
Abstract
Background:
The quality of data in electronic health records (EHRs) depends on adherence of clinicians to principles of diagnosis documentation.
Objective:
A concept mapping (CM) approach was used to extract factors related to quality of clinicians’ documentation that govern EHR data quality.
Method:
Influential factors extracted from brainstorming sessions were sorted by individual participants, followed by a quantitative analysis using multidimensional scaling and cluster analysis to categorise sorted factors. Finally, a questionnaire was used to elicit the importance-feasibility of the extracted factors. Results were visualised by cluster maps and Go-Zone plots.
Result:
Factors were classified into seven clusters: “knowledge about International Classification of Diseases and clinical coding,” “need for facilitators and guidelines,” “explaining the importance of the issue and defining responsibilities,” “cooperation of other personnel,” “codify legal requirements,” “workload” and “clinical obstacles,” as ranked by importance.
Conclusion:
To enhance the quality of EHR data, a collaboration between physicians, nurses, managers and EHR developers is required. CM is an acceptable approach to meet this objective. Our findings highlight the significance of clinical coding knowledge, awareness about its importance and applicability and use of well-structured information systems. In combination, these three factors can have a strong positive impact on the quality of EHR data.
Implications:
A list of solutions is provided for policymakers, and two interventions suggested, based on the findings of this study, including the adoption of EHRs that incorporate documentation guidelines. We further propose updated clinical training programs and a monitoring and feedback mechanism to facilitate the EHR documentation process.
Keywords
Introduction
A typical piece of healthcare management data is the principal (final) diagnosis and its associated clinical codes. A clinical code is assigned to all final diagnoses according to World Health Organization’s (WHO) International Classification of Diseases (ICD). These clinical codes reveal important information about the diagnosis and patient conditions. Diagnosis codes are used for processing reimbursements in hospitals based on the diagnosis-related group, assessing healthcare quality, monitoring patients and conducting clinical and epidemiological research (Hay et al., 2020; Lucyk et al., 2017; Tsopra et al., 2018). Also, inpatient registry, along with diagnosis codes as one of its most important fields, is a vital source of data for numerous research projects (Ludvigsson et al., 2011). There is a significant variation in the accuracy of diagnosis codes among different countries. Even different hospitals within the same healthcare system, which use the same ICD standards, report different figures for coding accuracy (Ahmadi and Madani, 2016; Burns et al., 2012; O’Malley et al., 2005). In most countries, clinical coding is undertaken by a person other than the attending physician. Likewise, in Iran, after documenting the diagnosis and related clinical procedures by clinicians, clinical coders assign codes to the medical records at discharge or shortly after (depending on the hospital) and register the clinical codes in the health information system (HIS). As such, the quality of diagnosis codes is directly related to the quality of documentation and adherence of healthcare providers to ICD standards (Tang et al., 2017). However, previous studies have highlighted the fact that accuracy of clinical coding is significantly undermined by poor clinician documentation even in developed countries (Lucyk et al., 2017; Tang et al., 2017).
With the gradual shift from paper to electronic health records (EHRs), opportunities and challenges associated with presentation of healthcare data have emerged (Jensen and Bossen, 2016). Although previous studies report different outcomes about the impact of EHRs on the quality of healthcare (Buntin et al., 2011; Joukes et al., 2016; Mohan et al., 2013; Nguyen et al., 2014; Pollak and Lorch, 2007), improving the quality of documentation is often regarded as one of the advantages of EHRs (Nguyen et al., 2014). On the other hand, quality and accuracy of data is an important contributing factor for a better acceptance of EHRs (Häyrinen et al., 2008). To improve the quality of diagnosis documentation, it is essential to first identify the reasons behind poor adherence of clinicians to principles of diagnosis documentation and design appropriate interventions to overcome this problem.
Concept mapping (CM) is a visualised mixed method which has been extensively applied in the healthcare domain, as well as areas such as psychology, education and evaluation (Donnelly, 2017). Examples of using the CM approach in the healthcare domain include extraction of factors influencing influenza vaccination in emergency medical services (Subramaniam et al., 2016), analysis of expectations of healthcare professionals for EHR implementation (Joukes et al., 2016), identification of barriers and facilitators for healthcare IT-based interventions (Donaldson et al., 2018; van Engen-Verheul et al., 2015; van Engen-Verheul et al., 2017), extraction of system requirements (Ogden et al., 2017), identifying policy options and interventions to achieve people-centered healthcare services (Leyns et al., 2018) and national prioritisation for prevention of chronic disease (Wutzke et al., 2017).
The purpose of the present study was to extract the factors influencing clinicians’ adherence to principles of diagnosis documentation. The results can help decision makers design suitable interventions. As such, a quantitative–qualitative CM approach was used to maximally collect the views of end users and stakeholders and to illustrate the results using visualised tools.
Method
This study was performed in Mashhad University of Medical Sciences with the ethics approve code of IRMUMS.MEDICAL.REC.1397.376. Participants in different CM steps were clinicians, nurses and administrators, who were employed in different specialised and general hospitals, including two main referral hospitals in eastern Iran. Although the responsibility of clinical documentation lies with the attending physician, other individuals are also involved with the documentation and clinical coding process, so the main focus of this study was clinicians. However, since nurses work alongside clinicians in the documentation process, a few experienced nurses were also involved in the CM steps. As well, the views of administrators as stakeholders can also facilitate the CM sessions from a practical and administrative perspective. Therefore, administrators were also included in the CM steps.
