
Abstract
Background:
Hand osteoarthritis (HOA) is a prevalent degenerative joint disorder that causes pain, functional disability, and considerable socioeconomic burden. China’s rapid population aging and widespread engagement in repetitive manual labor may have accelerated to the rise of HOA. However, long-term trends and future projections of its disease burden remain insufficiently characterized.
Objective:
To describe trends in HOA incidence, prevalence, and DALYs from 1990 to 2021, examine differences across age and sex, and project future disease burden.
Design:
A population-based descriptive study using GBD 2021 data to examine trends and project the burden of hand osteoarthritis in Chinese adults aged 30 years and older across national and subnational regions.
Methods:
Age-standardized incidence rate (ASIR), prevalence rate (ASPR), and disability-adjusted life year rate (ASDR) were analyzed by sex and age group. Temporal trends were quantified using Joinpoint regression to calculate annual and average annual percent changes (APC, AAPC), and future trends were projected to 2036 using an autoregressive integrated moving average (ARIMA) model.
Results:
Between 1990 and 2021, the burden of HOA increased substantially worldwide, with China showing a faster rise than the global average. In China, ASIR rose from 59.12 to 92.70 per 100,000, ASPR from 988.51 to 1603.85, and ASDR from 31.57 to 51.26, corresponding to AAPCs of 1.46%–1.58%. Females experienced consistently higher rates than males and faster growth. The disease burden rose sharply after age 50 and peaked between 65 and 79 years. Joinpoint analysis revealed multiple inflection points, with the steepest acceleration occurring from 2015 to 2019 (APC >5%). ARIMA projections indicate that male rates will plateau or slightly decline by 2035, whereas female rates will continue rising, potentially exceeding 150 per 100,000 for incidence and 3000 per 100,000 for prevalence.
Conclusion:
The burden of HOA in China is increasing rapidly and is likely associated with population aging, sex-specific biological vulnerability, and occupational exposure. Women and elderly adults are disproportionately affected, with widening sex and age disparities. Targeted interventions—including ergonomic protection, menopausal health management, and early rehabilitation—are essential to mitigate the projected rise in disease burden and to improve musculoskeletal health in an aging population.
Plain language summary
Hand osteoarthritis is a common condition where the joints in the fingers and thumbs break down, causing pain and stiffness that can make daily tasks difficult. As China’s population gets older and people use their hands intensively for both manual jobs and digital devices like smartphones, this problem is getting much worse. A new study looked at data from 1990 to 2021 to understand how widespread and severe hand osteoarthritis has become in China. The findings show a fast and significant increase. The number of new cases, the total number of people living with the condition, and its overall impact on people’s lives and health have all nearly doubled over those 30 years. This rise in China has been faster than the global average. The burden of this disease is not shared equally. Women are affected more often and more severely than men, and the gap is widening. For everyone, the risk increases sharply after age 50, with the highest rates seen in adults aged 65 to 79. The fastest period of increase happened very recently, between 2015 and 2019. Using this data, researchers forecast trends to 2036. They predict that while the rate for men may level off, the number of women developing and living with hand osteoarthritis will continue to climb significantly. The main drivers behind this rising trend are the aging population, hormonal changes after menopause in women, repetitive hand use in certain jobs, and the widespread use of digital technology. To address this growing public health challenge, the study suggests that targeted steps are needed. These include promoting hand-friendly work tools and habits, providing better health support for women around menopause, and offering early rehabilitation programs. Taking action is crucial to reduce future pain and disability and improve the quality of life for China’s aging population.
Introduction
Osteoarthritis (OA) is the most common degenerative joint disorder worldwide and a leading cause of chronic pain, disability, and reduced quality of life among adults. Hand osteoarthritis (HOA), a major subtype of OA, is characterized by progressive cartilage degradation, osteophyte formation, and functional impairment of the hands. According to the 1990 diagnostic criteria of the American College of Rheumatology, the diagnosis of HOA is based on hand pain, soreness, or stiffness together with characteristic clinical features involving the distal interphalangeal (DIP), proximal interphalangeal (PIP), carpometacarpal (CMC), and metacarpophalangeal (MCP) joints. 1
In China, the combined effects of rapid population aging and widespread engagement in repetitive manual labor—particularly in manufacturing, agriculture, and handicrafts—may have contributed to a steady rise in the burden of HOA. The incidence of cases of Chinese patients requiring rehabilitation increased from 4.38 million in 1990 to 10.98 million in 2019. 2 Beyond direct medical costs, HOA leads to pain, reduced dexterity, and work-related disability, and it often causes psychological distress and social withdrawal. The indirect economic burden, including loss of productivity and early retirement, represents more than 40% of total costs and exerts a significant impact on families and society.3,4
Although progress has been made in understanding the metabolic, hormonal, and occupational factors that contribute to HOA, comprehensive analyses of its long-term trends in China remain scarce. Most existing studies rely on data collected before 2019 and provide limited insight into recent demographic and regional patterns or the evolving disease trajectory in the context of population aging. To address these gaps, this study analyzes the changing burden of HOA in China over the past three decades using the most recent national-level data. We examine how the incidence, prevalence, and disability-adjusted life years (DALYs) associated with HOA have evolved between 1990 and 2021, explore differences across age and sex groups, and project the likely trajectory of disease burden in the coming years. These findings are expected to support early screening, preventive strategies, and optimized resource allocation for the management of HOA in an aging society.
Methods
Study design and data sources
This population-based descriptive study investigated long-term trends and future projections of HOA in China from 1990 to 2021. The analysis followed the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) to ensure methodological transparency. Data were obtained from the Global Burden of Disease Study 2021 (GBD 2021), which provides standardized estimates of disease incidence, prevalence, and DALYs across 204 countries and territories.
For China, national and subnational data were extracted for 31 provinces, autonomous regions, and municipalities directly under the Central Government, as well as the Hong Kong and Macao Special Administrative Regions (excluding Taiwan). The indicators included incidence, prevalence, and DALYs, along with their corresponding age-standardized rates—namely, the age-standardized incidence rate (ASIR), age-standardized prevalence rate (ASPR), and ASDR. Because GBD does not report HOA estimates for individuals younger than 30 years, analyses were restricted to adults aged 30 years and older.
Definition and modeling framework
Within the GBD analytical framework, HOA is defined as a degenerative joint disorder diagnosed by established clinical or radiographic criteria. Non-fatal outcomes, including pain and functional impairment, were estimated using the Bayesian meta-regression model DisMod-MR 2.1, which synthesizes evidence from peer-reviewed studies, population surveys, hospital records, and health system data. The model incorporates hierarchical smoothing across age, time, and geography to ensure consistency, while spatiotemporal Gaussian process regression was applied to improve precision in data-sparse regions. Estimates were harmonized across symptomatic and radiographic osteoarthritis to produce comparable and comprehensive results.
