, study end, death, switching to another class of b/tsDMARDs, or 90 days after stopping the index drug (extended to 180 days for RIT cessation).
Moreover, we established another cohort comprising patients who initiated cDMARD therapy to evaluate the relative impact of each specific b/tsDMARD class compared with that of MTX. Cohort B consisted of individuals newly initiated on cDMARDs. The patients were classified into five groups: those who transitioned from MTX to b/tsDMARDs, which were further divided based on the specific b/tsDMARD-initiated (TNF, JAK, TOC, ABA), and those who maintained their MTX-based cDMARDs regimen (MTX group). Notably, because RIT is not allowed to be used as a primary b/tsDMARD after failure of cDMARD treatment in Korea, its users were not included in Cohort B. The detailed inclusion and exclusion criteria and enrollment conditions are presented in the Supplemental Materials. Briefly, eligibility for this cohort required a minimum of 90 days of MTX administration in cDMARD-naïve patients. Transition to b/tsDMARDs had to occur within 28 days following the decision to start b/tsDMARDs after MTX discontinuation, with a prerequisite of at least 180 days of follow-up after initiating b/tsDMARDs (Figure 1).
Patients with other autoimmune diseases that could develop ILD, such as sarcoidosis, systemic scleroderma, inflammatory myositis, granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, or microscopic polyangiitis, were excluded from both cohorts. Patients with idiopathic pulmonary fibrosis were also excluded based on the presence of the International Classification of Diseases, Tenth Revision (ICD-10) code J84.18 or the special payment calculation system registry V-codes of the Korean Ministry of Health and Welfare. Patients who were administered RIT for lymphoproliferative or other hematologic and non-hematologic diseases were excluded.
Outcomes and risk factors
ILD occurrence was defined according to the ICD-10, specifically the J84 category (Supplemental Table 1), requiring at least two outpatient visits spaced over 30 days with ILD diagnosis supported by chest computed tomography scans, pulmonary function tests, or lung biopsies within 180 days of diagnosis. This method of defining ILD has a sensitivity of 73.2% and a specificity of 98.2%. 10
The following patient demographics and clinical characteristics were collected for all patients: age, sex, Charlson comorbidity index (CCI) score, presence of chronic obstructive pulmonary disease (COPD), emphysema, Sjögren’s syndrome, use of immunosuppressive agents, MTX or non-MTX-based cDMARDs combination, average daily prednisolone equivalent dosage, smoking, yearly outpatient department (OPD) visit count, yearly hospitalization count, and facility location. These were assessed during 1 year prior to enrollment in Cohort A. In Cohort B, these characteristics were assessed during the period of 1 year after enrollment when they started MTX for the first time, because Cohort B included patients who initiated cDMARDs at the time of enrollment, compared to those in Cohort A who were enrolled during the phase of switching to b/tsDMARDs. We calculated CCI scores for each cohort, as it is the most widely used comorbidity index containing 19 factors, including diabetes with diabetic complications, congestive heart failure, peripheral vascular disease, chronic pulmonary disease, mild and severe liver disease, hemiplegia, renal disease, leukemia, lymphoma, metastatic tumor, and acquired immunodeficiency syndrome, each of which was weighted. 11
Ethics
This study was approved by the Severance Hospital Institutional Review Board (IRB; 4-2023-0467). The IRB waived the requirement for informed consent owing to the retrospective study design and analysis of de-identified patient data. This study used anonymized patient data and complied with the principles outlined in the Declaration of Helsinki.
Statistical analysis
Patient demographics, including sex, age, and underlying diseases, were assessed along with the CCI score, presence of COPD, emphysema, Sjögren’s syndrome, and medication history, focusing on cDMARDs, immunosuppressants, glucocorticoids, smoking, yearly OPD visit count, yearly hospitalization count, and location of the medical facility. 12 Categorical variables were analyzed using the Chi-square or Fisher’s exact test, as appropriate, and continuous variables were analyzed using the t-test or analysis of variance. The incidence of ILD among the various b/tsDMARD classes was compared using Cox proportional hazards models, delineating survival curves and estimating the incidence rates (IRs) and incidence rate ratios (IRRs). Univariate and multivariate Cox proportional analyses incorporating age, sex, smoking status, CCI score, presence of COPD or emphysema, Sjögren’s syndrome, use of MTX or immunosuppressive agents, average daily prednisolone equivalent dosage, yearly OPD visit count, yearly hospitalization count, and facility location were performed to calculate the crude and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs), with TNF in Cohort A as reference.
