
Abstract
Background:
Tocilizumab (TCZ), an interleukin-6 receptor inhibitor, is effective for moderate to severe rheumatoid arthritis (RA). However, maintaining remission after TCZ withdrawal remains challenging, and the treatment duration required before discontinuation to minimize relapse risk is unclear.
Objectives:
To identify a TCZ treatment-duration threshold before withdrawal that is associated with a lower risk of relapse in patients with RA.
Design:
This was a retrospective study including 97 patients with RA who discontinued intravenous TCZ after stable disease control.
Methods:
We retrospectively analyzed 97 RA patients who achieved remission or low disease activity prior to TCZ withdrawal. The primary outcome was relapse within 12 months post-discontinuation. Cox proportional hazards regression identified independent predictors, while restricted cubic spline (RCS) modeling assessed non-linear associations between treatment duration and relapse risk. A simplified risk stratification tool was developed and internally validated using bootstrap resampling.
Results:
Among 97 patients with RA who discontinued TCZ after stable disease control, most were biologic-naïve (98.9%), the mean disease duration was 72.9 ± 52.7 months, and concomitant methotrexate and hydroxychloroquine were used in 73.2% and 47.4% of patients, respectively. During the 12-month follow-up, 54 patients (55.7%) relapsed. TCZ treatment duration was an independent protective factor (adjusted HR = 0.892 per month, p = 0.002), whereas anti-citrullinated protein antibody (ACPA) positivity was associated with increased relapse risk (adjusted HR = 2.122, p = 0.031). RCS analysis demonstrated an L-shaped non-linear relationship, identifying an empirically derived duration threshold at approximately 200 days associated with lower relapse risk. A simplified score assigning 1 point each for ACPA positivity and TCZ duration < 200 days stratified patients into low- (0 points), intermediate- (1 point), and high-risk (2 points) groups, with relapse rates of 27.3%, 53.8%, and 91.7%, respectively; the model showed acceptable discrimination (AUC = 0.76).
Conclusion:
Longer TCZ treatment duration and ACPA negativity were associated with a lower risk of relapse after TCZ withdrawal. An approximately 200-day treatment duration may serve as a clinically informative threshold for risk-stratified withdrawal decisions in routine practice, although disease control after withdrawal should be interpreted in the context of ongoing background therapy rather than confirmed drug-free remission.
Plain language summary
Rheumatoid arthritis is a long-term condition in which the immune system attacks the joints, causing pain, swelling, and damage. Tocilizumab is a medicine that can control the disease well, but doctors and patients often face an important question: when can it be safely stopped? In this study, we reviewed 97 patients with rheumatoid arthritis whose disease was well controlled before they stopped tocilizumab. We then followed them for 12 months to see who remained stable and who had a return of symptoms. We found that a little more than half of the patients had a relapse within 1 year after stopping treatment. Two factors were especially important. First, patients who stayed on tocilizumab for a longer time were less likely to relapse. Second, patients who had a positive anti-citrullinated protein antibody blood test were more likely to relapse. Our analysis suggested that about 200 days of treatment may be an important time point. Patients who stopped treatment before this were much more likely to have their disease come back. We also developed a simple tool based on treatment duration and antibody status that could separate patients into low-, medium-, and high-risk groups. These results suggest that stopping tocilizumab too early may increase the chance of relapse, especially in patients with a positive antibody test. This may help doctors and patients make more informed decisions about treatment withdrawal. However, because this was a single-center retrospective study, larger studies are needed to confirm these findings.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by persistent synovial inflammation, progressive cartilage destruction, and bone erosion, ultimately leading to irreversible joint damage and disability. Over the past decade, biologic disease-modifying antirheumatic drugs (bDMARDs) have revolutionized RA management by enabling tight disease control and radiographic stabilization. Among these, interleukin-6 (IL-6) receptor blockade with tocilizumab (TCZ) has proven highly effective in both monotherapy and combination regimens, offering suppression of systemic inflammation and structural protection.1,2
Despite these advances, long-term biologic therapy raises concerns regarding infection risk, immunosuppression, treatment cost, and patient burden. Consequently, biologic dose reduction and discontinuation have been evaluated in patients with RA who achieve sustained remission or low disease activity.3 –5 While some patients successfully maintain drug-free remission, a substantial proportion experience relapse, suggesting heterogeneity in underlying disease biology and immune reactivation potential.6,7
Previous investigations have identified several potential predictors of successful biologic withdrawal, such as disease duration, baseline activity, and autoantibody status.8,9 However, the duration of TCZ therapy prior to discontinuation remains insufficiently characterized. Observational evidence suggests that longer exposure may consolidate immunological remission, but the potentially informative treatment window required to minimize relapse risk remains undefined.10,11 Importantly, prior studies have typically assumed linear relationships between treatment duration and outcomes, which may obscure clinically meaningful inflection points.
Restricted cubic spline (RCS) modeling provides a flexible approach to evaluate potential non-linear associations between treatment duration and relapse risk. Using this approach, we hypothesized that a specific “exposure window” exists during which adequate IL-6 suppression stabilizes immune homeostasis, reducing the likelihood of post-withdrawal flare. The present study aimed to explore whether TCZ treatment duration before withdrawal was associated with relapse risk, to identify clinical predictors of relapse, and to develop a simple risk stratification tool for patients undergoing TCZ withdrawal in routine practice.
Methods
Study design and population
This retrospective cohort study was conducted in the Department of Rheumatology and Immunology, The First Affiliated Hospital of Nanchang University, Nanchang, China. Consecutive patients with RA who received TCZ therapy between January 2019 and December 2022 were screened. The study protocol was approved by the institutional ethics committee (Approval No. TTIS2025350) and conducted in accordance with the Declaration of Helsinki. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 12
Eligible participants met the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for RA and had active disease at the time of TCZ initiation (DAS28-CRP > 3.2). Inclusion required receipt of TCZ (intravenous) for at least 3 months, followed by treatment discontinuation due to sustained remission or low disease activity, as judged by the treating rheumatologist. Patients were required to have maintained stable disease control for at least three consecutive months before TCZ withdrawal, defined as remission (DAS28-CRP < 2.6) or low disease activity (DAS28-CRP 2.6–3.2).