Uncertainty quantification and stratification
Uncertainty was addressed using GBD’s standard 1000-draw simulation method, with the 2.5th and 97.5th percentiles representing the 95% uncertainty intervals (UIs). All results are presented as mean values with 95% UIs. Analyses were stratified by sex (male, female) and age group (in 5-year intervals from 30 to 95+ years). Regional comparisons were conducted, where available, to identify geographic heterogeneity in HOA burden across China.
Statistical analysis and projections
All statistical analyses were performed using R software (version 4.4.3). Temporal trends in incidence, prevalence, and DALYs were assessed using the Joinpoint regression model (Joinpoint Regression Program, version 5.3.0). Joinpoints, representing statistically significant inflection points, were detected by a grid search algorithm with Monte Carlo permutation testing. The annual percentage change (APC) and average annual percentage change (AAPC) with 95% confidence intervals (CIs) were calculated to quantify long-term changes.
Future trends were projected using an autoregressive integrated moving average (ARIMA) model based on the annual series of age-standardized rates. This time-series approach accounts for autocorrelation and non-stationarity, providing reliable forecasts of short- to medium-term dynamics. Non-stationary time series were transformed to stationarity using differencing. ARIMA model parameters (p, d, q) were selected by minimizing the Akaike and Bayesian information criteria to balance model fit and complexity. Model adequacy was assessed using residual diagnostics. The Ljung–Box test was applied to the residuals with a lag of 10 to detect any remaining autocorrelation; all models yielded non‑significant results (p > 0.05), supporting model adequacy. The final ARIMA model specifications (p, d, q) for each sex and outcome are provided in Supplemental Table 1, and the corresponding Ljung–Box test results are detailed in Supplemental Table 2. Sensitivity analyses were conducted by varying the autoregressive and moving average orders (p and q ± 1) around the optimal model to evaluate the robustness of projections. Projections for 2022–2036 were generated to visualize potential changes in HOA incidence, prevalence, and DALYs among Chinese adults.
Visualization and ethical considerations
All visualizations were produced in R using the ggplot2, dplyr, and sf packages. Temporal changes were illustrated through line graphs with 95% UIs, and spatial patterns were displayed as choropleth maps of provincial-level estimates. All data used were publicly available and de-identified; no individual-level or confidential information was accessed. Therefore, ethical approval and informed consent were not required for this research.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 5
Results
Overall burden of hand osteoarthritis in China and globally
From 1990 to 2021, the ASIR, ASPR, and ASDR of HOA showed consistent increases both globally and in China (Table 1, Supplemental Table 3). Globally, ASIR rose from 100.57 (95% UI: 74.51–128.13) to 119.09 (95% UI: 88.73–151.13) per 100,000, with an AAPC of 0.54% (95% CI: 0.52–0.57; p < 0.05). During the same period, the global prevalence rate increased from 1944.84 to 2237.78 per 100,000 (AAPC = 0.44%, 95% CI: 0.39–0.49), while the DALY rate rose from 61.67 to 70.94 per 100,000 (AAPC = 0.44%, 95% CI: 0.40–0.48) (Figure 1(a)–(c)).
Age-standardized incidence, prevalence, and DALY rates of hand osteoarthritis in China, 1990–2021.
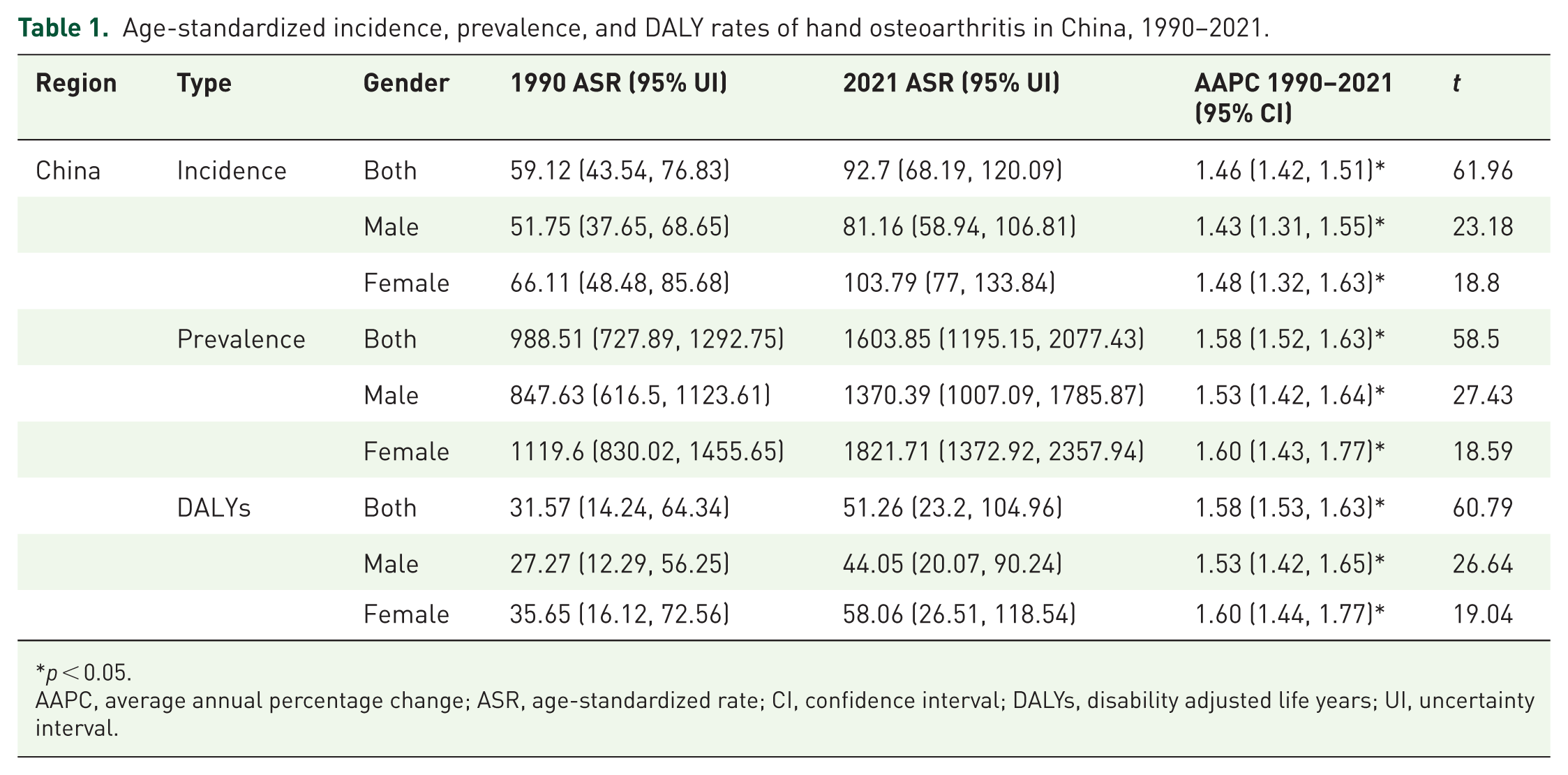
p < 0.05.
