
Abstract
Aim:
To evaluate the radiological outcomes of femoral head osteonecrosis (FHO) in children with sickle cell disease (SCD), comparing non-operative treatment (bisphosphonates) and head-preserving surgical interventions—core decompression with bone marrow aspirate concentrate (CD-BMAC) and proximal femur reorientation osteotomy (PFRO)—by analyzing changes in Steinberg stage before treatment to final follow-up.
Methods:
Retrospective review of 28 hips from 17 pediatric SCD patients treated between 2010 and 2024, analyzed patient demographics, disease stage, treatment modalities, disease progression, and follow-up duration; and compared pre-collapse and post-collapse stages.
Results:
Among 75 hips with FHO in 51 children, 61 (81%) were non-traumatic. Of the 28 hips (13 pre-collapse, 15 post-collapse) in 17 children (mean age 11.6 years; 58.8% male), the average interval from SCD diagnosis to FHO onset was 78.8 months (Standard deviation-36.6). Treatments included bisphosphonates (11 hips), CD-BMAC (5), and PFRO (6). After excluding salvage procedures and lost follow-up, 20 hips were available for the final outcome analysis. At final follow-up (mean 30.7 months), FHO improved or remained stable in 15 hips (75%), while it progressed by at least 1 Steinberg stage in 5 hips (25%). In pre-collapse hips, no further disease progression was seen. In post-collapse cases, progression was noted in three of five bisphosphonate-treated hips and two CD-BMAC-treated hips; PFRO-treated hips showed no progression. Two hips developed arthritis.
Conclusion:
Bisphosphonates, CD-BMAC, and PFRO prevent disease progression in pre-collapse hips. In post-collapse hips, PFRO showed no further progression, while CD-BMAC and bisphosphonates showed mixed results.
Significance of Study:
Early radiological screening and intervention before femoral head collapse is critical to preserving joint anatomy.
Level of Evidence:
Level IV
Keywords
Introduction
Femoral head osteonecrosis (FHO) is a degenerative condition marked by reduced blood flow to the femoral head, resulting in bone death and potential collapse. 1 In children, FHO can lead to severe pain, disability, and joint deterioration. While the exact cause remains unclear, contributing factors may include corticosteroid use, sickle cell disease (SCD), trauma, infections, and idiopathic origins. 2 Treating FHO in children is particularly challenging and remains controversial due to the lack of consensus on the best approach and timing for intervention. Without targeted treatment, around 80% of clinically diagnosed FHO cases worsen, often leading to the need for hip arthroplasty. 3 The primary treatment goals are to preserve the shape and functionality of the femoral head, decelerating the progression of osteonecrosis, and preventing the need for total hip arthroplasty (THR). 4
In pediatric populations, SCD is a leading cause of non-traumatic FHO, 5 with about 28% of children with SCD developing FHO. 6 Radiography is the primary imaging method used to track structural changes and monitor the progression of osteonecrosis. 4 However, magnetic resonance imaging is considered the gold standard for diagnosing osteonecrosis due to its high sensitivity in detecting early signs. 7 The University of Pennsylvania classification, developed by Steinberg et al., aims to precisely outline the progression of osteonecrosis, differentiate between stages, compare management methods, and provide prognostic information to guide and determine the best treatment approach.8,9
Various treatment modalities have been used in the management of FHO in children. Intravenous bisphosphonate (BP) therapy for FHO in children with SCD, has been found to positively impact the treatment of painful bone morbidity. 10 Core decompression of the femoral head removes the necrotic core and decompresses the femoral head, leading to the restoration of intraosseous pressure. 11 Combining bone marrow stem cell implantation with core decompression for treating FHO, has shown to enhance regeneration and facilitate the remodeling of the necrotic bone.12 –14 Proximal femoral reorientation osteotomy (PFRO) has been performed in pediatric patients with FHO to reposition the necrotic or collapsed segment away from the weight-bearing region of the hip joint or to improve femoral head coverage, thereby minimizing mechanical loading stress.15,16
Despite the wealth of data on FHO in adults, there is a notable lack of information regarding outcomes in pediatric patients. 4 Although osteonecrosis is a recognized complication of SCD, the literature on the effectiveness of bisphosphonates and osteotomy for FHO in children with SCD is limited. Comprehensive studies comparing the efficacy of different treatment modalities for osteonecrosis in pediatric population are scarce. This study aims to address these gaps and provide more definitive guidance on managing FHO in children with SCD, offering insights into the disease characteristics, treatment outcomes, and factors influencing the progression and management of FHO in children with SCD.
The primary objective is to compare the radiological outcomes of different treatment modalities for managing FHO in children with SCD, like non-operative (bisphosphonates) and head-preserving surgeries (core decompression (CD) and bone marrow aspirate concentrate (BMAC), proximal femur reorientation osteotomy (PFRO)), by assessing the Steinberg stage of FHO prior to treatment and at final follow-up.
The secondary objectives include describing the demographic and clinical characteristics of children with SCD who develop FHO, determining the average time between the onset of SCD and the diagnosis of FHO, and identifying factors associated with disease progression and the development of arthritis in these patients. Additionally, this study aims to evaluate the effectiveness of different treatment modalities (bisphosphonates, CD-BMAC, and PFRO) in managing FHO in both pre-collapse and post-collapse stages.