Subsequently, a propensity score-matched analysis of the ILD incidence between each b/tsDMARD and TNF (reference) user was conducted, controlling for the abovementioned demographic and clinical variables from Cohort A. The propensity score for the predicted probability of receiving b/tsDMARDs for each patient was estimated using a logistic regression model fitted with the aforementioned covariables. A nearest-neighbor-matching algorithm with a “greedy” heuristic was used to match patients based on the logit of their propensity score; matching occurred if the difference in the logit of the propensity scores was <0.2 times the standard deviation of the scores (caliper width). Cox proportional hazard models with pair-level random intercepts were used to assess the HR and 95% CI for developing ILD among RA patients treated with b/tsDMARDs compared with those treated with TNF. After matching, covariates with a standardized mean difference >0.2 were adjusted in the final model.
In Cohort B, a time-dependent Cox proportional hazard analysis, incorporating MTX pretreatment duration as a time adjustment, was performed to assess the comparative effects of MTX versus each b/tsDMARD class. We considered ILD to be linked to previous cDMARD treatment if it manifested within 28 days after transitioning from a cDMARD-based regimen to a b/tsDMARD-based regimen, considering the possibility of a diagnostic delay rather than the immediate impact of the new index drug. Univariate and multivariate time-dependent Cox proportional hazards analyses were conducted.
Statistical analyses were conducted using SAS 9.4 Enterprise Guide (SAS Institute, Cary, NC, USA). All 95% CI and p-values were based on two-sided hypothesis tests, with p < 0.05 considered statistically significant.
Results
Study population
In Cohort A, 13,908 b/tsDMARD-naïve patients (11,381 women and 2527 men; mean age, 54.3 ± 12.7 years) were administered the index drug as their first b/tsDMARD for at least 6 months. Among them, 7993 patients received TNF as their first b/tsDMARD, 3042 received JAK, 1595 received TOC, 1246 received ABA, and 32 received RIT (Table 1, Figure 2). Cohort B comprised 75,013 patients (17,519 men and 57,494 women; mean age, 54.9 ± 13.3 years) who initiated MTX therapy and were monitored for the continuation of MTX-based treatment. Among these, 8493 patients transitioned from the MTX-based regimen to the b/tsDMARD regimen (Table 1).
Demographic characteristics of Cohort A and B.

ANOVA test.
Chi-square test.
In Cohort A, 1 year before enrollment. In Cohort B, 1 year after enrollment.
Fisher’s exact test.
cDMARDs: MTX, leflunomide, hydroxychloroquine, sulfasalazine, and bucillamine.
Immunosuppressive agents: azathioprine, tacrolimus, and cyclosporine.