AAPC, average annual percentage change; ASR, age-standardized rate; CI, confidence interval; DALYs, disability adjusted life years; UI, uncertainty interval.
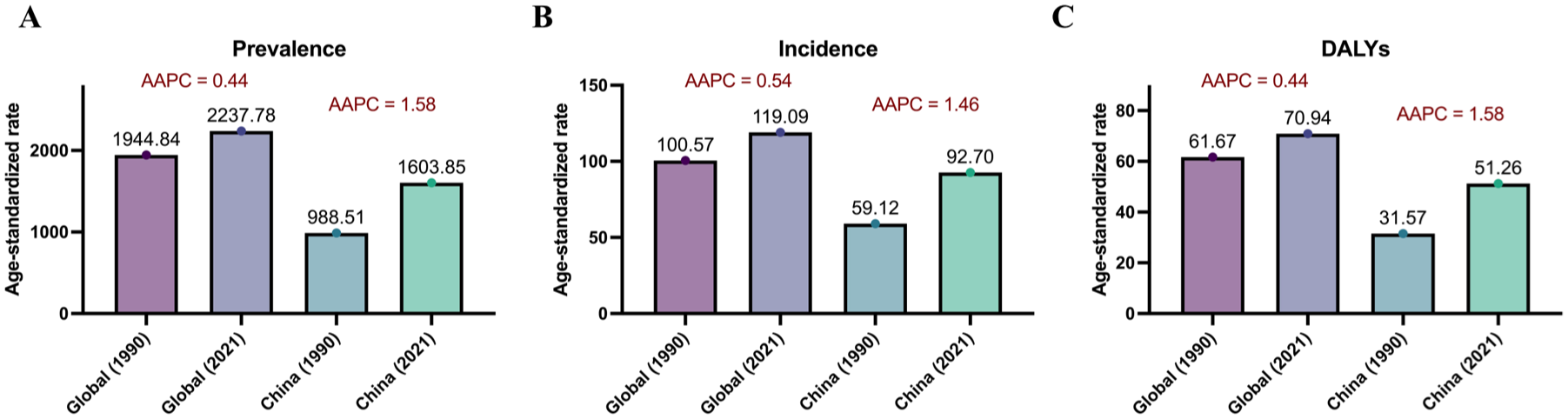
Temporal changes in the age-standardized rates of hand osteoarthritis globally and in China, 1990–2021. (a) ASPR of HOA in 1990 and 2021 for the global and Chinese populations. (b) ASIR of HOA during the same period. (c) ASDR for HOA.
In China, the HOA burden increased more rapidly than the global average. ASIR grew from 59.12 (95% UI: 43.54–76.83) to 92.7 (95% UI: 68.19–120.09), corresponding to an AAPC of 1.46% (95% CI: 1.42–1.51; p < 0.05). ASPR nearly doubled, from 988.51 to 1603.85 per 100,000 (AAPC = 1.58%, 95% CI: 1.52–1.63), and ASDR increased from 31.57 to 51.26 per 100,000 (AAPC = 1.58%, 95% CI: 1.53–1.63). All these increments were statistically significant (Figure 1(a)–(c)). Overall, China not only exhibited higher growth rates across all indicators but also a steeper increase among females than males, suggesting a substantial and accelerating disease burden over the past three decades.
Sex-specific differences in hand osteoarthritis burden
Females consistently experienced a higher HOA burden than males across all indicators and regions (Table 1, Supplemental Table 3, Figure 2(a)–(c)). In 2021, the global ASIR, ASPR, and ASDR among females were 150.77, 2,817.28, and 89.06 per 100,000, respectively—approximately 1.7–1.8 times those in males (86.09, 1585.11, and 50.62 per 100,000). In China, this disparity was even more pronounced, with female ASIR, ASPR, and ASDR of 103.79, 1821.71, and 58.06, compared with 81.16, 1370.39, and 44.05 in males, respectively. The AAPC also revealed faster growth among females from 1990 to 2021. Globally, the female AAPC values were 0.54%, 0.47%, and 0.46% for incidence, prevalence, and DALYs, all slightly lower than in males (0.54%, 0.48%, and 0.49%, respectively). In China, female AAPCs were consistently higher than male AAPCs for incidence, prevalence, and DALYs, reaching 1.48%, 1.60%, and 1.60%, respectively, compared with 1.43%, 1.53%, and 1.53% in males. These data indicate a persistently widening sex gap in disease progression over the past three decades. As visualized in Figure 2(d)–(f), female cases exceeded male cases in nearly all age groups, particularly between 55 and 79 years. The steeper increase in female ASPR and ASDR curves suggests that postmenopausal hormonal decline, longer life expectancy, and repetitive manual labor may contribute to the disproportionate HOA burden in women.