Materials and methods
This study was a single-center retrospective analysis conducted at a tertiary-care pediatric referral center, focusing on FHO in children with SCD. Approval was obtained from the institutional review board before commencing the study. The electronic medical records of the hospital from 2010 to 2024 were cross-referenced to identify children who met the study’s inclusion criteria.
Initial institutional screening identified 75 hips for application of study criteria. Inclusion criteria were children diagnosed with FHO in the context of SCD who received treatments such as bisphosphonate infusion, core decompression with BMAC injection, proximal femur reorientation osteotomy (PFRO), and salvage surgeries. Children were excluded if they had FHO due to other causes such as Perthes disease, trauma, steroid use, malignancy, chemotherapy, or other blood dyscrasias. The sample size comprised of all eligible patients identified during the 14-year study period.
For each patient, baseline characteristics, diagnosis details, and treatment records documenting conservative or operative methods, as well as the duration of follow-up, were recorded from their electronic medical records. The hospital’s picture archiving and communication system was utilized to review each patient’s pre-operative and final follow-up radiographs.
The collected data were analyzed to assess patient demographics, disease stage, treatment modalities, disease progression, follow-up duration, and comparisons between hips in the pre-collapse and post-collapse stages. The data were categorized based on the treatment modalities received, such as non-operative (bisphosphonate infusion), head-preserving (CD-BMAC/ PFRO), and salvage surgeries. The choice of treatment modality was based on surgeon preference and experience rather than a randomized clinical protocol. Subgroup analysis was performed based on the femoral head Steinberg stage, dividing them into pre-collapse and collapsed head stages. The reconstitution of the femoral head was evaluated through follow-up plain radiography, and any residual deformity at final follow-up was recorded. The hips were classified using the Steinberg system both pre-operatively and at final follow-up. Successful treatment was defined as the absence of radiological progression of the FHO Steinberg stage. 17 Disease progression was defined as at least one Steinberg stage progression, from presentation to final follow-up. Progression to arthritis was defined as stage progression to Steinberg stage 6, at final follow-up.
Statistical analysis included descriptive statistics for all variables, such as mean, standard deviation, frequency, and percentage, to describe the demographics and characteristics of the study participants. Statistical analysis was performed using SPSS software (IBM) 21. Due to the small sample sizes, formal comparative statistical analyses were not performed as they would be underpowered and potentially misleading.
Results
A total of 75 hips with FHO in 51 children were identified for application of the study criteria. Among these, 61 hips (81%) were due to non-traumatic etiology, while 14 were secondary to trauma. Out of the 75 hips, 47 were excluded from the study for various reasons: 20 were secondary to steroids, 14 post-traumatic cases, 6 with thalassemia, 5 atypical presentations without an identifiable cause, 1 with septic sequela, and 1 post-chondroblastoma of femoral head. Twenty-eight hips in 17 children with FHO and underlying SCD were available for study inclusion (Figure 1).
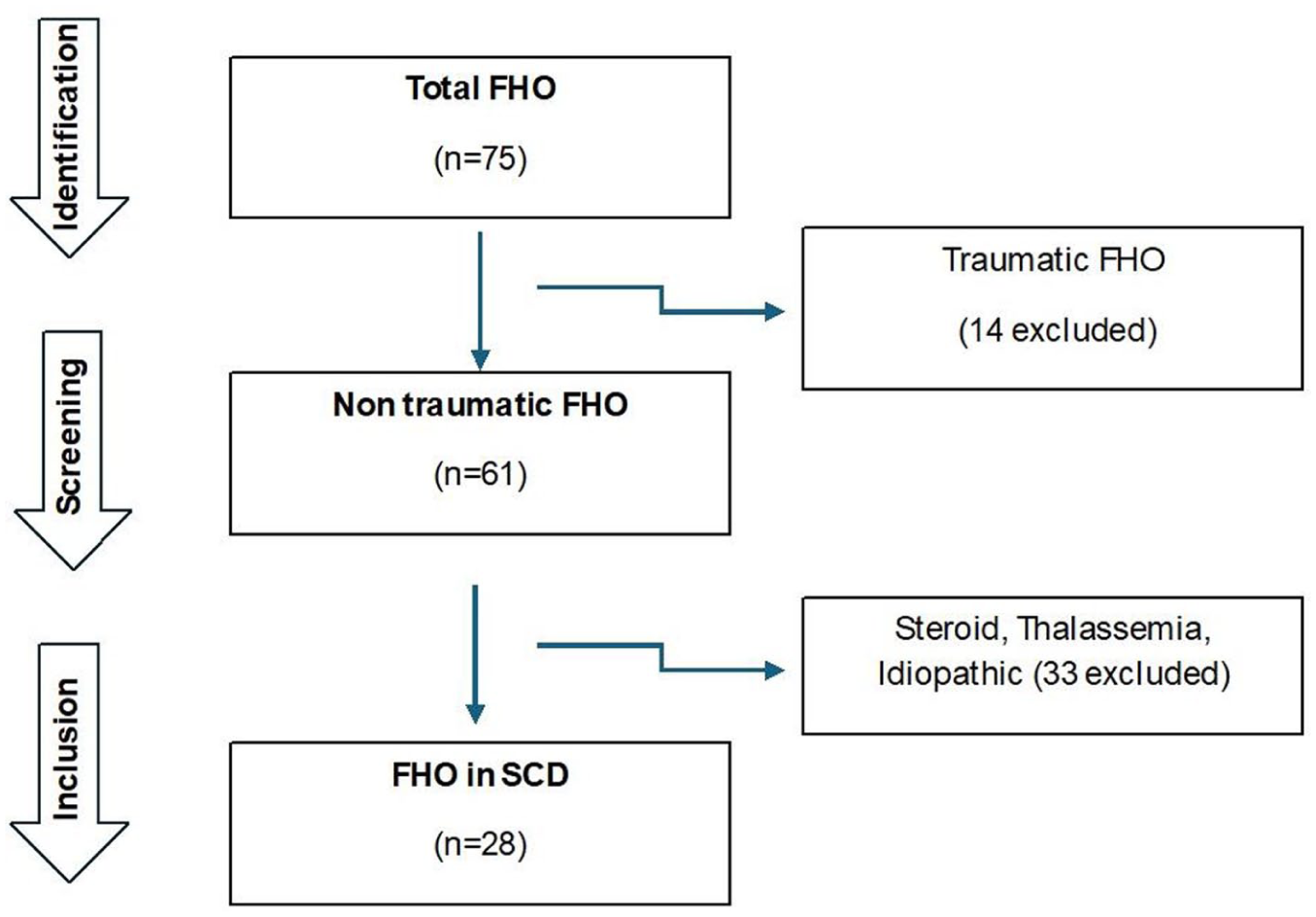
STROBE diagram illustrating the patient selection process.