Patients were excluded if they had other systemic autoimmune diseases, active malignancy, discontinued TCZ for reasons unrelated to disease control (e.g., adverse events, infection, poor adherence, or economic reasons), or had incomplete clinical data or loss to follow-up within 12 months after TCZ withdrawal.
Data collection
Demographic, clinical, and laboratory data were extracted from electronic medical records using a standardized case report form. Baseline variables were defined as those recorded at TCZ initiation, whereas pre-withdrawal data were collected from the last visit before discontinuation.
Collected data included demographic information (age, sex, body mass index (BMI)), disease-related variables (disease duration, rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA) status, DAS28-CRP, swollen and tender joint counts, clinical disease activity index (CDAI) and simplified disease activity index (SDAI)), comorbidities (hypertension, diabetes, coronary artery disease, chronic kidney disease and cancer history), and history of prior biologic use.
Treatment-related variables included TCZ administration route, total duration of therapy, and concomitant medications, including conventional synthetic DMARDs (csDMARDs: methotrexate (MTX), hydroxychloroquine (HCQ)). Glucocorticoid (GC) exposure prior to TCZ withdrawal was recorded, including the daily dose at withdrawal and the cumulative prednisone-equivalent dose from TCZ initiation to TCZ withdrawal.
Outcome definition and follow-up
The primary outcome was disease relapse within 12 months following TCZ withdrawal. Relapse was defined as a DAS28-CRP score ⩾ 3.2 with a clinically meaningful increase from the pre-withdrawal baseline, or the need for treatment escalation, including initiation or dose escalation of glucocorticoids or disease-modifying antirheumatic drugs, as documented in the medical record.
Time-to-relapse was defined as the interval from the date of TCZ discontinuation to the first documented relapse event. Patients without relapse were censored at the end of the 12-month follow-up period.
Statistical analysis
Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation (SD), and non-normally distributed data as median with interquartile range (IQR). Between-group comparisons (relapse vs non-relapse) were performed using Student’s t test, Mann–Whitney U test, or Fisher’s exact test as appropriate.
Kaplan–Meier curves were generated to evaluate relapse-free survival, and differences were assessed using the log-rank test. Cox proportional hazards regression was applied to identify independent predictors of relapse. Covariates with p < 0.10 in univariate analysis or those of clinical relevance were entered into the multivariable model. Multicollinearity was examined using the variance inflation factor (VIF), with a threshold of 5 for exclusion.
To explore non-linear associations between TCZ treatment duration and relapse risk, RCS regression models were constructed with three knots placed at the 10th, 50th, and 90th percentiles of treatment duration. Non-linearity was evaluated using the likelihood ratio test comparing spline and linear models.
Based on the β-coefficients of the final multivariable model, a simplified risk score was derived and validated internally using bootstrap resampling (1000 iterations). Model discrimination was assessed with Harrell’s concordance index (C-index), and calibration was evaluated graphically. Statistical analyses were performed using R software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria) and SPSS (version 26.0; IBM Corp., Armonk, NY, USA). A two-tailed p value < 0.05 was considered statistically significant.
Results
Baseline characteristics and treatment course
A total of 97 patients with RA who discontinued TCZ after achieving sustained clinical control were included in the final analysis. Of these, 96 (98.9%) were biologic-naïve. The mean disease duration in the overall cohort was 72.9 ± 52.7 months, and concomitant MTX and HCQ were used in 71 (73.2%) and 46 (47.4%) patients, respectively. During the 12-month follow-up period, 54 patients (55.7%) experienced disease relapse, while 43 (44.3%) maintained stable disease control.
At TCZ initiation, patients who subsequently relapsed had a higher DAS28-CRP score than those who maintained disease control (4.5 ± 1.1 vs 4.1 ± 0.9, p = 0.047). RF positivity (81.5% vs 58.1%, p = 0.022) and ACPA positivity (77.8% vs 51.2%, p = 0.011) were also more frequent in the relapse group. Age, sex, BMI, and comorbidities did not differ significantly between the two groups.
Regarding treatment variables, the mean TCZ treatment duration was significantly shorter among relapsing patients (8.3 ± 5.6 months) than among those who remained in stable disease control (13.3 ± 8.0 months, p < 0.001). Similarly, the duration of stable disease control before TCZ withdrawal was also shorter in the relapse group than in the non-relapse group (5.5 ± 2.3 vs 7.2 ± 4.5 months, p = 0.028). At the time of TCZ withdrawal, all patients fulfilled remission or low disease activity criteria, and DAS28-CRP, CDAI, and SDAI were low in both groups. These scores did not differ significantly between patients who subsequently relapsed and those who did not relapse. Compared with the TCZ initiation baseline, all included patients had undergone glucocorticoid dose reduction before TCZ withdrawal, although some remained on concomitant low-dose glucocorticoids at the time of withdrawal. Concomitant use of csDMARDs (MTX or HCQ), glucocorticoid use and dose at withdrawal, cumulative glucocorticoid dose before withdrawal, and prior JAK inhibitor exposure did not differ significantly between groups. Importantly, this was a predominantly biologic naïve cohort, with only one patient having prior biologic exposure. At the time of TCZ withdrawal, the patients remained on background csDMARD therapy, and some continued low-dose glucocorticoids (Table 1).
Characteristics of study participants stratified by relapse status.