Principles of diagnosis documentation, which is established based on WHO guidelines and clinical coding requirements, are divided into two categories. One category is concerned with general principles such as avoiding the use of ambiguous abbreviations for diagnoses, specifying, as far as possible, both the etiological nature (underlying cause of the disease or medical condition) and the clinical manifestation, and documenting entities and external causes and so on. The other category varies across different departments and diagnoses: in some cases, extra information is required to be documented by physicians for more accurate coding. For example, in burns cases, anatomical site, depth of burn, extent, external cause and probable clinical complications such as infection should be documented. In fractures, the anatomical site, open or closed fracture, external cause, shape and other injuries should be mentioned, and more details are needed if the fracture resulted from a traffic accident. In documenting poisoning, the nature of the poisoning should be clear, to differentiate a poisoning from an adverse effect (poisoning because of the correct use of prescribed drugs). Then, based on the nature, the agent, clinical manifestations and poisoning external cause should be documented. Also, activity and location of all incidents are important.
Accuracy of coding is directly related to the quality of documentation by clinicians (Lucyk et al., 2017). Therefore, participants were invited from different departments such as clinical toxicology, gynecology, internal medicine, cardiology, pediatrics, dermatology and orthopedics. All hospitals used both EHR and paper-based records. CM consists of five major steps (Trochim and McLinden, 2017). Figure 1 shows an overview of these steps (Kane and Trochim, 2007). The CM process was undertaken face-to-face for all steps.
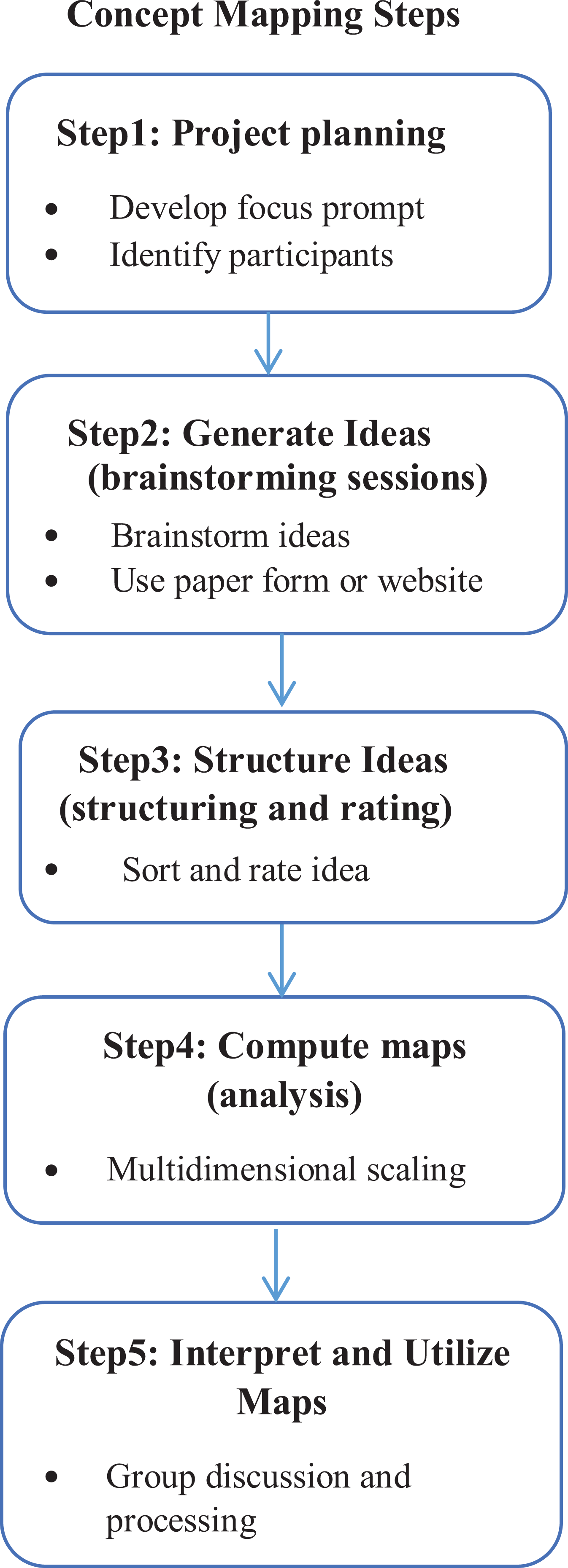
Concept mapping steps.
Step 1: Project planning
To design the focus prompt, several meetings were held between the research team, consisting of medical informaticians, health information technology and health management professionals, physicians and three members who held administrative positions. In alignment with the purpose of this study, the following focus prompt question was used to start the discussion with the participants: “In your opinion, what are the factors affecting the adherence of clinicians to principles of diagnosis documentation in inpatient medical records?”