The baseline characteristics of the 28 hips (17 patients) are detailed in Table 1. The age at presentation ranged from 6 to 15 years with a mean of 11.6 years (Standard deviation (SD) 2.8). The cohort was predominantly male, with slightly more than half of the hips having collapsed at the time of diagnosis. Eleven patients (64.7%) had a bilateral involvement at presentation. The interval between SCD onset and FHO diagnosis was 78.8 months (SD 36.6). Systemic treatment information was retrieved for the cohort, with hydroxyurea administered to 15 out of the 17 children (88.2%). Hemoglobin variant testing data were available for 14 children; 13 (76.5%) showed a homozygous HbSS genotype, while 1 (5.9%) had a heterozygous HbSD-Punjab genotype. Genotypic data were missing for three patients.
Baseline characteristics of the 28 hips included after screening criteria.
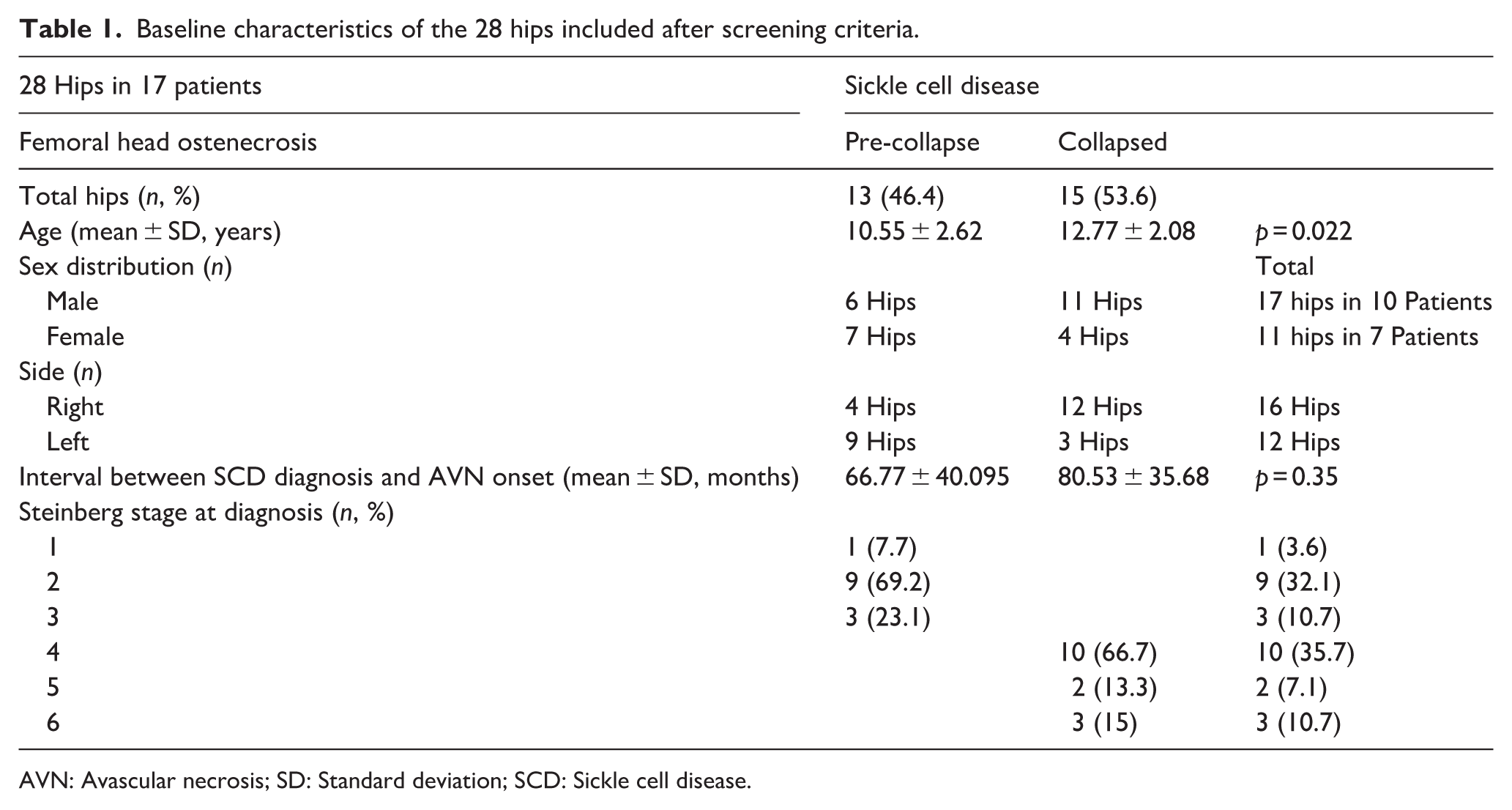
AVN: Avascular necrosis; SD: Standard deviation; SCD: Sickle cell disease.