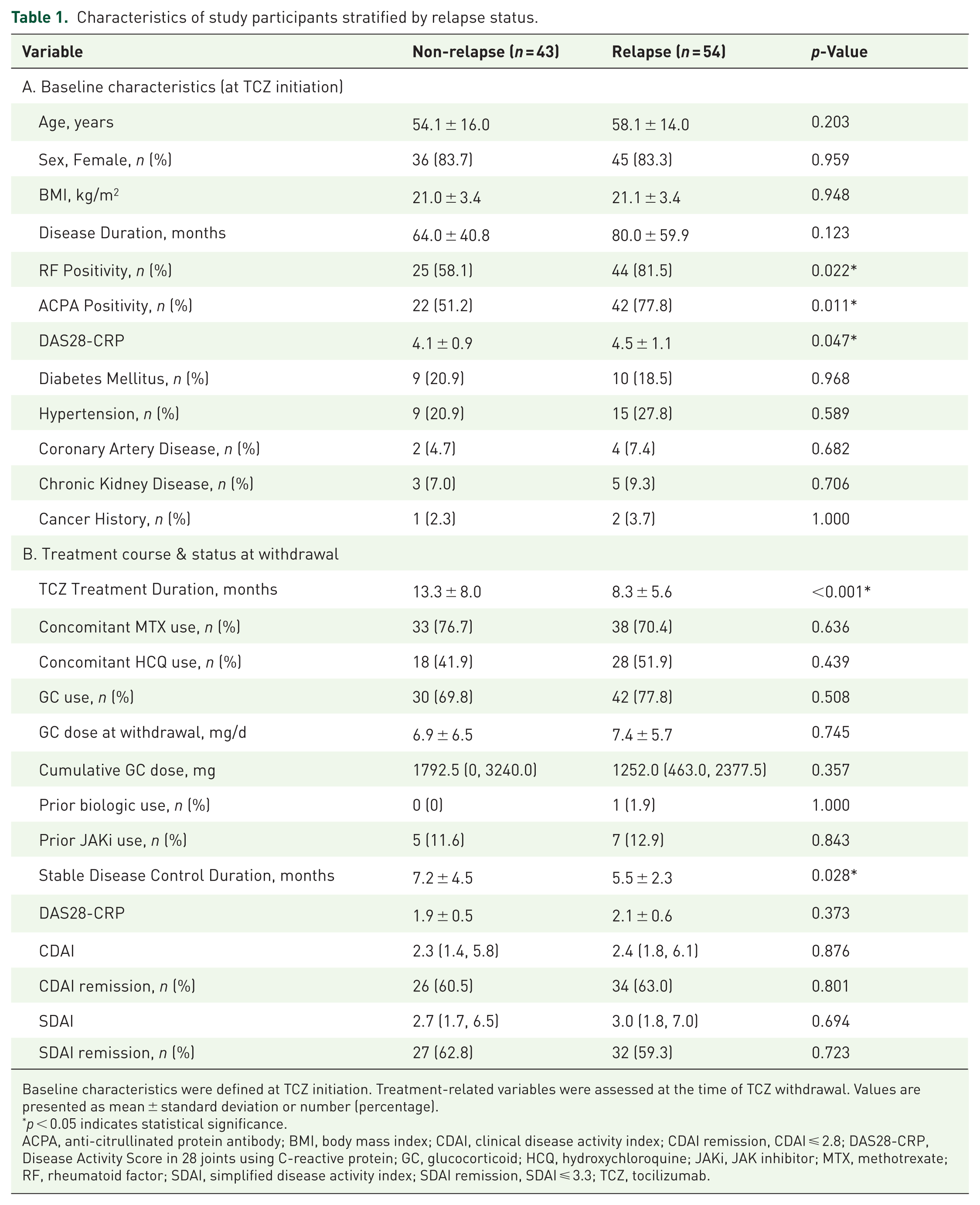
Baseline characteristics were defined at TCZ initiation. Treatment-related variables were assessed at the time of TCZ withdrawal. Values are presented as mean ± standard deviation or number (percentage).
p < 0.05 indicates statistical significance.
ACPA, anti-citrullinated protein antibody; BMI, body mass index; CDAI, clinical disease activity index; CDAI remission, CDAI ⩽ 2.8; DAS28-CRP, Disease Activity Score in 28 joints using C-reactive protein; GC, glucocorticoid; HCQ, hydroxychloroquine; JAKi, JAK inhibitor; MTX, methotrexate; RF, rheumatoid factor; SDAI, simplified disease activity index; SDAI remission, SDAI ⩽ 3.3; TCZ, tocilizumab.
Predictors of relapse following TCZ withdrawal
In univariate Cox regression, shorter TCZ treatment duration, higher baseline DAS28-CRP, and seropositivity for RF or ACPA were all associated with increased relapse risk. Because of strong collinearity between RF and ACPA (Spearman’s ρ = 0.76, p < 0.001), only ACPA was included in the multivariable model due to its higher prognostic specificity.
In the adjusted multivariable Cox regression (Table 2), TCZ treatment duration was independently associated with a lower risk of relapse (adjusted HR = 0.892 per month, 95% CI 0.831–0.957, p = 0.002). This indicates that each additional month of TCZ exposure was associated with an approximately 10.8% lower hazard of relapse. In contrast, ACPA positivity was independently associated with an increased risk of relapse (adjusted HR = 2.122, 95% CI 1.073–4.196, p = 0.031). Other variables, including age, sex, baseline DAS28-CRP, and concomitant csDMARD use, were not significantly associated with relapse risk.
Univariate and multivariable Cox proportional hazards regression analysis for predictors of relapse.