CM achieves the best results when working with a heterogeneous group (Kane and Trochim, 2007). Therefore, the target group included physicians, nurses and hospital managers with different specialties and levels of work experience. To maximise the participation of the target group, CM sessions were held as part of research fellowship meetings. Participating in the sessions was fully voluntary and any person not willing to participate was allowed to leave anytime during the sessions. Maximum care was taken to provide comfort, relaxation and reassurance for the participants during the CM process.
Step 2: Idea generation
A brainstorming session was held after designing the focus prompt. Participants were given approximately 20 min to individually come up with statements in accordance with the focus prompt. At the beginning of the session, the facilitator (S.E.) explained the CM approach, purpose of the study and the focus prompt to the participants. There was enough allocated time to allow for writing and the facilitator (S.E.) answered any questions.
The facilitator asked every participant in turn, to present one statement from their list. Then, a discussion was held about the statement to clarify the main idea presented by the participant. Finally, the main point of each statement was extracted and the participant was asked whether this summary was correct. Complex statements were split into simpler, single statements after consulting with the participants. All participants were asked to remove items that were already mentioned by others. After the first round of statement gathering, the process continued until none of the participants could add a new statement. The maximum duration of a session was 2 hours.
Step 3: Structuring and rating of ideas
The list containing all statements from the brainstorming sessions was unified into one general list of statements. A list of a small number of statements is feasible for clustering (Kane and Trochim, 2007). As such, statements that described the same topic were combined to create a shorter encompassing list.
During the structuring sessions, participants individually categorised similar statements and assigned an appropriate name to each cluster. There was no limitation for this categorisation except that the size of each cluster must be greater than 0 and smaller than the number of total statements (Trochim and McLinden, 2017). Participants were asked not to create a category as “other cases” or categories with a single item. Finally, in a separate session, all participants were asked to rate each statement based on their opinion of its importance and feasibility, to determine the final statements. The rating tool was a 5-point Likert-type scale ranging from 1 = relatively unimportant to 5 = very important and 1 = relatively not feasible to 5 = very feasible. Both importance and feasibility are reported as mean values. Additionally, participants were asked to provide demographic information about age, sex, work experience and so on.
Step 4: Computation of maps
In this step, data were represented in the form of maps and Go-Zone plots using two-dimensional non-metric multidimensional scaling (MDS) and cluster analysis. Two-dimensional non-metric MDS is a set of related statistical techniques, which is used to visualise relative positions among members in a group with respect to some features. The input data for MDS analysis are a similarity matrix which employs a least-squares criterion and finally represents each brainstormed statement as a point on a two-dimensional plane. The closer the statements are in the two-dimensional plane, the more similarity they are expected to carry in meaning (Mukherjee et al., 2018; Saeed et al., 2018; Trochim and McLinden, 2017). The stress factor is a number between 0 and 1 calculated using MDS and shows the fitness of input data to the model where 0 is a perfect map. According to a meta-analysis of some CM studies, the average stress score is S = 0.285 and SD = 0.04 (Rosas and Kane, 2012). Finally, statements were classified hierarchically by cluster analysis. There is no simple mathematical criterion to select the number of clusters. The typical procedure involves examining an initial cluster solution that is maximally desirable for interpretation. Then, successively lower cluster solutions are examined. At each level, a decision was made as to whether the merger seems substantively reasonable. This procedure was repeated and the final number of clusters was chosen in such a way that it preserves the amount of detail and still results in substantively interpretable clusters (Trochim and McLinden, 2017). Accordingly, a cut-off point was determined based on possible similarity of statements and the group size. SPSS was used for MDS and hierarchical cluster analysis.
Step 5: Interpretation and utilisation of maps
The cluster map and Go-Zone plot were discussed by the research team. The naming of clusters was performed by the participants, but final names for the clusters were assigned by the research team. After a review of results, possible interventions were examined.
Results
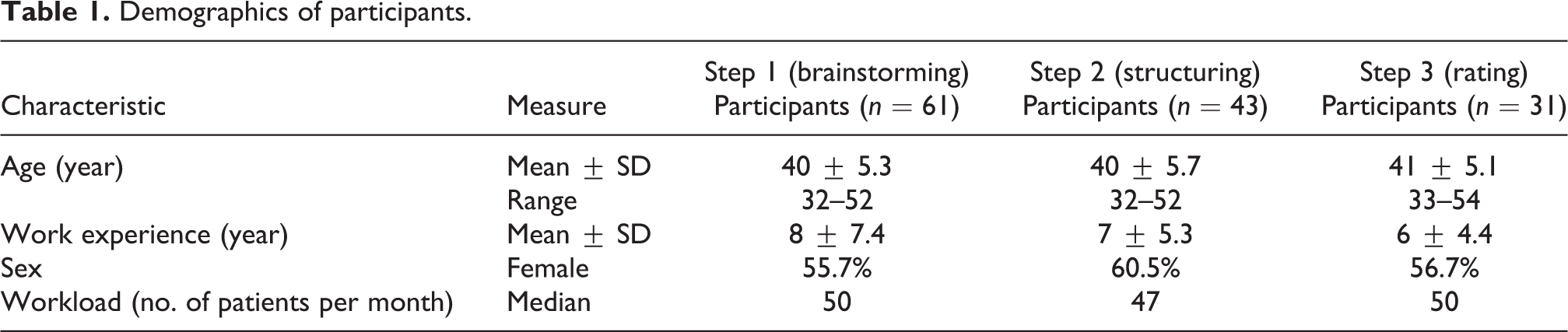
Of a total of 70 invitees, 61 participants took part in brainstorming sessions (Table 1). Response rate was 87%. For the later CM steps (participants of step 1), the response rates were also appropriate (70% and 50%).