Among the pre-collapse hips, 69.2% (9 out of 13) were classified as Steinberg stage 2, while the majority of the collapsed hips, 66.7% (10 out of 15) were categorized as stage 4. Patients received non-operative, head-preserving, or salvage procedures as outlined in Table 2.
Treatment distribution in the 28 hips included after screening criteria.
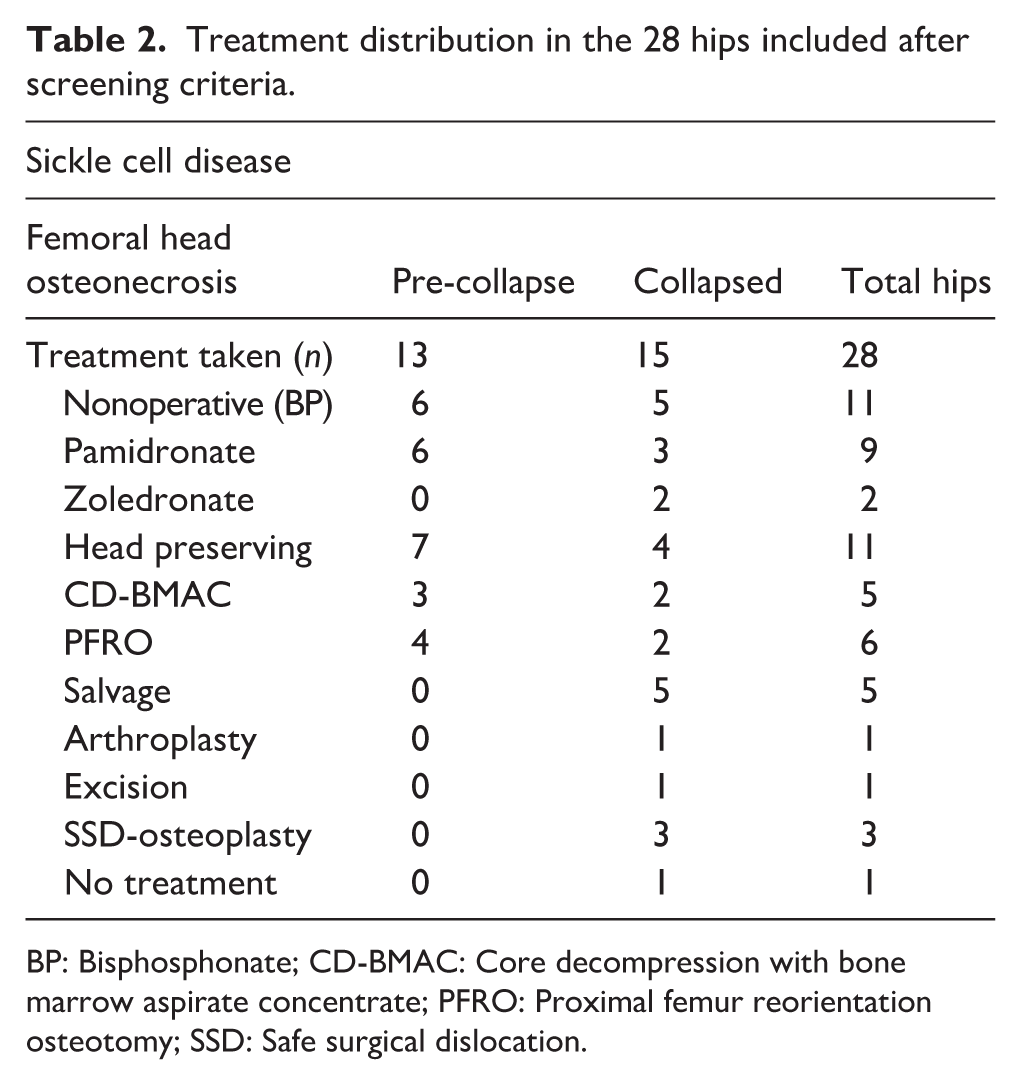
BP: Bisphosphonate; CD-BMAC: Core decompression with bone marrow aspirate concentrate; PFRO: Proximal femur reorientation osteotomy; SSD: Safe surgical dislocation.
Post-treatment, 2 hips were lost to follow-up, and 20 hips were available for the final outcome analysis. Of the 20 hips included, 15 (75%) demonstrated successful treatment, with no progression in Steinberg stage at final follow-up. Disease progression, defined as advancement by at least one Steinberg stage, was observed in five hips (25%). Among the five hips that progressed, two hips (10%) progressed to arthritis at final follow-up. The mean follow-up duration was 30.7 months (SD-4.5).