Prednisolone dose: all glucocorticoid dosages used were converted into prednisone equivalent doses.
ABA, abatacept; CCI, Charlson comorbidity index; cDMARDs, conventional disease-modifying antirheumatic drugs; COPD, chronic obstructive pulmonary disease; ILD, interstitial lung disease; JAK, JAK inhibitor; MTX, methotrexate; OPD, outpatient department; RIT, rituximab; SD, standard deviation; TNF, TNF inhibitor; TOC, tocilizumab.

Study flow diagram.
Patient characteristics of ILD patients in Cohort A and the incidence
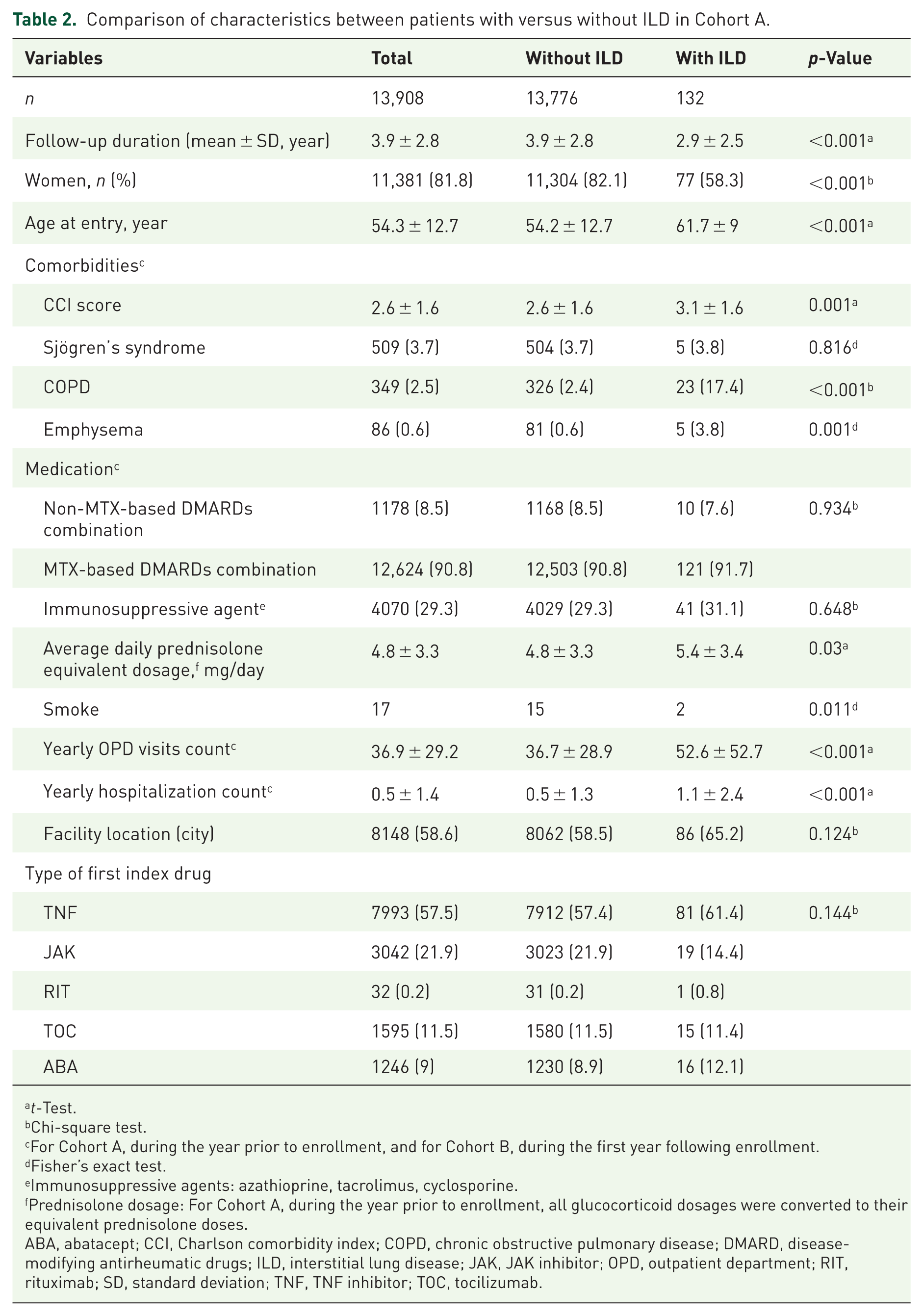
Patients in Cohort A who developed ILD were older, more likely to be male, had higher CCI scores, more frequently had COPD or emphysema, used higher prednisolone doses, and had more outpatient visits and hospitalization compared to those who did not develop ILD (Table 2).
Comparison of characteristics between patients with versus without ILD in Cohort A.
t-Test.
Chi-square test.
For Cohort A, during the year prior to enrollment, and for Cohort B, during the first year following enrollment.
Fisher’s exact test.
Immunosuppressive agents: azathioprine, tacrolimus, cyclosporine.
Prednisolone dosage: For Cohort A, during the year prior to enrollment, all glucocorticoid dosages were converted to their equivalent prednisolone doses.
ABA, abatacept; CCI, Charlson comorbidity index; COPD, chronic obstructive pulmonary disease; DMARD, disease-modifying antirheumatic drugs; ILD, interstitial lung disease; JAK, JAK inhibitor; OPD, outpatient department; RIT, rituximab; SD, standard deviation; TNF, TNF inhibitor; TOC, tocilizumab.
During 53,602 person-years of follow-up, 132 patients (1.0%) developed ILD in Cohort A, yielding an overall IR of 3.05 (95% CI: 1.99–4.68) per 1000 person-years. The incidence by drug class was 1.0% (n = 81), 0.6% (n = 19), 0.9% (n = 15), 1.3% (n = 16), and 3.1% (n = 1) in TNF, JAK, TOC, ABA, and RIT users, respectively. The IR for each b/tsDMARDs class was as follows: TNF users, 2.26; JAK users, 2.72; TOC users, 2.41; ABA users, 3.62; and RIT users, 4.91. With TNF as the reference, the IRRs for ILD were 1.2 (0.73–1.98) for JAK, 1.07 (0.61–1.85) for TOC, 1.60 (0.94–2.74) for ABA, and 2.17 (0.3–15.6) for RIT (Table 3).
IR, IRR, and HR for ILD in each of the five class users in Cohorts A.

Patients with events per 1000 person-years.
Adjusted for age (⩾50 years), gender, presence of COPD, emphysema, Sjögren’s syndrome, Charlson comorbidity index score (⩾2), use of an immunosuppressive agent, MTX-based cDMARDs combination, average daily prednisolone equivalent dosage (⩾5 mg/day), yearly outpatient department visit count (⩾36/year), yearly hospitalization count (⩾1/year), and facility location (city).
