
Abstract
Aim
To investigate developmental trajectories in early childhood and predictors of class assignment.
Methods
Data were available for Gen2 infants at 12 (n = 2275), 24 (n = 1845) and 36 (n = 2110) months of age in the Raine Study. Latent growth class analysis was used to identify developmental trajectories based on the Ages and Stages Questionnaire. Multivariate logistic regression analyses were used to estimate associations between foetal growth restriction, gestational age, child biological sex, breast feeding, parental age, socioeconomic factors and developmental trajectories.
Results
Two groups of infants were identified, one typically performing and one poorer performing. Being born early-term, pre-term and male were associated with poorer development. Not exposed to breastfeeding was associated with the lower trajectories in the adaptive and personal-social domains.
Conclusions
Developmental surveillance and advice for early-term infants should be considered. Findings highlight the continued need to support and promote breastfeeding as a protective mechanism for child development.
Introduction
Biological, social and economic risk and resilience factors during early childhood combine to influence the development of brain capacity to support the development of skills and learning (Shonkoff, 2003). Biological risk factors associated with increased risk of developmental delays include pre-term birth (Spittle et al., 2018), foetal growth restriction (FGR) (Levine et al., 2015) and male biological sex (O' Driscoll et al., 2018). Characteristics of the child’s broader social environment also contribute to developmental outcomes. For example, nearly half of children from under-resourced communities (e.g. low-income households) are developmentally vulnerable when starting school (Woolfenden et al., 2018). Under-resourced communities also suffer a higher burden of disability. For example, the prevalence of mild to moderate intellectual disability is higher where mothers are single, teenaged or under-resourced (Leonard et al., 2005). On the other hand, protective factors such as duration of breastfeeding can protect child development (Oddy et al., 2011).
Worldwide, 10% of children have developmental delays or disabilities (Clark et al., 2020). This is then associated with substantial individual and societal burden over the life course, including poorer physical and mental health (Shonkoff & Garner, 2012), high use of health services (Caspi et al., 2016), challenges to social inclusion and difficulties with productivity during adulthood (Palisano et al., 2017).
Earlier detection of children with poorer developmental performance is a key step in mitigating adverse long-term impacts. Early identification enables referral to early intervention services to take advantage of the heightened neuroplasticity of the developing brain, thereby optimising opportunities for learning (Finlay-Jones et al., 2019; Knudsen, 2004). To improve interpretation of early performance, understanding the trajectories of development across domains is required. Available population-based longitudinal studies of early development suggest differences in developmental trajectories between domains (Nishimura et al., 2016; Valla et al., 2017). Assessing Norwegian infants at six time points from 4 (n = 1246) to 24 (n = 677) months with the Ages and Stages Questionnaire (ASQ), two developmental trajectories were identified for communication, fine motor and personal-social domains, and three developmental trajectories were identified in the gross motor and problem-solving domains with varying proportions of children achieving high stable scores in each domain. Low gestational age, low Apgar score and male biological sex were associated with poorer developmental performance (Valla et al., 2017). Using the Mullen Scale of Early Learning (MSEL) in 952 Japanese infants from 1 to 24 months of age, five developmental trajectories were identified where 18.1% classified as delayed across all of the developmental domains, and delay in motor domains preceded delay in language domains (Nishimura et al., 2016). Similar to the Norwegian study (Valla et al., 2017), the risk factors for Japanese children in the delayed groups were pre-term birth, being small for gestational age, male biological sex and low maternal education (Nishimura et al., 2016).
Advancing understanding of the biological and environmental predictors of developmental trajectories can support differentiation between infants who are most in need of support (McManus et al., 2016). The primary aim of this study was to investigate patterns of developmental trajectories of infants from 12 months to 36 months of age in a cohort of Australian infants. A secondary aim was to identify early risk and protective factors that predict the child’s membership to a developmental trajectory.
Materials and Methods
Study Design and Setting
The Raine Study is an ongoing prospective, observational study examining the health and well-being of a Western Australian (WA) pregnancy cohort. Expectant mothers (generation 1 or ‘Gen1’) at antenatal clinics at and near King Edward Memorial Hospital were invited to participate at 18 weeks gestation if they had proficient English language skills, were expected to deliver at the hospital and intended to remain in WA (Straker et al., 2017). Between May 1989 and November 1991, a total of 2900 pregnant women were enrolled, there were 2868 live births (generation 2, or ‘Gen2’) between August 1989 and April 1992, including 60 sets of twins and two sets of triplets. The Raine Study participants were representative of the general WA population at the time of recruitment and into infancy (Straker et al., 2017; White et al., 2017). These data from 1989 and 1994 have current value because there are limited trajectory studies of developmental domains in early childhood, and findings can be compared to more contemporary datasets to evaluate secular trends.
Medical, obstetric history and sociodemographic data were collected on enrolment and updated during the 34th week of pregnancy with questionnaire and clinical assessment. Infants were assessed immediately after birth by a paediatrician or midwife. Follow-up assessments, including clinical assessments, questionnaires and interviews took place when the child was ∼12, ∼24 and ∼36 months of age.
Participants
To be included in the present study, the mother must have been participating in the Raine Study from 18 weeks’ gestation. The recruitment period was over 3 years, as such some mothers had more than one baby enrolled in the Study. To avoid multiple counting, 74 infants whose older siblings were already enrolled were excluded from the current study. In addition, one infant from each of the multiple births (n = 64) was randomly selected from each family. After further excluding non-participating families (i.e. did not participate in all three follow-up assessments, n = 255) and those with short inter-assessment period (<6 months, n = 37), the final number of live births available for follow-up at 12 months was 2438 infants and their families. The current study was approved by the Raine Study Scientific Review Committee (RA-4-1–2100) and Curtin Human Research Ethics Committee (HRE2018-0546).