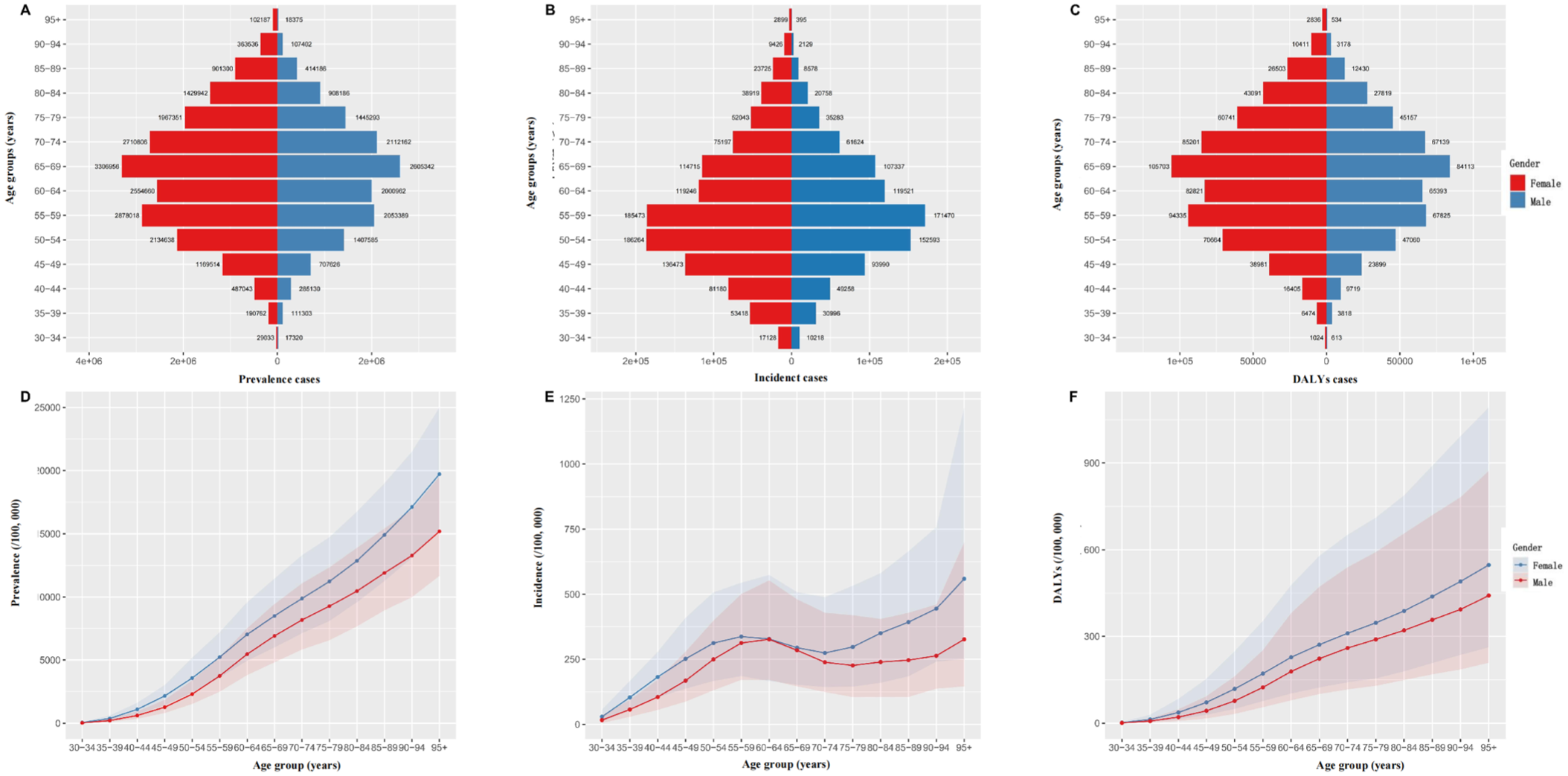
Age- and sex-specific distribution and trends of hand osteoarthritis in China, 2021. (a–c) Age- and sex-specific numbers of prevalent cases (a), incident cases (b), and DALYs (c) of HOA in China. Red bars represent females and blue bars represent males. (d–f) Corresponding ASPR (d), ASIR (e), and ASDR (f) per 100,000 population. Shaded areas indicate 95% uncertainty intervals.
Age-specific trends of HOA burden
The burden of HOA rose sharply with advancing age (Table 1, Supplemental Table 3, Figure 2(a)–(c)). In both sexes, disease rates remained low before age 40, followed by a steep increase thereafter. The number of prevalent and incident cases grew rapidly after age 50, peaking between 65 and 79 years, which together accounted for approximately one-third of the total cases nationwide. Among females, prevalence reached over 3.3 million in the 70–74-year group and 2.7 million in those aged 75–79 years, compared with 2.0–2.1 million in males in the same age bands.
The age-specific curves (Figure 2(d)–(f)) clearly demonstrated this accelerating pattern. The ASPR rose from fewer than 2,000 per 100,000 at ages 35–39 to more than 20,000 per 100,000 at ages 75–79—a tenfold increase. Similar upward trajectories were observed for ASIR and ASDR, both showing pronounced acceleration after age 60. DALYs followed the same pattern, increasing from under 100 per 100,000 in middle-aged adults to over 800 per 100,000 among those aged 90 and above. Overall, these findings confirm that aging is the strongest determinant of HOA burden. The rapid rise after midlife highlights the cumulative effects of joint wear, metabolic changes, and chronic inflammation associated with aging, suggesting that targeted prevention and early rehabilitation in middle-aged and elderly populations could substantially mitigate the disease impact.
Temporal trends of hand osteoarthritis burden in China
Joinpoint regression revealed that the overall burden of HOA in China increased significantly from 1990 to 2021, with multiple inflection points identified across incidence, prevalence, and DALY rates (Table 2, Figure 3(a), (d), (g)). For the total population, the ASIR remained relatively stable before 2000 (APC = 0.55%, 95% CI: 0.47–0.63) but rose sharply during 2000–2005 (APC = 2.89%, 95% CI: 2.78–3.01). A brief decline occurred between 2005 and 2010 (APC = –0.63%), followed by a renewed and accelerated increase from 2010 to 2019 (APC = 1.36%–5.51%) and a sustained upward trend thereafter (APC = 1.29%). The ASPR and ASDR followed similar trajectories, showing mild increases before 2000, steeper climbs between 2001 and 2005 (APC ≈ 3.6%), and the most rapid growth after 2015 (APC = 5.5%, p < 0.05), indicating that the HOA burden has accelerated markedly in the past decade.
Results of joinpoint regression model for the trend of hand osteoarthritis in China from 1990 to 2021.