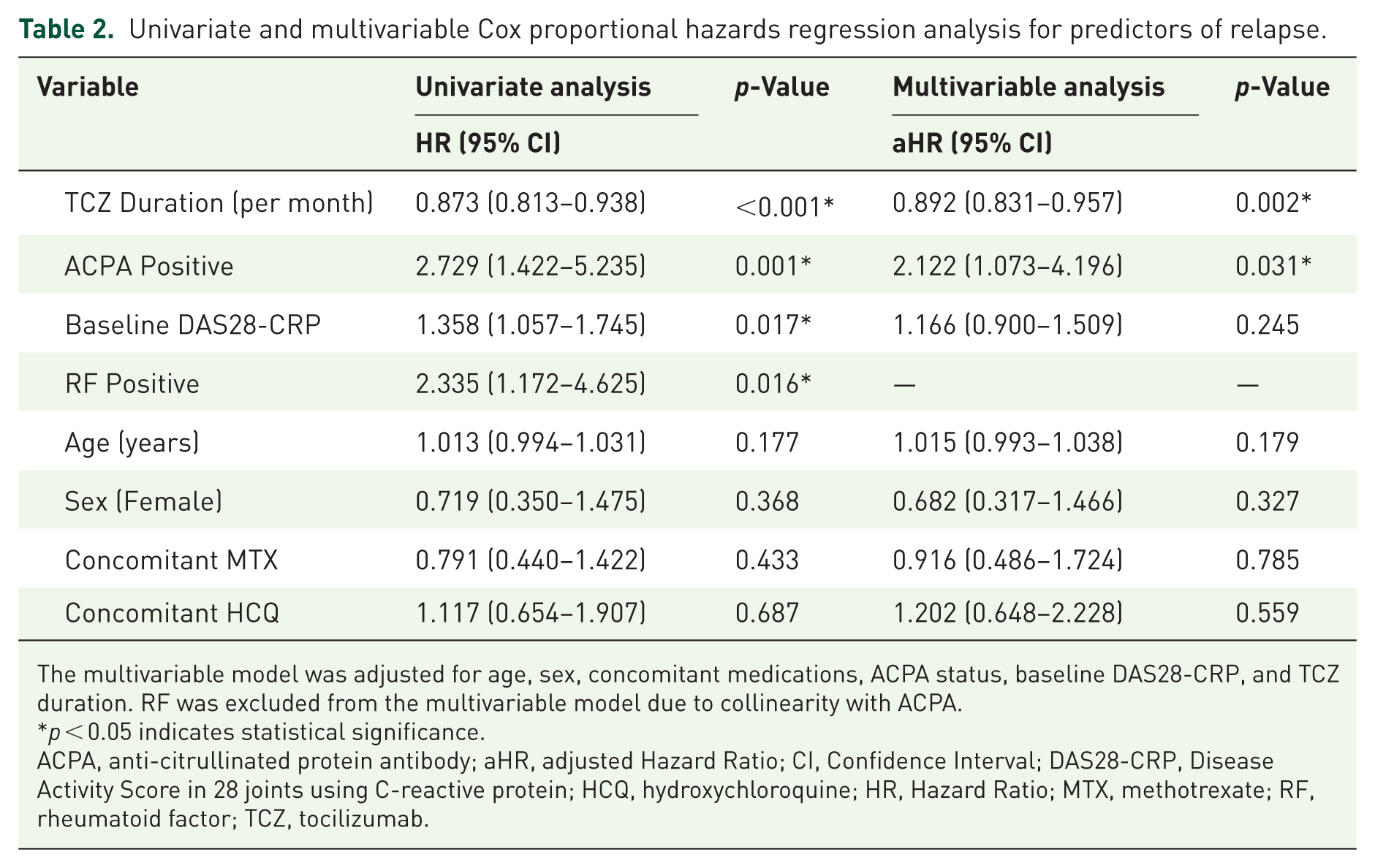
The multivariable model was adjusted for age, sex, concomitant medications, ACPA status, baseline DAS28-CRP, and TCZ duration. RF was excluded from the multivariable model due to collinearity with ACPA.
p < 0.05 indicates statistical significance.
ACPA, anti-citrullinated protein antibody; aHR, adjusted Hazard Ratio; CI, Confidence Interval; DAS28-CRP, Disease Activity Score in 28 joints using C-reactive protein; HCQ, hydroxychloroquine; HR, Hazard Ratio; MTX, methotrexate; RF, rheumatoid factor; TCZ, tocilizumab.
Exploration of a treatment-duration threshold
To characterize the relationship between TCZ duration and relapse risk, RCS modeling was applied. The RCS curve suggested an L-shaped association between TCZ duration and relapse risk (Figure 1). The risk of relapse was higher among patients receiving shorter courses of TCZ, followed by a sharp decline once the duration exceeded approximately 200 days.
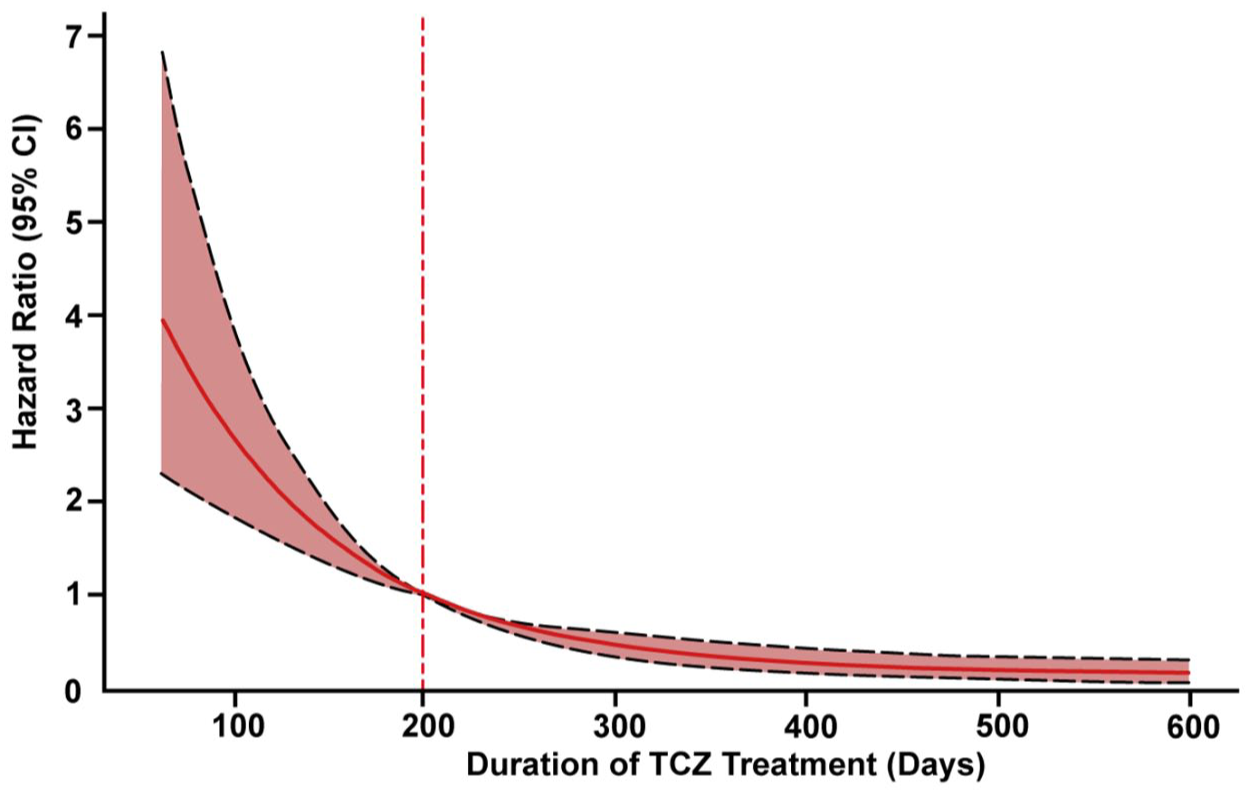
Non-linear association between TCZ treatment duration and relapse risk.