Measures
Developmental Assessment
Child development was captured using the Infant Monitoring Questionnaire, now known as the Ages and Stages Questionnaire (ASQ) (Bricker & Squires, 1989). It was completed by parents when infants were 12 (n = 2,275, 93.3%), 24 (n = 1,845, 76.7%) and 36 (n = 2,110, 86.5%) months of age. The ASQ comprises five domains: gross motor, fine motor, communication, adaptive and personal-social skills (Bricker & Squires, 1989). For each domain, total scores (range from 0 to 6) with more than 2 missing items were considered missing. If one item was missing, missing item values were imputed using the mean domain score. Cut-off values to classify infants (1) in need of monitoring or continued surveillance, or (2) who were at risk and needed referral to early intervention services were derived for each domain from the ASQ manual (Squires & Bricker, 2009).
Sociodemographic Factors
Parental annual income was reported as the annual family income before tax and was grouped either below (<$24,000) or above (≥$24,000) the poverty line, according to Australian Bureau of Statistics data from 1991 (Whitehouse et al., 2012). Maternal education was categorised as (i) university degree; (ii) trade, diploma, TAFE certificate or professional registration; or (iii) no additional qualifications post-school past Year 12. Maternal and paternal ages at delivery were included as continuous variables.
Biological Factors
Peri and antenatal medical records were used to determine child biological sex, gestational age (GA) and FGR status. Ultrasound biometry or the date taken from the mother’s last menstrual period at delivery was used to determine GA. GA at birth was categorised by (i) < 37 weeks (pre-term); (ii) 37–38 weeks (early-term) or (iii) ≥ 39 weeks (full term). FGR is defined as a significant deviation from the expected foetal growth rate resulting from multiple adverse effects on the foetus (Sharma et al., 2016). To distinguish true growth restriction as opposed to infants who were constitutionally small, FGR was calculated from the predicted birth weight customised for GA, child biological sex, parity, maternal height, maternal weight, the presence of maternal anaemia and the placental weight (White et al., 2016).
Breastfeeding History
Breastfeeding was grouped by duration of exposure to breast milk, based on the available data: (i) not exposed to breastfeeding; (ii) breastfed up to 2 months; (iii) breastfed up to 6 months and (iv) over 6 months of breastfeeding. Data were not available on whether infants were exclusively breastfed or receiving mixed or complementary feeding.
Statistical Analysis
Latent Class Growth Analysis
Latent class growth analysis (LCGA) (Nagin, 2005) was employed to identify developmental trajectories for each ASQ domain as a continuous function of age from 1 (12 months) to 3 (36 months) years of age, with the intercept placed at 1 year. The analysis aimed to identify distinct subgroups of children who would follow a similar pattern of development over time, based on their ASQ performance. The ASQ domain scores at each time point were assumed to follow a censored normal distribution with a minimum and maximum value of 0 and 6, respectively. The trajectories were estimated for participants who provided data for at least one of the three time points, and missing data were handled by using full information maximum likelihood assuming they were missing at random. The number of latent classes was initially unknown, and models were run from simple one-class solutions through to five-class solutions. To allow heterogeneity in magnitude and direction of change between trajectories, different combinations of continuous latent growth parameters (i.e. intercept, linear slope and quadratic slope terms) for each class solution were investigated. Each model was interrogated and models containing non-significant (i.e. p > .05) terms were excluded. To ensure that the optimum model was selected, the number of trajectories was selected by interpreting and comparing the Bayesian Information Criterion (BIC) (Andruff et al., 2009), the posterior probability and the group membership probability. The BIC is a fit index and is used to compare competing models that include different numbers of trajectories or trajectories of various shapes (e.g. linear versus quadratic) (Andruff et al., 2009). The estimate of the log Bayes factor defined here (2(BICc – BICc-1)) allows comparison of more complex versus simpler models (Jones et al., 2001). A value greater than 10 was deemed acceptable as guidelines suggest this value indicates ‘very strong evidence’ surrounding the more complex model and thereby ensuring parsimony (Jones et al., 2001). To further assess optimal number of classes, both the group-specific average posterior probabilities (AvePP) and the probability of group membership for each trajectory were examined. An AvePP value of more than 0.7 for each group was stipulated (Nagin, 2005). The group membership probability equates to the proportion of infants belonging to a given group using the maximum-probability assignment rule, and a probability of at least 5% of the participants in the smaller group was required (Andruff et al., 2009).
Logistic Regression
Logistic regression was used to identify protective and risk factors that influence membership of a developmental trajectory. Independent variables including biological sex, pre-term birth, FGR, paternal and maternal age, maternal education level, family income and breastfeeding, were used as predictors. All statistical analyses were undertaken with Stata version 15 (StataCorp, College Station, TX, USA) and the user-written command ‘traj’ (Jones et al., 2001).
Results
Characteristics of 2438 infants and their parents (n (%) or median (IQR)).