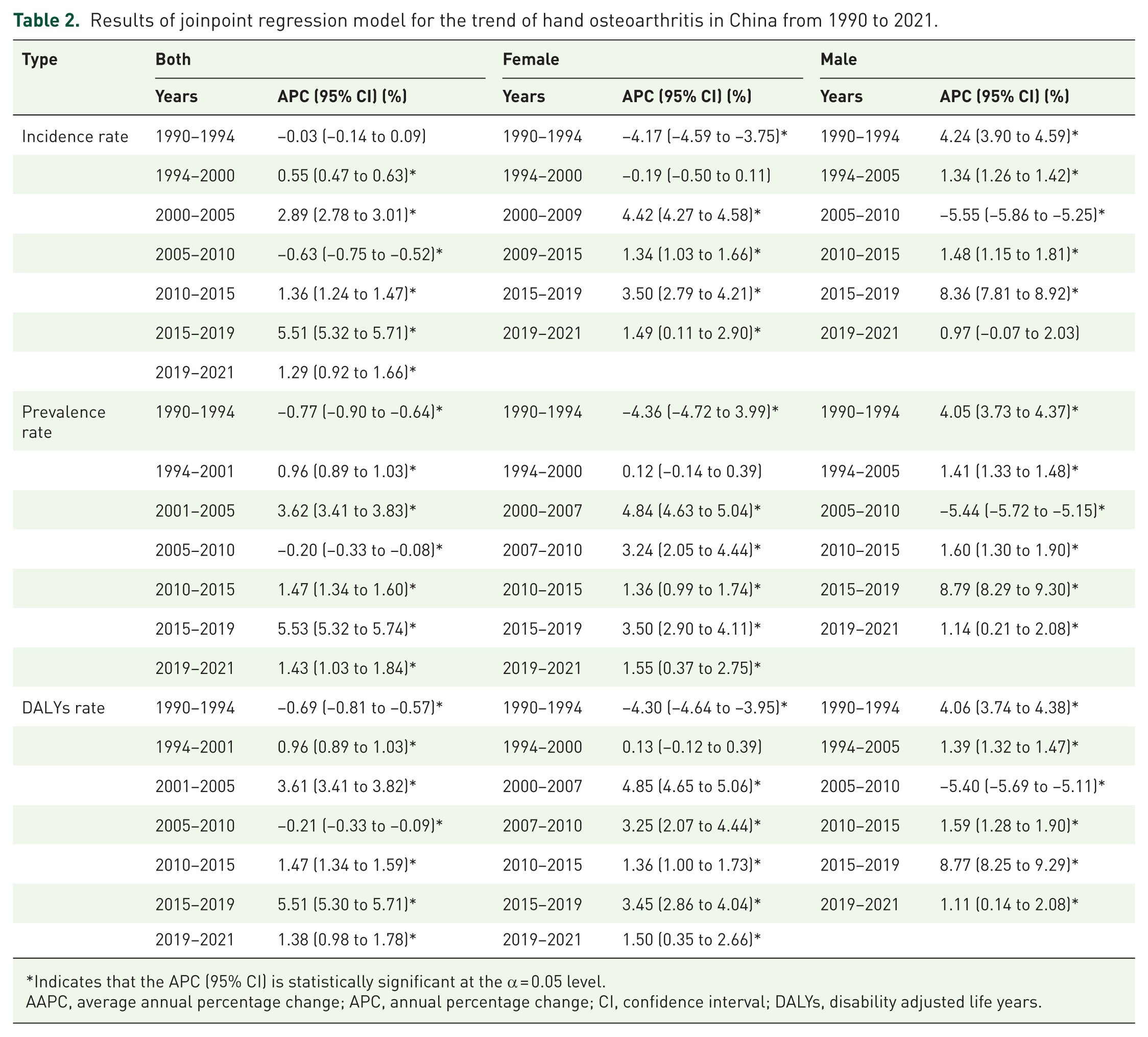
Indicates that the APC (95% CI) is statistically significant at the α = 0.05 level.
AAPC, average annual percentage change; APC, annual percentage change; CI, confidence interval; DALYs, disability adjusted life years.
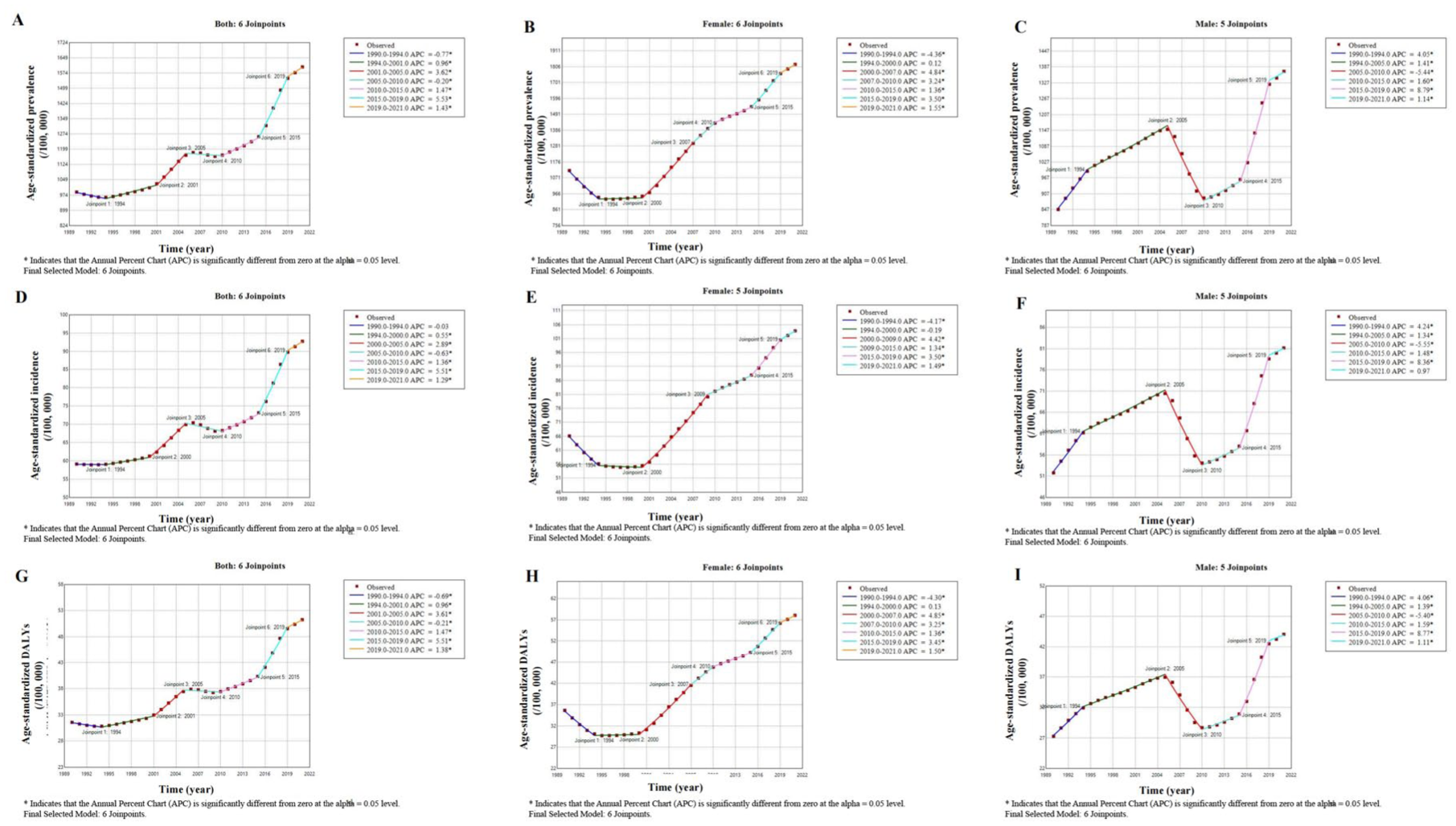
Temporal trends in ASPR, ASIR, and ASDR of hand osteoarthritis in China from 1990 to 2021 based on Joinpoint regression analysis. (a–c) Trends in the ASPR of HOA among both sexes (a), females (b), and males (c). (d–f) Corresponding ASIR for both sexes (d), females (e), and males (f). (g–i) ASDR for both sexes (g), females (h), and males (i).