Based on this inflection point, patients were stratified into a short-course group (<200 days) and a standard-course group (⩾200 days). The cumulative relapse rate was higher in the short-course group compared with the standard-course group (84.8% vs 40.6%, p < 0.001). Kaplan–Meier survival analysis confirmed that patients treated for ⩾200 days exhibited significantly greater relapse-free survival (log-rank p < 0.0001; Figure 2). Extending treatment beyond 300 days offered diminishing incremental benefit, suggesting that 200–300 days may provide a clinically informative reference point for withdrawal consideration.
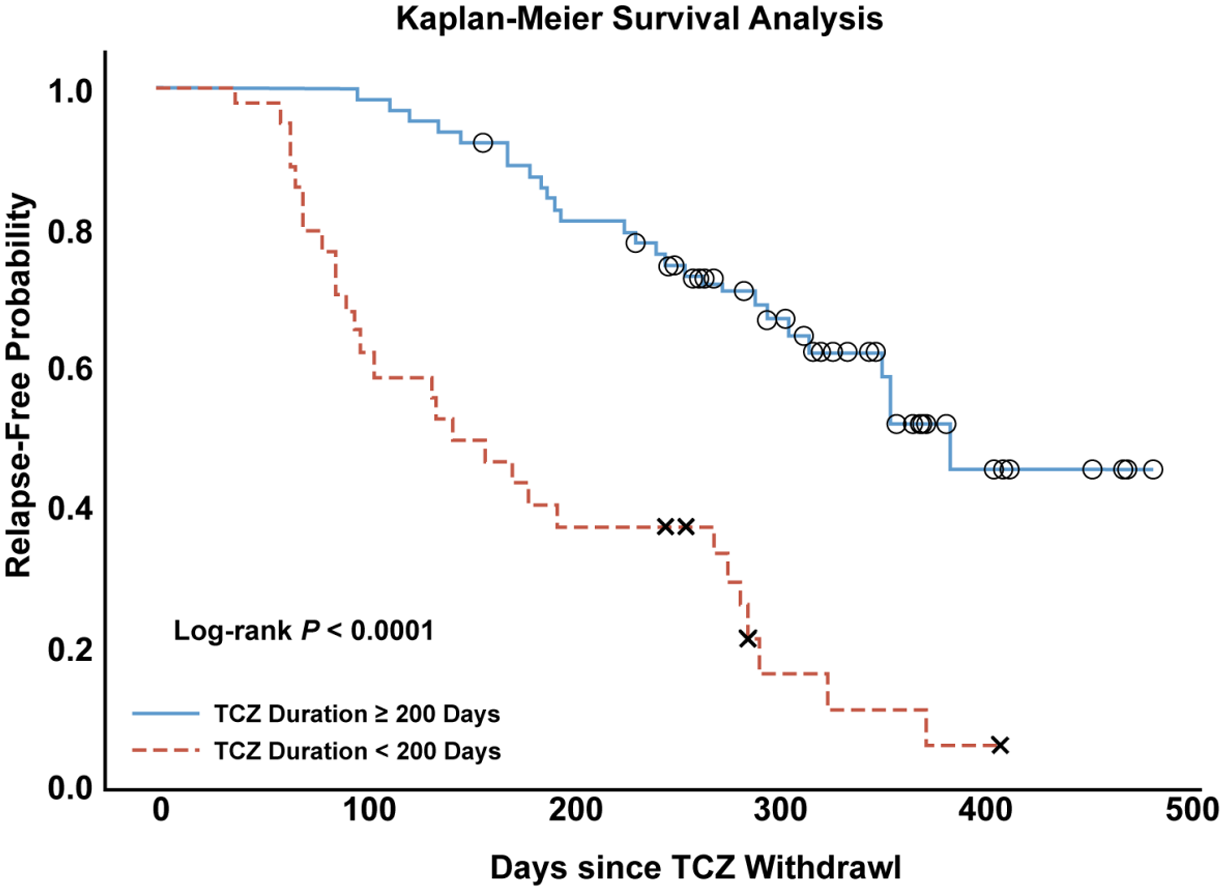
Kaplan–Meier relapse-free survival curves stratified by tocilizumab treatment duration.