ABA, abatacept; cDMARDs, conventional disease-modifying antirheumatic drugs; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; ILD, interstitial lung disease; IR, incidence rate; IRR, incidence rate ratio; JAK, JAK inhibitor; NA, not applicable; RIT, rituximab; TNF, TNF inhibitor; TOC, tocilizumab.
Multivariate Cox analysis and propensity score matching in Cohort A
After multivariable adjustment for age, sex, comorbidities, and medication-related variables, no statistically significant differences in ILD risk were observed across b/tsDMARD classes compared to TNF (adjusted HR range: 0.81–1.37; all p > 0.05; Table 3). In the Cox model, older age (>50 years), male sex, smoking, COPD, and higher yearly hospitalization count were independently associated with ILD development (Table 4). The Kaplan–Meier curves did not reveal significant differences in the survival outcomes across each b/tsDMARD class (Supplemental Figure 1).
Result of Cox’s proportional hazard model of Cohorts A (n = 13,908).

Adjusted for categorized variables of age (⩾50 years), sex, presence of COPD, emphysema, Sjögren’s syndrome, CCI score (⩾2), use of an immunosuppressive agent, MTX-based cDMARDs combination, average daily prednisolone equivalent dosage (⩾5 mg/day), yearly OPD visit count (⩾36/year), yearly hospitalization count (⩾1/year), and facility location (city). All covariates were evaluated in the year preceding enrollment.
Immunosuppressive agents: azathioprine, tacrolimus, and cyclosporine.
Prednisolone dose: all glucocorticoid dosages were converted into prednisone equivalent doses.
**p < 0.01. ***p < 0.001.
ABA, abatacept; b/tsDMARDs, biologic and targeted synthetic disease-modifying antirheumatic drugs; CCI, Charlson comorbidity index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; ILD, interstitial lung disease; JAK, JAK inhibitor; MTX, methotrexate; N/A, not applicable; OPD, outpatient department; RIT, rituximab; TNF, TNF inhibitor; TOC, tocilizumab.
In the propensity score matching (PSM) analysis, rituximab was omitted because of the small sample size, which led to unbalanced matching. The analysis, with TNF as the reference, revealed no statistically significant differences in the adjusted HR for ILD among the various b/tsDMARDs (Figure 3).

HRs from Cohort A, propensity score matching with TNF as reference, 1:1.
ILD incidence in Cohort B
During a follow-up period encompassing 346,804 person-years, 912 patients (1.22%) in Cohort B developed ILD, resulting in an overall IR of 2.8 (95% CI: 2.23–3.51) per 1000 person-years. Within this cohort, 853 patients (1.28%) in the MTX group and 59 patients (0.69%) in the b/tsDMARD group developed ILD. In each DMARD class, IR was as follows: 1.92 (1.33–2.78) for TNF, 2.78 (1.58–4.9) for JAK, 3.23 (1.79–5.83) for TOC, 3.76 (1.88–7.53) for ABA, and 2.65 (2.47–2.83) for MTX. Upon comparing the IRs between the MTX group and each b/tsDMARD group, the relative IRRs were 0.73 (0.5–1.06), 1.05 (0.59–1.86), 1.22 (0.67–2.21), and 1.42 (0.71–2.85) for the TNF, JAK, TOC, and ABA groups (Table 5).
IR, IRR, and HR for ILD in each of the five class users in Cohorts B.