Sex-specific analyses revealed distinct temporal patterns. Among females (Figure 3(b), (e), and (h)), the HOA burden increased continuously across all indicators. The ASIR rose rapidly between 2000 and 2009 (APC = 4.42%, 95% CI: 4.27–4.58) and maintained positive growth thereafter (2009–2015: 1.34%; 2015–2019: 3.50%). ASPR and ASDR exhibited similar upward trends, with sustained increases from 2000 to 2021 (APC range: 3.2–5.5%, all p < 0.05). In contrast, the male subgroup (Figure 3(c), (f), and (i)) displayed a more fluctuating pattern: incidence and prevalence increased in the early 1990s (APC ≈ 4.2%), dropped significantly between 2005 and 2010 (APC ≈ –5.4 to –5.6%), and rebounded sharply after 2010, peaking between 2015 and 2019 (APC ≈ 8.4%–8.8%, p < 0.05). This rebound phase after 2010 was particularly evident for DALYs, highlighting renewed growth in disease-related disability among men.
Overall, the Joinpoint analysis identified five to six turning points (1994, 2000, 2005, 2010, 2015, and 2019) across all indicators, signifying dynamic transitions in HOA epidemiology. The most pronounced and synchronized rise occurred after 2015, with the AAPC for females exceeding 1.5% for incidence, prevalence, and DALYs (all p < 0.05), compared with approximately 1.4%–1.5% in males. These findings underscore an accelerating disease trend, particularly among women in recent years, emphasizing the growing need for age- and sex-targeted prevention strategies and early management in China.
Projected burden of hand osteoarthritis in China
The ARIMA-based forecast indicated distinct sex-specific trajectories in the future burden of HOA in China (Figure 4(a)–(f)). For males, all three indicators—ASIR, ASPR, and ASDR—are expected to plateau or slightly decline after peaking around 2025 (Figure 4(a)–(c)). Specifically, the male ASIR is projected to decrease from approximately 86 per 100,000 in 2021 to around 70 per 100,000 by 2035, while the ASPR may fluctuate between 1500 and 2,000 per 100,000 with a gradually widening UI. Similarly, the ASDR in men is forecasted to stabilize near 60 per 100,000, indicating a potential slowdown in disease-related disability among males in the coming decade.
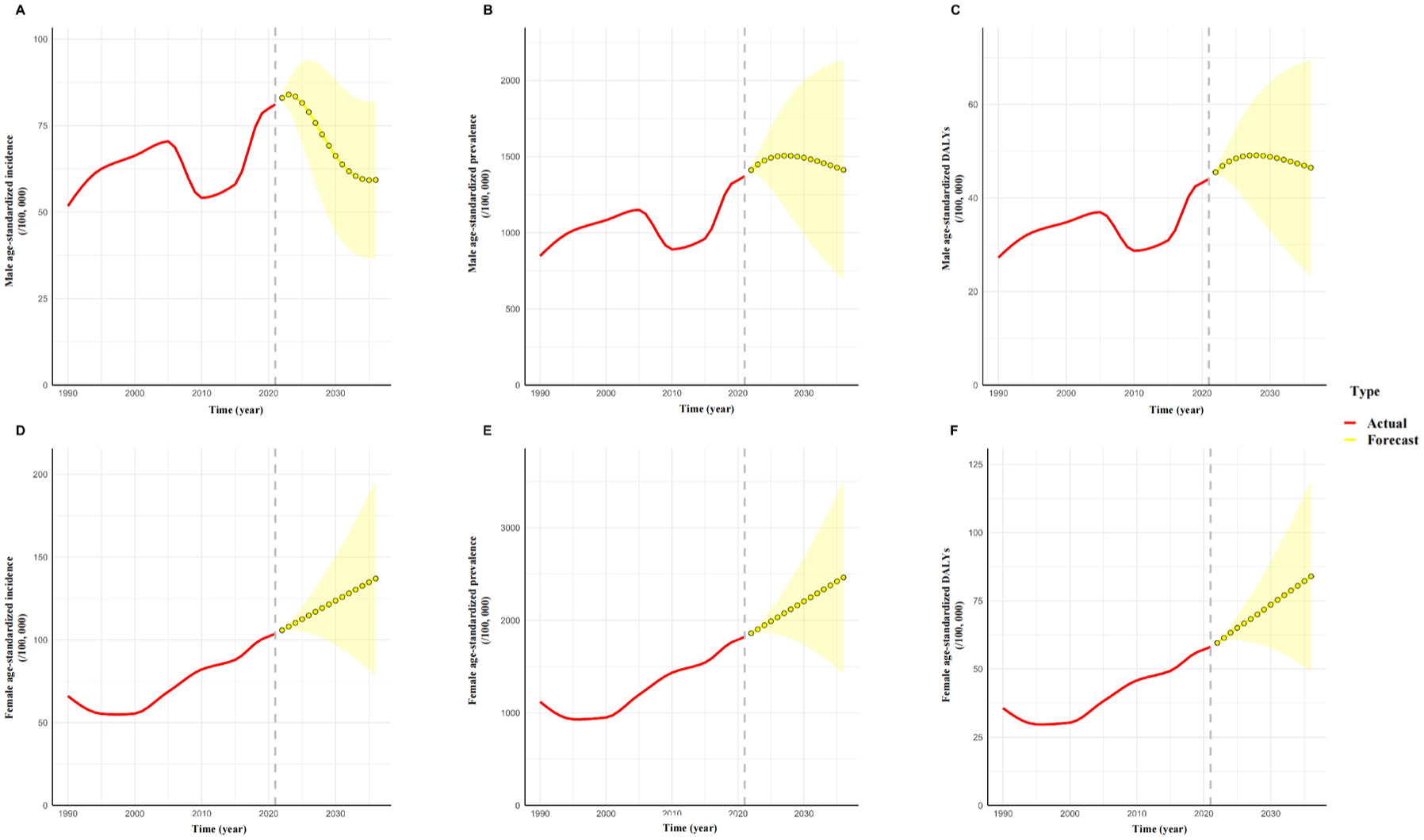
Projected trends in ASPR, ASIR, and ASDR of hand osteoarthritis in China from 1990 to 2036 based on ARIMA modeling. (a–c) ASIR (a), ASPR (b), and ASDR (c) of HOA among males from 1990 to 2021, with projections to 2036. (d–f) Corresponding ASIR (d), ASPR (e), and ASDR (f) for females.