On subgroup analysis, among the 13 hips in the pre-collapse stage, 6 received bisphosphonate infusion (Figure 2), 3 underwent CD-BMAC (Figure 3), and 4 underwent PFRO (Figure 4). Among the post-collapse hips, five received bisphosphonate infusion, two underwent CD-BMAC, and two underwent PFRO.
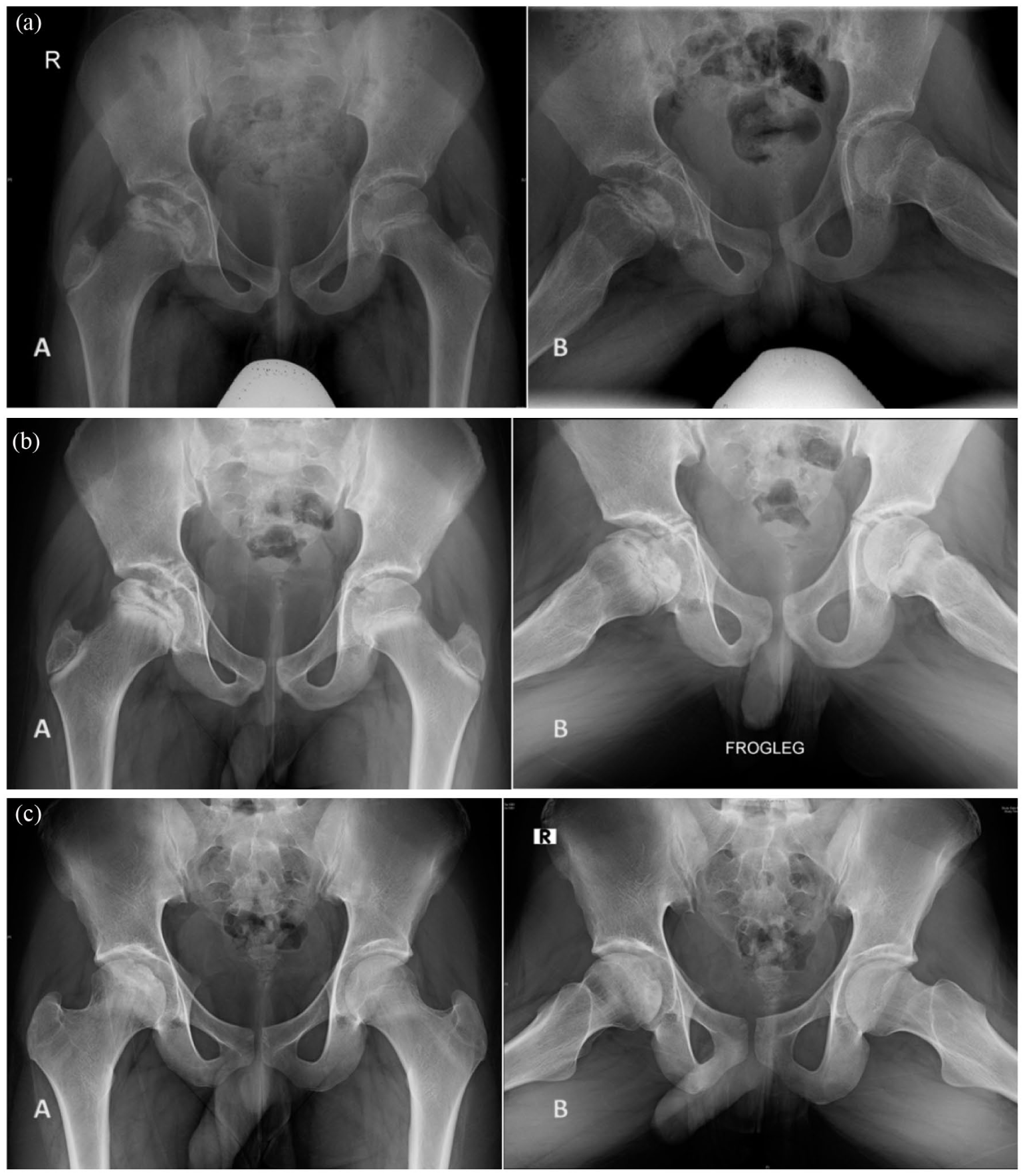
(a) Initial plain radiographs of a 13-year-old male with Sickle cell disease, demonstrating right femoral head osteonecrosis Steinberg stage 4 on (a.A) Anteroposterior and (a.B) Lateral views. (b) Post-bisphosphonate infusion treatment: Follow-up (b.A) Anteroposterior and (b.B) Lateral X-rays obtained 1 year after initial imaging, revealing no progression or collapse. (c) Long-term outcome: (c.A) Anteroposterior and (c.B) Lateral X-rays after 6 years (at age 19), patient presented with resolution of clinical symptoms, and imaging showed a congruent head with no disease progression.

(a) Initial anteroposterior radiographs of an 11-year-old female showing bilateral femoral head osteonecrosis. The right hip was classified as pre-collapse stage 2, and the left hip as post-collapse stage 4 (Steinberg). (b) (b.A) Anteroposterior and (b.B) lateral X-rays Both hips were treated with core decompression and bone marrow aspirate concentrate (CD-BMAC). (c) At final follow-up, (c.A) anteroposterior and (c.B) lateral X rays, the right hip remained stable without progression, while the left hip showed radiographic signs of secondary osteoarthritis.