Demographics of participants.
Brainstorming
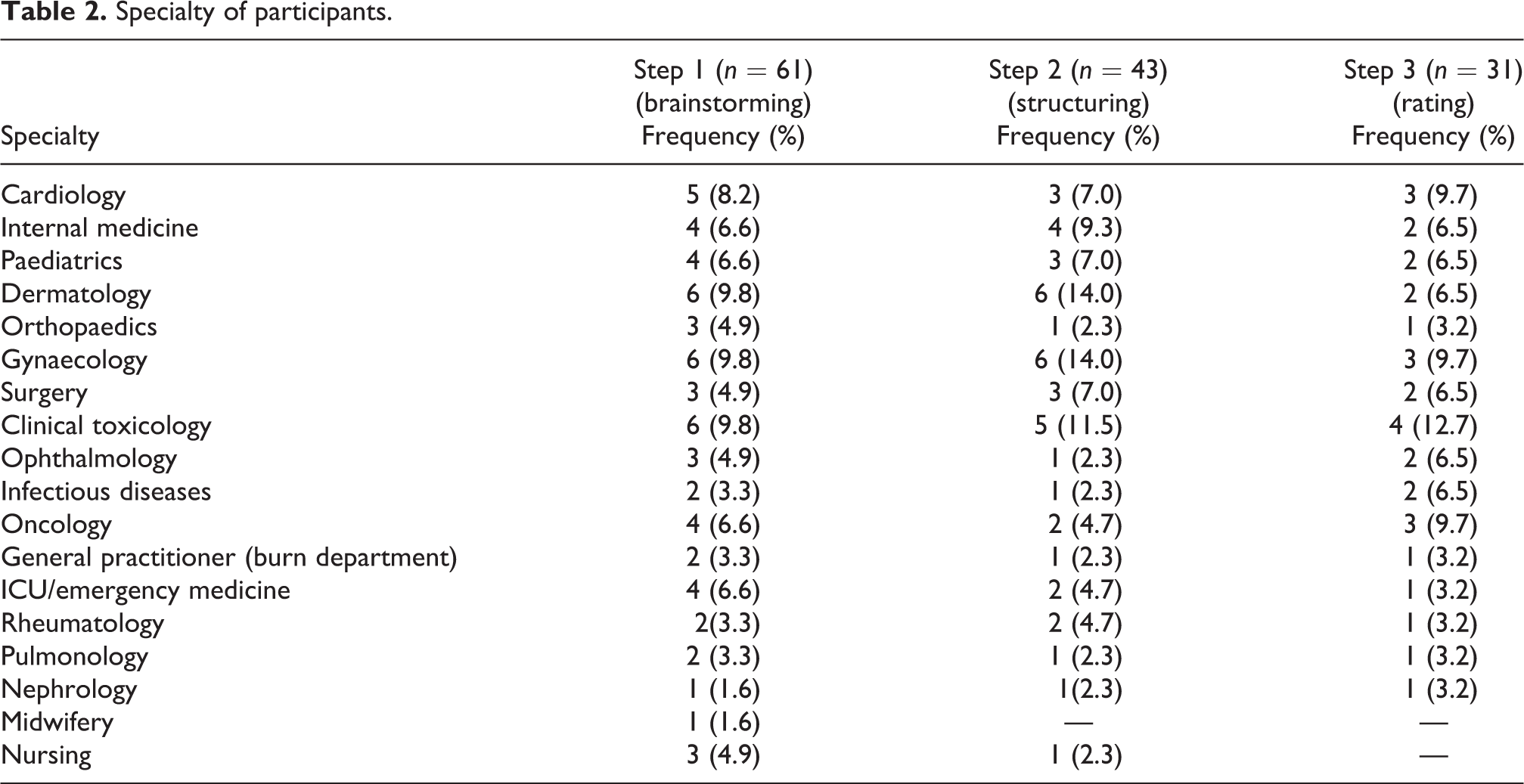
Participants in step 1 of CM consisted of 61 individuals, 55.7% female, with an average age of 40 years (range = 32–52) and an average work experience of 8 ± 7.4 years. Their median workload (number of patients per month) was 50 (Table 1). Participants included clinicians, nurses and administrators, who worked in different specialised and general hospitals including two main referral hospitals in eastern Iran. Specialties were cardiology, internal medicine, clinical toxicology, gynaecology, orthopaedics and so on (Table 2). The brainstorming session lasted for about 120 min. A total of 105 statements were extracted from the brainstorming session. After the initial editing and merging of similar statements, a total of 35 simple unique statements (Table 3) entered the next step.
Specialty of participants.