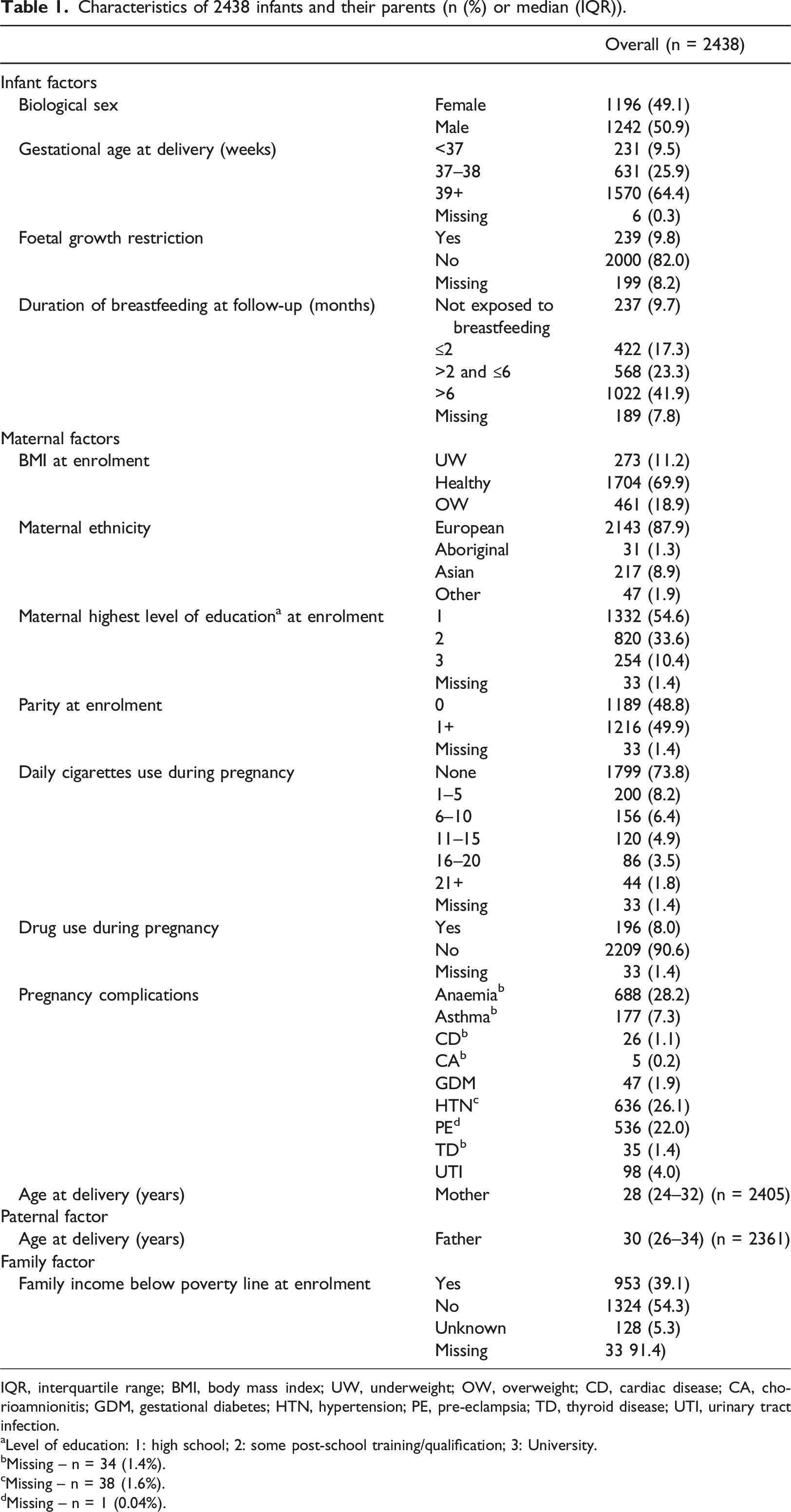
IQR, interquartile range; BMI, body mass index; UW, underweight; OW, overweight; CD, cardiac disease; CA, chorioamnionitis; GDM, gestational diabetes; HTN, hypertension; PE, pre-eclampsia; TD, thyroid disease; UTI, urinary tract infection.
aLevel of education: 1: high school; 2: some post-school training/qualification; 3: University.
bMissing – n = 34 (1.4%).
cMissing – n = 38 (1.6%).
dMissing – n = 1 (0.04%).
Developmental Trajectories
Descriptive statistics of Ages and Stages Questionnaire (ASQ) domain scores at 12-, 24- and 36-month follow-up in 2,438 Raine Study participants.
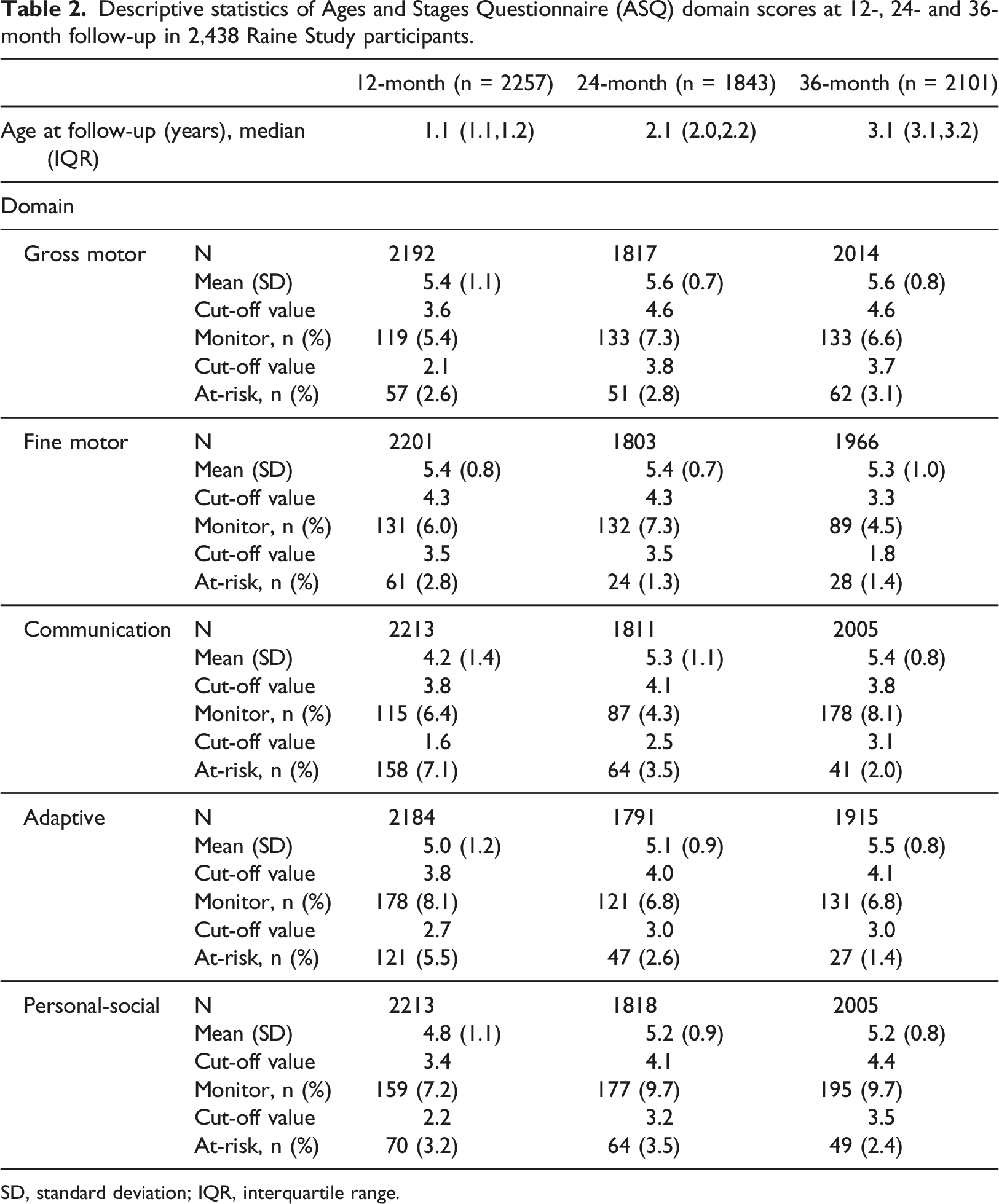
SD, standard deviation; IQR, interquartile range.