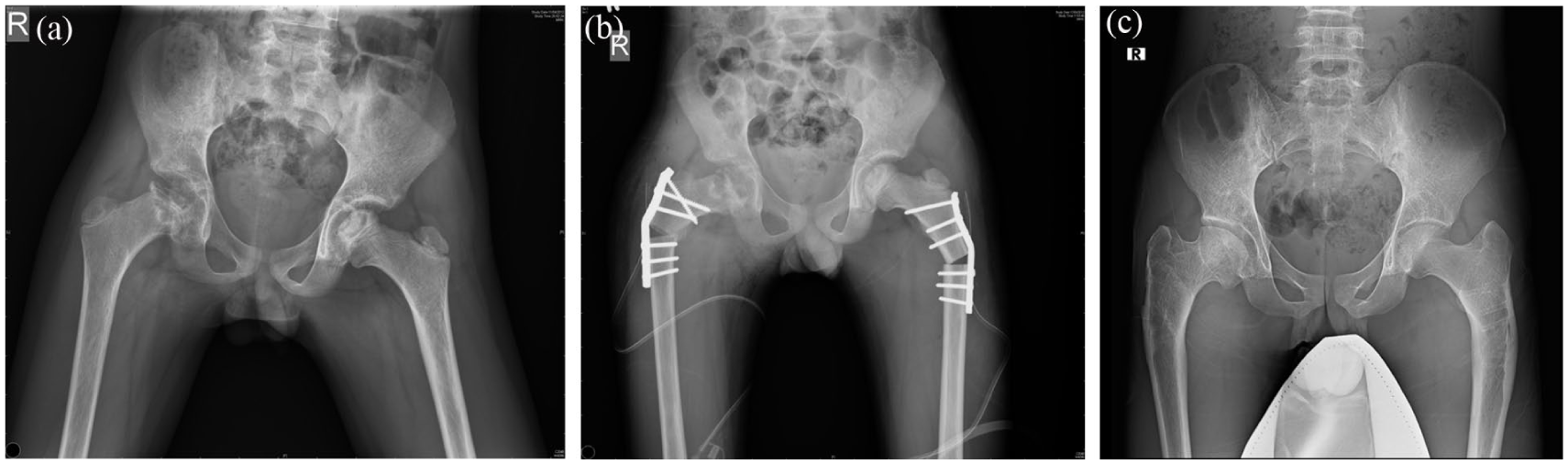
(a) Pre-operative anteroposterior radiographs of a 9-year-old girl with bilateral femoral head osteonecrosis. The right hip demonstrated collapse, while the left hip was in pre-collapse stage 3 Steinberg classification.b) Immediate post-operative anteroposterior radiograph—The patient underwent bilateral femoral varus derotation osteotomy. Note the varus over-correction (approx. 90°), which, while not the intended long-term anatomical goal, resulted in containment. (c) At 11-year follow-up (age 20), anteroposterior radiograph—the right hip maintained joint congruity without further collapse. The left femoral head remained spherical, with near-normal morphology, effectively delaying the need for total hip arthroplasty.
As detailed in Table 3, no disease progression was observed in any pre-collapse hip, regardless of treatment. In contrast, outcomes for post-collapse hips were more variable; disease progression occurred in both the bisphosphonate and CD-BMAC groups, with the two hips in the latter group advancing to arthritis.
Treatment outcomes following bisphosphonates, CD-BMAC, and proximal femur reorientation osteotomy of the 20 hips available at final follow-up.
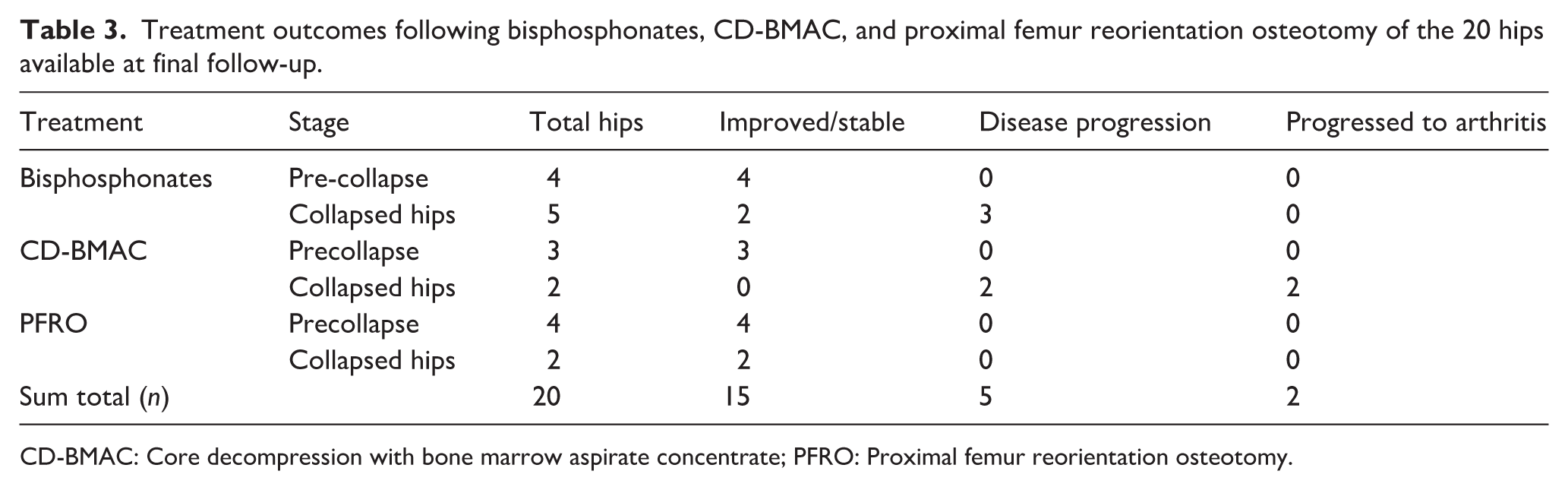
CD-BMAC: Core decompression with bone marrow aspirate concentrate; PFRO: Proximal femur reorientation osteotomy.