Number of statements per cluster.a
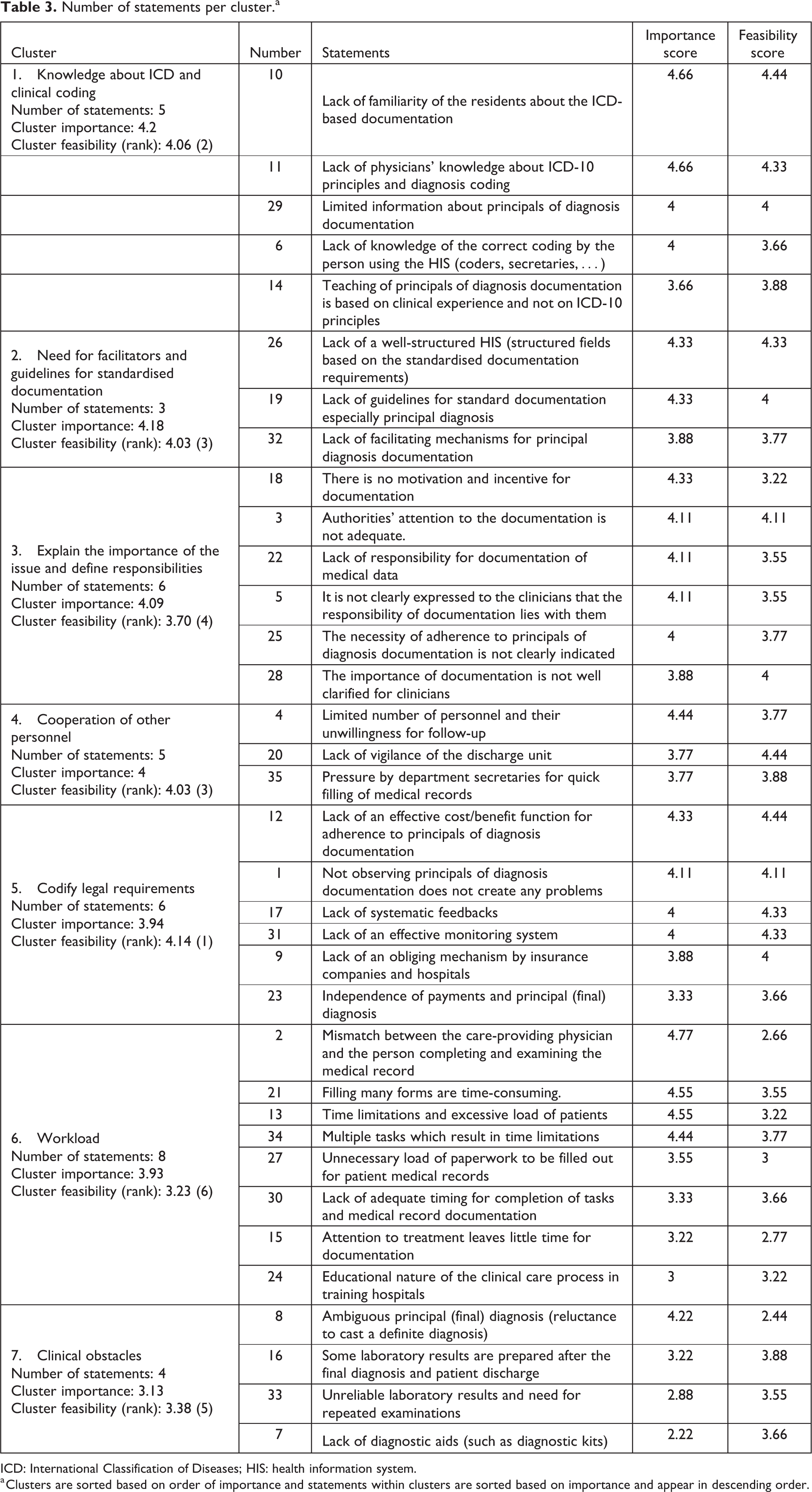
ICD: International Classification of Diseases; HIS: health information system.
a Clusters are sorted based on order of importance and statements within clusters are sorted based on importance and appear in descending order.
Structuring and rating
Sorting of statements was performed over two sessions, each lasting for about 90 min. Participants in this step of the CM consisted of 43 participants, 60.5% female, with an average age of 40 (range = 32–52) and average 7 years of work experience. Their median workload (number of patients per month) was 47 (see Table 1). The specialties of participants are presented in Table 2. Characteristics of participants in the brainstorming, structuring and rating steps were similar. The 35 statements from the previous step were categorised into seven clusters based on the sorting of statements and the resulting final similarity matrix (see Figure 2). The stress value for calculation of the point map was 0.29 (the stress score indicates goodness of fit of the model to the data).