Development of a simplified risk stratification tool
To facilitate clinical translation, a simplified relapse risk stratification model was constructed based on the two strongest predictors identified in multivariable analysis, namely ACPA positivity and TCZ treatment duration shorter than 200 days. Each predictor was assigned one point, yielding a total risk score ranging from 0 to 2. Accordingly, patients with neither risk factor (ACPA-negative and TCZ duration ⩾ 200 days) were classified as low risk, those with one risk factor as intermediate risk, and those with both ACPA positivity and TCZ treatment duration <200 days as high risk. Relapse rates increased progressively across these strata, from 27.3% in the low-risk group to 53.8% in the intermediate-risk group and 91.7% in the high-risk group (p < 0.001; Figure 3).
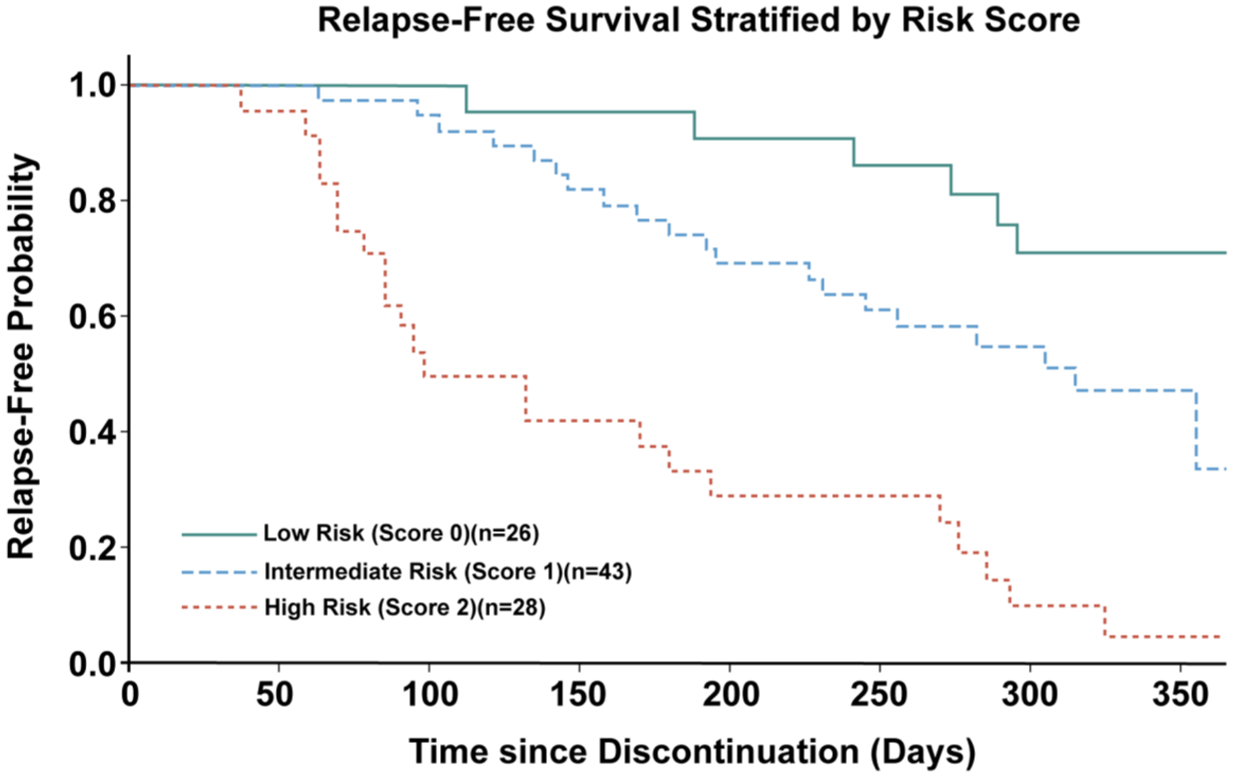
Kaplan–Meier estimates of relapse-free survival stratified by the simplified risk score.
The risk stratification model demonstrated acceptable discriminatory performance, with an area under the receiver operating characteristic curve (AUC) of 0.76 (95% CI, 0.65–0.84), and calibration analysis suggested reasonable agreement between predicted and observed relapse risk (Figures 4 and 5). Bootstrap resampling suggested reasonable internal consistency of the model. In addition, sensitivity analyses applying alternative relapse definitions (DAS28-ESR > 3.2), yielded consistent predictive performance.
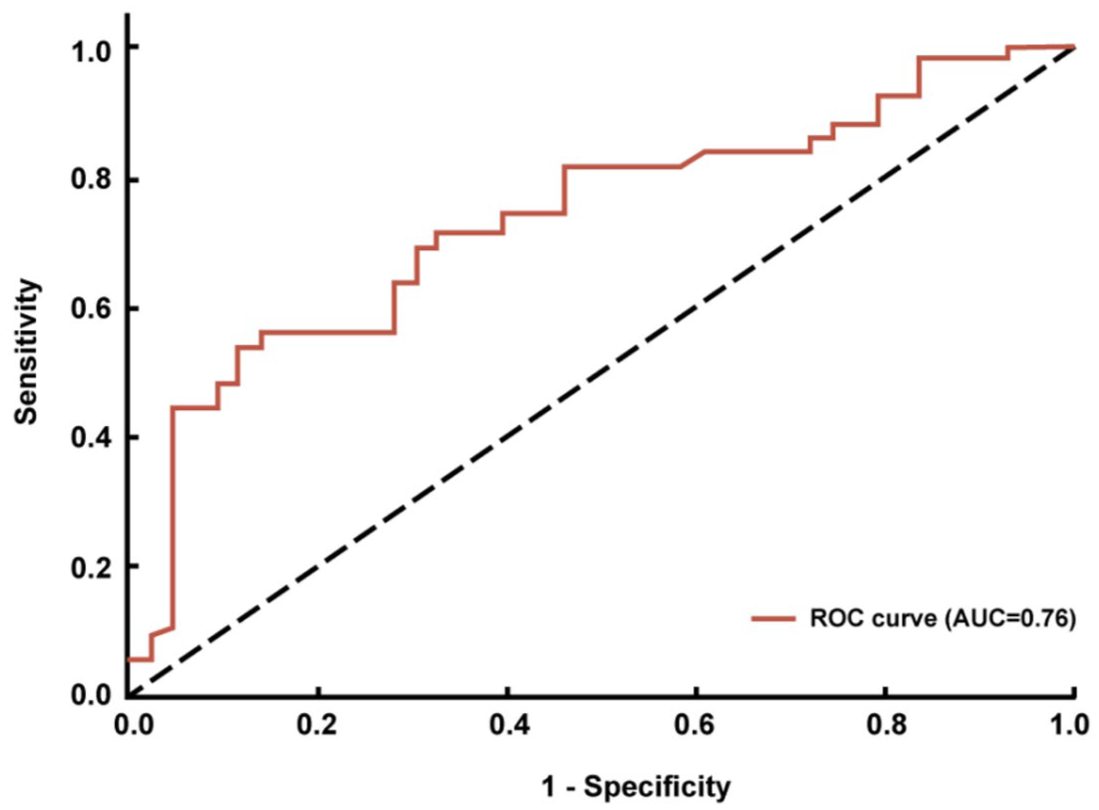
ROC curve of the relapse risk stratification model after tocilizumab withdrawal.