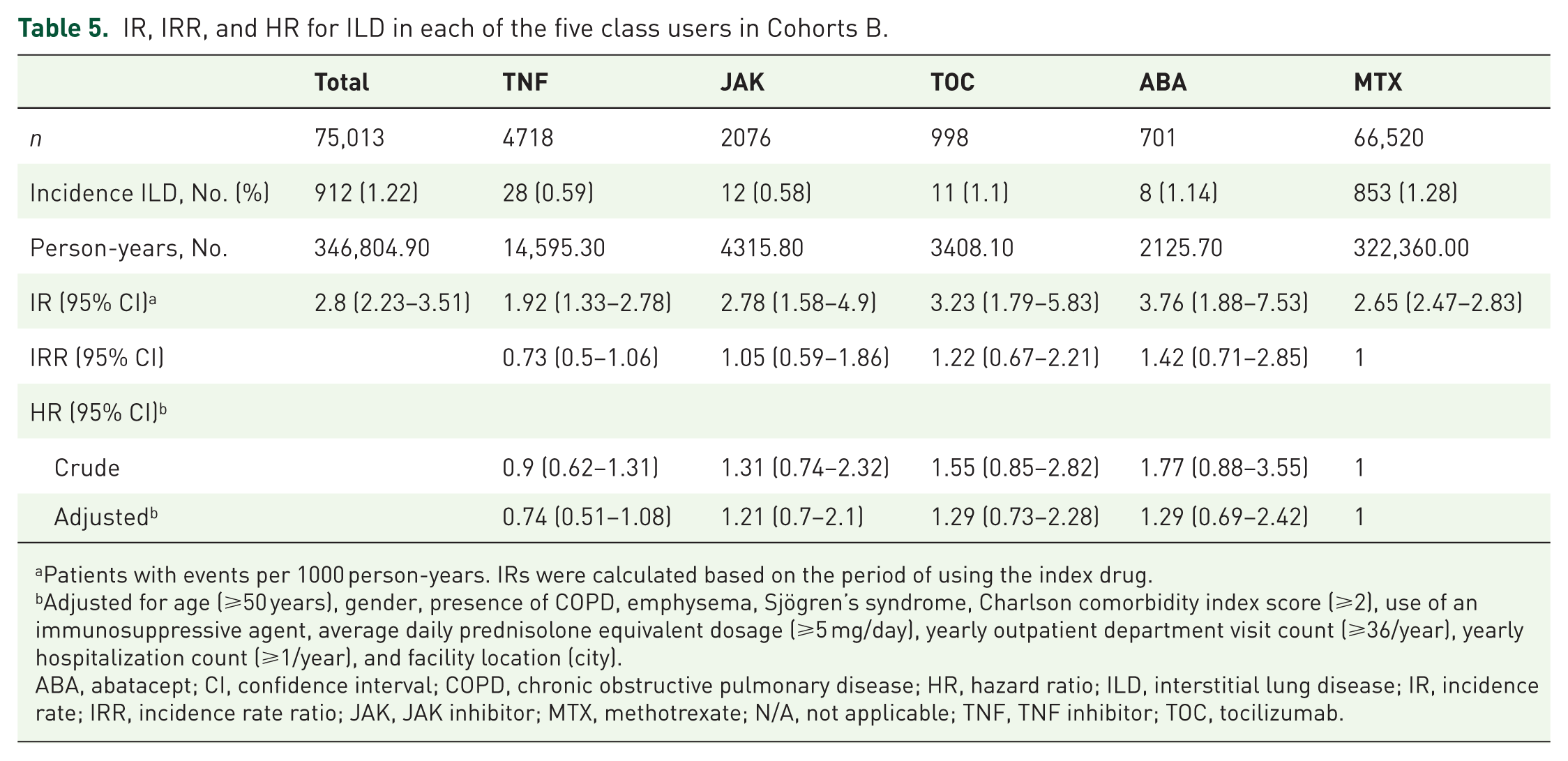
Patients with events per 1000 person-years. IRs were calculated based on the period of using the index drug.
Adjusted for age (⩾50 years), gender, presence of COPD, emphysema, Sjögren’s syndrome, Charlson comorbidity index score (⩾2), use of an immunosuppressive agent, average daily prednisolone equivalent dosage (⩾5 mg/day), yearly outpatient department visit count (⩾36/year), yearly hospitalization count (⩾1/year), and facility location (city).
ABA, abatacept; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; ILD, interstitial lung disease; IR, incidence rate; IRR, incidence rate ratio; JAK, JAK inhibitor; MTX, methotrexate; N/A, not applicable; TNF, TNF inhibitor; TOC, tocilizumab.
HR from time-dependent Cox regression analysis of Cohort B
In the multivariable analysis that included demographic and clinical factors, the HRs for ILD from a time-dependent Cox model, which accounted for the duration of MTX pretreatment, were as follows: 0.74 (0.51–1.08) for TNF, 1.21 (0.7–2.1) for JAK, 1.29 (0.73–2.28) for TOC, and 1.29 (0.69–2.42) for ABA (Table 5). The results indicated no statistically significant difference between patients initiating b/tsDMARDs and those maintaining MTX treatment (overall adjusted HR for b/tsDMARDs users: 0.90 (95% CI: 0.69–1.16)). In addition to sex, age, smoking, presence of COPD, and yearly hospitalization count, which were statistically significant in Cohort A, the daily prednisolone dose, use of immunosuppressive agents, and yearly OPD visit count also affected ILD incidence in Cohort B (Table 6). Kaplan–Meier curves did not reveal significant differences in survival outcomes across the b/tsDMARDs classes (Supplemental Figure 2).
Result of time-dependent Cox’s proportional hazard model of Cohort B (n = 75,013).