Comparison of latent class trajectory models by Ages and Stages Questionnaire (ASQ) domain.
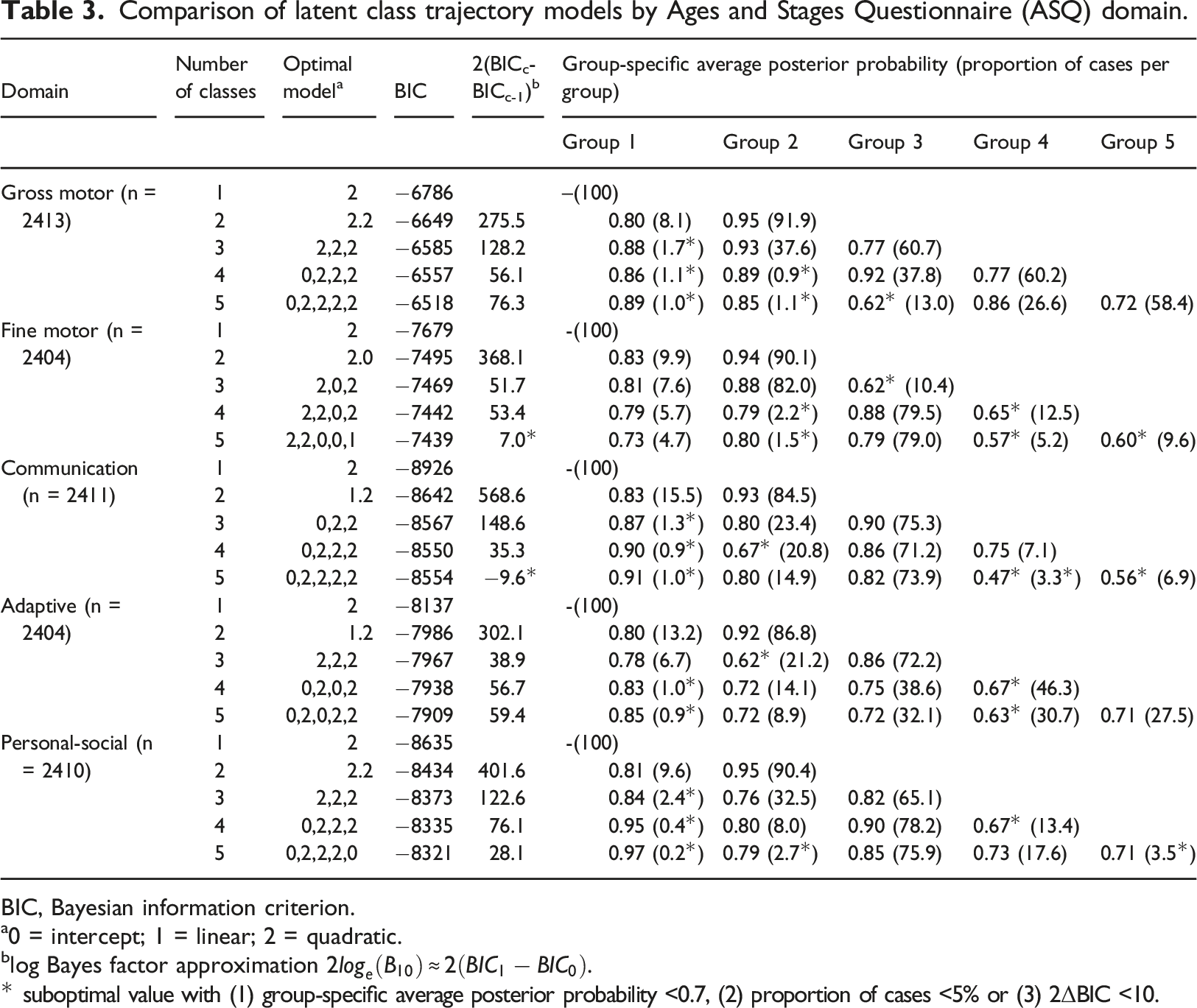
BIC, Bayesian information criterion.
a0 = intercept; 1 = linear; 2 = quadratic.
blog Bayes factor approximation
* suboptimal value with (1) group-specific average posterior probability <0.7, (2) proportion of cases <5% or (3) 2ΔBIC <10.