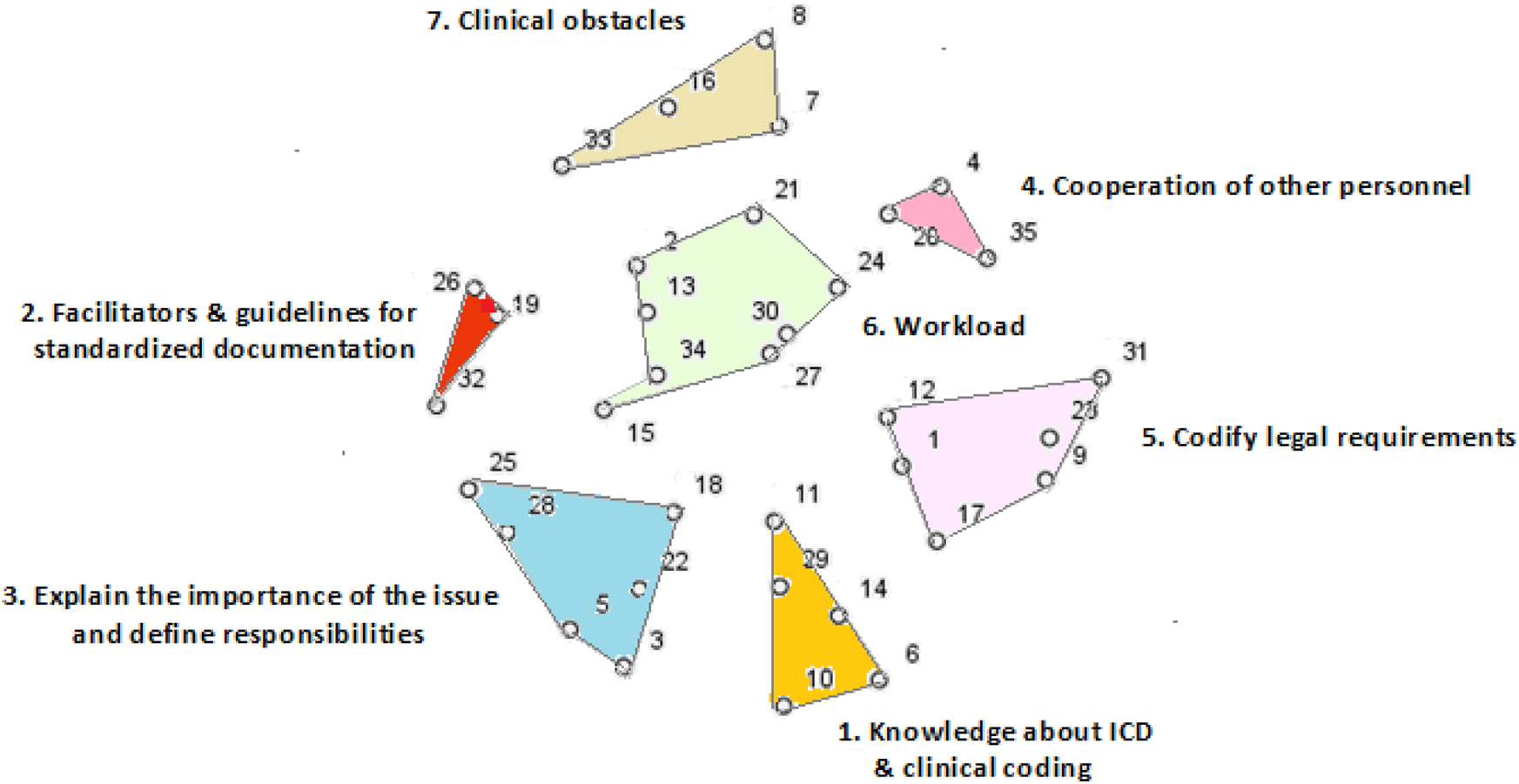
Concept mapping clusters.
Rating of statements was also performed in another session. This step consisted of 31 participants, 56.7% female, with an average age of 41 (range = 33–54) and an average work experience of 6 years. Their median workload (number of patients per month) was 50 (Table 1). The importance and feasibility score for each cluster and statements of each cluster (in the view of participants) are presented in Table 3. The average importance score ranged between 2.22 for statement “7” and 4.77 for statement “2.” The feasibility score ranged between 2.44 for statement “8” and 4.44 for statements “10,” “12” and “20.”
As presented in Table 3, “knowledge about ICD,” “need for facilitators and guidelines for standardised documentation” and “explaining the importance of the issue and defining responsibilities” were identified as the most important clusters. These clusters contained information about the feasibility and usefulness of information systems, training diagnosis documentation based on principles of ICD as well as awareness of the applicability and importance of clinical coding.
Interpretation and utilisation
The resulting outcomes of the previous step were discussed by the research team and healthcare policymakers to come up with an overview of the clusters. Each cluster and the appropriate type of intervention to cover the cluster were then discussed in detail. The seven extracted clusters covered different dimensions of the main issue (focus prompt). According to the average stress score reported by a meta-analysis of a few CM studies (S = 0.285, SD = 0.04) (Rosas and Kane, 2012), the stress score for our study indicates an appropriate fit to the data. Results of the clustering analysis and Go-Zone plot (Figures 2 and 3) can be used to design appropriate interventions. This can be done in such a way that not only maximally covers the requirements of clinicians and the hospital workflow but can also be accepted by the clinical staff and healthcare providers. Based on the clusters and Go-Zone diagram (Figure 3), a list of solutions and appropriate interventions were identified: The development of the HIS, based on the documentation by clinicians, needs to be customised for different departments. An academic training program for clinical documentation, based on WHO principles of clinical coding and documentation, is required for medical students. The sociotechnical responsibility of physicians in medical record documentation should be promoted. This can be achieved with an emphasis on the applicability and importance of clinical coding and the role of clinicians’ documentation in the accuracy of coding and related statistics. The documentation process should be monitored using engaging and punitive policies with effective feedback.