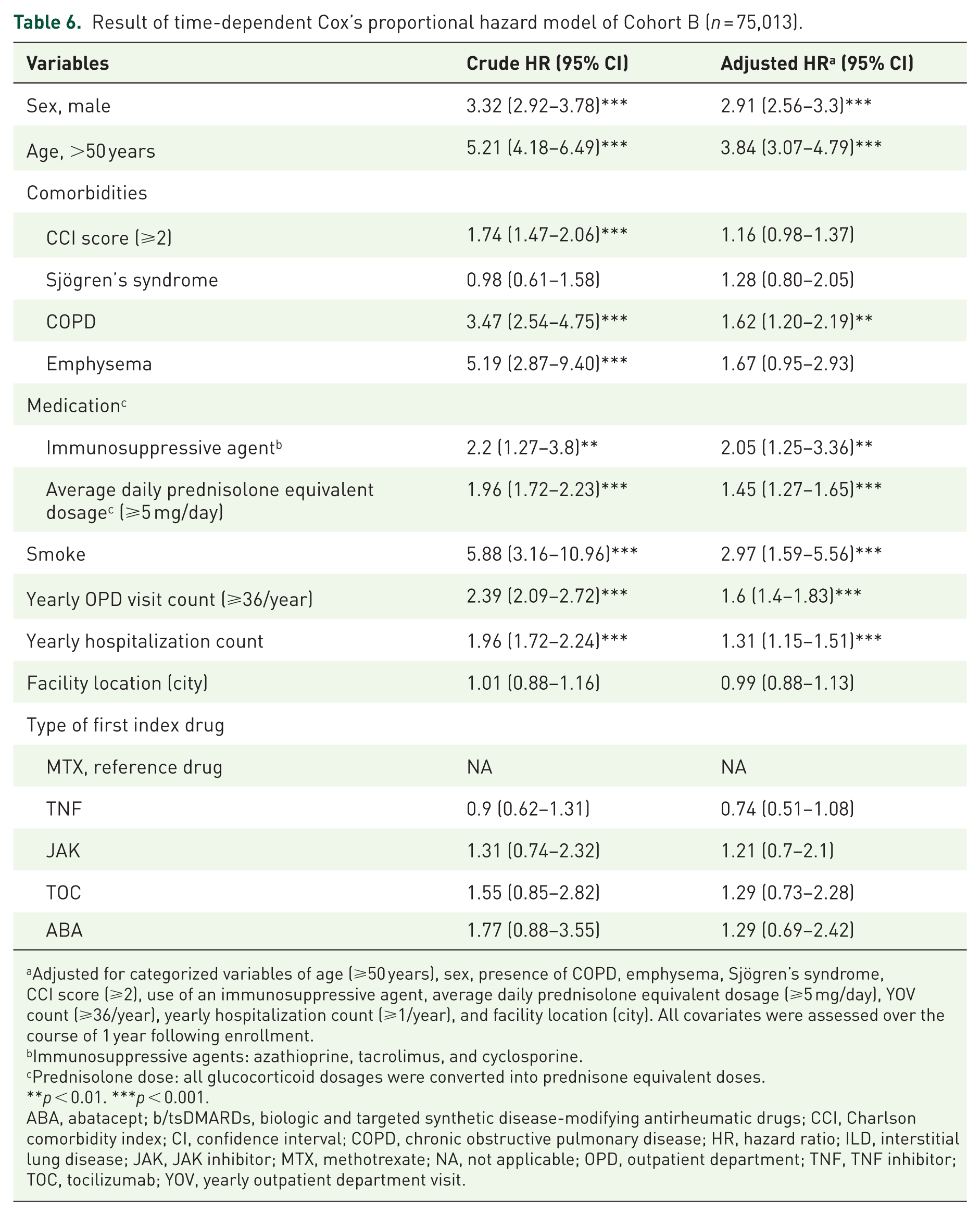
Adjusted for categorized variables of age (⩾50 years), sex, presence of COPD, emphysema, Sjögren’s syndrome, CCI score (⩾2), use of an immunosuppressive agent, average daily prednisolone equivalent dosage (⩾5 mg/day), YOV count (⩾36/year), yearly hospitalization count (⩾1/year), and facility location (city). All covariates were assessed over the course of 1 year following enrollment.
Immunosuppressive agents: azathioprine, tacrolimus, and cyclosporine.
Prednisolone dose: all glucocorticoid dosages were converted into prednisone equivalent doses.
**p < 0.01. ***p < 0.001.
ABA, abatacept; b/tsDMARDs, biologic and targeted synthetic disease-modifying antirheumatic drugs; CCI, Charlson comorbidity index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; ILD, interstitial lung disease; JAK, JAK inhibitor; MTX, methotrexate; NA, not applicable; OPD, outpatient department; TNF, TNF inhibitor; TOC, tocilizumab; YOV, yearly outpatient department visit.