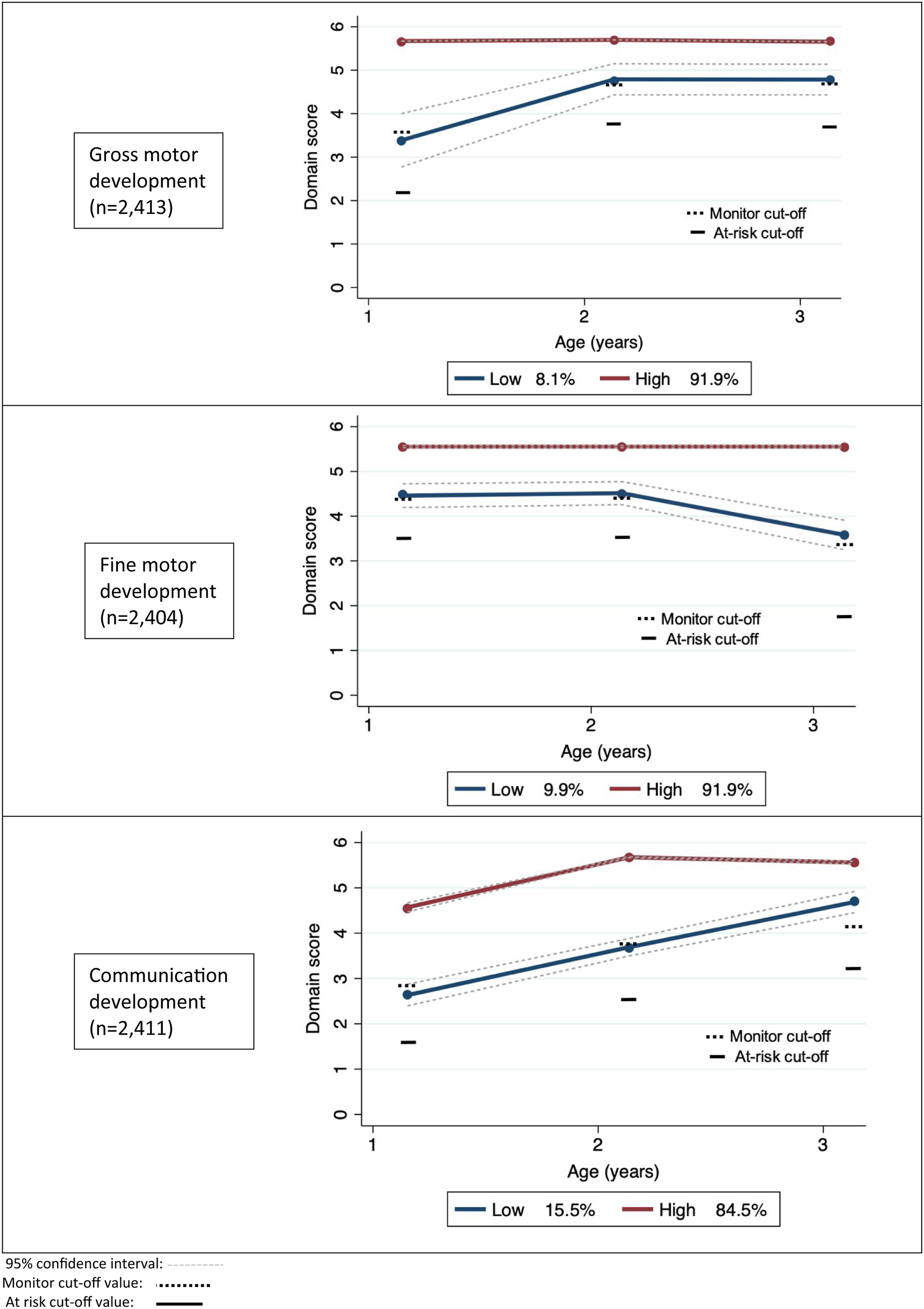
Distinct trajectories (low and high performing) of Ages and Stages Questionnaire (ASQ) gross motor, fine motor and communication development from age 12–36 months and their group membership probability.
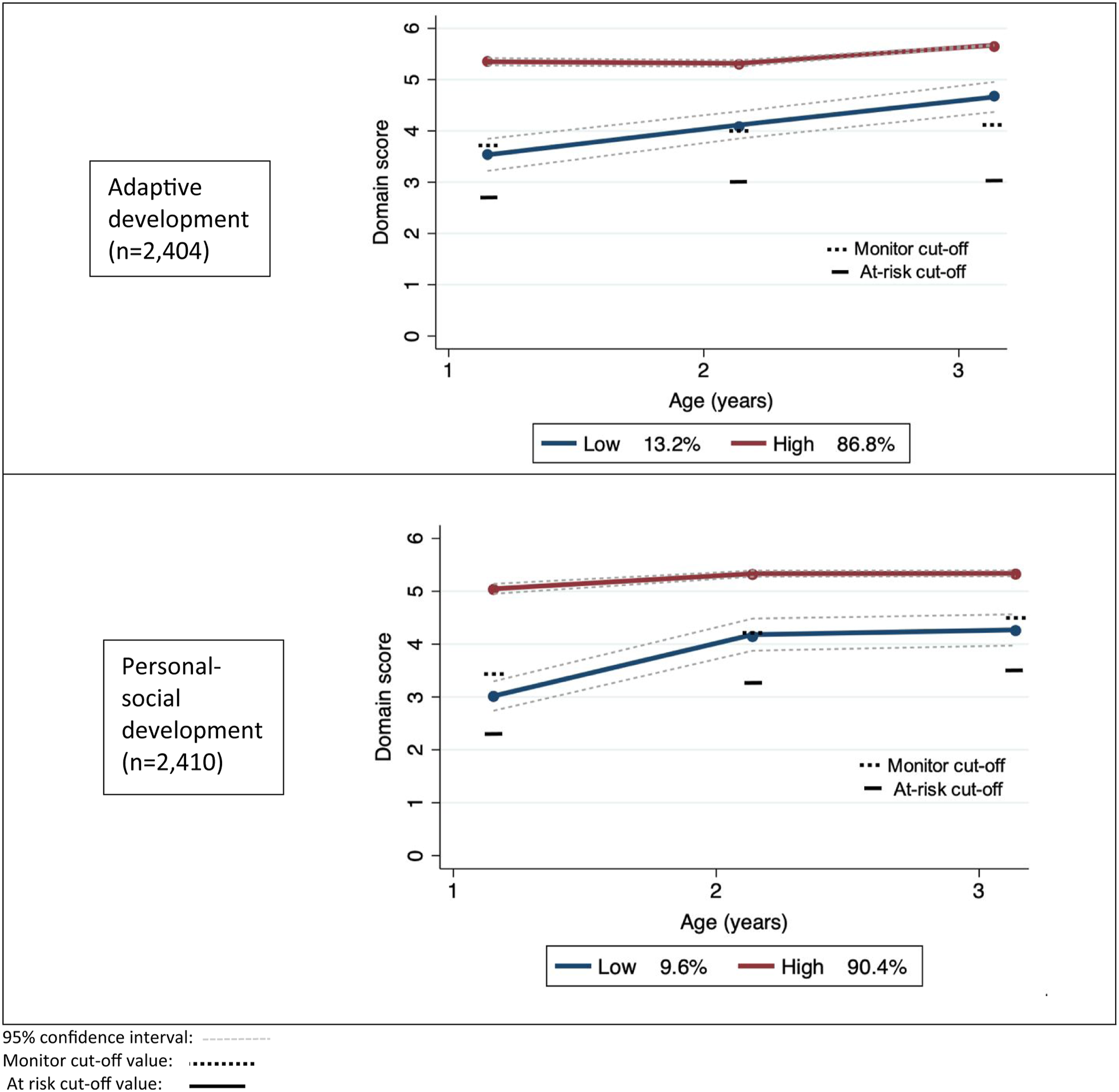
Distinct trajectories (low and high performing) of Ages and Stages Questionnaire (ASQ) adaptive and personal-social development from age 12–36 months and their group membership probability in 2404 infants.