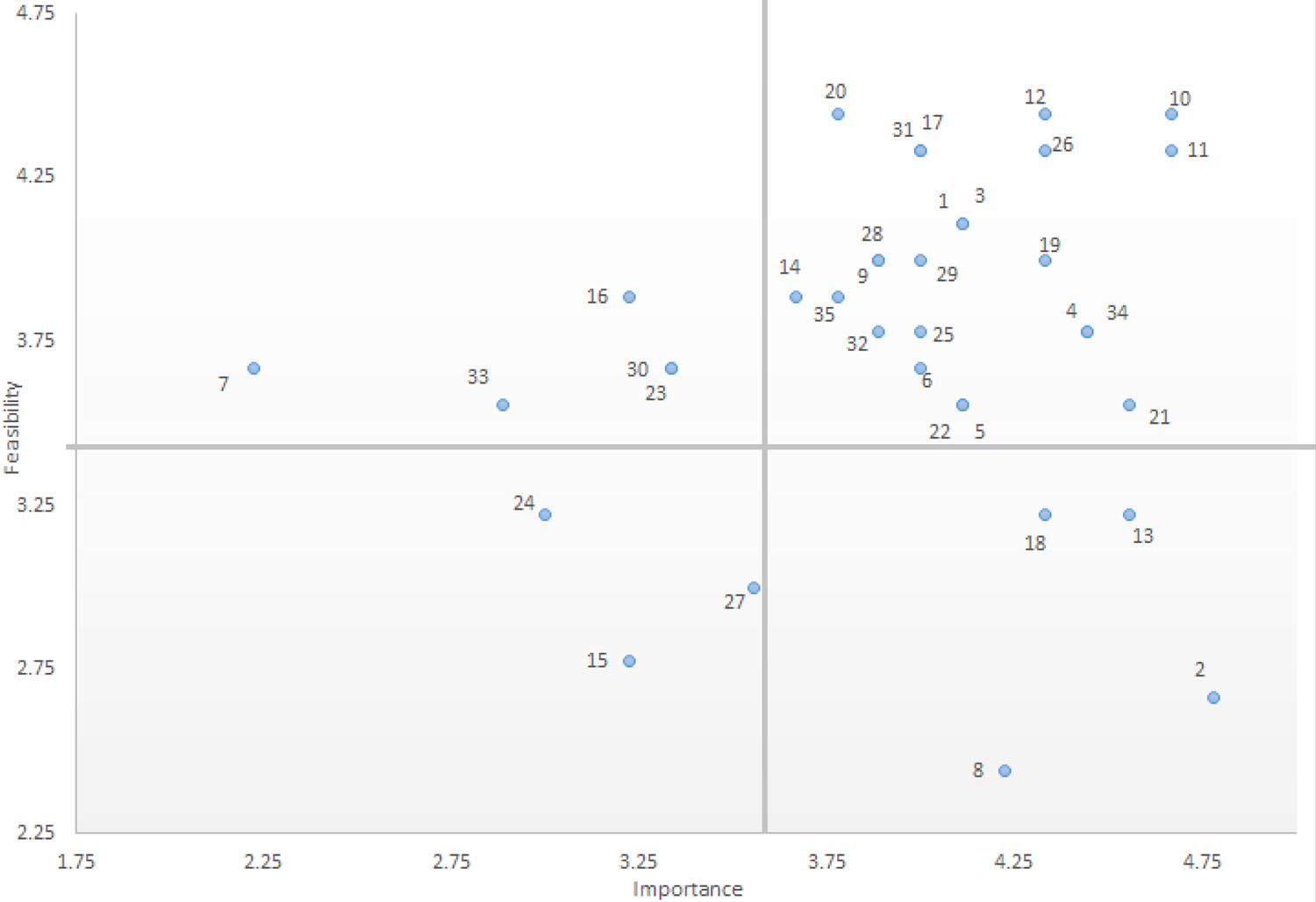
Importance-feasibility rate of brainstormed statements.
Discussion
The purpose of the present study was to extract the influential factors in clinicians’ adherence to principles of diagnosis documentation. This was done using an effective and efficient method based on CM. Development of health management systems and quality improvement interventions is a major concern for healthcare policymakers. However, bringing about changes in such systems is often slow and accompanied by substantial risks (Coiera, 2011). This is due to several reasons including complications associated with development of healthcare systems, preserving patients’ safety and privacy as well as the omnipresent challenge of resistance against change in any system development project. As such, the success in bringing about change in such systems mandates an in-depth analysis of the organisational workflow and system users’ requirements (Abdekhoda et al., 2015; Hepworth et al., 1992; Hossain et al., 2019; Joukes et al., 2016; Nguyen et al., 2014; Rezvani and Khosravi, 2019; Sidek and Martins, 2017; Vasconcelos, 2007). CM allowed us to collectively organise the viewpoints of various stakeholders as well as physicians of different specialties and to arrange common brainstorming sessions in which participants were able to exchange ideas over a short time period. Moreover, using quantitative analysis along with the qualitative steps has brought about added confidence in our reported results. The final results were produced in the form of transparent, easy-to-understand concept maps for different stakeholders along with the Go-Zone plots. This is very important for the design and implementation of efficient interventions.