Discussion
In this study, we assessed the incidence of ILD and the factors contributing to an increased ILD risk among patients with RA who were administered various b/tsDMARDs. Our findings showed that, overall, no specific b/tsDMARDs exhibited significant differences in HR compared to the other b/tsDMARDs for ILD in either Cohort A or B. Among the various b/tsDMARDs classes, no specific class showed consistently significant differences in the incidence of ILD in both cohorts.
In relation to the different patterns of ILD occurrence between cohorts in our study, compared to Cohort A, Cohort B can be considered the early cohort, as it included patients who were initiators of MTX, which can be assumed to have participated in the study at an earlier stage than the initiators of biologics. In addition, Time-dependent Cox regression analysis was performed in Cohort B, comparing MTX (a representative cDMARD) users with switchers from an MTX-based regimen to b/tsDMARD-based treatment while adjusting for MTX pretreatment duration before b/tsDMARD initiation. We believe that this approach enabled survival analysis by aligning diverse patient populations to the same set of observation starting points, thereby mitigating the potential impact of disease duration on ILD incidence. Thus, our comprehensive analysis, including propensity matching in Cohort A and time-dependent Cox regression analysis in Cohort B, consistently showed that no specific biologics were better in terms of ILD incidence. JAK was not better than other biologics. Our study, which focused on an Asian cohort, provides unique insights into the prevalence and risk factors of ILD in patients with RA treated with b/tsDMARDs. Notably, our findings showed a different pattern compared to that of studies using predominantly Caucasian cohorts, where a lower ILD incidence was reported for the JAK inhibitor tofacitinib use when comparing each b/tsDMARD in US claims data. Baker et al. 13 showed that tofacitinib significantly decreased adjusted HR for ILD to 68% compared to adalimumab in their claim database cohort study. They reported that the frequency of ILD in tofacitinib users was the lowest in a prevalent new user cohort after PSM. However, in our Cohort A, with similar enrollment conditions for b/tsDMARD initiators, the ILD incidence was not lower in the JAK group than in the TNF group. This difference in the results among Koreans might stem from differences in ethnic or genetic backgrounds. However, we believe that the incidence of ILD in JAK users was not overestimated in this study. In our study, the IR of ILD in JAK users was 2.72 and 2.78 per 1000 person-years in Cohorts A and B, respectively, consistent with the results of a post hoc analysis of 21 clinical trials of RA treatment with tofacitinib. 14 This analysis reported a relatively higher incidence of ILD in Asians than in Caucasians, with rates of 0.26 (95% CI: 0.14–0.44) for Asians and 0.15 (95% CI: 0.09–0.22) for Caucasians per 100 person-years, respectively. 14 Again, these differences highlight the potential impact of ethnic variations on drug responses and ILD onset. Our incidence also agreed with the ILD incidence from the ORAL Surveillance trial, which was 2.9 per 1000 person-years in the tofacitinib 5 mg twice daily group (95% CI: 0.16–0.48). 15 Generally, Asian ancestry is regarded as a risk factor for ILD, and the higher incidence of ILD in Asian patients than in Caucasian patients may be attributable to genetic factors and susceptibility. 16 Therefore, ethnically diverse studies are important for better understanding the pathophysiological mechanisms underlying ILD in various populations.
Regarding the impact of non-TNF biologics and tsDMARDs on ILD, many studies have focused on the progression or stabilization of prevalent ILD cases. While there are some early reports of TNF worsening ILD in a few cases, this was not always true, as many patients with ILD continued TNF use without switching, and other biologics also had similar reports of some patients developing or worsening existing ILD.17–19 However, many experts still support a cautious approach to selecting TNF for RA patients with ILD.20–22 In a retrospective study evaluating JAK inhibitors in patients with RA-ILD, approximately 16% experienced ILD progression, 65%–73% maintained stable pulmonary function, and 16%–19% showed improvement over 18 months. 23 A systematic review of abatacept in RA-ILD confirmed similar findings, reporting imaging improvement or stabilization rates of 76.6%–92.7%. 24 In rituximab-treated patients, a single-center study over a prolonged follow-up period showed that 52% remained stable, 16% improved, and 32% progressed, with the majority of progressive cases having severe ILD at baseline. 25 Similarly, in a multicenter retrospective study of 28 RA-ILD patients treated with tocilizumab for a mean of 30 months, Forced Vital Capacity (FVC) remained stable in 56% and improved in 20%, while Diffusing Capacity of the Lungs for Carbon Monoxide (DLCO) showed similar patterns (56% stable, 20% improved), with High-Resolution Computed Tomography (HRCT) remaining stable in 89% of cases. 26 These response distributions—approximately 10%–20% showing worsening, 50%–70% maintaining stability, and 10%–20% experiencing improvement—across different b/tsDMARD classes (abatacept, rituximab, tocilizumab, and JAK inhibitors) are further confounded by heterogeneous individual patient characteristics, underlying disease biology, genetic factors, and baseline disease severity to lead definite conclusion about the choice of the drug. These findings align with our observation that no single b/tsDMARD demonstrated overwhelming superiority or inferiority in preventing new-onset ILD in our cohort.