In the high performing group, gross motor, fine motor, adaptive and personal-social trajectories were stable from 12 to 36 months of age. Communication scores were lower at 12 months but high and stable at 24 and 36 months. Within the low performing group, there was more variability in trajectory shape across the five domains. Scores at all three time points for all domains were close to the ASQ monitoring cut-off values. Scores at 12 months were low in the gross motor, communication, adaptive and personal-social domains, and then increased but remained lower than the high performing group at 36 months. From 24 months, the fine motor skills of infants in the low performing group diverged downwardly from that of peers in the high performing group. Whereas divergence between the high and low performing groups was different for each domain, the low performing group did not catch up with the high performing groups by 36 months. The scores at each assessment time point for all domains of the low performing group indicate that monitoring of children may have been beneficial (Figures 1 and 2).
Predictors of Group Membership
Comparisons of the relative risk of belonging to the low performing group versus high performing group for selected predictors by Ages and Stages Questionnaire (ASQ) domain for the multivariate model.
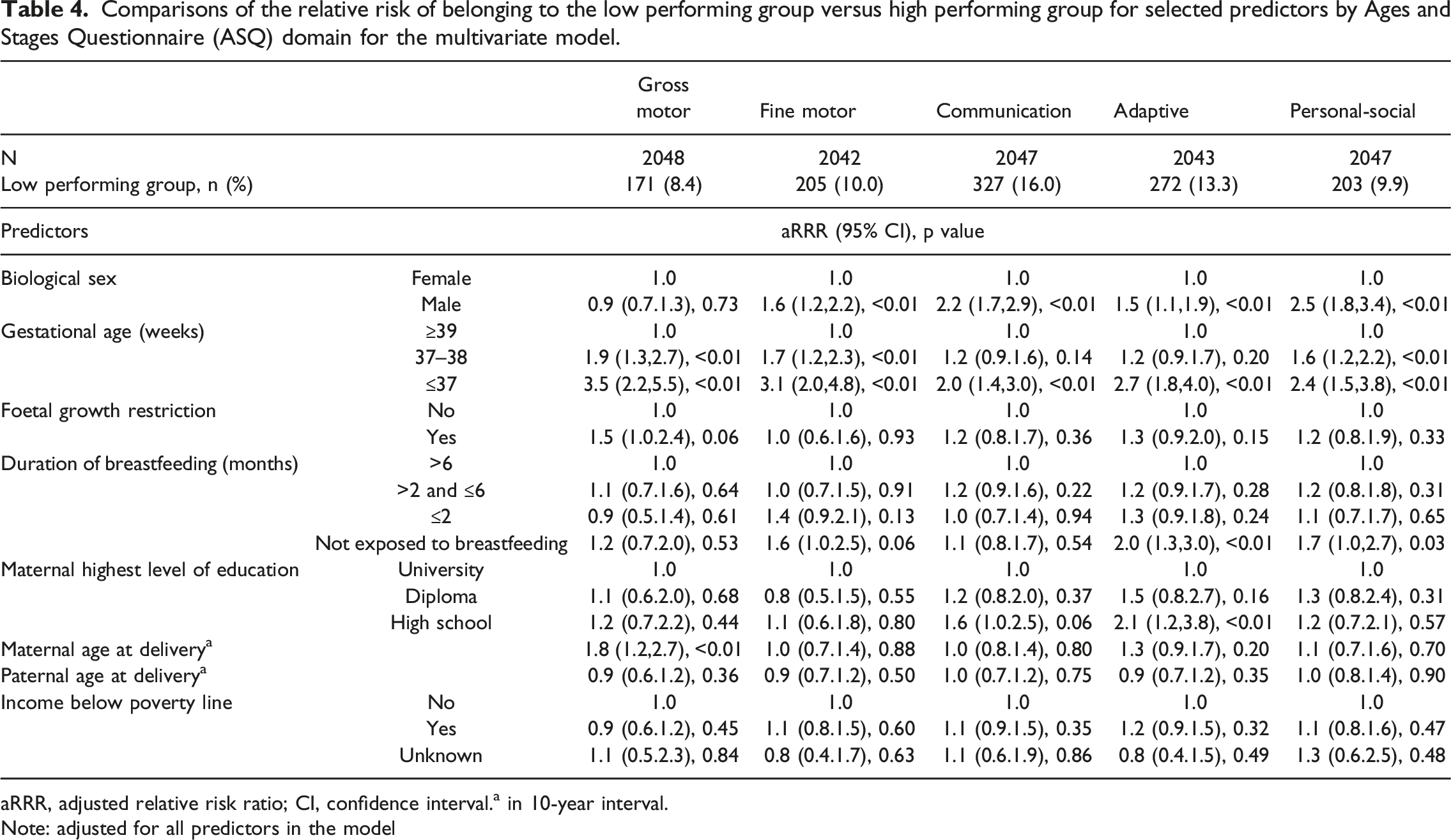
aRRR, adjusted relative risk ratio; CI, confidence interval.a in 10-year interval.