Of the five hips that exhibited disease progression (by at least one stage), all were collapsed hips at presentation, three belonged to male patients, three affected the right hip, and four were part of bilateral involvement. Similarly, the two hips that further progressed to arthritis, were collapsed hips at initial presentation and were part of bilateral involvement.
Discussion
This study reports the outcomes of both conservative and operative treatments in FHO in SCD children. Conservative treatment with bisphosphonate infusion and operative treatment with CD-BMAC and PFRO were compared for treatment outcomes with regard to progression of the stage of avascular necrosis and development of arthritis. Our results showed that in the majority of hips (75%), FHO either improved or remained stable, and 90% of hips did not develop arthritis by the final follow-up.
The average age at presentation in our study was 11.6 years (SD-2.8), with bilateral hip involvement in 11 of the 17 children. This is consistent with other reports on FHO in children with SCD. Baghdadi et al. 17 studied 23 hips with femoral head avascular necrosis in 17 patients with SCD, with a median age at surgery of 15.8 years. Similarly, Griffith et al. 18 examined the treatment of FHO in pediatric SCD patients, including 13 patients (average age 14.1 ± 2.8 years, 84.6% male) with 18 affected extremities.
As reported in literature,19,20 SCD was identified as the most common cause of pediatric FHO in our study cohort, accounting for 37% of all cases and 45% of non-traumatic etiologies.
In a case series by Itzep et al., 21 involving 16 SCD patients with FHO, with a mean age of 13.2 years at diagnosis, most patients had femoral head collapse at diagnosis. This finding aligns with our study, where the majority (15 out of 28 hips) had varying degrees of femoral head collapse at diagnosis.
Among the 17 children in our study, 10 (58.8%) were male, and of the 28 hips evaluated, the right side was involved in 16 hips (57.1%). The interval between the onset of SCD and the diagnosis of avascular necrosis (AVN) in our study was 78.8 months (SD-36.6), when compared to 97 months in the study by Almeida-Matos et al., 20 highlighting the chronic nature of disease progression and hence an opportunity for appropriate intervention if diagnosed early.
The literature on managing the FHO in children with SCD is quite limited. 19 Our study explored various treatment modalities, including non-operative intravenous bisphosphonates, head-preserving procedures such as CD + BMAC or PFRO, and salvage procedures like SSD-Osteoplasty, arthroplasty, or excision.
Reconstitution of the femoral head following treatment was indicated by regression of at least one Steinberg stage and no instances of stage progression, as demonstrated in the study by Griffith et al. 18 The same was used in our study. Post-treatment, AVN progressed by at least 1 stage in 5 hips (25%), while 15 hips (75%) improved or remained stable.
At the final follow-up, 2 hips (10%) progressed to arthritis, while 18 hips (90%) did not develop arthritis. The mean follow-up duration was 30.76 months (SD ± 4.46).
We agree with the review by Barney et al. 22 that treatment decisions for FHO should be based primarily on the lesion stage and the presence or absence of collapse. In our study, among the 13 hips in the pre-collapse stage, 6 received bisphosphonate infusion, 3 underwent CD-BMAC, and 4 underwent PFRO. Among the post-collapse hips, 5 received bisphosphonate infusion, 2 underwent CD-BMAC, and 2 underwent PFRO.
Grimbly et al. 10 studied the response to intravenous bisphosphonates in children with sickle cell bone disease and reported significant or complete resolution of bone pain in all 23 children treated with IV bisphosphonates. Among the patients who received bisphosphonates in our study, none of the pre-collapse hips showed further disease progression, while three out of five hips in the post-collapse stage had disease progression, but did not progress to advanced arthritis at final follow-up.
Griffith et al. reported that core decompression combined with BMAC injection in patients with SCD led to radiological reconstitution of the femoral head in 72% of the treated extremities (13 in total), compared to 66% (3 out of 5) in the CD-BMAC treatment group in our study.
At final follow-up, while the pre-collapse hips in our study who received CD-BMAC showed no further disease progression, both hips in the collapsed stage progressed to advanced arthritis. This is similar to the findings of a case series of 16 patients with SCD and FHO by Itzep et al., 21 in which all 5 patients who received core decompression with BMAC showed no improvement, as most of the femoral heads had collapse at diagnosis.