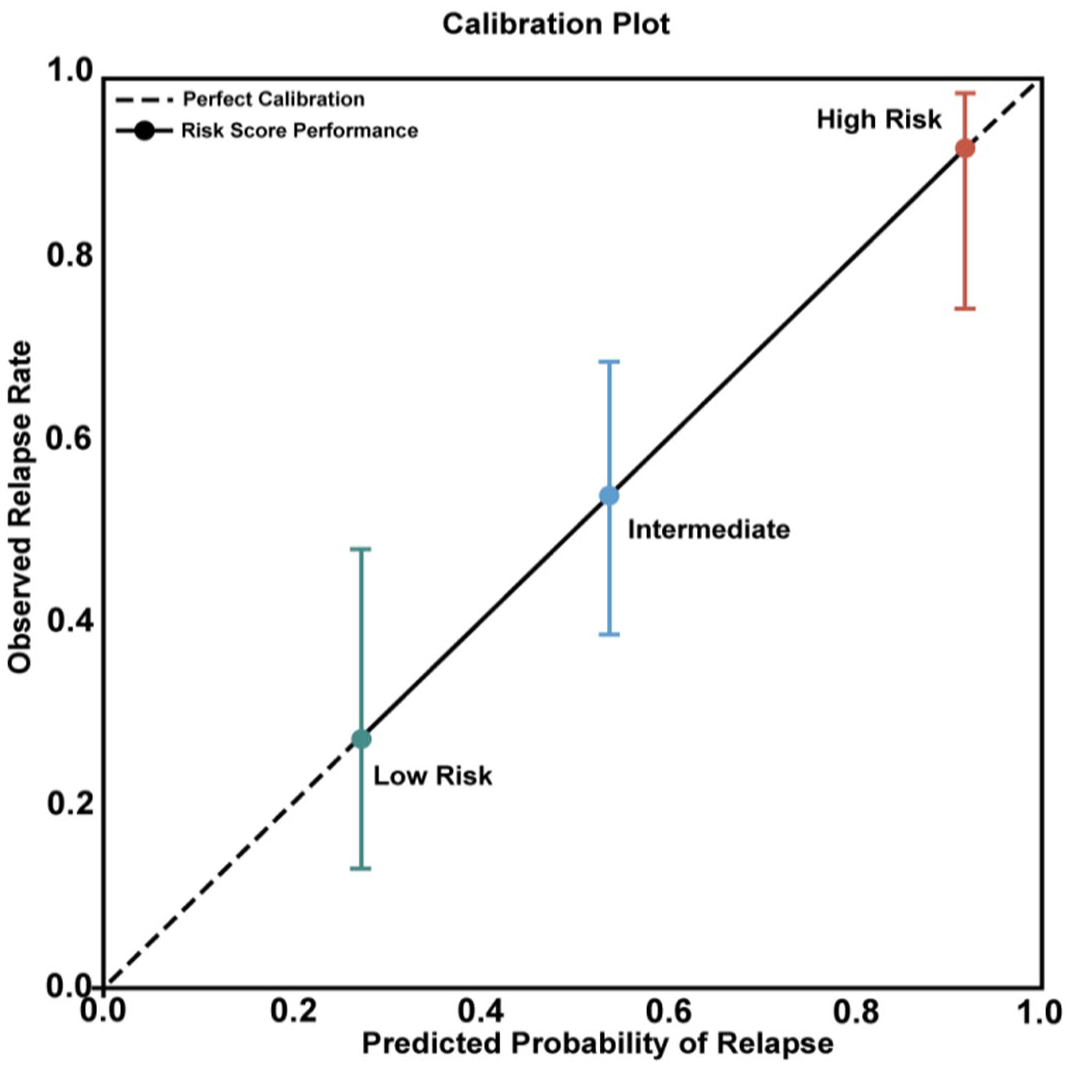
Calibration plot of the risk stratification model.
Discussion
TCZ has demonstrated efficacy in controlling synovial inflammation and preventing structural damage in patients with moderate-to-severe RA. 13 Nonetheless, sustaining disease control after TCZ withdrawal remains a complex clinical challenge. In this retrospective cohort study, shorter TCZ treatment duration and ACPA positivity were independently associated with relapse within 1 year after discontinuation.