Note: adjusted for all predictors in the model
Gross motor domain: Pre-term birth conferred the greatest risk to gross motor performance (aRRR 5.9; 95% CI 2.5.14.1), although high risk was also observed in infants born early-term (aRRR 3.5; 95% CI 2.2.5.5), infants with FGR (aRRR 1.5; 95%C CI 1.0.2.4) and with every additional year in maternal age at birth (aRRR 1.8; 95% CI 1.2.2.7).
Fine motor domain: Pre-term birth was associated with more than three times (aRRR 3.1; 95%CI 2.0.4.8) and early-term birth had nearly twice (aRRR 1.7; 95% CI 1.2.2.3) the risk of being in the low performing group. Male biological sex (aRRR 1.6; 95% CI 1.2.2.2) and not exposed to breastfeeding (aRRR 1.6; 95% CI 1.0.2.5) were associated with greater risk.
Communication domain: Male biological sex (aRRR 2.2; 95% CI 1.7.2.9) and pre-term birth (aRRR 2.0; 95% CI 1.4.3.0) were associated with twice the risk of belonging to the low performing communication group. Risk was increased when maternal education was limited to high school (aRRR 1.6; 95% CI 1.0.2.5).
Adaptive domain: Pre-term birth was associated with nearly a threefold increased risk of belonging to the low performing group (aRRR 2.7; 95% CI 1.8.4.0). Those who were not exposed to breastfeeding (aRRR 2.0; 95% CI 1.3.3.0) or whose mothers had no additional qualifications post-school (aRRR 2.1; 95% CI 1.2.3.8) had approximately twice the risk. Male biological sex (aRRR 1.5; 95% CI 1.1.1.9) was associated with smaller increase in risk of belonging to the low performing group.
Personal-social domain: Male biological sex was associated with more than twice the risk of belonging to the low performance group (aRRR 2.5; 95% CI 1.8.3.4) as was pre-term birth (aRRR 2.4; 95% CI 1.5.3.8). Infants born early-term also had increased risk of low performance (aRRR 1.6; 95% CI 1.2.2.2).
Discussion
This longitudinal study demonstrated that most infants had stable developmental trajectories between 12 and 36 months of age with ASQ scores within the normal range. A smaller group of infants had a trajectory with consistently poorer performance at all three time points. Risk factors for poorer development included being born early-term, pre-term and male biological sex.
Previous longitudinal population studies have suggested different numbers of developmental groups and patterns of development. For example, five groups comprising three normal and two delayed trajectories were identified following administration of the MSEL on seven occasions from 1 month to 24 months (Nishimura et al., 2016). Alternatively, Valla et al., used the ASQ on six occasions from 4 to 24 months and identified three groups for the gross motor and adaptive functioning domains and two groups for the fine motor, communication and personal-social domains (Valla et al., 2017). Conflicting findings between the studies could be explained by differences in sociocultural factors that influence antenatal care and child rearing practices, developmental tests, length of follow-up and assessment frequency. Standardised assessment frequencies and measures are necessary if we are to gain consistent insights into similarities and differences in developmental trajectory classes across populations and time.
Our study found 15.5% of infants or less were in the low performing group for all domains, broadly similar with previous trajectory studies (3%–18% of infants by 24 months (Nishimura et al., 2016; Valla et al., 2017)). Developmental monitoring was indicated by the average scores in our low performing group, which were consistently below the high performing group, and did not show catch up at 36 months. This trajectory over 36 months suggests that children in the low performing group might benefit from early intervention as previous work has demonstrated the predictive utility of 36–48 month ASQ scores on special education use (Kerstjens et al., 2009), IQ (Charkaluk et al., 2017) and school difficulties (Halbwachs et al., 2014) at age 5–6 years. The linking of early developmental assessments to evaluations of child development at school entry is an essential next step, to understand strategies for early childhood policies to support child performance when at school.
More nuanced differences in the shapes of the trajectories were observed. For example, infants in the low performing trajectory group failed to ‘catch up’ to their higher performing peers by 36 months, consistent with the findings in the Japanese study of infants to 24 months (Nishimura et al., 2016). In contrast, the Norwegian study illustrated catch up by 24 months of age, except for the communication domain (Valla et al., 2017). There were similarities. In our low performing group, gross motor and personal-social domain scores increased between 12 and 24 months, fine motor scores declined between 24 and 36 months and communication and adaptive development scores steadily increased from 12 to 36 months. These observations align with the Japanese where deviation from the higher performing groups was most marked in the motor domains at 10 months of age and deviation within the language domain was apparent after 12 months of age (Nishimura et al., 2016). It has been proposed that attaining motor skills during infancy provides opportunity to interact physically in the environment and creates new learning opportunities, in turn promoting cognitive development (Thelen, 1989) and allowing a cascade of learning in other developmental domains (Oudgenoeg-Paz et al., 2017). Motor delays in infancy can be a precursor to delays in other domains of development and suggest need for more detailed assessment.
Pre-term or early-term birth and male biological sex have previously been associated with poorer ASQ scores at 12 months of age for this population (Baumgartel et al., 2020). In this analysis, these same risk factors were associated with greater probability of belonging to the low performing developmental trajectory to 36 months, in agreement with other trajectory studies (Nishimura et al., 2016; Valla et al., 2017). The adverse sequelae of pre-term birth (<37 weeks) on neurodevelopment are well known (Saigal & Doyle, 2008). The developmental outcomes of early-term (37–38 weeks) infants are less well understood. Our results indicated that early-term infants were more likely to be assigned to the low performing trajectory across all domains. This might be because a large portion of brain maturation takes place in the last four to 5 weeks of gestation (Saigal & Doyle, 2008). The population attributable fraction for early-term birth could be relatively high because of the higher prevalence of early-term birth compared to pre-term birth. As such, surveillance and delivery of support strategies, such as in play groups for population scale, for both pre-term and early-term infants could yield advantages to these children’s development.