In contrast, the female HOA burden is projected to continue increasing steadily across all indicators (Figure 4(d)–(f)). The female ASIR is estimated to rise from ~104 per 100,000 in 2021 to nearly 150 per 100,000 by 2035, while ASPR could surpass 2500–3000 per 100,000 in the same period. The corresponding ASDR is expected to exceed 100 per 100,000, with an expanding confidence range suggesting persistent upward uncertainty. The sustained rise among females aligns with the long-term acceleration observed in the Joinpoint analysis and may be partly explained by aging, hormonal factors, and occupational exposure. Overall, the predicted trends suggest a diverging trajectory between sexes—stabilization or mild decline in men versus continued escalation in women. The widening gap implies that future HOA-related healthcare demand will increasingly concentrate among elderly females. These findings underscore the importance of early lifestyle modification, ergonomic interventions, and community-level musculoskeletal health programs targeted specifically toward middle-aged and older women to mitigate the anticipated increase in disease burden.
Discussion
From 1990 to 2021, the global burden of HOA showed a steady increase, with a more pronounced rise observed in China. China’s HOA burden has increased rapidly over the past three decades, showing an accelerating trend compared with global patterns. Several factors may help explain this rapid growth, with population aging being a commonly cited explanation in previous studies. China’s proportion of individuals aged 60 years or older rose from 8.6% in 1990 to 18.9% in 2021, with an annual growth rate twice the global average. 6 Aging has been associated with impaired cartilage metabolism, and the elderly population tends to exhibit a higher burden of HOA in population-based studies. In addition, obesity has emerged as a potential contributor. The number of overweight and obese adults in China reached 402 million in 2021, ranking first globally, and the prevalence of obesity increased from 11.7% to 34.3% since 1990. 7 Excess adipokines have been reported to be associated with low-grade inflammation and increased mechanical stress on the joints, which may be relevant to cartilage degeneration described in previous research. 8 Occupational exposure also plays a critical role. Nearly 28% of China’s labor force—over 200 million individuals—is employed in manufacturing, with 70% engaged in repetitive manual labor. 9 Prolonged mechanical strain was associated with an approximately 3.2-fold higher risk of HOA compared with non-manual laborers. 10 In addition, frequent use of chopsticks in daily life may cause repetitive stress on the thumb interphalangeal and metacarpophalangeal joints. 11 Furthermore, early structural changes in HOA may be under-recognized when conventional radiography is used alone, because radiographic findings do not always fully capture early cartilage abnormalities.1,12 By contrast, in high-income countries, the HOA burden has possibly plateaued partly because of early screening and preventive education. Overall, the epidemiological shift in China indicates a transition from low to high incidence, suggesting that targeted prevention—particularly for elderly women—is essential to prevent surpassing global disease levels.
Globally, substantial regional heterogeneity persists, closely related to socioeconomic development, population aging, and lifestyle factors. HOA burden is highest in high-income and aging societies such as Nordic countries, where long life expectancy and comprehensive medical systems yield higher recorded DALYs. This reflects not only the true disease burden but also improved case detection of non-fatal conditions. Conversely, Mediterranean countries exhibit relatively low HOA prevalence, potentially linked to long-term adherence to a diet rich in fiber, vitamin K, and vitamin D, which may exert protective effects. In contrast, sub-Saharan Africa and South Asia report low HOA rates largely because of underdiagnosis rather than genuine scarcity. Short life expectancy, young population structure, and competing health priorities such as infectious diseases and limited healthcare access contribute to substantial underreporting. 13 Hence, the apparent global imbalance in HOA burden partly mirrors disparities in healthcare infrastructure and data completeness.
Women consistently bear a greater HOA burden than men both globally and within China, where the sex gap is particularly pronounced. Hormonal, anatomical, and sociocultural factors collectively contribute to this disparity. After menopause, estrogen decline diminishes cartilage protection, increases inflammation, and enhances matrix metalloproteinase activity.10,14 Moreover, women show higher genetic susceptibility for HOA-related variants. 15 In China, inadequate postmenopausal care exacerbates this vulnerability—among more than 230 million women over 50, only about 12% receive standard hormone therapy. Estrogen deficiency has been proposed to influence cartilage metabolism through pathways involving matrix metalloproteinase-13 (MMP-13). 10 Consistent with previous epidemiological reports, women over 50 tend to show a higher HOA risk than men of the same age. 16 Biomechanical factors further heighten susceptibility: women have smaller joint surfaces, looser ligaments, and weaker periarticular muscles, increasing exposure to microtrauma. 15 Occupational and domestic workloads reinforce this effect—women dominate in sectors such as nursing, education, and textile work, which require repetitive hand motions, and they spend two to three times longer on household tasks than men. In addition, women are more sensitive to pain and more likely to seek medical care,10,15 contributing to higher detection rates. Together, these factors produce a disproportionately higher HOA burden in women, both biologically and socially.
From 1990 to 2021, the overall HOA burden in China showed a continuous increase, with significant differences across sex and age. Sex divergence has deepened over time, influenced by demographic aging, shifting labor structures, and evolving health policies. Before 2005, the sex gap remained modest, shaped mainly by occupational roles—female-dominated light manufacturing and textile work caused moderate risk, while male-dominated heavy industry later contributed to higher male exposure. The turning point occurred around 2005, possibly coinciding with China’s rapid transition toward a service-oriented economy and expansion of healthcare coverage may have exposed more women to repetitive occupational strain and simultaneously may have improved case detection. Since then, accelerated aging, longer female life expectancy, and increased participation in repetitive-service jobs have resulted in a persistent rise in female burden. By 2021, women accounted for over half of China’s elderly population, and their HOA-related DALYs increased steeply, while automation and ergonomic advances may have mitigated men’s occupational risk.