Limitations
Our study had some limitations. This retrospective cohort study may not have accounted for all potential confounding factors. To address this limitation, we examined the cohorts using PSM and time-dependent Cox regression analysis, along with well-defined enrollment and exclusion criteria, as well as thorough outcome verification to emulate the target trial. Numerous risk factors have been identified for ILD in patients with RA, including older age, male sex, smoking, Asian ethnicity, and higher disease activity.2,27,28 While our study highlights the impact of older age, smoking, and male sex, we could not account for disease activity, as in many other investigations based on retrospective claims data. However, it is important to note that under the Korean National Health Insurance system, with specific threshold criteria for DAS28 and joint erosions for b/tsDMARD reimbursement eligibility, there is no differential coverage or hierarchical selection among b/tsDMARD classes based on disease activity severity. Once the minimum eligibility criteria were met, the selection of specific b/tsDMARDs was not systematically influenced by the degree of disease activity, potentially reducing the channeling bias related to disease severity in our analysis. Furthermore, our analyses were adjusted for surrogate markers of disease activity, such as cumulative corticosteroid dosage as average daily dose, frequency of hospital visits or hospitalizations, and the combination of immunosuppressive agents. Additionally, we could not fully analyze the dynamic changes in concomitant MTX use (i.e., continuation vs discontinuation) after the initiation of b/tsDMARDs in Cohort B. Because Cohort B consisted of prevalent MTX users, the vast majority (>96%) initiated biologics as an add-on therapy, lacking sufficient baseline variance. Furthermore, attempting to adjust for the duration of concomitant MTX use during follow-up introduced significant survival bias and reverse causality, as patients who develop respiratory symptoms or ILD are more likely to discontinue MTX immediately. Exploring this dynamic treatment trajectory would require complex causal inference modeling, which was beyond the computational scope of this large-scale claims database study. Second, as the NHIS claims database does not contain imaging or histopathological data, ILD subtype classification (e.g., UIP, NSIP) was not possible. However, this is a recognized limitation common to claim-databased epidemiological studies. ILD and RA case identification in our cohort relied on validated algorithms using diagnostic codes, and prescription records, which, by their nature, cannot distinguish radiologic or histologic subtypes. Third, we were unable to conduct a more comprehensive examination of smoking behaviors, such as through quantitative analyses or by differentiating between former and current smokers, because of the characteristics of the database based on claims data. However, smoking was identified as a significant risk factor in this study. Finally, a definitive investigation into the impact of RIT on ILD incidence was precluded by the limited number of first uses of the drug per the current guidelines, which prevented the acquisition of sufficient data for a comprehensive analysis. However, the findings from both cohorts and the statistical analysis support the hypothesis that no specific b/tsDMARDs were worse than the others.
Conclusion
In summary, our retrospective cohort study using Korean national registry data found that b/tsDMARDs users did not have a higher incidence of ILD than MTX users. Non-TNF biologics or JAK showed no better results than TNF in terms of ILD incidence. Further studies are needed to determine the complex association between b/tsDMARDs and RA-ILD in different ethnic groups.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261453781 – Supplemental material for Incidence of interstitial lung disease in seropositive rheumatoid arthritis patients receiving biologics, Janus kinase inhibitors, or methotrexate
Supplemental material, sj-docx-1-tab-10.1177_1759720X261453781 for Incidence of interstitial lung disease in seropositive rheumatoid arthritis patients receiving biologics, Janus kinase inhibitors, or methotrexate by Jiyeol Yoon, Minkyung Han, Jason Jungsik Song, Sang-Won Lee, Inkyung Jung and Yong-Beom Park in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X261453781 – Supplemental material for Incidence of interstitial lung disease in seropositive rheumatoid arthritis patients receiving biologics, Janus kinase inhibitors, or methotrexate
Supplemental material, sj-docx-2-tab-10.1177_1759720X261453781 for Incidence of interstitial lung disease in seropositive rheumatoid arthritis patients receiving biologics, Janus kinase inhibitors, or methotrexate by Jiyeol Yoon, Minkyung Han, Jason Jungsik Song, Sang-Won Lee, Inkyung Jung and Yong-Beom Park in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
Data were accessed and analyzed through the cooperation of Korean Health Insurance Review and Assessment Service (HIRA) with the given project name as HIRA research data (M20230602001).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.