Membership to the low developmental performance trajectory was more likely for biological males in the fine motor, communication, personal-social and adaptive ASQ domains, consistent with previous trajectory studies (Nishimura et al., 2016; Valla et al., 2017) and observations of their greater vulnerability to early biological pressures during childhood (O' Driscoll et al., 2018) and later sequelae such as intellectual disability (Bourke et al., 2016). Advancing maternal age was associated with increased risk of poorer performance in the gross motor domain trajectories whereas advancing paternal age had a seemingly protective effect, each observation in the opposite direction to the risks reported in the Nishimura study (Nishimura et al., 2016). We note that the longer duration of follow-up in our study could yield different findings in relation to the presence of a neurodevelopmental condition. For example, a population-based birth cohort study found that children with mild intellectual disability were more likely to have younger parents, and children with autism and comorbid intellectual disability were more likely to have older parents (Leonard et al., 2011).
While duration of breastfeeding was not investigated as a factor in the Japanese nor Norwegian trajectory studies, not exposed to breastfeeding was associated with the low trajectories in the adaptive and personal-social domains in our current study. This is consistent with another analyses of Raine data suggesting that breastfeeding for less than 4 months increased the risk of atypical development between 1 and 3 years (Oddy et al., 2011) and not exposed to breastfeeding was associated with language delay at 5 and 10 years (Whitehouse et al., 2011). At the time of data collection for the current study (1989–1991), the Australian National Health and Medical Research Council recommended exclusive breastfeeding for at least the first 4 months, based on the World Health Organisation’s recommendations (World Health Organisation, 2010). Data collected in the 1989–1990 National Health Survey indicated that 77% of Australian infants were breastfed at 2 months, 75% at 6 months and 72% at 12 months (Australian Bureau of Statistics, 1991). These proportions are substantially higher than observed in our current study but are likely an over-estimation of breastfeeding rates due to methodological flaws in the survey (Lund-Adams & Heywood, 1994). Exclusive breastfeeding fractions in 2020–21 were 75% at 2 months and 35% at 6 months, 50% of infants were receiving mixed or complementary breastfeeding at 12 months (ABS, 2022). Australia continues to fall short of meeting the targets for exclusive breastfeeding for infants up to 6 months, despite the strong evidence that exclusive and mixed breastfeeding confer physical and cognitive benefits to the child, including reduced risk of chronic diseases such as type I and type II diabetes, cardiovascular disease and obesity (Binns et al., 2016). These findings highlight the need for continued attention to this public health policy.
The main strength of this study is the use of data from a large pregnancy cohort, where children were followed at multiple time intervals up until 36 months of age. The dataset also provided a wide range of pre- and post-natal biological and environmental factors, which allowed multiple risk and protective factors to be analysed. The selection bias of the Raine Study has been evaluated with an exposure-outcome association analysis and suggests that there is no apparent resulting bias (White et al., 2017) and population-representativeness was maintained over the follow-up period (Straker et al., 2017), which may allow generalisability for other populations of infants. However, changes in population characteristics such as relating to economic wealth and immigration change which could limit ongoing generalisability.
We recognise limitations. The ASQ fails to capture infant irritability and disruptive behaviour which can help in identifying developmental vulnerability (Wakschlag et al., 2018) or young children who have experienced trauma (Choi et al., 2019). Although the ASQ is a valid parent-reported assessment tool it may lack sensitivity to more subtle development impairments and there could be an element of reporting error, leading to over- or under-estimation of developmental difficulties. Our trajectories captured development up to 36 months of age and we are therefore unable to comment how developmental vulnerabilities become apparent during the later stage of early childhood. The trajectory analysis was limited by some missing data, but the issue was largely overcome by using full information maximum likelihood estimation to enable inclusion of nearly all children. Due to the limitations of the group-based trajectory modelling software used, model selection was carried out using information criteria measures only. Additional socioeconomic factors such as parental occupation and area of residence could also have influenced class membership. Finally, breastfeeding status was classified by the duration of the infant receiving breast milk. We acknowledge that there is variation in classifications of breastfeeding across the literature, often classified as exclusive or predominant breastfeeding, or a mix of breast/complementary feeding (Labbok & Starling, 2012).
Conclusion
With limited developmental trajectories in the literature, this longitudinal study provides further insights into early childhood developmental trajectories. Their linkage with developmental vulnerabilities at school entry is an important next step. Findings indicate that early-term and pre-term born infants are particularly vulnerable to having poorer developmental trajectories and mechanisms for developmental surveillance and advice for early-term infants should be considered. The findings also highlight the continued need to promote breastfeeding as a protective mechanism for early child development. Early childhood developmental surveillance programs monitor trajectories and have an important role in early identification and timely referral to at-risk children to early intervention pathways.
Footnotes
Acknowledgements
We are grateful to the Raine Study participants and their families, and we thank the Raine Study research staff for cohort coordination and data collection. The core management of the Raine Study is funded by the University of Western Australia, Curtin University, Telethon Kids Institute, Women and Infants Research Foundation, Edith Cowan University, Murdoch University, The University of Notre Dame Australia and the Raine Medical Research Foundation. The collection of antenatal and perinatal data was funded by the Raine Medical Research Foundation and the collection of one-year follow-up data was funded by the NHMRC and the Raine Medical Research Foundation. The funders for the data collection have had no part in determining the study design, analysis and collection of data, writing this manuscript and publication decisions. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The collection of antenatal and perinatal data was funded by the Raine Medical Research Foundation and the collection of one-year follow-up data was funded by the NHMRC and the Raine Medical Research Foundation. There was no funding for the current data analyses. The funders for the Raine Study have had no part in determining the study design, analysis, and collection of data, writing this manuscript and publication decisions.