Our findings add to current evidence on biologic withdrawal by showing a time-dependent, non-linear association between TCZ exposure and relapse risk. RCS modeling suggested an L-shaped relationship, with an apparent inflection point at approximately 200 days. Relapse risk was higher among patients treated for shorter durations and appeared to decrease after treatment extended beyond this period. These results suggest that biologic withdrawal strategies should not be attempted prematurely. This aligns with the “deep remission” hypothesis, suggesting that prolonged suppression of proinflammatory cytokine networks is required to stabilize the adaptive immune response.14,15 Mechanistically, extended IL-6 receptor blockade may allow sufficient time for the restoration of Treg/Th17 balance and the downregulation of synovial macrophage activation, thereby potentially reducing the likelihood of pathogenic immune reactivation upon withdrawal.16,17 Consequently, the approximately 200-day threshold identified in this study provides a quantitative reference point for delaying TCZ withdrawal until the consolidation phase is achieved. However, it should not be interpreted as a universal biological threshold. Rather, it represents a data-derived, clinically informative estimate observed in a real-world cohort that requires validation in independent populations.
Furthermore, our study highlights the critical role of serological status in guiding withdrawal decisions. We found that ACPA-positive patients had a twofold higher risk of relapse compared to seronegative patients. ACPA-positive RA reflects a distinct immunopathogenic phenotype characterized by epitope spreading and prolonged plasma cell survival, which may require longer suppression to achieve immunological quiescence.18,19 Interestingly, our multivariable analysis did not find a significant independent protective effect for concomitant MTX or HCQ use after adjusting for treatment duration and serostatus. This suggests that while comedication is important for induction, the duration of IL-6 blockade and the underlying immunopathology (ACPA status) are the primary determinants of withdrawal success in this specific setting. These findings reinforce the concept that serological phenotype should be a central consideration in individualized withdrawal algorithms.
To translate these findings into clinical practice, we developed a simplified risk stratification tool based on the two core predictors: treatment duration < 200 days and ACPA positivity. This tool stratified patients into three distinct risk groups, with observed relapse rates ranging from 27.3% in the low-risk group (seronegative, treated > 200 days) to 91.7% in the high-risk group (seropositive, treated < 200 days). The model showed acceptable discrimination (AUC = 0.76) and reasonable calibration. This stratification suggests that ACPA-positive patients may require more prolonged TCZ treatment before withdrawal is considered, whereas seronegative patients may have greater flexibility. However, this interpretation should be made with caution, as the non-relapse group should be understood as patients who maintained disease control after TCZ discontinuation under background therapy, rather than as patients in confirmed drug-free remission.
An important implication of our findings is that treatment duration and serological status, although clinically accessible, may still be insufficient to fully characterize relapse risk at the time of TCZ withdrawal. In patients with RA who are in apparent clinical remission or low disease activity, subclinical synovitis is well documented, and several studies suggest that ultrasonography may provide clinically relevant information for biologic tapering and withdrawal decisions. Naredo reported that Doppler-detected synovitis predicted failed biologic tapering in patients with sustained clinical remission. 20 Alivernini further suggested that ultrasound-defined remission may help identify patients who can taper and discontinue anti-TNF therapy without relapse, and Terslev demonstrated that lower baseline Doppler sum scores independently predicted successful bDMARD discontinuation at 2 years, whereas clinical parameters alone were not predictive.21,22 Together, these findings indicate that ultrasound may provide additional information beyond composite disease activity indices. In this context, our model based on TCZ treatment duration and ACPA status may serve as a clinically accessible first-step framework, while imaging could provide further risk refinement. A reasonable future strategy would be to integrate treatment-duration threshold, ACPA status, and standardized pre-withdrawal ultrasound assessment, particularly residual power Doppler activity, into a multidimensional tapering algorithm. Such an approach may help distinguish patients with truly consolidated remission from those with clinically silent but persistent synovitis. At the same time, imaging-based strategies have not yet been standardized, and their future role may lie more in selective risk refinement at the time of tapering or withdrawal than in universal routine use.
Limitations
Despite the strengths of this study, several limitations should be acknowledged. First, this was a retrospective single-center real-world study, which may have introduced selection bias and limits the generalizability of the findings to other clinical settings and patient populations. Second, patients were identified on the basis of actual TCZ discontinuation in routine practice rather than a predefined tapering protocol, and the findings should therefore be interpreted in the context of real-world withdrawal practice. Third, the sample size was modest, and the number of relapse events may have been insufficient to fully evaluate weaker predictors or more complex interactions, which may have affected the stability of the model estimates. In addition, potentially relevant prognostic information, including extra-articular disease burden, was not fully reflected in the present analysis. Finally, the non-relapse state observed in this cohort reflects maintenance of disease control after TCZ withdrawal under background therapy rather than confirmed drug-free remission. In addition, the definition of disease control before TCZ withdrawal remains subject to the known limitations of DAS28-CRP under IL-6 blockade, which may overestimate remission or low disease activity. Although sensitivity analyses using DAS28-ESR showed a consistent overall direction of the findings, the absence of musculoskeletal ultrasound means that residual clinical or subclinical synovitis could not be fully excluded at the time of TCZ withdrawal. This may have limited the ability of our model to capture inflammatory activity beyond treatment duration and serological status.
Conclusion
In conclusion, our study supports a risk-stratified approach to TCZ withdrawal in RA. Patients with longer TCZ exposure and lower serological risk may be better candidates for treatment discontinuation, whereas those with shorter exposure and ACPA positivity may require greater caution. The proposed 200-day threshold should be viewed as a clinically informative reference derived from a real-world cohort, pending validation in broader prospective populations.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261464266 – Supplemental material for Restricted cubic spline analysis of treatment duration before tocilizumab withdrawal and relapse risk in rheumatoid arthritis
Supplemental material, sj-docx-1-tab-10.1177_1759720X261464266 for Restricted cubic spline analysis of treatment duration before tocilizumab withdrawal and relapse risk in rheumatoid arthritis by Houhui Jiang, Yuxin Yan, Sheng Zhao and Rui Wu in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors sincerely thank all patients who participated in this study and the clinical staff of the Department of Rheumatology and Immunology, The First Affiliated Hospital of Nanchang University, for their assistance with data collection.
Declarations
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence statement
During the preparation of this work, the authors used ChatGPT in order to refine the structure of the text and enhance its academic clarity. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the published article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.