Using the CM approach, the affecting factors in clinicians’ adherence to principles of diagnosis documentation were categorised into seven clusters based on the views of participants. These clusters include “knowledge about ICD and clinical coding,” “need for facilitators and guidelines for standardised documentation,” “explain the importance of the issue and define responsibilities,” “cooperation of other personnel,” “codify legal requirements,” “work load” and “clinical obstacles.”
Our previous results (Hosseini et al., 2019; unpublished results) indicated the importance of the physicians’ role in the quality of clinical coding from the viewpoint of coders. Factors such as incompetent knowledge of physicians about ICD and principles of diagnosis documentation, insufficient awareness of the importance and application of coding, non-prioritisation of coding by physicians and flawed hospital workflow resulting in problems such as delayed delivery of laboratory results were mentioned in the physician-related category. In the present study, the clinicians acknowledged these findings and added some other factors.
Previous studies have utilised the CM method in many healthcare applications (Donaldson et al., 2018; Hackett et al., 2016; Hargett et al., 2017; Ogden et al., 2017; Rosas and Ridings, 2017; Subramaniam et al., 2016; van Bon-Martens et al., 2017; van Engen-Verheul et al., 2015, 2017; Wutzke et al., 2017). However, to the best of our knowledge, our study is the first to use the CM approach for extraction of influential factors in non-adherence to ICD-10 principles by the clinicians. Studies conducted in Canada used semi-structured interviews and thematic analysis to identify the physician-related barriers to producing high-quality clinical coding from the viewpoint of coders (Lucyk et al., 2017; Tang et al., 2017). This study noted that these barriers should also be investigated from the viewpoint of physicians. Another study investigated the factors affecting accuracy of data abstraction from medical records and identified the role of training (Zozus et al., 2015).
Our results underscore the significance of interventions aimed at improving diagnosis documentation based on ICD principles and elaborating the importance of quality of management data such as diagnosis codes and their application in large-scale policymaking. Our results highlight the flaws and pitfalls of the current medical education program and underscore the need for alternative educational media such as e-learning and social networks. Physicians’ sociotechnical responsibilities about documentation would be increased by highlighting the applications of diagnosis coding such as reimbursement, quality care reporting and disease surveillance and monitoring. So far, there have been studies that focus on the improvement of documentation quality using in-person educational interventions (Farzandipour et al., 2012; Kulkarni et al., 2018; Otokiti et al., 2018; Walker et al., 2012). Nevertheless, IT-based interventions may prove to be more effective since they offer more flexible timings, which make them an easier fit for a typically busy physician schedule. Efficient monitoring, providing feedback as well as preventive and supportive policies may prove to be beneficial in improving ICD-based documentation.
Given the heavy workload of physicians and increasingly fast development of EHRs and their significant impact on the completeness and quality of clinical data (Nguyen et al., 2014), it is important to structure some of the most important fields such as the final diagnosis in the current EHRs and forms. This should be done so that it makes these EHRs compatible with principles of diagnosis documentation. When developing an EHR, incorporating the requirements of end users, and in particular physicians, plays an important role in the acceptance of information systems (Joukes et al., 2016). Furthermore, usability and user-friendliness of the system is effective in improving the completeness and quality of resulting data (Jensen and Bossen, 2016; Sidek and Martins, 2017). Therefore, it is vital to reflect on the barriers for the acceptance of technology by the physicians (Abdekhoda et al., 2015; Lluch, 2011). This will pave the way for the design of systems which can collect data that are compatible with principles of ICD and diagnosis documentation in an efficient and structured manner and over a reasonable time frame.
Conclusion
In the present study, influential factors in clinicians’ adherence to principles of diagnosis documentation were extracted. Poor adherence of clinicians leads to lower quality of management data, of which diagnosis codes are an important piece. CM was found as a suitable method to approach diagnosis coding from the viewpoint of different stakeholders. The most influential identified factors were “knowledge about ICD,” “need for facilitators and guidelines” and “explaining the importance of the issue and defining responsibilities” from the viewpoint of participants, respectively. Results were visualised using easy-to-understand plots that help policy makers and information system developers reach the best decisions. Using the importance-feasibility plot (Go-Zone), handling factors with high importance and feasibility will be more efficient. Findings from this study suggest that to improve the quality of documentation, the development of future EHRs should be based on international documentation guidelines and customised for different departments. As well, training of medical students should profoundly emphasise the necessity and importance of medical record coding. Finally, continuous monitoring and increased sociotechnical responsibility of clinicians in documentation should be reflected on as part of future healthcare policies.
Supplemental Material
sj-pdf-1-him-10.1177_1833358321991362 – Supplemental material for Factors affecting clinicians’ adherence to principles of diagnosis documentation: A concept mapping approach for improved decision-making
Supplemental material, sj-pdf-1-him-10.1177_1833358321991362 for Factors affecting clinicians’ adherence to principles of diagnosis documentation: A concept mapping approach for improved decision-making by Nafiseh Hosseini, Sayyed Mostafa Mostafavi, Kazem Zendehdel and Saeid Eslami in Health Information Management Journal
Footnotes
Acknowledgements
The authors would like to thank all participants of the study and Mashhad University of Medical Science for support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant provided by Mashhad University of Medical Science [970415].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.