Novais et al. reported the results of CD-BMAC in 14 pediatric non-traumatic FHO cases due to SCD. At a mean follow-up of 25 months, 80% of the hips did not progress clinically or radiographically. 23 Several studies have demonstrated that epiphyseal drilling combined with BMAC injection may improve pain and promote revascularization and healing of necrotic bone in patients with FHO associated with SCD.4,18,23
Clinical studies evaluating treatment outcomes after proximal femoral or pelvic osteotomies in pediatric patients with SCD and FHO, or corticosteroid-induced FHO, are quite limited and insufficient to provide evidence-based treatment guidance. 4 In a retrospective study of 25 hips from 17 patients with SCD and FHO, with a mean age at diagnosis 11.4 years, followed up for a mean 7.5 years, favorable radiographic outcomes (Stulberg grades 1 or 2) were observed in 7 of 12 hips managed nonoperatively, and in 5 of 13 hips treated with femoral varus osteotomy and/or pelvic osteotomy. Additionally, femoral and/or pelvic osteotomy has shown promising functional outcomes in patients with advanced osteonecrosis (Ficat stages 3 and 4). 24
In our study, none of the six hips (both pre-collapse and post-collapse) that underwent PFRO showed disease progression or arthritis. Athanassiou-Metaxa et al. 25 compared functional and radiological outcomes between subtrochanteric varus osteotomy and non-surgical treatment. However, their study lacked evaluation of the initial disease severity and criteria guiding surgical intervention.
Disease progression (advancing by at least one stage) and development of arthritis at final follow-up in our study, were predominantly observed in hips that were collapsed at presentation, belonged to male patients, affected the right side, and were part of bilateral involvement.
Thus, screening and early detection of pre-collapse disease are crucial for proposing conservative treatments. Gupta and Adekile, in their prospective study, reported significant lesion progression in 65% of children, even for asymptomatic cases. 9
Hip preservation procedures can influence the outcomes of subsequent interventions. The International Consensus on Periprosthetic Joint Infection has emphasized that prior open surgeries may predispose patients to a higher risk of infection if THR becomes necessary. 26 In pediatric population, this potential risk must be carefully balanced against the advantages of deferring arthroplasty to preserve native hip function.
Limitations of our study include the retrospective nature of the study, the bias associated with it, and the heterogeneity of the treatment options employed. Even though the sample size of our study is comparable to most of the other studies in literature,17,18 the number of children in each treatment limb may not be sufficient for a statistically significant comparison. Further, the choice of treatment was surgeon-dependent, and indications for each modality were based on individual clinical assessment. This selection bias results in outcomes that are not predictive, but reflects the real-world clinical decision making in the absence of standard treatment algorithms. Also, there were no untreated control group available for comparison in our study.
Though our study is unique for comparing treatment outcomes in the pre-collapse and collapsed stage of FHO in SCD, formulation of a treatment algorithm may not be feasible with the available data. The small sample size (n = 20) limits the ability to draw statistically significant conclusions. Further, outcome evaluation was performed based on radiological disease progression alone, and functional or patient reported outcome measures have not been studied.
However, our study shows that bisphosphonates, CD-BMAC, and PFRO are successful in preventing disease progression in all pre-collapse hips. In post-collapse hips, CD-BMAC failed to arrest disease progression, bisphosphonates showed mixed results, and PFRO prevented further disease progression. But these treatment modalities may not be directly comparable due to differences in the baseline characteristics of all post-collapse cases. Moreover, longer follow-up into adulthood is required to assess further progression and development of arthritis.
In our study, the risk factors for disease progression and arthritis include the stage of avascular necrosis (collapsed hips), male sex, right hip involvement, and bilateral involvement.
Our study supports early intervention in avascular hips at the pre-collapse stage, with appropriate, patient-tailored treatments, aligning with current literature.
Conclusion
All three treatment modalities, bisphosphonates, CD-BMAC, and PFRO, appear to yield similar outcomes in pre-collapse hips. It would be prudent to offer bisphosphonates, as a non-operative treatment, to all patients. For post-collapse hips, PFRO seems to be an appropriate intervention if technically feasible, providing good outcomes by offloading the avascular segment.
Future studies with larger sample sizes and prospective evaluations, incorporating patient reported outcome measures, will be more effective in determining the outcomes of FHO treatments in children with SCD.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261436299 – Supplemental material for Retrospective cohort study assessing radiological outcomes and risk factors for progression of femoral head osteonecrosis in children with sickle cell disease, following bisphosphonate therapy, CD-BMAC and proximal femoral reorientation osteotomy
Supplemental material, sj-pdf-1-cho-10.1177_18632521261436299 for Retrospective cohort study assessing radiological outcomes and risk factors for progression of femoral head osteonecrosis in children with sickle cell disease, following bisphosphonate therapy, CD-BMAC and proximal femoral reorientation osteotomy by Rasim Abid Elayedatt, Abhay Deodas Gahukamble, Arul Murugan A, Vikaas Ethanur Thuppale, Aby Abraham, Madhavi Kandagaddala and Thomas Palocaren in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors used AI tools for language refinement and formatting. All intellectual content and interpretation are original, and author driven. Ms. Rekha, Department of Biostatistics, assisted with statistical analysis.
Author contributions
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional policy and patient confidentiality constraints. However, de-identified data supporting the findings of this study will be made available from the corresponding author upon reasonable request.*
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study was approved by the Institutional Review Board (Silver Ethics and Research Committee), Christian Medical College, Vellore (IRB Min. No. 2411150 dated 20.11.2024). Individual patient consent was not obtained due to the retrospective nature of the study, which involved only radiological data and did not disclose any patient-identifying information. This waiver was approved by the ethics committee.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.