Age-stratified patterns indicate that HOA predominantly affects middle-aged and elderly adults, especially women in the postmenopausal period. Aging leads to impaired cartilage repair, collagen loss, and sarcopenia, which increase joint vulnerability. 17 Repetitive microinjuries from earlier manual labor or housework may evolve into chronic joint pathology. 3 Comorbidities such as obesity and diabetes further exacerbate inflammation and bone remodeling 18 ; for instance, advanced glycation end products in diabetics promote fibrotic changes in articular cartilage. 8
In 2021, the HOA burden began to rise more noticeably in women around 50–54 years and in men around 55–59 years. These ages may represent a transition period during which sex-specific biological and occupational factors begin to exert a stronger influence on disease burden. 1 However, the greatest absolute case burden was concentrated in individuals aged 65–79 years, whereas the highest ASIR and ASDR were observed in the oldest age groups, particularly among those aged 90 years and above, likely reflecting the cumulative progression from joint stiffness to functional loss. 19 The modest decline in absolute case numbers after age 70 in some strata may partly reflect survival bias and reduced population size at older ages, 20 whereas the persistently elevated age-specific rates are consistent with the cumulative and progressive nature of cartilage degeneration. 21
The Joinpoint regression results further illuminate the dynamic progression of HOA in China. Between 1990 and 2021, ASIR, ASPR, and ASDR increased markedly, with the sharpest acceleration observed between 2015 and 2019—when male APCs exceeded 8%. This pronounced fluctuation in men was broadly consistent with previous GBD-based reports on osteoarthritis burden in China, which also suggested a more variable temporal pattern for male HOA than for female HOA.2,22,23 In women, the increase was more continuous and may be related to population aging, menopausal transition, and sustained exposure to repetitive hand use.24,25 In contrast, the male pattern was more distinctly V‑shaped: rapid growth before 2005, a notable decline from 2005 to 2010, followed by a subsequent rebound. The increase before 2005 may have been associated with rapid industrialization and expansion of labor-intensive occupations, which increased male exposure to repetitive hand loading and vibration.22,26 The decline during 2005–2010 may partly reflect strengthened occupational protection, industrial upgrading, and increasing mechanization and automation.27,28 The renewed rise after 2010, particularly during 2015–2019, may be related to cumulative occupational exposure in aging male workers, as well as rising metabolic risk factors such as obesity. 22 Nevertheless, because these estimates were derived from modeled GBD data, part of the magnitude of the observed swings may also reflect variation in data availability, reporting practices, and diagnostic ascertainment rather than true epidemiological shifts alone. Notably, the growth rate of HOA slowed after 2019, with the APC declining from over 5% to approximately 1.3%. As the data in this paper go up to 2021, encompassing the COVID-19 pandemic years (2020 and 2021), non-emergency medical services in China were substantially reduced during this time, which likely affected the diagnosis and recording of HOA cases.
Model-based projections suggest that China’s HOA burden will continue rising through 2036, with divergent trajectories between men and women. The male rates are expected to stabilize or decline slightly, while female rates will continue increasing across all indicators. Two factors may help contextualize these forecasts: rapid population aging—over 30% of the population will be aged ⩾60 years by 2035, 29 and improved diagnostic capabilities expanding case ascertainment. 30 The persistent female increase underscores the intersection of biological susceptibility, occupational exposure, and longevity. Conversely, male stabilization may reflect reduced mechanical workload and improved occupational ergonomics, although delayed care-seeking and underdiagnosis could obscure the true male burden. These findings highlight the need for sex-specific prevention: enhancing occupational protection and menopausal health care for women, while promoting early detection and rehabilitation for men.
Limitations
Several limitations should be considered when interpreting the findings of this study. The analysis is based on GBD 2021 estimates, which depend on modeled data and may be influenced by underreporting or variability in the diagnosis of HOA, particularly in rural or resource-limited settings. In addition, the use of aggregated national data limits the ability to explore regional heterogeneity, including potential differences between provinces or between urban and rural populations. Comparisons between China and global trends should be interpreted cautiously, as differences in healthcare systems, diagnostic capacity, and reporting practices may affect observed patterns. The restriction of the analysis to adults aged 30 years and older may also lead to an underestimation of the burden of early-onset HOA. While the ARIMA model was used to project future trends, these projections reflect extensions of past patterns and do not incorporate potential changes in health policy, healthcare access, or broader societal conditions. Finally, as this study is descriptive in nature, the observed patterns should be interpreted as epidemiological trends rather than evidence of direct causal relationships with occupational, hormonal, or other risk factors. As a descriptive study based on modeled GBD estimates, no formal sample size calculation or power analysis was performed.
Conclusion
In conclusion, the burden of HOA in China has steadily increased between 1990 and 2021, with higher rates in women and older adults. Age- and sex-specific differences have grown over time. Projections indicate that these trends are likely to continue, particularly among elderly women, highlighting the ongoing public health relevance of HOA.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261460128 – Supplemental material for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021
Supplemental material, sj-docx-1-tab-10.1177_1759720X261460128 for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021 by Yijia Gao, Lei Chen, Siwei Yang, Fengyuan Yu, Baoxuan Lin, Botao Zhou and Yingjun Nie in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-xlsx-1-tab-10.1177_1759720X261460128 – Supplemental material for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021
Supplemental material, sj-xlsx-1-tab-10.1177_1759720X261460128 for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021 by Yijia Gao, Lei Chen, Siwei Yang, Fengyuan Yu, Baoxuan Lin, Botao Zhou and Yingjun Nie in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-xlsx-2-tab-10.1177_1759720X261460128 – Supplemental material for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021
Supplemental material, sj-xlsx-2-tab-10.1177_1759720X261460128 for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021 by Yijia Gao, Lei Chen, Siwei Yang, Fengyuan Yu, Baoxuan Lin, Botao Zhou and Yingjun Nie in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-xlsx-3-tab-10.1177_1759720X261460128 – Supplemental material for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021
Supplemental material, sj-xlsx-3-tab-10.1177_1759720X261460128 for Temporal trends and future projections of hand osteoarthritis burden in China from 1990 to 2021 by Yijia Gao, Lei Chen, Siwei Yang, Fengyuan Yu, Baoxuan Lin, Botao Zhou and Yingjun Nie in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors gratefully acknowledge the financial support from the 2022 Philosophy and Social Sciences Research Project (Key Project) of the Hubei Provincial Department of Education, China (Grant No. 22D102).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.